
AR Expression Correlates with Distinctive Clinicopathological and Genomic Features in Breast Cancer Regardless of ESR1 Expression Status

 , and
, and
Abstract
:1. Introduction
2. Results
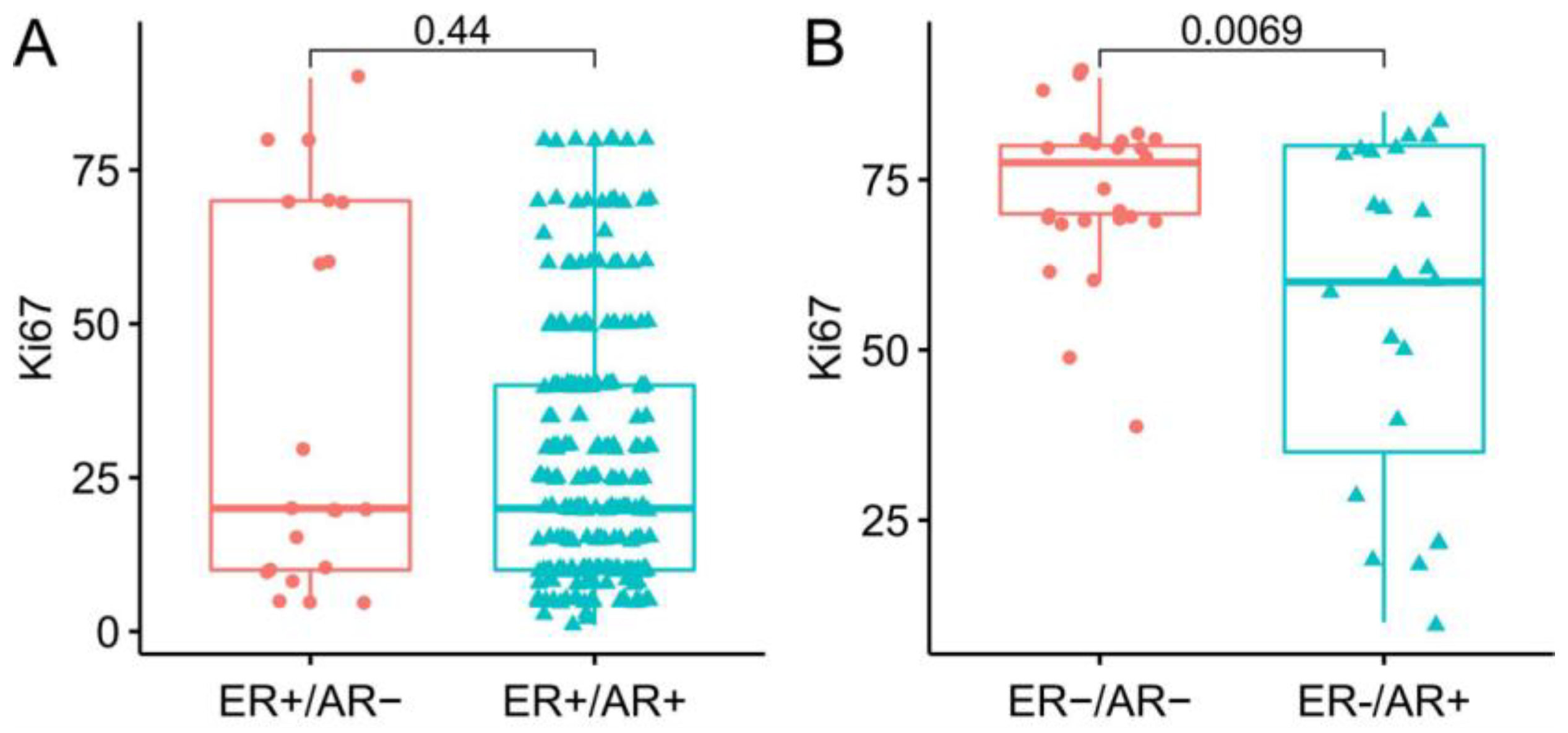
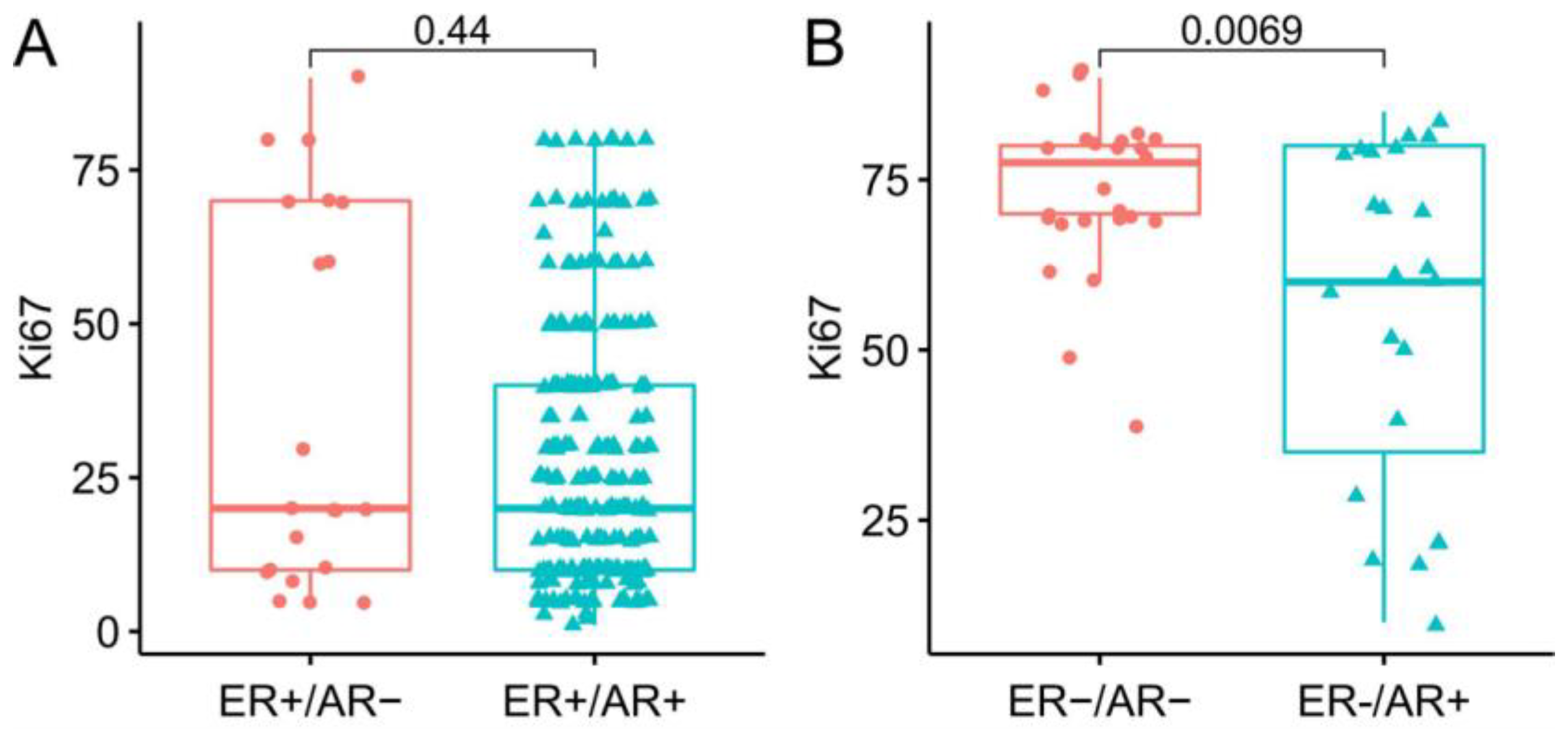
2.1. AR Expression and Clinicopathological Features in ER-Positive and ER-Negative Breast Cancer
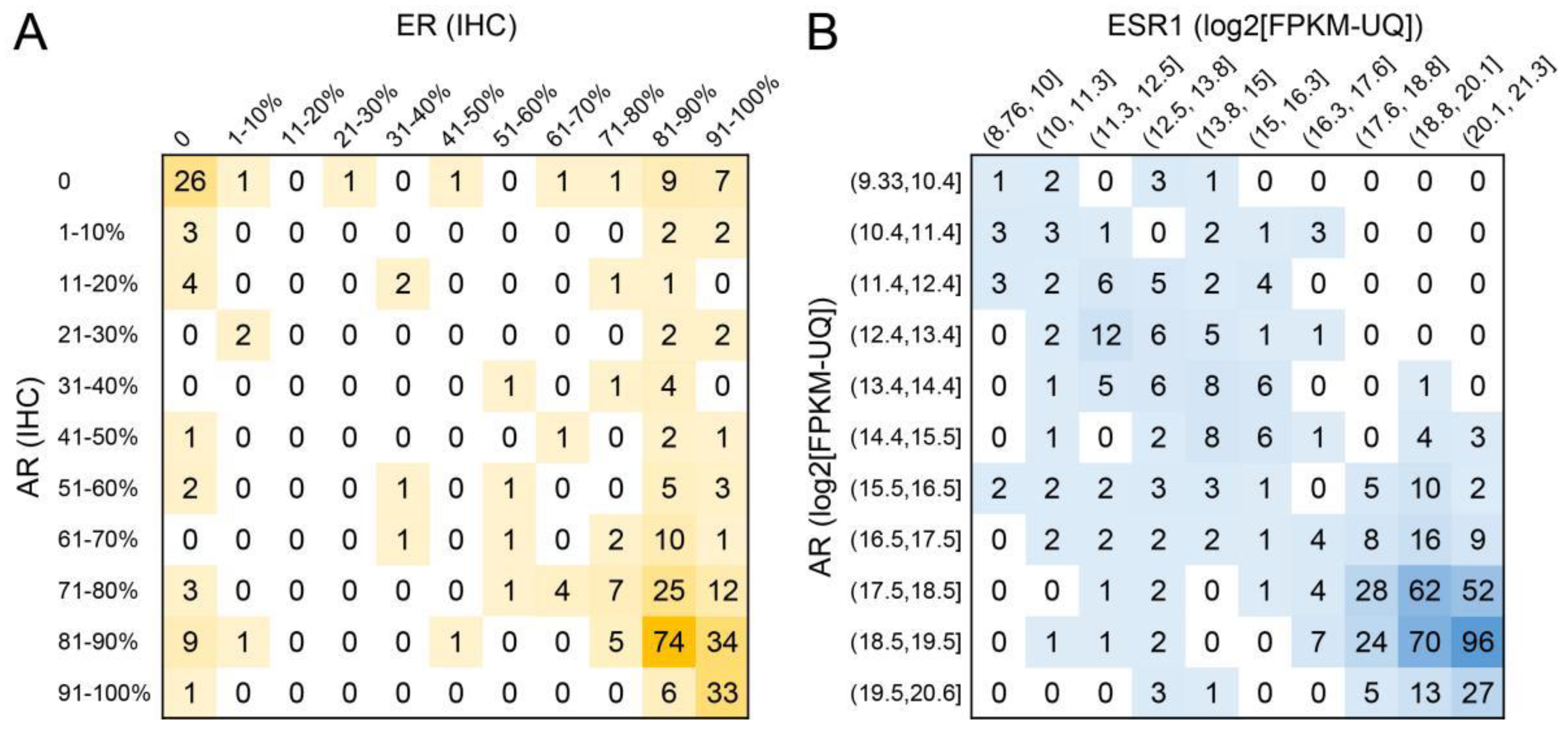
2.2. Estrogen Receptor Expression Correlates with Androgen Receptor Expression
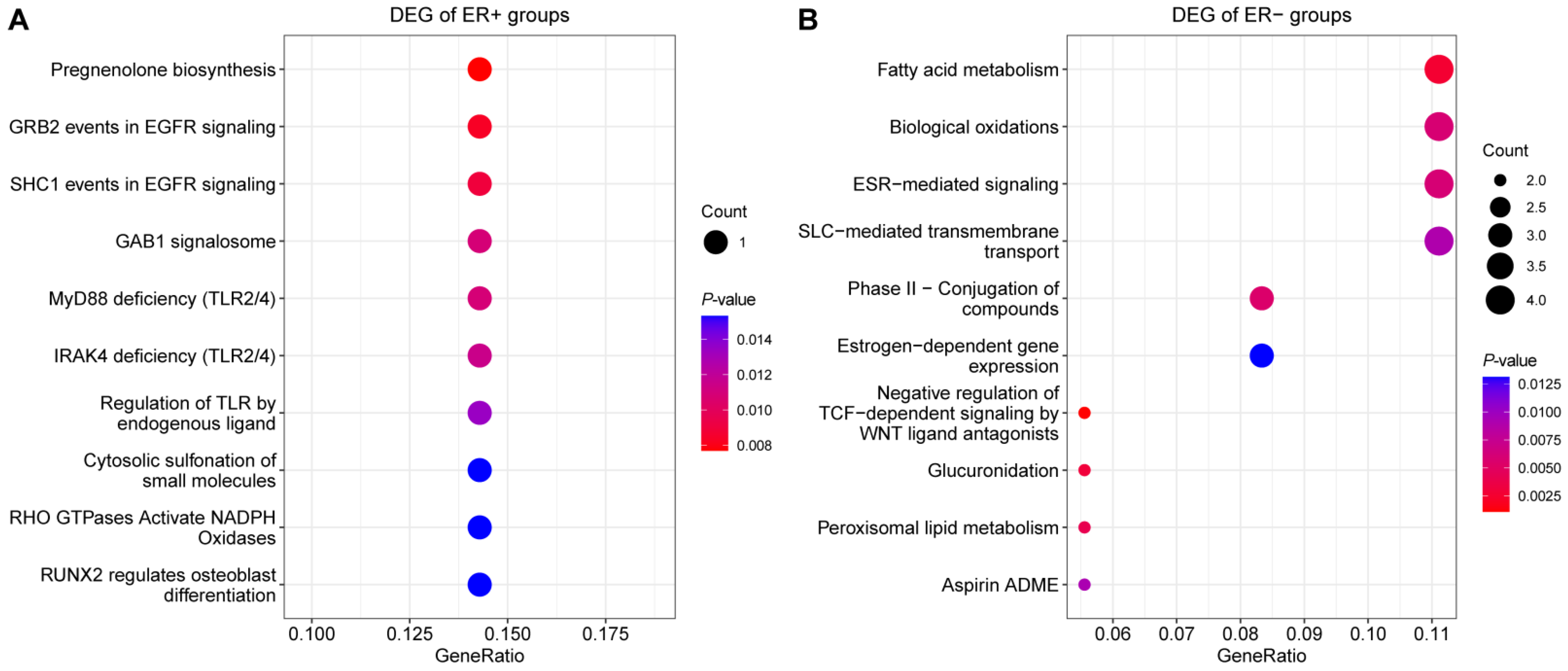
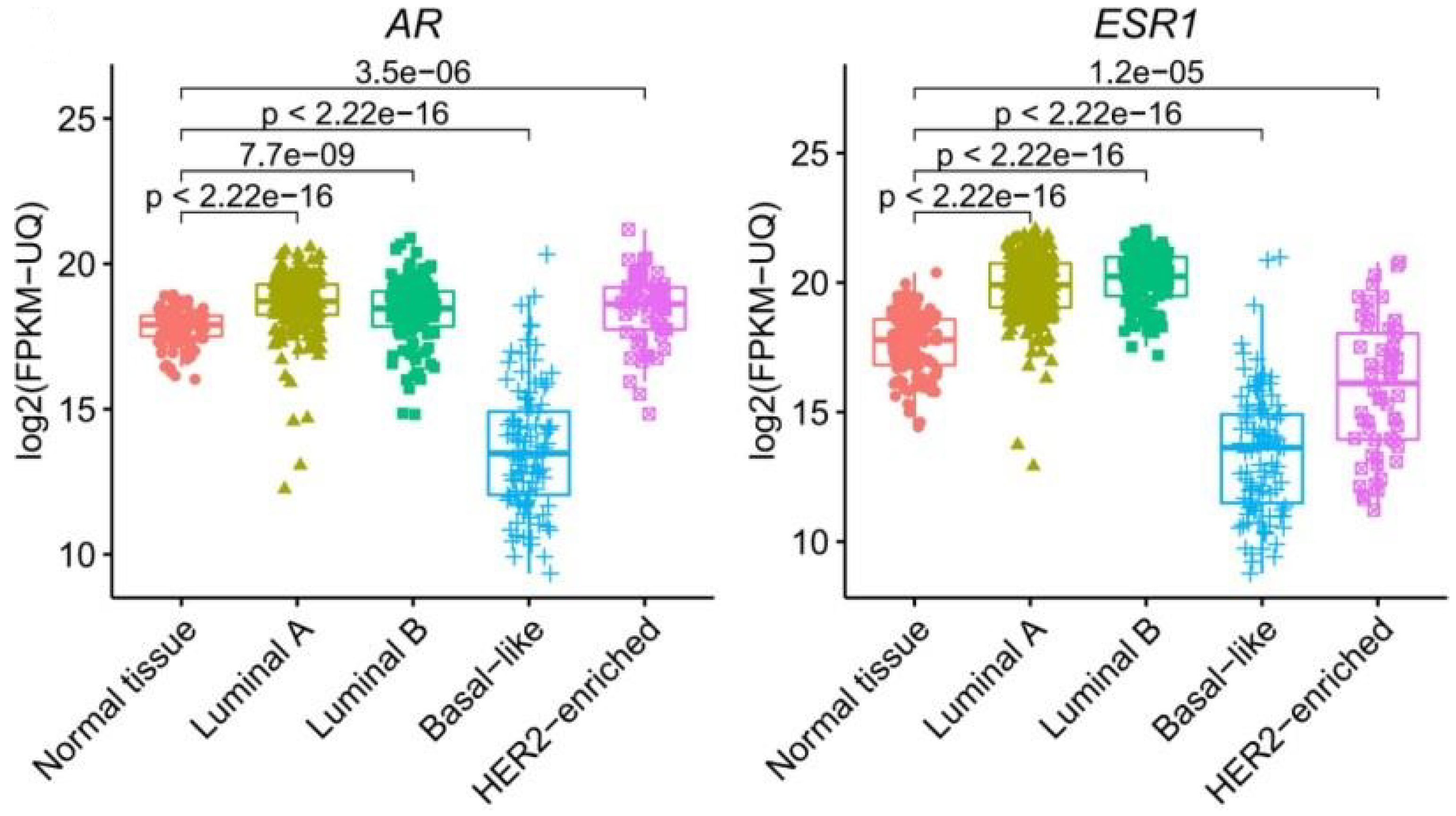
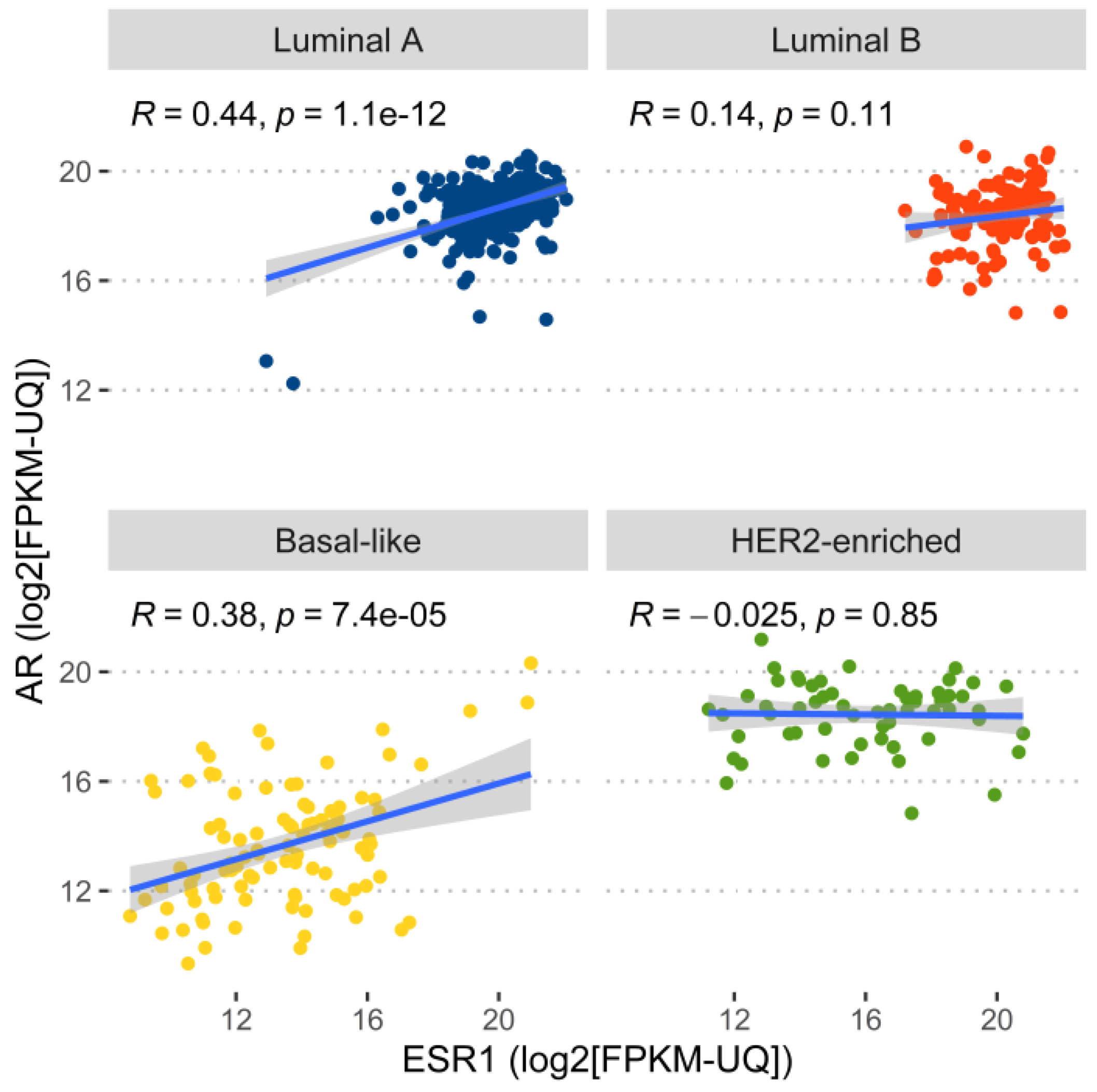
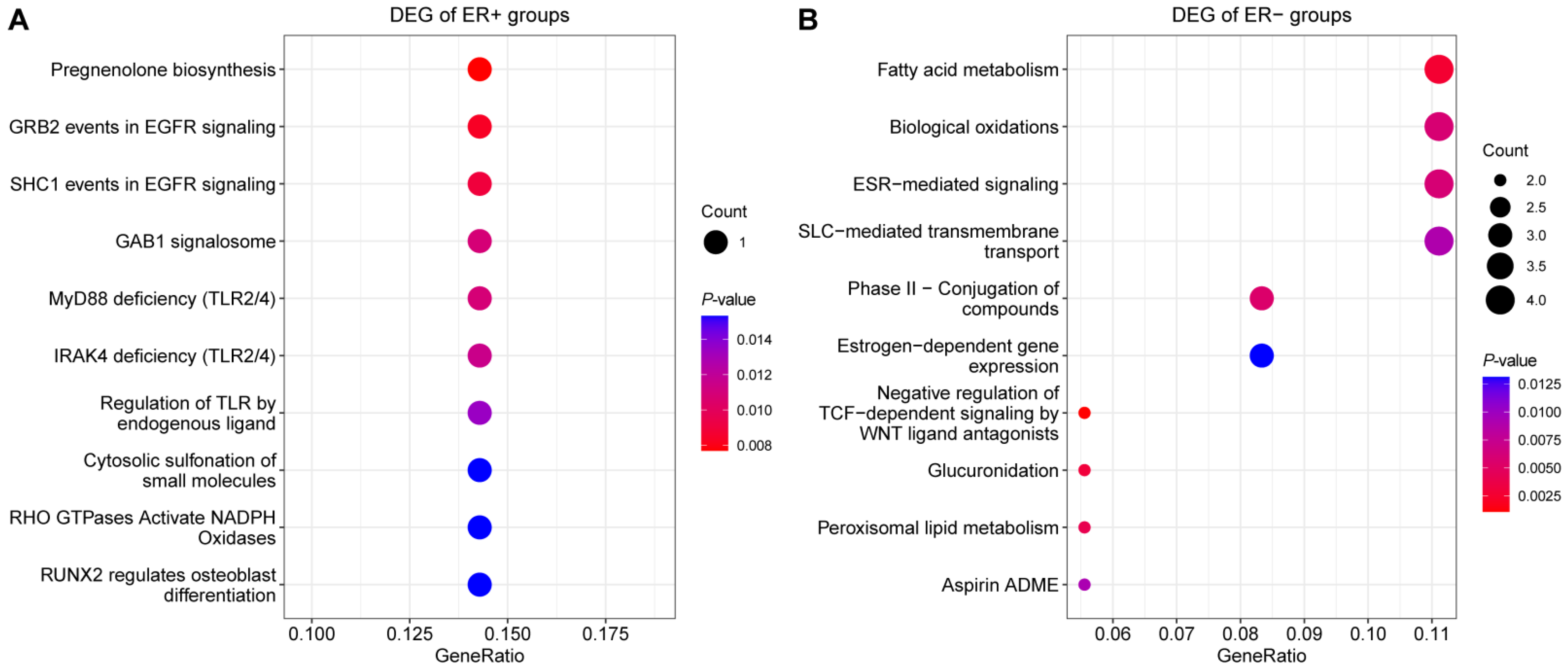
2.3. Androgen Receptor Expression Regulation Was Different in ER-Positive and ER-Negative Breast Cancer
3. Discussion
4. Materials and Methods
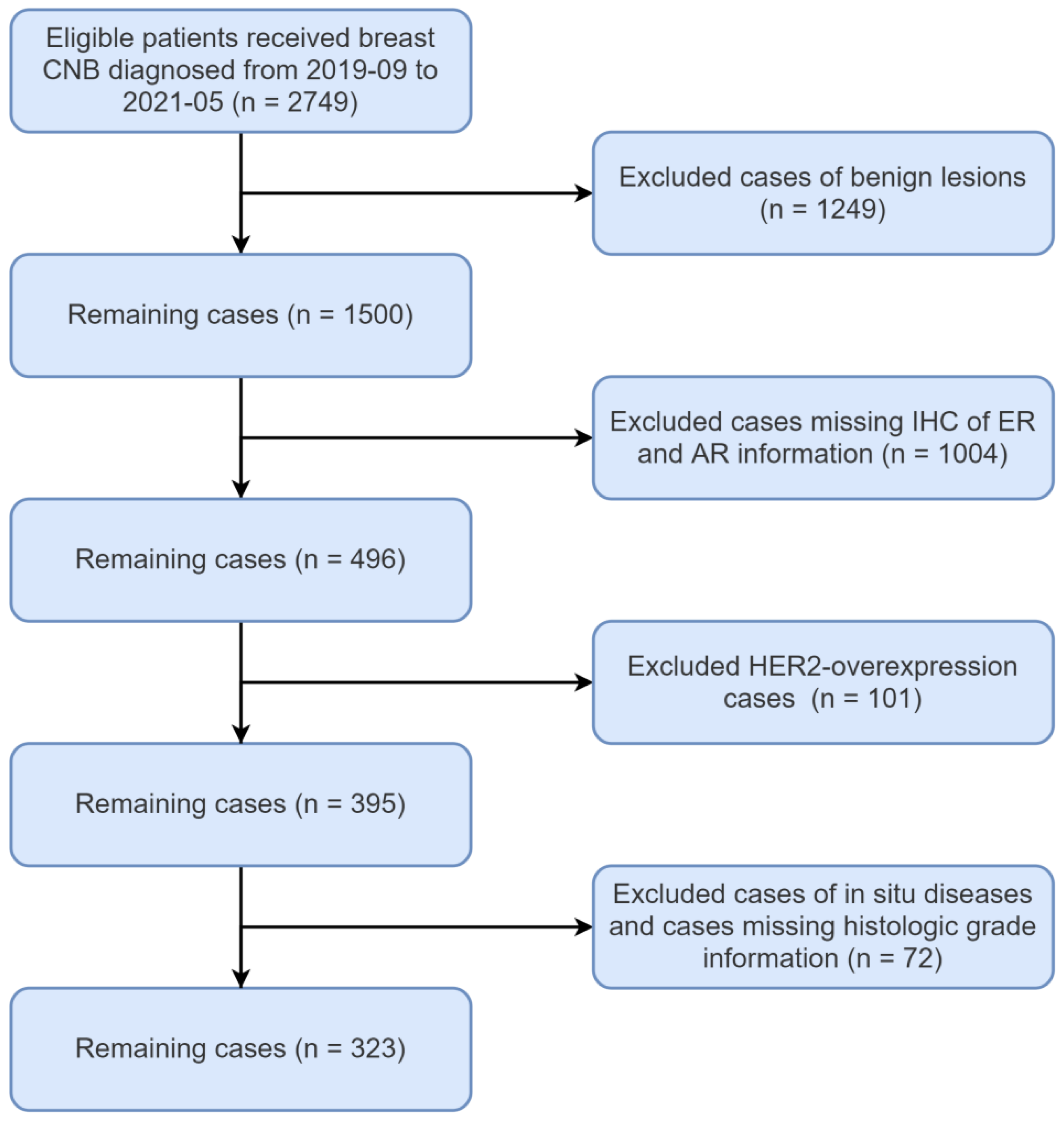
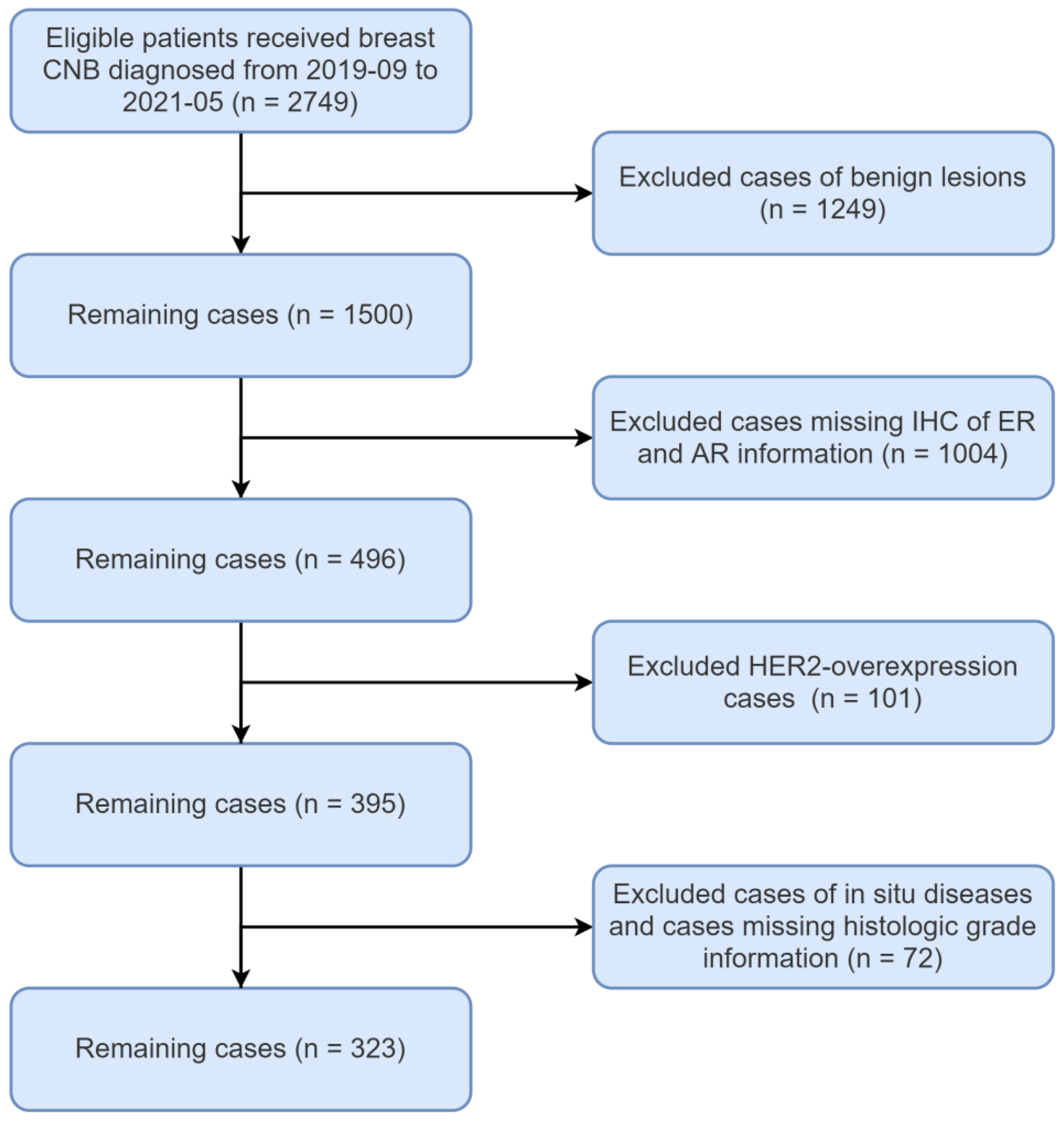
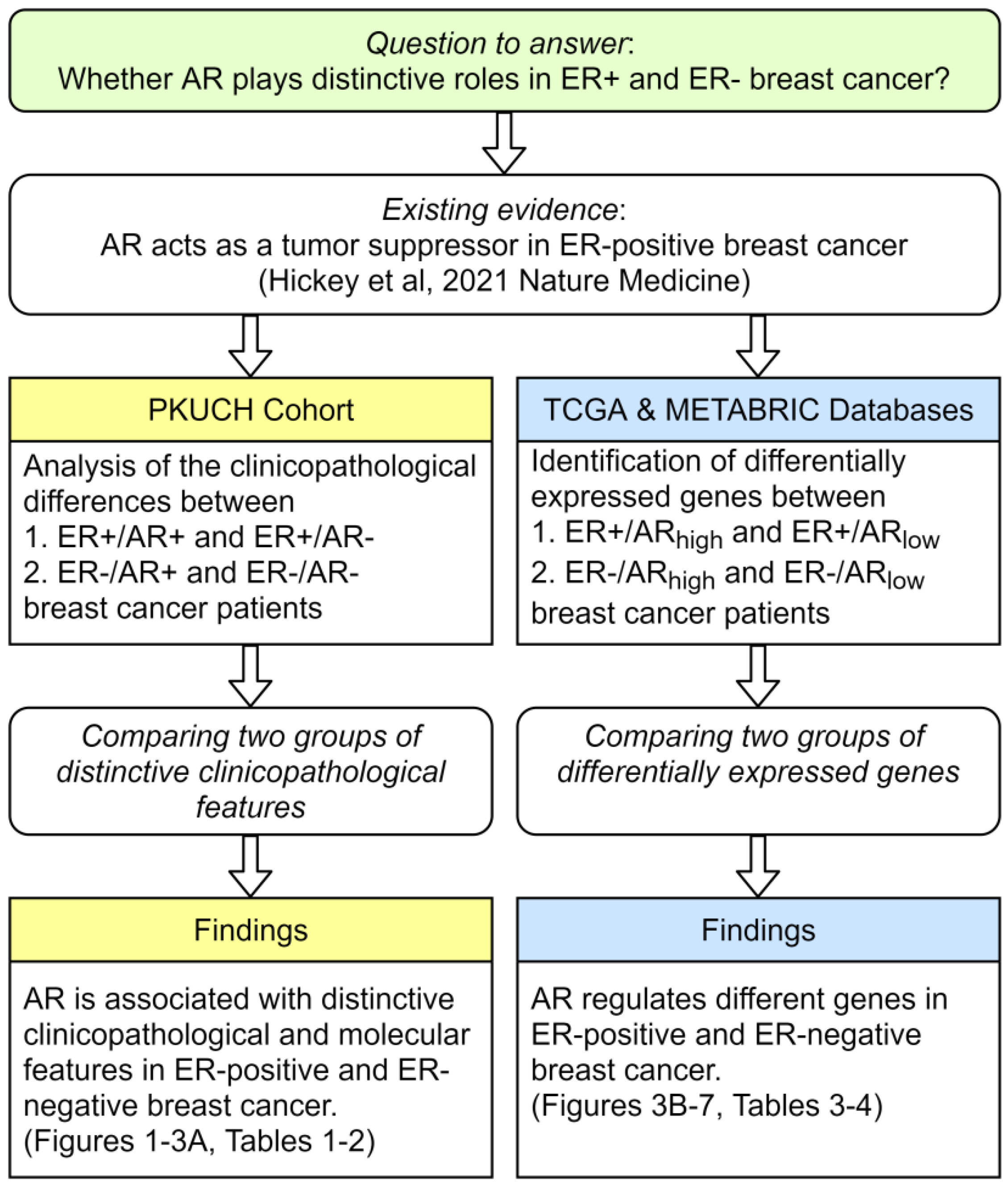
4.1. Study Design
4.2. Patient Selection in PKUCH Cohort
4.3. Immunohistochemical Staining and Analysis of PKUCH Cohort
4.4. Analysis of Differentially Expressed Genes in Breast Cancer from TCGA
4.5. Analysis of Differentially Expressed Genes in Breast Cancer from METABRIC
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, Y.; Yang, D.; Yin, X.; Zhang, X.; Huang, J.; Wu, Y.; Wang, M.; Yi, Z.; Li, H.; Li, H.; et al. Clinicopathological Characteristics and Breast Cancer–Specific Survival of Patients with Single Hormone Receptor–Positive Breast Cancer. JAMA Netw. Open 2020, 3, e1918160. [Google Scholar] [CrossRef] [PubMed]
- Knight, W.A., 3rd; Osborne, C.K.; Yochmowitz, M.G.; McGuire, W.L. Steroid hormone receptors in the management of human breast cancer. Ann. Clin. Res. 1980, 12, 202–207. [Google Scholar] [PubMed]
- Anestis, A.; Zoi, I.; Papavassiliou, A.G.; Karamouzis, M.V. Androgen Receptor in Breast Cancer—Clinical and Preclinical Research Insights. Molecules 2020, 25, 358. [Google Scholar] [CrossRef] [PubMed]
- Astvatsaturyan, K.; Yue, Y.; Walts, A.E.; Bose, S. Androgen receptor positive triple negative breast cancer: Clinicopathologic, prognostic, and predictive features. PLoS ONE 2018, 13, e0197827. [Google Scholar] [CrossRef]
- Niemeier, L.A.; Dabbs, D.J.; Beriwal, S.; Striebel, J.M.; Bhargava, R. Androgen receptor in breast cancer: Expression in estrogen receptor-positive tumors and in estrogen receptor-negative tumors with apocrine differentiation. Mod. Pathol. 2010, 23, 205–212. [Google Scholar] [CrossRef]
- Brumec, M.; Sobočan, M.; Takač, I.; Arko, D. Clinical Implications of Androgen-Positive Triple-Negative Breast Cancer. Cancers 2021, 13, 1642. [Google Scholar] [CrossRef]
- Rangel, N.; Lagos, M.R.; Annaratone, L.; Osella-Abate, S.; Metovic, J.; Mano, M.P.; Bertero, L.; Cassoni, P.; Sapino, A.; Castellano, I. The role of the AR/ER ratio in ER-positive breast cancer patients. Endocr. Relat. Cancer 2018, 25, 163–172. [Google Scholar] [CrossRef]
- Vera-Badillo, F.E.; Templeton, A.J.; De Gouveia, P.; Diaz-Padilla, I.; Bedard, P.L.; Al-Mubarak, M.; Seruga, B.; Tannock, I.F.; Ocana, A.; Amir, E. Androgen Receptor Expression and Outcomes in Early Breast Cancer: A Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2014, 106, djt319. [Google Scholar] [CrossRef]
- Bozovic-Spasojevic, I.; Zardavas, D.; Brohée, S.; Ameye, L.; Fumagalli, D.; Ades, F.; de Azambuja, E.; Bareche, Y.; Piccart, M.; Paesmans, M.; et al. The Prognostic Role of Androgen Receptor in Patients with Early-Stage Breast Cancer: A Meta-analysis of Clinical and Gene Expression Data. Clin. Cancer Res. 2017, 23, 2702–2712. [Google Scholar] [CrossRef]
- Jiang, H.-S.; Kuang, X.-Y.; Sun, W.-L.; Xu, Y.; Zheng, Y.-Z.; Liu, Y.-R.; Lang, G.-T.; Qiao, F.; Hu, X.; Shao, Z.-M. Androgen receptor expression predicts different clinical outcomes for breast cancer patients stratified by hormone receptor status. Oncotarget 2016, 7, 41285–41293. [Google Scholar] [CrossRef] [Green Version]
- Kensler, K.H.; Regan, M.M.; Heng, Y.J.; Baker, G.M.; Pyle, M.E.; Schnitt, S.J.; Hazra, A.; Kammler, R.; Thürlimann, B.; Colleoni, M.; et al. Prognostic and predictive value of androgen receptor expression in postmenopausal women with estrogen receptor-positive breast cancer: Results from the Breast International Group Trial 1–98. Breast Cancer Res. 2019, 21, 30. [Google Scholar] [CrossRef] [PubMed]
- Hickey, T.E.; Robinson, J.L.L.; Carroll, J.S.; Tilley, W.D. Minireview: The Androgen Receptor in Breast Tissues: Growth Inhibitor, Tumor Suppressor, Oncogene? Mol. Endocrinol. 2012, 26, 1252–1267. [Google Scholar] [CrossRef] [PubMed]
- D’Amato, N.C.; Gordon, M.A.; Babbs, B.L.; Spoelstra, N.S.; Butterfield, K.T.C.; Torkko, K.C.; Phan, V.T.; Barton, V.N.; Rogers, T.J.; Sartorius, C.A.; et al. Cooperative Dynamics of AR and ER Activity in Breast Cancer. Mol. Cancer Res. 2016, 14, 1054–1067. [Google Scholar] [CrossRef]
- Okano, M.; Oshi, M.; Butash, A.L.; Asaoka, M.; Katsuta, E.; Peng, X.; Qi, Q.; Yan, L.; Takabe, K. Estrogen Receptor Positive Breast Cancer with High Expression of Androgen Receptor has Less Cytolytic Activity and Worse Response to Neoadjuvant Chemotherapy but Better Survival. Int. J. Mol. Sci. 2019, 20, 2655. [Google Scholar] [CrossRef] [PubMed]
- Hickey, T.E.; Selth, L.A.; Chia, K.M.; Laven-Law, G.; Milioli, H.H.; Roden, D.; Jindal, S.; Hui, M.; Finlay-Schultz, J.; Ebrahimie, E.; et al. The androgen receptor is a tumor suppressor in estrogen receptor–positive breast cancer. Nat. Med. 2021, 27, 310–320. [Google Scholar] [CrossRef]
- You, C.-P.; Leung, M.-H.; Tsang, W.-C.; Khoo, U.-S.; Tsoi, H. Androgen Receptor as an Emerging Feasible Biomarker for Breast Cancer. Biomolecules 2022, 12, 72. [Google Scholar] [CrossRef]
- Ni, M.; Chen, Y.; Lim, E.; Wimberly, H.; Bailey, S.T.; Imai, Y.; Rimm, D.L.; Liu, X.S.; Brown, M. Targeting Androgen Receptor in Estrogen Receptor-Negative Breast Cancer. Cancer Cell 2011, 20, 119–131. [Google Scholar] [CrossRef]
- Doane, A.S.; Danso, M.; Lal, P.; Donaton, M.; Zhang, L.; Hudis, C.; Gerald, W.L. An estrogen receptor-negative breast cancer subset characterized by a hormonally regulated transcriptional program and response to androgen. Oncogene 2006, 25, 3994–4008. [Google Scholar] [CrossRef]
- Traina, T.A.; Miller, K.; Yardley, D.A.; Eakle, J.; Schwartzberg, L.S.; O’Shaughnessy, J.; Gradishar, W.; Schmid, P.; Winer, E.; Kelly, C.; et al. Enzalutamide for the Treatment of Androgen Receptor–Expressing Triple-Negative Breast Cancer. J. Clin. Oncol. 2018, 36, 884–890. [Google Scholar] [CrossRef]
- Krop, I.; Abramson, V.G.; Colleoni, M.; Traina, T.A.; Holmes, F.A.; Garcia-Estevez, L.; Hart, L.; Awada, A.; Zamagni, C.; Morris, P.G.; et al. A Randomized Placebo Controlled Phase II Trial Evaluating Exemestane with or without Enzalutamide in Patients with Hormone Receptor–Positive Breast Cancer. Clin. Cancer Res. 2020, 26, 6149–6157. [Google Scholar] [CrossRef]
- Narayanan, R.; Coss, C.C.; Dalton, J.T. Development of selective androgen receptor modulators (SARMs). Mol. Cell. Endocrinol. 2018, 465, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Cheang, M.C.; Voduc, D.; Bajdik, C.; Leung, S.; McKinney, S.; Chia, S.K.; Perou, C.M.; Nielsen, T.O. Basal-Like Breast Cancer Defined by Five Biomarkers Has Superior Prognostic Value than Triple-Negative Phenotype. Clin. Cancer Res. 2008, 14, 1368–1376. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Liu, L.; Li, Y.; Song, Z.; Jing, Y.; Fan, Z.; Zhang, S. Analysis of CK5/6 and EGFR and Its Effect on Prognosis of Triple Negative Breast Cancer. Front. Oncol. 2021, 10, 575317. [Google Scholar] [CrossRef] [PubMed]
- Tsang, J.Y.S.; Ni, Y.-B.; Chan, S.-K.; Shao, M.-M.; Law, B.K.B.; Tan, P.H.; Tse, G.M. Androgen Receptor Expression Shows Distinctive Significance in ER Positive and Negative Breast Cancers. Ann. Surg. Oncol. 2014, 21, 2218–2228. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Tapias, P.; Rubiano, W.; Rondón-Lagos, M.; Villegas, V.-E.; Rangel, N. Intrinsic Subtypes and Androgen Receptor Gene Expression in Primary Breast Cancer. A Meta-Analysis. Biology 2021, 10, 834. [Google Scholar] [CrossRef]
- Rangel, N.; Rondon-Lagos, M.; Annaratone, L.; Aristizábal-Pachon, A.F.; Cassoni, P.; Sapino, A.; Castellano, I. AR/ER Ratio Correlates with Expression of Proliferation Markers and with Distinct Subset of Breast Tumors. Cells 2020, 9, 1064. [Google Scholar] [CrossRef]
- Yin, L.; Duan, J.-J.; Bian, X.-W.; Yu, S.-C. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res. 2020, 22, 61. [Google Scholar] [CrossRef]
- Masuda, H.; Baggerly, K.A.; Wang, Y.; Zhang, Y.; Gonzalez-Angulo, A.M.; Meric-Bernstam, F.; Valero, V.; Lehmann, B.D.; Pietenpol, J.A.; Hortobagyi, G.N.; et al. Differential Response to Neoadjuvant Chemotherapy Among 7 Triple-Negative Breast Cancer Molecular Subtypes. Clin. Cancer Res. 2013, 19, 5533–5540. [Google Scholar] [CrossRef]
- Jiang, Y.-Z.; Ma, D.; Suo, C.; Shi, J.; Xue, M.; Hu, X.; Xiao, Y.; Yu, K.-D.; Liu, Y.-R.; Yu, Y.; et al. Genomic and Transcriptomic Landscape of Triple-Negative Breast Cancers: Subtypes and Treatment Strategies. Cancer Cell 2019, 35, 428–440.e5. [Google Scholar] [CrossRef]
- Angajala, A.; Mothershed, E.; Davis, M.B.; Tripathi, S.; He, Q.; Bedi, D.; Dean-Colomb, W.; Yates, C. Quadruple Negative Breast Cancers (QNBC) Demonstrate Subtype Consistency among Primary and Recurrent or Metastatic Breast Cancer. Transl. Oncol. 2019, 12, 493–501. [Google Scholar] [CrossRef]
- Kim, E.Y.; Lee, K.H.; Yun, J.-S.; Park, Y.L.; Park, C.H.; Do, S.-I.; Chae, S.W. Clinicopathologic significance of androgen receptor expression and discordant receptor status during progression in breast cancer. Int. J. Clin. Exp. Pathol. 2017, 10, 7929–7939. [Google Scholar] [PubMed]
- Dieci, M.V.; Tsvetkova, V.; Griguolo, G.; Miglietta, F.; Mantiero, M.; Tasca, G.; Cumerlato, E.; Giorgi, C.A.; Giarratano, T.; Faggioni, G.; et al. Androgen Receptor Expression and Association With Distant Disease-Free Survival in Triple Negative Breast Cancer: Analysis of 263 Patients Treated With Standard Therapy for Stage I-III Disease. Front. Oncol. 2019, 9, 452. [Google Scholar] [CrossRef] [PubMed]
- Sunar, V.; Dogan, H.T.; Sarici, F.; Ates, O.; Akin, S.; Baspinar, B.; Aksoy, S.; Altundag, K. Association between androgen receptor status and prognosis in triple negative breast cancer. J. BUON 2018, 23, 1325–1330. [Google Scholar] [PubMed]
- Pistelli, M.; Caramanti, M.; Biscotti, T.; Santinelli, A.; Pagliacci, A.; De Lisa, M.; Ballatore, Z.; Ridolfi, F.; Maccaroni, E.; Bracci, R.; et al. Androgen Receptor Expression in Early Triple-Negative Breast Cancer: Clinical Significance and Prognostic Associations. Cancers 2014, 6, 1351–1362. [Google Scholar] [CrossRef] [PubMed]
- Liu, D. AR pathway activity correlates with AR expression in a HER2-dependent manner and serves as a better prognostic factor in breast cancer. Cell. Oncol. 2020, 43, 321–333. [Google Scholar] [CrossRef]
- Lin, C.-H.; Yap, Y.S.; Lee, K.-H.; Im, S.-A.; Naito, Y.; Yeo, W.; Ueno, T.; Kwong, A.; Li, H.; Huang, S.-M.; et al. Contrasting Epidemiology and Clinicopathology of Female Breast Cancer in Asians vs the US Population. JNCI J. Natl. Cancer Inst. 2019, 111, 1298–1306. [Google Scholar] [CrossRef]
- Lee, S.K.; Kim, S.W.; Yu, J.H.; Lee, J.E.; Kim, J.Y.; Woo, J.; Lee, S.; Kim, E.K.; Moon, H.G.; Ko, S.S.; et al. Is the high proportion of young age at breast cancer onset a unique feature of Asian breast cancer? Breast Cancer Res. Treat. 2018, 173, 189–199. [Google Scholar] [CrossRef]
- Jones, M.E.; Schoemaker, M.J.; Wright, L.B.; Ashworth, A.; Swerdlow, A.J. Smoking and risk of breast cancer in the Generations Study cohort. Breast Cancer Res. 2017, 19, 118. [Google Scholar] [CrossRef]
- The Premenopausal Breast Cancer Collaborative Group; Schoemaker, M.J.; Nichols, H.B.; Wright, L.B.; Brook, M.N.; Jones, M.E.; O’Brien, K.M.; Adami, H.-O.; Baglietto, L.; Bernstein, L.; et al. Association of Body Mass Index and Age with Subsequent Breast Cancer Risk in Premenopausal Women. JAMA Oncol. 2018, 4, e181771. [Google Scholar] [CrossRef]
- Anderson, W.F.; Pfeiffer, R.M.; Wohlfahrt, J.; Ejlertsen, B.; Jensen, M.-B.; Kroman, N. Associations of parity-related reproductive histories with ER± and HER2± receptor-specific breast cancer aetiology. Int. J. Epidemiol. 2016, 46, 86–95. [Google Scholar] [CrossRef] [Green Version]
- The Cancer Genome Atlas (TCGA) Research Network. Comprehensive molecular portraits of human breast tumours. Nature 2012, 490, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Colaprico, A.; Silva, T.C.; Olsen, C.; Garofano, L.; Cava, C.; Garolini, D.; Sabedot, T.S.; Malta, T.M.; Pagnotta, S.M.; Castiglioni, I.; et al. TCGAbiolinks: An R/Bioconductor package for integrative analysis of TCGA data. Nucleic Acids Res. 2016, 44, e71. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Chen, Y.; Liu, Y.; Zhang, D.; Pan, J.; Long, M. Classification of PR-positive and PR-negative subtypes in ER-positive and HER2-negative breast cancers based on pathway scores. BMC Med. Res. Methodol. 2021, 21, 108. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Zhao, G.; Liu, Y.; Long, M. A Machine Learning Approach to Differentiate Two Specific Breast Cancer Subtypes Using Androgen Receptor Pathway Genes. Technol. Cancer Res. Treat. 2021, 20, 15330338211027900. [Google Scholar] [CrossRef]
- Long, M.; Hou, W.; Liu, Y.; Hu, T. A Histone Acetylation Modulator Gene Signature for Classification and Prognosis of Breast Cancer. Curr. Oncol. 2021, 28, 928–939. [Google Scholar] [CrossRef]
- Long, M.; Liu, H.; Wu, J.; Wang, S.; Liao, X.; Liu, Y.; Hu, T. Expression of DNA Helicase Genes Was Correlated with Homologous Recombination Deficiency in Breast Cancer. Comput. Math. Methods Med. 2022, 2022, 5508301. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.A.; Ferretti, V.; Grossman, R.L.; Staudt, L.M. The NCI Genomic Data Commons as an engine for precision medicine. Blood 2017, 130, 453–459. [Google Scholar] [CrossRef]
- Ritchie, M.E.; Phipson, P.; Wu, D.; Hu, Y.; Law, C.W.; Shi, W.; Smyth, G.K. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015, 43, e47. [Google Scholar] [CrossRef]
- Pereira, B.; Chin, S.-F.; Rueda, O.M.; Vollan, H.-K.M.; Provenzano, E.; Bardwell, H.A.; Pugh, M.; Jones, L.; Russell, R.; Sammut, S.-J.; et al. The somatic mutation profiles of 2433 breast cancers refine their genomic and transcriptomic landscapes. Nat. Commun. 2016, 7, 11479. [Google Scholar] [CrossRef]
- Rueda, O.M.; Sammut, S.-J.; Seoane, J.A.; Chin, S.-F.; Caswell-Jin, J.L.; Callari, M.; Batra, R.; Pereira, B.; Bruna, A.; Ali, H.R.; et al. Dynamics of breast-cancer relapse reveal late-recurring ER-positive genomic subgroups. Nature 2019, 567, 399–404. [Google Scholar] [CrossRef]
- Curtis, C.; Shah, S.P.; Chin, S.-F.; Turashvili, G.; Rueda, O.M.; Dunning, M.J.; Speed, D.; Lynch, A.G.; Samarajiwa, S.; Yuan, Y.; et al. The genomic and transcriptomic architecture of 2000 breast tumours reveals novel subgroups. Nature 2012, 486, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Yu, G.; He, Q.-Y. ReactomePA: An R/Bioconductor package for reactome pathway analysis and visualization. Mol. BioSyst. 2016, 12, 477–479. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | ER+/AR− (n = 21) | ER+/AR+ (n = 253) | p |
|---|---|---|---|
| Age | |||
| Mean (SD) | 52.2 (11.7) | 53.5 (11.4) | 0.603 |
| Grade | |||
| I | 1 (4.8) | 26 (10.3) | 0.062 |
| II | 16 (76.2) | 212 (83.8) | |
| III | 4 (19.0) | 15 (5.9) | |
| Histology | |||
| IDC-NST | 21 (100.0) | 243 (96.0) | 0.835 |
| Invasive lobular carcinoma | 0 (0) | 5 (2.0) | |
| Micropapillary carcinoma | 0 (0) | 3 (1.2) | |
| Mucinous carcinoma | 0 (0) | 2 (0.8) | |
| EGFR | |||
| Negative | 16 (76.2) | 210 (83.0) | 0.386 |
| Positive | 3 (14.3) | 16 (6.3) | |
| Unknown | 2 (9.5) | 27 (10.7) | |
| CK5/6 | |||
| Negative | 19 (90.5) | 246 (97.2) | 0.168 |
| Positive | 2 (9.5) | 6 (2.4) | |
| Unknown | 0 (0) | 1 (0.4) | |
| PR | |||
| Negative | 5 (23.8) | 15 (5.9) | 0.010 |
| Positive | 16 (76.2) | 238 (94.1) |
| Group | ER−/AR− (n = 26) | ER−/AR+ (n = 23) | p |
|---|---|---|---|
| Age | |||
| Mean (SD) | 49.1 (12.9) | 58.1 (12.9) | 0.019 |
| Grade | |||
| I | 0 (0) | 0 (0) | 0.016 |
| II | 5 (19.2) | 13 (56.5) | |
| III | 21 (80.8) | 10 (43.5) | |
| Histology | |||
| IDC | 26 (100.0) | 22 (95.7) | 0.951 |
| Apocrine Carcinoma | 0 (0) | 1 (4.3) | |
| EGFR | |||
| Negative | 3 (11.5) | 2 (8.7) | 0.943 |
| Positive | 21 (80.8) | 19 (82.6) | |
| Unknown | 2 (7.7) | 2 (8.7) | |
| Ki67 | |||
| Mean (SD) | 74.0 (12.0) | 55.4 (24.5) | 0.001 |
| CK5/6 | |||
| Negative | 6 (23.1) | 8 (34.8) | 0.556 |
| Positive | 20 (76.9) | 15 (65.2) | |
| PR | |||
| Negative | 26 (100.0) | 19 (82.6) | 0.090 |
| Positive | 0 (0) | 4 (17.4) |
| Name | TCGA | METABRIC | ||
|---|---|---|---|---|
| logFC | FDR | logFC | FDR | |
| AR | −1.817124266 | 2.48 × 10−51 | −1.759114522 | 0 |
| SEC14L2 | −1.456398856 | 4.22 × 10−18 | −1.064295136 | 1.51 × 10−45 |
| SCUBE2 | −1.247527072 | 6.05 × 10−8 | −1.160267382 | 2.79 × 10−22 |
| PIP | −2.242869262 | 2.14 × 10−7 | −1.359740461 | 2.97 × 10−13 |
| ANKRD30A | −2.441016285 | 5.80 × 10−7 | −1.406985552 | 6.46 × 10−18 |
| S100A9 | 1.105746351 | 3.28 × 10−5 | 1.042302941 | 1.32 × 10−16 |
| Name | TCGA | METABRIC | ||
|---|---|---|---|---|
| logFC | FDR | logFC | FDR | |
| AR | −4.295925031 | 1.45 × 10−27 | −1.901442266 | 5.66 × 10−50 |
| FOXA1 | −3.213843492 | 5.08 × 10−8 | −3.115137129 | 7.19 × 10−30 |
| NOSTRIN | −1.40887953 | 5.49 × 10−8 | −1.17526932 | 2.44 × 10−19 |
| HMGCS2 | −5.982850557 | 1.02 × 10−7 | −2.142998338 | 8.17 × 10−15 |
| ANKRD30A | −5.84612794 | 2.76 × 10−7 | −2.019088917 | 4.89 × 10−12 |
| GATA3 | −2.12904346 | 3.03 × 10−7 | −1.015513328 | 3.14 × 10−10 |
| MLPH | −2.443517722 | 4.28 × 10−7 | −2.48627378 | 8.21 × 10−22 |
| CYP4Z2P | −5.757726105 | 7.55 × 10−7 | −1.349071614 | 9.92 × 10−16 |
| RGMA | 1.523559476 | 7.55 × 10−7 | 1.044105908 | 3.13 × 10−11 |
| SCUBE2 | −2.061767467 | 1.15 × 10−6 | −1.067324511 | 6.66 × 10−14 |
| TFAP2B | −4.414408204 | 2.45 × 10−6 | −2.248879556 | 4.39 × 10−27 |
| PIP | −5.159250207 | 5.79 × 10−6 | −3.564551947 | 4.33 × 10−18 |
| SPDEF | −2.849330312 | 6.05 × 10−6 | −2.786823851 | 3.59 × 10−29 |
| GABRP | 3.309171931 | 7.85 × 10−6 | 3.2837105 | 2.69 × 10−20 |
| CYB5A | −1.146286537 | 8.90 × 10−6 | −1.38527235 | 4.09 × 10−16 |
| SFRP2 | −1.264969291 | 1.03 × 10−5 | −1.216259253 | 1.80 × 10−08 |
| CNTNAP2 | −2.963699101 | 1.30 × 10−5 | −1.31705986 | 1.65 × 10−10 |
| UGT2B11 | −5.754824596 | 1.63 × 10−5 | −2.499376453 | 5.35 × 10−13 |
| SLC40A1 | −1.57457122 | 1.66 × 10−5 | −1.096405114 | 2.81 × 10−12 |
| C1orf64 | −4.891014419 | 2.04 × 10−5 | −1.358795191 | 3.39 × 10−10 |
| ALCAM | −1.421797594 | 3.11 × 10−5 | −1.492164324 | 6.29 × 10−16 |
| REEP6 | −2.131080407 | 3.45 × 10−5 | −1.991369244 | 1.26 × 10−17 |
| C9orf152 | −2.474497544 | 3.89 × 10−5 | −2.048343549 | 1.17 × 10−19 |
| TFF3 | −3.56815467 | 6.54 × 10−5 | −3.132898878 | 1.12 × 10−19 |
| CAPN13 | −2.994917078 | 6.98 × 10−5 | −1.827529993 | 1.03 × 10−16 |
| ART3 | 3.077955742 | 9.58 × 10−5 | 2.120528214 | 2.32 × 10−14 |
| CLCA2 | −3.498079139 | 9.58 × 10−5 | −2.085823499 | 1.91 × 10−14 |
| ABCC11 | −2.825338538 | 9.66 × 10−5 | −1.680069132 | 4.05 × 10−13 |
| FZD9 | 1.975719541 | 9.73 × 10−5 | 1.396728979 | 1.02 × 10−15 |
| ACOX2 | −1.470170247 | 0.000111929 | −1.023673661 | 5.08 × 10−9 |
| ROPN1B | 2.719861187 | 0.000142 | 2.245409862 | 1.17 × 10−19 |
| SLC7A2 | −1.595639475 | 0.000225608 | −1.259892508 | 1.42 × 10−14 |
| SLC44A4 | −2.297987517 | 0.000261259 | −1.232436236 | 4.19 × 10−12 |
| SHC4 | 2.112277227 | 0.000286784 | 1.413138021 | 4.05 × 10−14 |
| SOX8 | 2.394006019 | 0.00030181 | 1.308657841 | 1.87 × 10−07 |
| LEMD1 | 2.268752567 | 0.000338694 | 1.336755062 | 8.27 × 10−17 |
| MIA | 3.004452058 | 0.000374416 | 1.152236253 | 2.45 × 10−10 |
| SPINK8 | −4.801533789 | 0.000377021 | −1.932031705 | 3.75 × 10−16 |
| HPGD | −2.052376193 | 0.000407842 | −1.087467101 | 1.56 × 10−06 |
| FOXC1 | 1.355691626 | 0.000455715 | 2.177507604 | 9.92 × 10−16 |
| LRRC26 | −3.185218295 | 0.000464176 | −2.393564467 | 8.31 × 10−20 |
| HRCT1 | 1.836318744 | 0.000547387 | 1.217364186 | 4.05 × 10−15 |
| SFRP1 | 1.703174242 | 0.000558313 | 1.892525614 | 6.54 × 10−12 |
| CYP4Z1 | −3.331023389 | 0.001049392 | −1.898760109 | 3.49 × 10−17 |
| SLC26A3 | −2.886229901 | 0.001135615 | −1.038268061 | 1.64 × 10−7 |
| CRAT | −1.081040223 | 0.001213952 | −1.095934205 | 1.82 × 10−15 |
| MFGE8 | 1.120102102 | 0.001318467 | 1.051062396 | 1.72 × 10−9 |
| CILP | −1.432888244 | 0.001543574 | −1.047884501 | 1.77 × 10−6 |
| THRSP | −2.306889406 | 0.001957621 | −1.202083641 | 5.36 × 10−9 |
| C2CD4B | −1.600907683 | 0.00275741 | −1.177058074 | 5.67 × 10−11 |
| CMBL | −1.157470421 | 0.003567629 | −1.417268369 | 2.20 × 10−13 |
| SCGB2A2 | −3.739630635 | 0.00390212 | −2.033977043 | 3.77 × 10−6 |
| VGLL1 | 2.55783435 | 0.003989974 | 1.665891121 | 5.86 × 10−14 |
| SFRP4 | −1.069605879 | 0.007015003 | −1.206349248 | 1.73 × 10−8 |
| KRT6B | 1.985907376 | 0.007554538 | 2.171033331 | 6.20 × 10−10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Long, M.; You, C.; Song, Q.; Hu, L.X.J.; Guo, Z.; Yao, Q.; Hou, W.; Sun, W.; Liang, B.; Zhou, X.; et al. AR Expression Correlates with Distinctive Clinicopathological and Genomic Features in Breast Cancer Regardless of ESR1 Expression Status. Int. J. Mol. Sci. 2022, 23, 11468. https://doi.org/10.3390/ijms231911468
Long M, You C, Song Q, Hu LXJ, Guo Z, Yao Q, Hou W, Sun W, Liang B, Zhou X, et al. AR Expression Correlates with Distinctive Clinicopathological and Genomic Features in Breast Cancer Regardless of ESR1 Expression Status. International Journal of Molecular Sciences. 2022; 23(19):11468. https://doi.org/10.3390/ijms231911468
Chicago/Turabian StyleLong, Mengping, Chong You, Qianqian Song, Lina X. J. Hu, Zhaorong Guo, Qian Yao, Wei Hou, Wei Sun, Baosheng Liang, Xiaohua Zhou, and et al. 2022. "AR Expression Correlates with Distinctive Clinicopathological and Genomic Features in Breast Cancer Regardless of ESR1 Expression Status" International Journal of Molecular Sciences 23, no. 19: 11468. https://doi.org/10.3390/ijms231911468
APA StyleLong, M., You, C., Song, Q., Hu, L. X. J., Guo, Z., Yao, Q., Hou, W., Sun, W., Liang, B., Zhou, X., Liu, Y., & Hu, T. (2022). AR Expression Correlates with Distinctive Clinicopathological and Genomic Features in Breast Cancer Regardless of ESR1 Expression Status. International Journal of Molecular Sciences, 23(19), 11468. https://doi.org/10.3390/ijms231911468