
Intracavernous Injection of Platelet-Rich Plasma Therapy Enhances Erectile Function and Decreases the Mortality Rate in Streptozotocin-Induced Diabetic Rats

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Changes in Body Weight and Blood Glucose Level
2.2. PRP Treatment Decreases the Mortality Rate
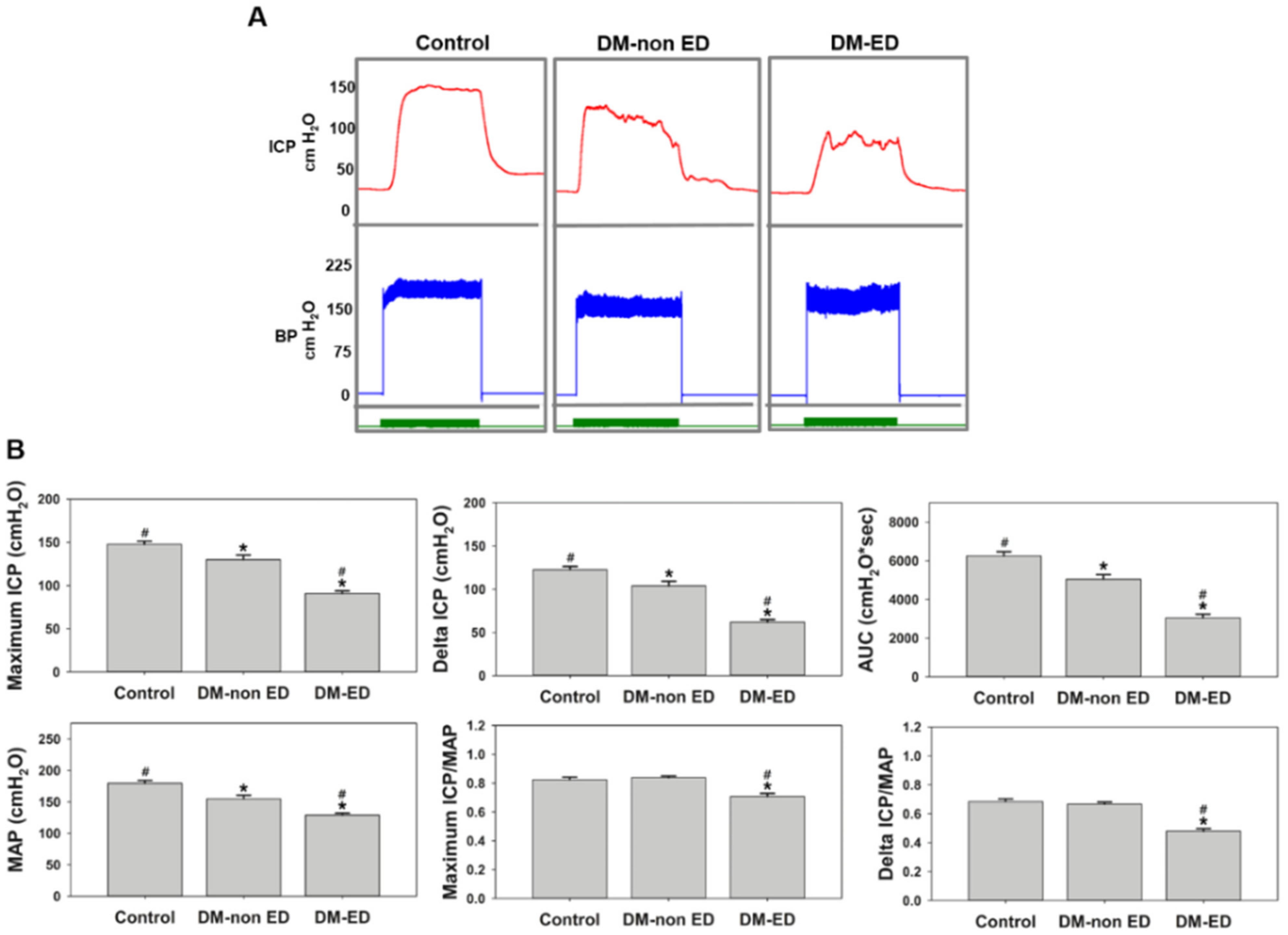
2.3. ICP Measurements after 12 Weeks of STZ Induction
2.4. ICP Changes Due to Different Treatments
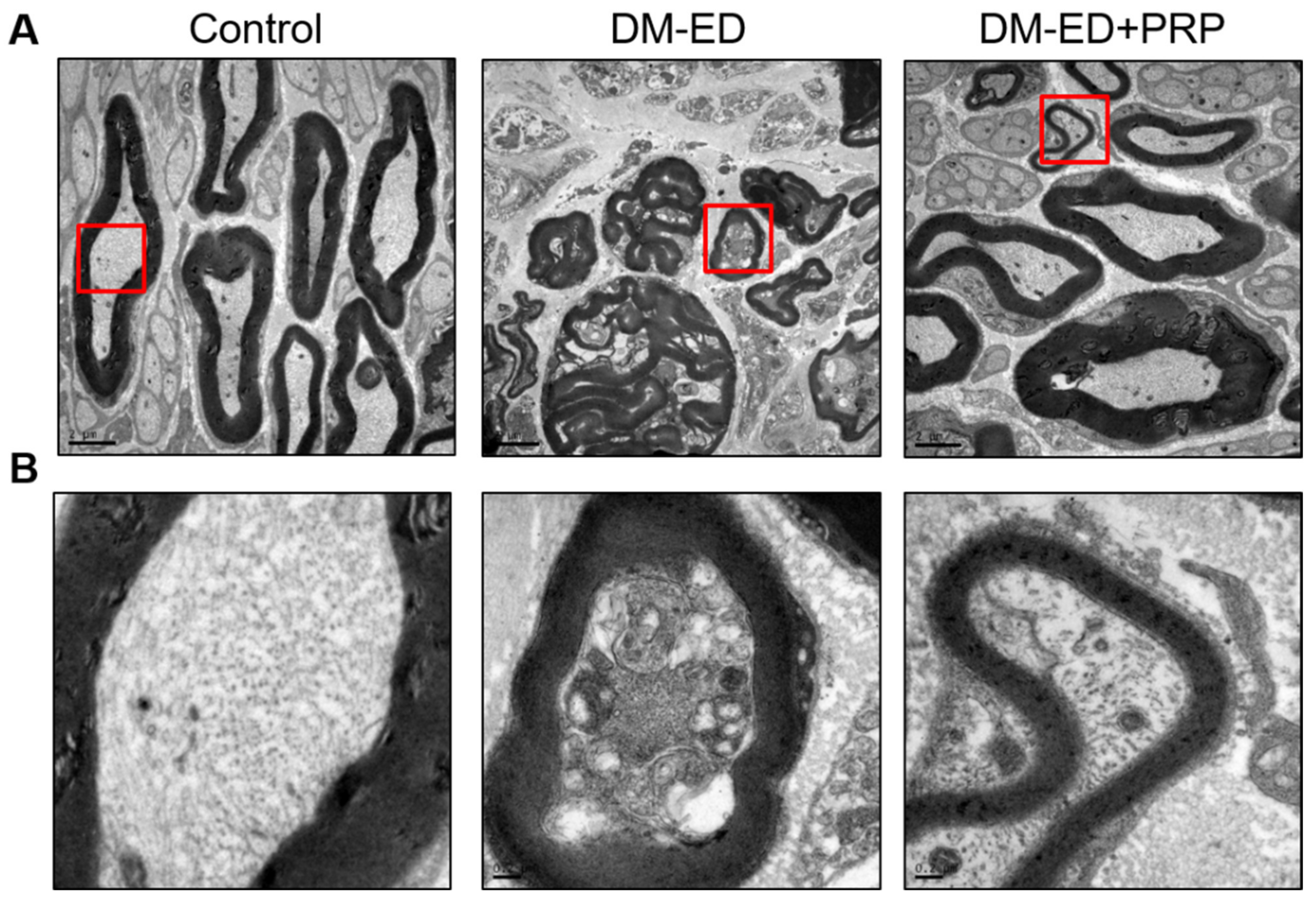
2.5. PRP Treatment Restored the Damaged Corpus Cavernosum
2.6. PRP Treatment Reversed Nerve Damage
3. Discussion
4. Materials and Methods
4.1. Experimental Animal
4.2. Experimental Design
4.3. PRP Preparation
4.4. Assessment of Erectile Function
4.5. Surgical Procedures
4.6. Histology and Immunofluorescence Staining
4.7. Transmission Electron Microscopy (TEM)
4.8. Statistical Analysis
5. Novelty and Application Potentials of PRP in DM-ED
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, F.; Hui, Y.; Xin, H.; Xu, Y.D.; Lei, H.E.; Yang, B.C.; Guan, R.L.; Li, M.; Hou, J.Q.; Xin, Z.C. Therapeutic effects of adipose-derived stem cells-based microtissues on erectile dysfunction in streptozotocin-induced diabetic rats. Asian J. Androl. 2017, 19, 91. [Google Scholar] [PubMed]
- Hafez, E.S.E.; Hafez, S.D. Erectile dysfunction: Anatomical parameters, etiology, diagnosis, and therapy. Arch. Androl. 2005, 51, 15–31. [Google Scholar] [CrossRef] [PubMed]
- Schauer, I.; Keller, E.; Müller, A.; Madersbacher, S. Have rates of erectile dysfunction improved within the past 17 years after radical prostatectomy? A systematic analysis of the control arms of prospective randomized trials on penile rehabilitation. Andrology 2015, 3, 661–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Defeudis, G.; Gianfrilli, D.; Di Emidio, C.; Pofi, R.; Tuccinardi, D.; Palermo, A.; Lenzi, A.; Pozzilli, P. Erectile dysfunction and its management in patients with diabetes mellitus. Rev. Endocr. Metab. Disord. 2015, 16, 213–231. [Google Scholar] [CrossRef]
- Papazafiropoulou, A.K.; Anagnostopoulou, K.; Petropoulou, K.; Melidonis, A. Prevalence of erectile dysfunction among Greek men with type 2 diabetes mellitus. Ann. Afr. Med. 2020, 19, 73. [Google Scholar] [CrossRef]
- Várkonyi, T.; Kempler, P. Sexual dysfunction in diabetes. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2014; Volume 126, pp. 223–232. [Google Scholar]
- Kouidrat, Y.; Pizzol, D.; Cosco, T.; Thompson, T.; Carnaghi, M.; Bertoldo, A.; Solmi, M.; Stubbs, B.; Veronese, N. High prevalence of erectile dysfunction in diabetes: A systematic review and meta-analysis of 145 studies. Diabet. Med. 2017, 34, 1185–1192. [Google Scholar] [CrossRef]
- Hatzimouratidis, K.; Hatzichristou, D. How to treat erectile dysfunction in men with diabetes: From pathophysiology to treatment. Curr. Diabetes Rep. 2014, 14, 545. [Google Scholar] [CrossRef]
- Thorve, V.S.; Kshirsagar, A.D.; Vyawahare, N.S.; Joshi, V.S.; Ingale, K.G.; Mohite, R.J. Diabetes-induced erectile dysfunction: Epidemiology, pathophysiology and management. J. Diabetes Its Complicat. 2011, 25, 129–136. [Google Scholar] [CrossRef]
- Derosa, G.; Romano, D.; Tinelli, C.; D’Angelo, A.; Maffioli, P. Prevalence and associations of erectile dysfunction in a sample of Italian males with type 2 diabetes. Diabetes Res. Clin. Pract. 2015, 108, 329–335. [Google Scholar] [CrossRef]
- Maiorino, M.I.; Bellastella, G.; Giugliano, D.; Esposito, K. From inflammation to sexual dysfunctions: A journey through diabetes, obesity, and metabolic syndrome. J. Endocrinol. Investig. 2018, 41, 1249–1258. [Google Scholar] [CrossRef]
- Gazzaruso, C. Erectile dysfunction and coronary atherothrombosis in diabetic patients: Pathophysiology, clinical features and treatment. Expert Rev. Cardiovasc. Ther. 2006, 4, 173–180. [Google Scholar] [CrossRef]
- Yu, X.D.; Wang, J.S.; Zuo, G.; Wang, X.; Ge, F.; Wu, S.; Lim, J.; Shang, J.; Zhang, Y. Traditional Chinese medicine on treating diabetic mellitus erectile dysfunction: Protocol for a systematic review and meta-analysis. Medicine 2019, 98, e14928. [Google Scholar] [CrossRef]
- Wang, J.; Mi, Y.; Wu, S.; You, X.; Huang, Y.; Zhu, J.; Zhu, L. Exosomes from adipose-derived stem cells protect against high glucose-induced erectile dysfunction by delivery of corin in a streptozotocin-induced diabetic rat model. Regen. Ther. 2020, 14, 227–233. [Google Scholar] [CrossRef]
- Malavige, L.S.; Levy, J.C. Erectile dysfunction in diabetes mellitus. J. Sex. Med. 2009, 6, 1232–1247. [Google Scholar] [CrossRef]
- Mehrabani, D.; Seghatchian, J.; Acker, J.P. Platelet rich plasma in treatment of musculoskeletal pathologies. Transfus. Apher. Sci. 2019, 58, 102675. [Google Scholar] [CrossRef]
- Mercuri, S.R.; Vollono, L.; Paolino, G. The Usefulness of Platelet-Rich Plasma (PRP) for the Treatment of Vitiligo: State of the Art and Review. Drug Des. Dev. Ther. 2020, 14, 1749–1755. [Google Scholar] [CrossRef]
- Marx, R.E.; Carlson, E.R.; Eichstaedt, R.M.; Schimmele, S.R.; Strauss, J.E.; Georgeff, K.R. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1998, 85, 638–646. [Google Scholar] [CrossRef]
- Luzo, A.C.M.; Fávaro, W.J.; Seabra, A.B.; Durán, N. What is the potential use of platelet-rich-plasma (PRP) in cancer treatment? A mini-review. Heliyon 2020, 6, e03660. [Google Scholar] [CrossRef]
- Elghblawi, E. Platelet-rich plasma, the ultimate secret for youthful skin elixir and hair growth triggering. J. Cosmet. Dermatol. 2018, 17, 423–430. [Google Scholar] [CrossRef]
- Wu, C.C.; Wu, Y.N.; Ho, H.O.; Chen, K.C.; Sheu, M.T.; Chiang, H.S. The neuroprotective effect of platelet-rich plasma on erectile function in bilateral cavernous nerve injury rat model. J. Sex. Med. 2012, 9, 2838–2848. [Google Scholar] [CrossRef]
- Wu, Y.N.; Wu, C.C.; Sheu, M.T.; Chen, K.C.; Ho, H.O.; Chiang, H.S. Optimization of platelet-rich plasma and its effects on the recovery of erectile function after bilateral cavernous nerve injury in a rat model. J. Tissue Eng. Regen. Med. 2016, 10, E294–E304. [Google Scholar] [CrossRef]
- Mirzaei, M.; Daneshpajooh, A.; Farsinezhad, A.; Jafarian, Z.; Ebadzadeh, M.R.; Saberi, N.; Teimorian, M. The therapeutic effect of intravesical instillation of platelet rich plasma on recurrent bacterial cystitis in women: A randomized clinical trial. Urol. J. 2019, 16, 609–613. [Google Scholar]
- Gajdosík, A.; Gajdosíková, A.; Stefek, M.; Navarová, J.; Hozová, R. Streptozotocin-induced experimental diabetes in male Wistar rats. Gen. Physiol. Biophys. 1999, 18, 54–62. [Google Scholar]
- Yang, R.H.; Qi, S.H.; Shu, B.; Ruan, S.B.; Lin, Z.P.; Lin, Y.; Shen, R.; Zhang, F.G.; Chen, X.D.; Xie, J.L. Epidermal stem cells (ESCs) accelerate diabetic wound healing via the Notch signalling pathway. Biosci. Rep. 2016, 36, e00364. [Google Scholar] [CrossRef] [Green Version]
- Motyl, K.; Mc Cabe, L.R. Streptozotocin, type I diabetes severity and bone. Biol. Proced. Online 2009, 11, 296–315. [Google Scholar] [CrossRef] [Green Version]
- Zafar, M.; Naeem-ul-Hassan Naqvi, S.; Ahmed, M.; Kaimkhani, Z.A. Altered kidney morphology and enzymes in streptozotocin induced diabetic rats. Int. J. Morphol. 2009, 27, 783–790. [Google Scholar] [CrossRef] [Green Version]
- Goyal, S.N.; Reddy, N.M.; Patil, K.R.; Nakhate, K.T.; Ojha, S.; Patil, C.R.; Agrawal, Y.O. Challenges and issues with streptozotocin-induced diabetes—A clinically relevant animal model to understand the diabetes pathogenesis and evaluate therapeutics. Chem.-Biol. Interact. 2016, 244, 49–63. [Google Scholar] [CrossRef]
- Ren, J.; Yang, M.; Xu, F.; Chen, J.; Ma, S. Acceleration of wound healing activity with syringic acid in streptozotocin induced diabetic rats. Life Sci. 2019, 233, 116728. [Google Scholar] [CrossRef]
- Eleazu, C.O.; Eleazu, K.C.; Chukwuma, S.; Essien, U.N. Review of the mechanism of cell death resulting from streptozotocin challenge in experimental animals, its practical use and potential risk to humans. J. Diabetes Metab. Disord. 2013, 12, 60. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.J.; Xie, X.S.; Feng, S.G.; Long, Q.X.; Ai, N.; Wang, B.F. Causes of death in STZ-induced rat models of diabetes mellitus. Sichuan Da Xue Xue Bao. Yi Xue Ban = J. Sichuan Univ. Med. Sci. Ed. 2014, 45, 691–695. [Google Scholar]
- Nørgaard, S.A.; Sand, F.W.; Sørensen, D.B.; Abelson, K.S.; Søndergaard, H. Softened food reduces weight loss in the streptozotocin-induced male mouse model of diabetic nephropathy. Lab. Anim. 2018, 52, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Schein, P.S.; Loftus, S. Streptozotocin: Depression of mouse liver pyridine nucleotides. Cancer Res. 1968, 28, 1501–1506. [Google Scholar] [PubMed]
- Jeon, S.H.; Zhu, G.Q.; Bae, W.J.; Choi, S.W.; Jeong, H.C.; Cho, H.J.; Ha, U.; Hong, S.H.; Lee, J.Y.; Kwon, E.B.; et al. Engineered mesenchymal stem cells expressing stromal cell-derived factor-1 improve erectile dysfunction in streptozotocin-induced diabetic rats. Int. J. Mol. Sci. 2018, 19, 3730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, M.; Horio, T.; Kishimoto, S.; Nakamura, S.; Takikawa, M.; Nakayama, T.; Yamamoto, Y.; Shimizu, M.; Hattori, H.; Tachibana, S.; et al. Effects of platelet-rich plasma-containing fragmin/protamine microparticles in enhancing endothelial and smooth muscle cell growth and inducing collateral vessels in a rabbit model of hindlimb ischemia. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.; Banie, L.; Ning, H.; Bella, A.J.; Lin, C.S.; Lue, T.F. Potential of adipose-derived stem cells for treatment of erectile dysfunction. J. Sex. Med. 2009, 6 (Suppl. 3), 320–327. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.N.; Chen, K.C.; Liao, C.H.; Liu, C.L.; Chiang, H.S. Smooth muscle progenitor cells preserve the erectile function by reducing corporal smooth muscle cell apoptosis after bilateral cavernous nerve crush injury in rats. BioMed Res. Int. 2019, 2019, 8520523. [Google Scholar] [CrossRef]
- Asahara, T.; Murohara, T.; Sullivan, A.; Silver, M.; van der Zee, R.; Li, T.; Witzenbichler, B.; Schatteman, G.; Isner, J. MIsolation of putative progenitor endothelial cells for angiogenesis. Science 1997, 275, 964–967. [Google Scholar] [CrossRef]
- Cho, M.C.; Park, K.; Chai, J.S.; Lee, S.H.; Kim, S.W.; Paick, J.S. Involvement of sphingosine-1-phosphate/RhoA/Rho-kinase signaling pathway in corporal fibrosis following cavernous nerve injury in male rats. J. Sex. Med. 2011, 8, 712–721. [Google Scholar] [CrossRef]
- Facio, F.N., Jr.; Burnett, A.L. Protective effect of annexin-A1 against irreversible damage to cavernous tissue after cavernous nerve injury in the rat. BJU Int. 2012, 110, 1346–1351. [Google Scholar] [CrossRef]
- Bakircioglu, M.E.; Sievert, K.D.; Nunes, L.; Lau, A.; Lin, C.S.; Lue, T.F. Decreased trabecular smooth muscle and caveolin-1 expression in the penile tissue of aged rats. J. Urol. 2001, 166, 734–738. [Google Scholar] [CrossRef]
- Böck, P.; Gorgas, K. Morphology and histochemistry of helicine arteries in the corpora cavernosa penis of mice. Arch. Histol. Jpn. 1977, 40, 265–281. [Google Scholar] [CrossRef] [Green Version]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, C.-H.; Lee, K.-H.; Chung, S.-D.; Chen, K.-C.; Praveen Rajneesh, C.; Chen, B.-H.; Cheng, J.-H.; Lin, W.-Y.; Chiang, H.-S.; Wu, Y.-N. Intracavernous Injection of Platelet-Rich Plasma Therapy Enhances Erectile Function and Decreases the Mortality Rate in Streptozotocin-Induced Diabetic Rats. Int. J. Mol. Sci. 2022, 23, 3017. https://doi.org/10.3390/ijms23063017
Liao C-H, Lee K-H, Chung S-D, Chen K-C, Praveen Rajneesh C, Chen B-H, Cheng J-H, Lin W-Y, Chiang H-S, Wu Y-N. Intracavernous Injection of Platelet-Rich Plasma Therapy Enhances Erectile Function and Decreases the Mortality Rate in Streptozotocin-Induced Diabetic Rats. International Journal of Molecular Sciences. 2022; 23(6):3017. https://doi.org/10.3390/ijms23063017
Chicago/Turabian StyleLiao, Chun-Hou, Kau-Han Lee, Shiu-Dong Chung, Kuo-Chiang Chen, Chellappan Praveen Rajneesh, Bo-He Chen, Jai-Hong Cheng, Wang-Ying Lin, Han-Sun Chiang, and Yi-No Wu. 2022. "Intracavernous Injection of Platelet-Rich Plasma Therapy Enhances Erectile Function and Decreases the Mortality Rate in Streptozotocin-Induced Diabetic Rats" International Journal of Molecular Sciences 23, no. 6: 3017. https://doi.org/10.3390/ijms23063017