
Analysis of Serum Advanced Glycation Endproducts Reveals Methylglyoxal-Derived Advanced Glycation MG-H1 Free Adduct Is a Risk Marker in Non-Diabetic and Diabetic Chronic Kidney Disease

 , , , , , ,
, , , , , , 
Abstract
1. Introduction
2. Results
2.1. Subject Characteristics
2.2. Serum Protein-Bound AGEs
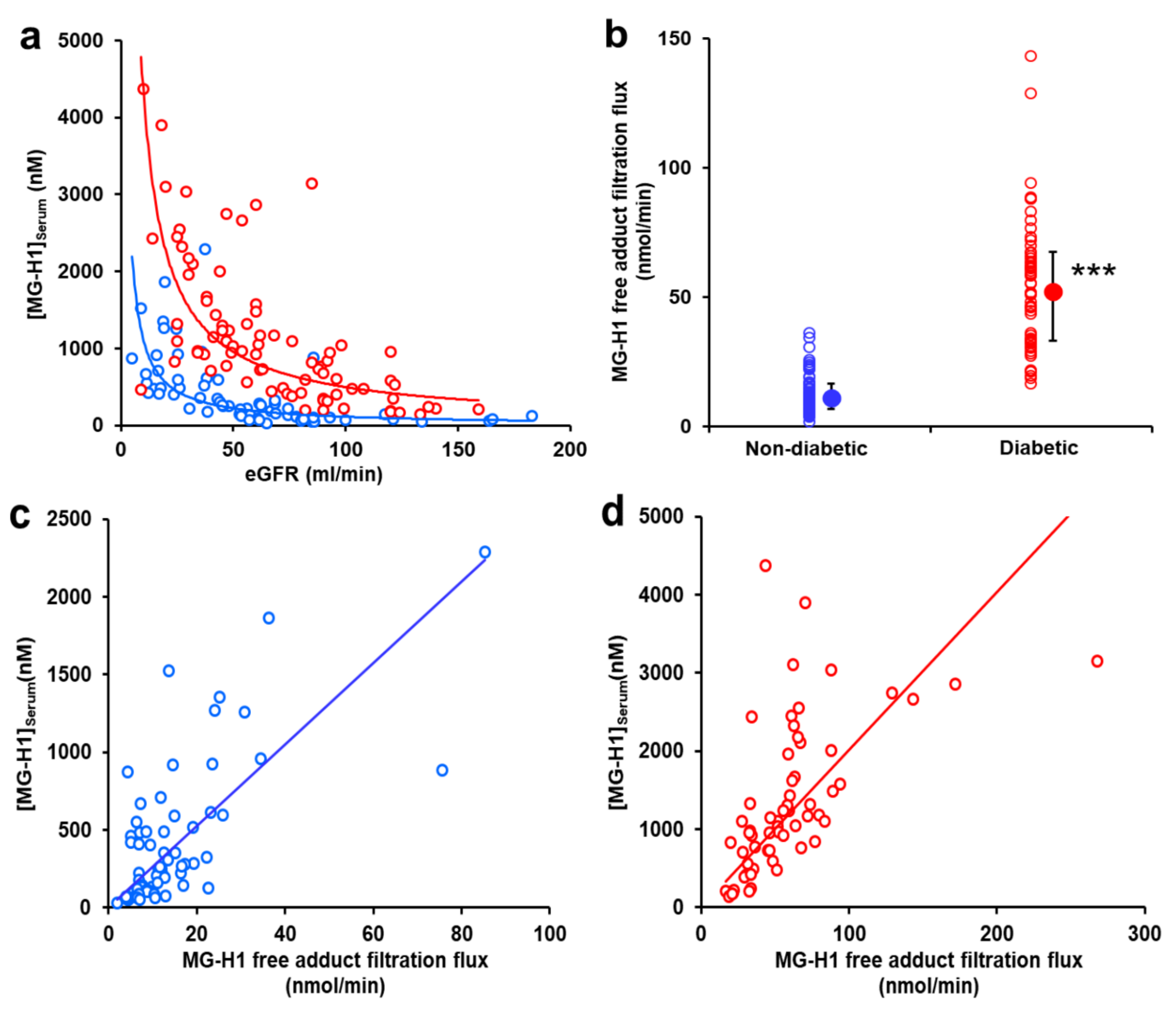
2.3. Serum AGE Free Adducts
2.4. AGE Free Adduct Glomerular Filtration Flux
3. Discussion
4. Materials and Methods
4.1. Patients and Study Design
4.2. Analysis of Serum Protein-Bound AGEs and AGE Free Adducts
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rabbani, N.; Thornalley, P.J. Advanced glycation end products in the pathogenesis of chronic kidney disease. Kidney Int. 2018, 93, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, N.; Thornalley, P.J. Protein glycation—Biomarkers of metabolic dysfunction and early-stage decline in health in the era of precision medicine. Redox Biol. 2021, 42, 101920. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Babaei-Jadidi, R.; Howell, S.K.; Beisswenger, P.J.; Thornalley, P.J. Degradation products of proteins damaged by glycation, oxidation and nitration in clinical type 1 diabetes. Diabetologia 2005, 48, 1590–1603. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.U.; Thorpe, S.R.; Baynes, J.W. Identification of Nε-carboxymethyl-lysine as a degradation product of fructoselysine in glycated protein. J. Biol. Chem. 1986, 261, 4889–4894. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Dobler, D.; Dean, M.; Thornalley, P.J. Peptide mapping identifies hotspot site of modification in human serum albumin by methylglyoxal involved in ligand binding and esterase activity. J. Biol. Chem. 2005, 280, 5724–5732. [Google Scholar] [CrossRef]
- Sell, D.R.; Monnier, V.M. Structure elucidation of a senescence crosslink from human extracellular matrix. Implication of pentoses in the aging process. J. Biol. Chem. 1989, 264, 21597–21602. [Google Scholar] [CrossRef]
- Wang, F.; Zhao, Y.; Niu, Y.; Wang, C.; Wang, M.; Li, Y.; Sun, C. Activated glucose-6-phosphate dehydrogenase is associated with insulin resistance by upregulating pentose and pentosidine in diet-induced obesity of rats. Horm. Metab. Res. 2012, 44, 938–942. [Google Scholar] [CrossRef]
- Masania, J.; Faustmann, G.; Anwar, A.; Hafner-Giessauf, H.; Rajpoot, R.; Grabher, J.; Rajpoot, K.; Tiran, B.; Obermayer-Pietsch, B.; Winklhofer-Roob, B.M.; et al. Urinary metabolomic markers of protein glycation, oxidation and nitration in early-stage decline in metabolic, vascular and renal health. Oxidative Med. Cell Longev. 2019, 2019, 4851323. [Google Scholar] [CrossRef]
- Hanssen, N.M.J.; Beulens, J.W.J.; van Dieren, S.; Scheijen, J.L.J.M.; van der A, D.L.; Spijkerman, A.M.W.; van der Schouw, Y.T.; Stehouwer, C.D.A.; Schalkwijk, C.G. Plasma advanced glycation endproducts are associated with incident cardiovascular events in individuals with type 2 diabetes: A case-cohort study with a median follow-up of 10 years (EPIC-NL). Diabetes 2014, 64, 257–265. [Google Scholar] [CrossRef]
- Monnier, V.M.; Sell, D.R.; Gao, X.; Genuth, S.M.; Lachin, J.M.; Bebu, I. Plasma advanced glycation end products and the subsequent risk of microvascular complications in type 1 diabetes in the DCCT/EDIC. BMJ Open Diabetes Res. Care 2022, 10, e002667. [Google Scholar] [CrossRef]
- Rabbani, N.; Adaikalakoteswari, A.; Rossing, K.; Rossing, P.; Tarnow, L.; Parving, H.-H.; Thornalley, P.J. Effect of Irbesartan treatment on plasma and urinary markers of protein damage in patients with type 2 diabetes and microalbuminuria. Amino Acids 2012, 42, 1627–1639. [Google Scholar] [CrossRef]
- Coughlan, M.T.; Patel, S.K.; Jerums, G.; Penfold, S.A.; Nguyen, T.V.; Sourris, K.C.; Panagiotopoulos, S.; Srivastava, P.M.; Cooper, M.E.; Burrell, L.M.; et al. Advanced glycation urinary protein-bound biomarkers and severity of diabetic nephropathy in man. Am. J. Nephrol. 2011, 34, 347–355. [Google Scholar] [CrossRef]
- Foerster, A.; Henle, T. Glycation in food and metabolic transit of dietary AGEs (advanced glycation end-products): Studies on the urinary excretion of pyrraline. Biochem. Soc. Trans. 2003, 31, 1383–1385. [Google Scholar] [CrossRef]
- Xue, M.; Weickert, M.O.; Qureshi, S.; Ngianga-Bakwin, K.; Anwar, A.; Waldron, M.; Shafie, A.; Messenger, D.; Fowler, M.; Jenkins, G.; et al. Improved glycemic control and vascular function in overweight and obese subjects by glyoxalase 1 inducer formulation. Diabetes 2016, 65, 2282–2294. [Google Scholar] [CrossRef]
- Agalou, S.; Ahmed, N.; Babaei-Jadidi, R.; Dawnay, A.; Thornalley, P.J. Profound mishandling of protein glycation degradation products in uremia and dialysis. J. Amer. Soc. Nephrol. 2005, 16, 1471–1485. [Google Scholar] [CrossRef]
- Thornalley, P.J.; Battah, S.; Ahmed, N.; Karachalias, N.; Agalou, S.; Babaei-Jadidi, R.; Dawnay, A. Quantitative screening of advanced glycation endproducts in cellular and extracellular proteins by tandem mass spectrometry. Biochem. J. 2003, 375, 581–592. [Google Scholar] [CrossRef]
- Rabbani, N.; Sebekova, K.; Sebekova, K., Jr.; Heidland, A.; Thornalley, P.J. Protein glycation, oxidation and nitration free adduct accumulation after bilateral nephrectomy and ureteral ligation. Kidney Internat. 2007, 72, 1113–1121. [Google Scholar] [CrossRef]
- Beisswenger, P.J.; Howell, S.K.; Touchette, A.; Lal, S.; Szwergold, B.S. Metformin reduces systemic methylglyoxal levels in type 2 diabetes. Diabetes 1999, 48, 198–202. [Google Scholar] [CrossRef]
- Nicolay, J.P.; Schneider, J.; Niemoeller, O.M.; Artunc, F.; Portero-Otin, M.; Haik, G.; Thornalley, P.J.; Schleicher, E.; Wieder, T.; Lang, F. Stimulation of suicidal erythrocyte death by methylglyoxal. Cell Physiol. Biochem. 2006, 18, 223–232. [Google Scholar] [CrossRef]
- Agalou, S.; Karachalias, N.; Tucker, B.; Thornalley, P.J.; Dawnay, A. Estimation of α-oxoaldehydes formed from the degradation of glycolytic intermediates and glucose fragmentation in blood plasma of human subjects with uraemia. Internat. Congr. Ser. 2002, 1245, 182. [Google Scholar] [CrossRef]
- Niwa, T.; Takeda, N.; Yoshizumi, H.; Takematsu, A.; Ohara, M.; Tomiyama, S.; Niimura, K. Presence of 3-deoxyglucosone, a potent protein crosslinking intermediate of the Maillard reaction, in diabetic serum. Biochem. Biophys. Res. Com. 1993, 196, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Niwa, T.; Takeda, N.; Yoshizumi, H.; Tatematsu, A.; Maeda, K.; Ohara, M.; Tomiyama, S.; Niimura, K. Elevated serum levels of 3-deoxyglucosone, a potent protein crosslinking intermediate of the Maillard reaction, in uremic patients. Nephron 1995, 69, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Tessari, P.; Kiwanuka, E.; Barazzoni, R.; Vettore, M.; Zanetti, M. Diabetic nephropathy is associated with increased albumin and fibrinogen production in patients with type 2 diabetes. Diabetologia 2006, 49, 1955–1961. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Karachalias, N.; Babaei-Jadidi, R.; Rabbani, N.; Thornalley, P.J. Increased protein damage in renal glomeruli, retina, nerve, plasma and urine and its prevention by thiamine and benfotiamine therapy in a rat model of diabetes. Diabetologia 2010, 53, 1506–1516. [Google Scholar] [CrossRef] [PubMed]
- Iliadis, F.; Didangelos, T.; Ntemka, A.; Makedou, A.; Moralidis, E.; Gotzamani-Psarakou, A.; Kouloukourgiotou, T.; Grekas, D. Glomerular filtration rate estimation in patients with type 2 diabetes: Creatinine- or cystatin C-based equations? Diabetologia 2011, 54, 2987–2994. [Google Scholar] [CrossRef]
- Rabbani, N.; Xue, M.; Thornalley, P.J. Methylglyoxal-induced dicarbonyl stress in aging and disease: First steps towards glyoxalase 1-based treatments. Clin. Sci. 2016, 130, 1677–1696. [Google Scholar] [CrossRef]
- Snelson, M.; Tan, S.M.; Clarke, R.E.; de Pasquale, C.; Thallas-Bonke, V.; Nguyen, T.-V.; Penfold, S.A.; Harcourt, B.E.; Sourris, K.C.; Lindblom, R.S.; et al. Processed foods drive intestinal barrier permeability and microvascular diseases. Sci. Adv. 2021, 7, eabe4841. [Google Scholar] [CrossRef]
- Xue, M.; Rabbani, N.; Thornalley, P.J. Glyoxalase in ageing. Semin. Cell Dev. Biol. 2011, 22, 293–301. [Google Scholar] [CrossRef]
- Eloot, S.; Schepers, E.; Barreto, D.V.; Barreto, F.C.; Liabeuf, S.; Van Biesen, W.; Verbeke, F.; Glorieux, G.; Choukroun, G.; Massy, Z.; et al. Estimated Glomerular Filtration Rate Is a Poor Predictor of Concentration for a Broad Range of Uremic Toxins. Clin. J. Am. Soc. Nephrol. 2011, 6, 1266–1273. [Google Scholar] [CrossRef]
- Perkins, B.A.; Rabbani, N.; Weston, A.; Adaikalakoteswari, A.; Lee, J.A.; Lovblom, L.E.; Cardinez, N.; Thornalley, P.J. High fractional excretion of glycation adducts is associated with subsequent early decline in renal function in type 1 diabetes. Sci. Rep. 2020, 10, 12709. [Google Scholar]
- Chambers, J.C.; Zhang, W.; Lord, G.M.; van der Harst, P.; Lawlor, D.A.; Sehmi, J.S.; Gale, D.P.; Wass, M.N.; Ahmadi, K.R.; Bakker, S.J.L.; et al. Genetic loci influencing kidney function and chronic kidney disease. Nat. Genet. 2010, 42, 373–375. [Google Scholar] [CrossRef]
- Chasman, D.I.; Fuchsberger, C.; Pattaro, C.; Teumer, A.; Böger, C.A.; Endlich, K.; Olden, M.; Chen, M.-H.; Tin, A.; Taliun, D.; et al. Integration of genome-wide association studies with biological knowledge identifies six novel genes related to kidney function. Hum. Mol. Genet. 2012, 21, 5329–5343. [Google Scholar] [CrossRef]
- Fu, M.X.; Requena, J.R.; Jenkins, A.J.; Lyons, T.J.; Baynes, J.W.; Thorpe, S.R. The advanced glycation end product, Nε-(carboxymethyl)lysine, is a product of both lipid peroxidation and glycoxidation reactions. J. Biol. Chem. 1996, 271, 9982–9986. [Google Scholar] [CrossRef] [PubMed]
- Castell, M.V.; van der Pas, S.; Otero, A.; Siviero, P.; Dennison, E.; Denkinger, M.; Pedersen, N.; Sanchez-Martinez, M.; Queipo, R.; van Schoor, N.; et al. Osteoarthritis and frailty in elderly individuals across six European countries: Results from the European Project on OSteoArthritis (EPOSA). BMC Musculoskelet. Disord. 2015, 16, 359. [Google Scholar] [CrossRef]
- Ahmed, U.; Anwar, A.; Savage, R.S.; Thornalley, P.J.; Rabbani, N. Protein oxidation, nitration and glycation biomarkers for early-stage diagnosis of osteoarthritis of the knee and typing and progression of arthritic disease. Arthritis Res. Ther. 2016, 18, 250. [Google Scholar] [CrossRef]
- American-Diabetes-Association, STANDARDS OF CARE. 11. Chronic Kidney Disease and Risk Management: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45 (Suppl. 1), S175–S184. [Google Scholar] [CrossRef]
- MacIsaac, R.J.; Tsalamandris, C.; Panagiotopoulos, S.; Smith, T.J.; McNeil, K.J.; Jerums, G. Nonalbuminuric renal insufficiency in type 2 diabetes. Diabetes Care 2004, 27, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Penno, G.; Solini, A.; Bonora, E.; Fondelli, C.; Orsi, E.; Zerbini, G.; Trevisan, R.; Vedovato, M.; Gruden, G.; Cavalot, F.; et al. Clinical significance of nonalbuminuric renal impairment in type 2 diabetes. J. Hypertens. 2011, 29, 1802–1809. [Google Scholar] [CrossRef]
- Premaratne, E.; Macisaac, R.J.; Tsalamandris, C.; Panagiotopoulos, S.; Smith, T.; Jerums, G. Renal hyperfiltration in type 2 diabetes: Effect of age-related decline in glomerular filtration rate. Diabetologia 2005, 48, 2486–2493. [Google Scholar] [CrossRef]
- Rabbani, N.; Shaheen, F.; Anwar, A.; Masania, J.; Thornalley, P.J. Assay of methylglyoxal-derived protein and nucleotide AGEs. Biochem. Soc. Trans. 2014, 42, 511–517. [Google Scholar] [CrossRef]
- Rabbani, N.; Thornalley, P.J. Reading patterns of proteome damage by glycation, oxidation and nitration: Quantitation by stable isotopic dilution analysis LC-MS/MS. Essays Biochem. 2020, 64, 169–183. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CKD Stage | Diabetes Status | Normal | 2 | 3 | 4 | p-Value |
|---|---|---|---|---|---|---|
| Number of subjects | No | 12 | 20 | 16 | 25 | |
| Yes | 7 | 15 | 29 | 11 | ||
| Age (years) | No | 67 ± 17 | 72 ± 13 | 80 ± 11 * | 76 ± 14 | |
| Yes | 43 ± 11 OO | 65 ± 9 *** | 74 ± 11 *** | 76 ± 15 *** | <0.001 | |
| Gender (M/F) | No | 4/8 | 6/14 | 12/4 | 20/5 | |
| Yes | 0/7 | 13/2 | 17/12 | 7/4 | ||
| Diabetes type (N for types 1 and 2) | Yes | 3,4 | 0,15 | 3,26 | 0,11 | |
| Duration of diabetes (years) | Yes | 13 ± 9 | 16 ± 8 | 20 ± 12 | 18 ± 9 | |
| A1C (%) | Yes | 7.9 ± 1.0 | 7.6 ± 0.8 | 7.9 ± 1.3 | 8.2 ± 1.3 | |
| eGFR (ml/min) | No | 130 ± 41 | 73 ± 11 ** | 49 ± 14 *** | 21 ± 10 *** | <0.001 |
| Yes | 126 ± 20 | 70 ± 14 *** | 46 ± 15 *** | 26 ± 11 *** | <0.001 | |
| Albumin excretion rate (mg/24 h) | No | NA | NA | NA | NA | |
| Yes | 24 (17–36) | 13 (12–92) | 53 (20–106) | 225 (44–722)** | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rabbani, N.; Adaikalakoteswari, A.; Larkin, J.R.; Panagiotopoulos, S.; MacIsaac, R.J.; Yue, D.K.; Fulcher, G.R.; Roberts, M.A.; Thomas, M.; Ekinci, E.; et al. Analysis of Serum Advanced Glycation Endproducts Reveals Methylglyoxal-Derived Advanced Glycation MG-H1 Free Adduct Is a Risk Marker in Non-Diabetic and Diabetic Chronic Kidney Disease. Int. J. Mol. Sci. 2023, 24, 152. https://doi.org/10.3390/ijms24010152
Rabbani N, Adaikalakoteswari A, Larkin JR, Panagiotopoulos S, MacIsaac RJ, Yue DK, Fulcher GR, Roberts MA, Thomas M, Ekinci E, et al. Analysis of Serum Advanced Glycation Endproducts Reveals Methylglyoxal-Derived Advanced Glycation MG-H1 Free Adduct Is a Risk Marker in Non-Diabetic and Diabetic Chronic Kidney Disease. International Journal of Molecular Sciences. 2023; 24(1):152. https://doi.org/10.3390/ijms24010152
Chicago/Turabian StyleRabbani, Naila, Antonysunil Adaikalakoteswari, James R. Larkin, Sianna Panagiotopoulos, Richard J. MacIsaac, Dennis K. Yue, Gregory R. Fulcher, Matthew A. Roberts, Merlin Thomas, Elif Ekinci, and et al. 2023. "Analysis of Serum Advanced Glycation Endproducts Reveals Methylglyoxal-Derived Advanced Glycation MG-H1 Free Adduct Is a Risk Marker in Non-Diabetic and Diabetic Chronic Kidney Disease" International Journal of Molecular Sciences 24, no. 1: 152. https://doi.org/10.3390/ijms24010152
APA StyleRabbani, N., Adaikalakoteswari, A., Larkin, J. R., Panagiotopoulos, S., MacIsaac, R. J., Yue, D. K., Fulcher, G. R., Roberts, M. A., Thomas, M., Ekinci, E., & Thornalley, P. J. (2023). Analysis of Serum Advanced Glycation Endproducts Reveals Methylglyoxal-Derived Advanced Glycation MG-H1 Free Adduct Is a Risk Marker in Non-Diabetic and Diabetic Chronic Kidney Disease. International Journal of Molecular Sciences, 24(1), 152. https://doi.org/10.3390/ijms24010152