
Polymorphisms in the Genes Coding for TLRs, NLRs and RLRs Are Associated with Clinical Parameters of Patients with Acute Myeloid Leukemia

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
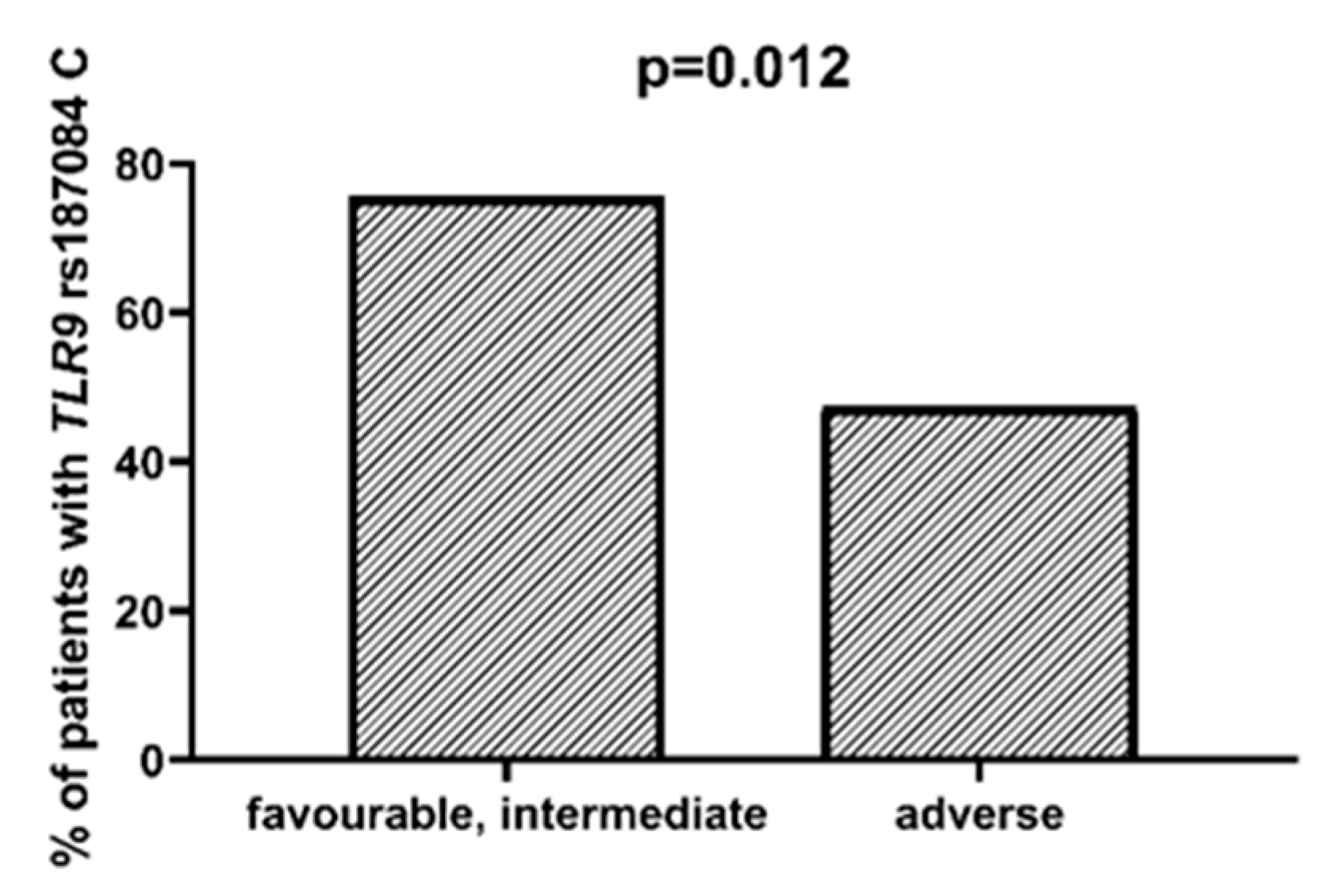
2.1. SNPs in Toll-like Receptors Genes
2.2. SNPs in NOD-like Receptors Genes
2.3. SNPs in the RIG-I-like Receptors Genes
2.4. SNPs in TLRs, NLRs, and RLRs in Groups of Patients >55 yo and ≤55 yo
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. DNA Isolation, Genotyping
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fitzgerald, K.A.; Kagan, J.C. Toll-like Receptors and the Control of Immunity. Cell 2020, 180, 1044–1066. [Google Scholar] [CrossRef]
- Kim, Y.K.; Shin, J.S.; Nahm, M.H. NOD-like receptors in infection, immunity, and diseases. Yonsei Med. J. 2016, 57, 5–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehwinkel, J.; Gack, M.U. RIG-I-like receptors: Their regulation and roles in RNA sensing. Nat. Rev. Immunol. 2020, 20, 537–551. [Google Scholar] [CrossRef]
- Roh, J.S.; Sohn, D.H. Origin and List of DAMPS. Immune Netw. 2018, 18, 1–14. [Google Scholar] [CrossRef]
- Gong, T.; Liu, L.; Jiang, W.; Zhou, R. DAMP-sensing receptors in sterile inflammation and inflammatory diseases. Nat. Rev. Immunol. 2020, 20, 95–112. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Ponzetta, A.; Inforzato, A.; Jaillon, S. Innate Immunity, Inflammation and Tumor Progression: Double Edged Swords. J. Intern. Med. 2019, 285, 524–532. [Google Scholar] [CrossRef] [Green Version]
- Cen, X.; Liu, S.; Cheng, K. The role of toll-like receptor in inflammation and tumor immunity. Front. Pharmacol. 2018, 9, 878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.Q.; Liu, L.; Liu, Y.; Zhang, K. TLR-2 gene polymorphisms and susceptibility to cancer: Evidence from meta-analysis. Genet. Test. Mol. Biomark. 2013, 17, 864–872. [Google Scholar] [CrossRef]
- Mukherjee, S.; Huda, S.; Sinha Babu, S.P. Toll-like receptor polymorphism in host immune response to infectious diseases: A review. Scand. J. Immunol. 2019, 90, e12771. [Google Scholar] [CrossRef] [Green Version]
- Trejo-De La, O.A.; Hernández-Sancén, P.; Maldonado-Bernal, C. Relevance of single-nucleotide polymorphisms in human TLR genes to infectious and inflammatory diseases and cancer. Genes Immun. 2014, 15, 199–209. [Google Scholar] [CrossRef]
- Medvedev, A.E. Toll-like receptor polymorphisms, inflammatory and infectious diseases, allergies, and cancer. J. Interf. Cytokine Res. 2013, 33, 467–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newell, L.F.; Cook, R.J. Advances in acute myeloid leukemia. BMJ 2021, 375, n2026. [Google Scholar] [CrossRef] [PubMed]
- Quirino, M.G.; Macedo, L.C.; Pagnano, K.B.B.; Pagliarini-e-Silva, S.; Sell, A.M.; Visentainer, J.E.L. Toll-like receptor gene polymorphisms in patients with myeloproliferative neoplasms. Mol. Biol. Rep. 2021, 48, 4995–5001. [Google Scholar] [CrossRef]
- Zhou, Y.; Yan, S.; Liu, N.; He, N.; Zhang, A.; Meng, S.; Ji, C.; Ma, D.; Ye, J. Genetic polymorphisms and expression of NLRP3 inflammasome-related genes are associated with Philadelphia chromosome-negative myeloproliferative neoplasms. Hum. Immunol. 2020, 81, 606–613. [Google Scholar] [CrossRef]
- Wang, H.; Hua, M.; Wang, S.; Yu, J.; Chen, C.; Zhao, X.; Zhang, C.; Zhong, C.; Wang, R.; He, N.; et al. Genetic polymorphisms of IL-18 rs1946518 and IL-1β rs16944 are associated with prognosis and survival of acute myeloid leukemia. Inflamm. Res. 2017, 66, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Logan, C.; Koura, D.; Taplitz, R. Updates in infection risk and management in acute leukemia. Hematology (U. S.) 2020, 20, 135–139. [Google Scholar] [CrossRef]
- Gupta, A.; Singh, M.; Singh, H.; Kumar, L.; Sharma, A.; Bakhshi, S.; Raina, V.; Thulkar, S. Infections in acute myeloid leukemia: An analysis of 382 febrile episodes. Med. Oncol. 2010, 27, 1037–1045. [Google Scholar] [CrossRef]
- Nganthavee, V.; Phutthasakda, W.; Atipas, K.; Tanpong, S.; Pungprasert, T.; Dhirachaikulpanich, D.; Krithin, S.; Tanglitanon, S.; Jutidamronphang, W.; Owattanapanich, W.; et al. High incidence of invasive fungal infection during acute myeloid leukemia treatment in a resource-limited country: Clinical risk factors and treatment outcomes. Support. Care Cancer 2019, 27, 3613–3622. [Google Scholar] [CrossRef]
- Chen, Y.; Lin, J.; Zhao, Y.; Ma, X.; Yi, H. Toll-like receptor 3 (TLR3) regulation mechanisms and roles in antiviral innate immune responses. J. Zhejiang Univ. Sci. B 2021, 22, 609–632. [Google Scholar] [CrossRef]
- Kantarjian, H.M.; Kadia, T.M.; DiNardo, C.D.; Welch, M.A.; Ravandi, F. Acute myeloid leukemia: Treatment and research outlook for 2021 and the MD Anderson approach. Cancer 2021, 127, 1186–1207. [Google Scholar] [CrossRef]
- Acharya, U.H.; Halpern, A.B.; Wu, Q.; Voutsinas, J.M.; Walter, R.B.; Yun, S.; Kanaan, M.; Estey, E.H. Impact of region of diagnosis, ethnicity, age, and gender on survival in acute myeloid leukemia (AML). J. Drug Assess. 2018, 7, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Yoneyama, M.; Kikuchi, M.; Natsukawa, T.; Shinobu, N.; Imaizumi, T.; Miyagishi, M.; Taira, K.; Akira, S.; Fujita, T. The RNA helicase RIG-I has an essential function in double-stranded RNA-induced innate antiviral responses. Nat. Immunol. 2004, 5, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Rintahaka, J.; Wiik, D.; Kovanen, P.E.; Alenius, H.; Matikainen, S. Cytosolic Antiviral RNA Recognition Pathway Activates Caspases 1 and 3. J. Immunol. 2008, 180, 1749–1757. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; Karin, M.; Sun, B. Targeting cancer-promoting inflammation—Have anti-inflammatory therapies come of age? Nat. Rev. Clin. Oncol. 2021, 18, 261–279. [Google Scholar] [CrossRef]
- Colotta, F.; Allavena, P.; Sica, A.; Garlanda, C.; Mantovani, A. Cancer-related inflammation, the seventh hallmark of cancer: Links to genetic instability. Carcinogenesis 2009, 30, 1073–1081. [Google Scholar] [CrossRef] [Green Version]
- Fianchi, L.; Quattrone, M.; Criscuolo, M.; Bellesi, S.; Dragonetti, G.; Maraglino, A.M.E.; Bonanni, M.; Chiusolo, P.; Sica, S.; Pagano, L. Extramedullary Involvement in Acute Myeloid Leukemia. A Single Center Ten Years’ Experience. Mediterr. J. Hematol. Infect. Dis. 2021, 13, e2021030. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.; Hascall, V.C.; Markwald, R.R.; O’Brien, P.E.; Ghatak, S. Inflammation and Cancer. Wound Heal. Stem Cells Repair Restor. Basic Clin. Asp. 2018, 420, 239–274. [Google Scholar] [CrossRef]
- Shrotriya, S.; Walsh, D.; Bennani-Baiti, N.; Thomas, S.; Lorton, C. C-reactive protein is an important biomarker for prognosis tumor recurrence and treatment response in adult solid tumors: A systematic review. PLoS ONE 2015, 10, e0143080. [Google Scholar] [CrossRef]
- Gradel, K.O.; Póvoa, P.; Garvik, O.S.; Vinholt, P.J.; Nielsen, S.L.; Jensen, T.G.; Chen, M.; Dessau, R.B.; Møller, J.K.; Coia, J.E.; et al. Longitudinal trajectory patterns of plasma albumin and C-reactive protein levels around diagnosis, relapse, bacteraemia, and death of acute myeloid leukaemia patients. BMC Cancer 2020, 20, 249. [Google Scholar] [CrossRef]
- Shaaban, Y.; Taalab, M.M.; Aref, S.; Mabed, M. AML-029: The Prognostic Significance of Serum Lactate Dehydrogenase Level in Egyptian AML Patients. Clin. Lymphoma Myeloma Leuk. 2020, 20, S174. [Google Scholar] [CrossRef]
- Xiao, Z.; Gong, R.; Chen, X.; Xiao, D.; Luo, S.; Ji, Y. Association between serum lactate dehydrogenase and 60-day mortality in Chinese Hakka patients with acute myeloid leukemia: A cohort study. J. Clin. Lab. Anal. 2021, 35, e24049. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SNPs in Gene for TLR3 | SNPs in Gene for TLR4 | SNPs in Gene for TLR9 | |
|---|---|---|---|
| Favorable/intermediate risk according to ELN | rs187084 C | ||
| Lower CRP level | rs4986791 T | rs5743836 C | |
| Higher CRP level | rs4986791 CC | rs5743836 TT | |
| Lower LDH level | rs3775291 A | ||
| Higher LDH level | rs3775291 G | ||
| Higher risk of infection | rs5743305 AA | ||
| Extramedullary metastases | rs3775296 T | rs4986790 G | |
| No extramedullary metastases | rs3775291 A | rs187084 C |
| Characteristic | Study Group (n = 90) |
|---|---|
| Median age | 61 (range 21–81) |
| Age ≤ 55 yo | 36 |
| Age > 55 yo | 54 |
| Gender | |
| Female | 48 |
| Male | 42 |
| % of blasts in bone marrow at diagnosis | |
| On average | 56 |
| <56 | 41 |
| ≥56 | 48 |
| LDH (U/L) at diagnosis | |
| Median | 540 |
| Within normal range (<220 U/L) | 8 |
| Elevated (≥220 U/L) | 82 |
| CRP (mg/L) at diagnosis | |
| Median | 31.15 |
| Within normal range (<5 mg/L) | 21 |
| Elevated (≥5 mg/L) | 69 |
| Extramedullary metastases at diagnosis | |
| Yes | 13 |
| No | 77 |
| Risk according to ELN | |
| Favorable/intermediate | 52 |
| Unfavorable | 38 |
| Infectious complications during treatment | |
| Yes | 50 |
| No | 40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wicherska-Pawłowska, K.; Bogunia-Kubik, K.; Kuszczak, B.; Łacina, P.; Dratwa, M.; Jaźwiec, B.; Wróbel, T.; Rybka, J. Polymorphisms in the Genes Coding for TLRs, NLRs and RLRs Are Associated with Clinical Parameters of Patients with Acute Myeloid Leukemia. Int. J. Mol. Sci. 2022, 23, 9593. https://doi.org/10.3390/ijms23179593
Wicherska-Pawłowska K, Bogunia-Kubik K, Kuszczak B, Łacina P, Dratwa M, Jaźwiec B, Wróbel T, Rybka J. Polymorphisms in the Genes Coding for TLRs, NLRs and RLRs Are Associated with Clinical Parameters of Patients with Acute Myeloid Leukemia. International Journal of Molecular Sciences. 2022; 23(17):9593. https://doi.org/10.3390/ijms23179593
Chicago/Turabian StyleWicherska-Pawłowska, Katarzyna, Katarzyna Bogunia-Kubik, Bartłomiej Kuszczak, Piotr Łacina, Marta Dratwa, Bożena Jaźwiec, Tomasz Wróbel, and Justyna Rybka. 2022. "Polymorphisms in the Genes Coding for TLRs, NLRs and RLRs Are Associated with Clinical Parameters of Patients with Acute Myeloid Leukemia" International Journal of Molecular Sciences 23, no. 17: 9593. https://doi.org/10.3390/ijms23179593
APA StyleWicherska-Pawłowska, K., Bogunia-Kubik, K., Kuszczak, B., Łacina, P., Dratwa, M., Jaźwiec, B., Wróbel, T., & Rybka, J. (2022). Polymorphisms in the Genes Coding for TLRs, NLRs and RLRs Are Associated with Clinical Parameters of Patients with Acute Myeloid Leukemia. International Journal of Molecular Sciences, 23(17), 9593. https://doi.org/10.3390/ijms23179593