

Efficacy of Lenvatinib Combined with Transcatheter Intra-Arterial Therapies for Patients with Advanced-Stage of Hepatocellular Carcinoma: A Propensity Score Matching

 , , , ,
, , , ,  ,
,  and
and 
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Patients
2.2. Therapeutic Outcomes of LEN according to mRECIST
2.3. Overall Survival with LEN for the Advanced Stage before PSM
2.4. Comparison of OS between LEN Combined with TIT and LEN Monotherapy before PSM
2.5. Patient Characteristics after PSM
2.6. Therapeutic Outcomes of LEN according to RECIST after PSM
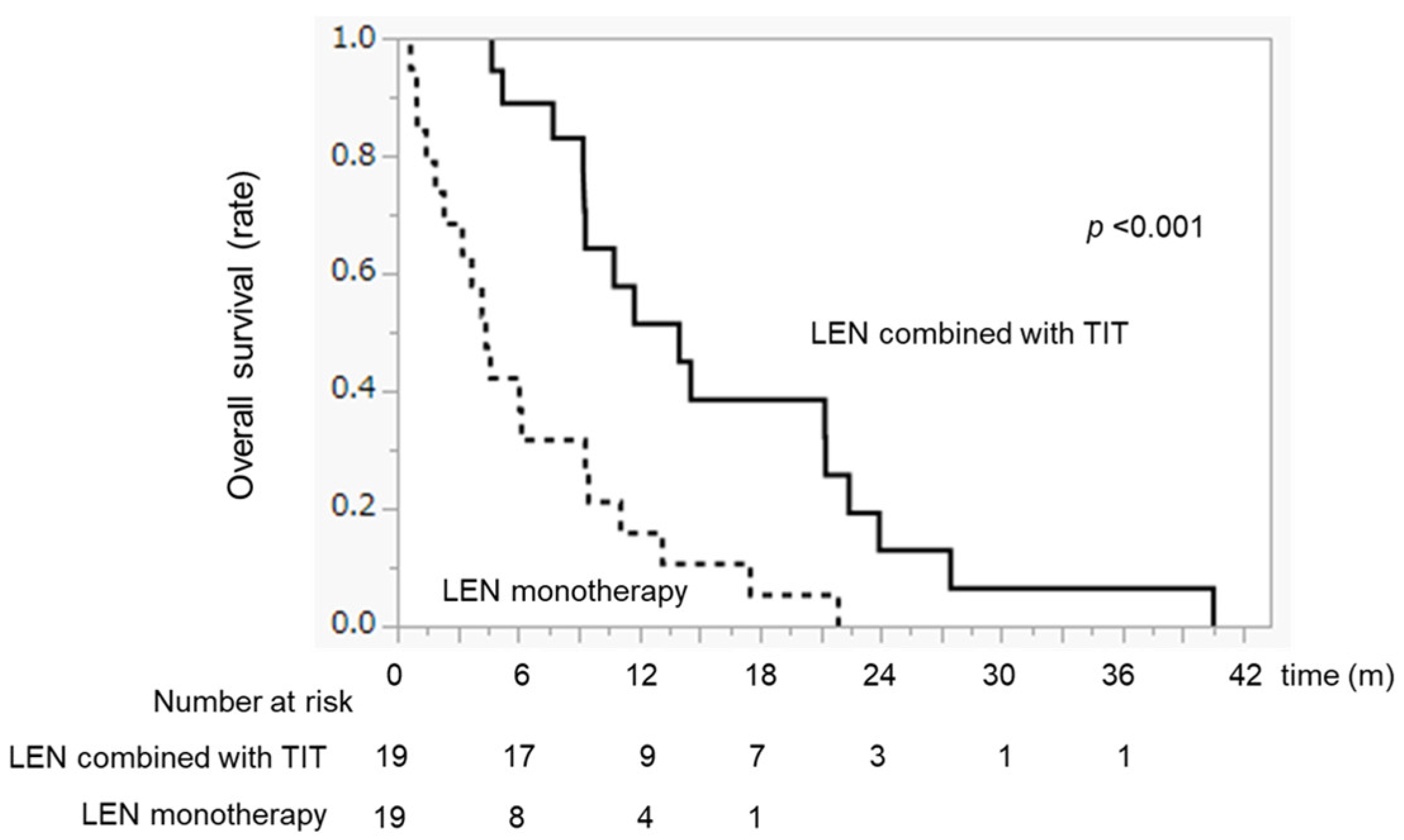
2.7. Comparison of OS between LEN Combined with TIT and LEN Monotherapy after PSM
2.8. Variables Associated with Overall Survival after PSM
2.9. Swimmer Plot Analysis in Patients Treated with LEN Combined with TIT
2.10. Treatment Duration of LEN with or without TIT after PSM
2.11. Additional Treatments after the Discontinuation of LEN after PSM
2.12. Decision-Tree Analysis for LEN Combined with TIT
2.13. Comparison of AEs between the Two Groups (Grade ≥ 3)
3. Discussion
4. Materials and Methods
4.1. Study Design and Patients
4.2. Lenvatinib Treatment Protocol
4.3. Evaluation of Therapeutic Response and Safety
4.4. LEN Combined with Transcatheter Intraarterial Therapies
4.5. TACE
4.6. HAIC
4.7. The Decision-Tree Algorithm
4.8. Propensity Score Matching
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Response Category | m-RECIST |
|---|---|
| CR | 0 (0.0%) |
| PR | 30 (26.1%) |
| SD | 49 (42.6%) |
| PD | 36 (31.3%) |
| ORR | 30 (26.1%) |
| DCR | 79 (78.7%) |

| LEN Combined with TIT | LEN Monotherapy | p | |
|---|---|---|---|
| n | 17 | 19 | |
| Additional treatment | 64.7% (11/17) | 73.6% (14/19) | 0.559 |
| Atez/Bev | 17.7% (3/17) | 21.0% (4/19) | |
| RAM | 11.8% (2/17) | 0.0% (0/19) | |
| SORA | 11.8% (2/17) | 21.0% (4/19) | |
| REGO | 0.0% (0/19) | 5.3% (1/19) | |
| TACE | 23.5% (4/17) | 10.7% (2/19) | |
| HAIC | 0.0% (0/17) | 21.0% (4/19) | |
| Best supportive care | 35.2% (6/17) | 21.0% (4/19) |
| LEN Combined with TIT (n = 30) | LEN Monotherapy (n = 85) | p-Value | |
|---|---|---|---|
| HFSR | 10.0% (3/30) | 5.9% (5/80) | 0.434 |
| Hypertension | 6.6% (2/30) | 10.5% (9/85) | 0.548 |
| Urine protein | 6.6% (2/30) | 12.9% (11/85) | 0.112 |
| Fatigue | 6.6% (2/30) | 10.5% (9/85) | 0.548 |
| Diarrhea | 6.6% (2/30) | 4.7% (4/85) | 0.657 |
| Loss of appetite | 3.3% (1/30) | 10.5% (9/85) | 0.200 |


References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. Bclc Strategy for Prognosis Prediction and Treatment Recommendation: The 2022 Update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Arii, S.; Yamaoka, Y.; Futagawa, S.; Inoue, K.; Kobayashi, K.; Kojiro, M.; Makuuchi, M.; Nakamura, Y.; Okita, K.; Yamada, R. Results of Surgical and Nonsurgical Treatment for Small-Sized Hepatocellular Carcinomas: A Retrospective and Nationwide Survey in Japan. The Liver Cancer Study Group of Japan. Hepatology 2000, 32, 1224–1229. [Google Scholar] [CrossRef] [PubMed]
- Shiina, S.; Sato, K.; Tateishi, R.; Shimizu, M.; Ohama, H.; Hatanaka, T.; Takawa, M.; Nagamatsu, H.; Imai, Y. Percutaneous Ablation for Hepatocellular Carcinoma: Comparison of Various Ablation Techniques and Surgery. Can. J. Gastroenterol. Hepatol. 2018, 2018, 4756147. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus Sorafenib in First-Line Treatment of Patients with Unresectable Hepatocellular Carcinoma: A Randomised Phase 3 Non-Inferiority Trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Kudo, M. Recent Advances in Systemic Therapy for Hepatocellular Carcinoma in an Aging Society: 2020 Update. Liver Cancer 2020, 9, 640–662. [Google Scholar] [CrossRef]
- Lin, L.W.; Ke, K.; Yan, L.Y.; Chen, R.; Huang, J.Y. Efficacy and Safety of Hepatic Artery Infusion Chemotherapy Combined with Tyrosine Kinase Inhibitors Plus Programmed Death-1 Inhibitors for Hepatocellular Carcinoma Refractory to Transarterial Chemoembolization. Front. Oncol. 2023, 13, 1178428. [Google Scholar] [CrossRef]
- Long, J.; Chen, B.; Liu, Z. Comparative Efficacy and Safety of Molecular Targeted Agents Combined with Transarterial Chemoembolization in the Treatment of Unresectable Hepatocellular Carcinoma: A Network Meta-Analysis. Front. Oncol. 2023, 13, 1179431. [Google Scholar] [CrossRef]
- Shimose, S.; Iwamoto, H.; Tanaka, M.; Niizeki, T.; Shirono, T.; Noda, Y.; Kamachi, N.; Okamura, S.; Nakano, M.; Suga, H.; et al. Alternating Lenvatinib and Trans-Arterial Therapy Prolongs Overall Survival in Patients with Inter-Mediate Stage Hepatocellular Carcinoma: A Propensity Score Matching Study. Cancers 2021, 13, 160. [Google Scholar] [CrossRef]
- Ding, X.; Sun, W.; Li, W.; Shen, Y.; Guo, X.; Teng, Y.; Liu, X.; Zheng, L.; Li, W.; Chen, J. Transarterial Chemoembolization Plus Lenvatinib versus Transarterial Chemoembolization Plus Sorafenib as First-Line Treatment for Hepatocellular Carcinoma with Portal Vein Tumor Thrombus: A Prospective Randomized Study. Cancer 2021, 127, 3782–3793. [Google Scholar] [CrossRef]
- Kawamura, Y.; Kobayashi, M.; Shindoh, J.; Kobayashi, Y.; Okubo, S.; Tominaga, L.; Kajiwara, A.; Kasuya, K.; Iritani, S.; Fujiyama, S.; et al. Lenvatinib-Transarterial Chemoembolization Sequential Therapy as an Effective Treatment at Progression during Lenvatinib Therapy for Advanced Hepatocellular Carcinoma. Liver Cancer 2020, 9, 756–770. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.; Yue, W.; Wen, H.; Wang, X.; Wang, Q. Analysis on Efficacy of Hepatic Artery Infusion Chemotherapy with or without Lenvatinib for Unresectable Hepatocellular Carcinoma. Eur. Surg. Res. 2023, 64, 268–277. [Google Scholar] [CrossRef]
- Peng, Z.; Fan, W.; Zhu, B.; Wang, G.; Sun, J.; Xiao, C.; Huang, F.; Tang, R.; Cheng, Y.; Huang, Z.; et al. Lenvatinib Combined with Transarterial Chemoembolization as First-Line Treatment for Advanced Hepatocellular Carcinoma: A Phase Iii, Randomized Clinical Trial (LAUNCH). J. Clin. Oncol. 2023, 41, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Uchino, K.; Tateishi, R.; Shiina, S.; Kanda, M.; Masuzaki, R.; Kondo, Y.; Goto, T.; Omata, M.; Yoshida, H.; Koike, K. Hepatocellular Carcinoma with Extrahepatic Metastasis: Clinical Features and Prognostic Factors. Cancer 2011, 117, 4475–4483. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.M.; Jang, J.W.; You, C.R.; Yoo, S.H.; Kwon, J.H.; Bae, S.H.; Choi, J.Y.; Yoon, S.K.; Chung, K.W.; Kay, C.S.; et al. Role of Intrahepatic Tumor Control in the Prognosis of Patients with Hepatocellular Carcinoma and Extrahepatic Metastases. J. Gastroenterol. Hepatol. 2012, 27, 684–689. [Google Scholar] [CrossRef]
- Lee, H.S. Management of Patients with Hepatocellular Carcinoma and Extrahepatic Metastasis. Dig. Dis. 2011, 29, 333–338. [Google Scholar] [CrossRef]
- Terashima, T.; Yamashita, T.; Horii, R.; Arai, K.; Kawaguchi, K.; Kitamura, K.; Yamashita, T.; Sakai, Y.; Mizukoshi, E.; Honda, M.; et al. Potential Efficacy of Therapies Targeting Intrahepatic Lesions after Sorafenib Treatment of Patients with Hepatocellular Carcinoma. BMC Cancer 2016, 16, 338. [Google Scholar] [CrossRef]
- Galle, P.R.; Foerster, F.; Kudo, M.; Chan, S.L.; Llovet, J.M.; Qin, S.; Schelman, W.R.; Chintharlapalli, S.; Abada, P.B.; Sherman, M.; et al. Biology and Significance of Alpha-Fetoprotein in Hepatocellular Carcinoma. Liver Int. 2019, 39, 2214–2229. [Google Scholar] [CrossRef]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular Carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef]
- Scheiner, B.; Pomej, K.; Kirstein, M.M.; Hucke, F.; Finkelmeier, F.; Waidmann, O.; Himmelsbach, V.; Schulze, K.; von Felden, J.; Fründt, T.W.; et al. Prognosis of Patients with Hepatocellular Carcinoma Treated with Immunotherapy—Development and Validation of the Crafity Score. J. Hepatol. 2022, 76, 353–363. [Google Scholar] [CrossRef]
- Peng, C.W.; Teng, W.; Lui, K.W.; Hung, C.F.; Jeng, W.J.; Huang, C.H.; Chen, W.T.; Lin, C.C.; Lin, C.Y.; Lin, S.M.; et al. Complete Response at First Transarterial Chemoembolization Predicts Favorable Outcome in Hepatocellular Carcinoma. Am. J. Cancer Res. 2021, 11, 4956–4965. [Google Scholar] [PubMed]
- Hatanaka, T.; Yata, Y.; Naganuma, A.; Kakizaki, S. Treatment Strategy for Intermediate-Stage Hepatocellular Carcinoma: Transarterial Chemoembolization, Systemic Therapy, and Conversion Therapy. Cancers 2023, 15, 1798. [Google Scholar] [CrossRef] [PubMed]
- Hou, W.; Bridgeman, B.; Malnassy, G.; Ding, X.; Cotler, S.J.; Dhanarajan, A.; Qiu, W. Integrin Subunit Beta 8 Contributes to Lenvatinib Resistance in HCC. Hepatol. Commun. 2022, 6, 1786–1802. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.M.; Zhang, J.G.; Zhang, X.; Li, Q. Targeting Cancer Stem Cells for Reversing Therapy Resistance: Mechanism, Signaling, and Prospective Agents. Signal Transduct. Target Ther. 2021, 6, 62. [Google Scholar] [CrossRef]
- Yao, X.H.; Ping, Y.F.; Bian, X.W. Contribution of Cancer Stem Cells to Tumor Vasculogenic Mimicry. Protein Cell 2011, 2, 266–272. [Google Scholar] [CrossRef]
- Guo, J.; Zhu, P.; Ye, Z.; Wang, M.; Yang, H.; Huang, S.; Shu, Y.; Zhang, W.; Zhou, H.; Li, Q. Yrdc Mediates the Resistance of Lenvatinib in Hepatocarcinoma Cells via Modulating the Translation of Kras. Front. Pharmacol. 2021, 12, 744578. [Google Scholar] [CrossRef]
- Suzuki, H.; Iwamoto, H.; Seki, T.; Nakamura, T.; Masuda, A.; Sakaue, T.; Tanaka, T.; Imamura, Y.; Niizeki, T.; Nakano, M.; et al. Tumor-Derived Insulin-like Growth Factor-Binding Protein-1 Contributes to Resistance of Hepatocellular Carcinoma to Tyrosine Kinase Inhibitors. Cancer Commun. 2023, 43, 415–434. [Google Scholar] [CrossRef]
- Carmeliet, P.; Jain, R.K. Molecular Mechanisms and Clinical Applications of Angiogenesis. Nature 2011, 473, 298–307. [Google Scholar] [CrossRef]
- Une, N.; Takano-Kasuya, M.; Kitamura, N.; Ohta, M.; Inose, T.; Kato, C.; Nishimura, R.; Tada, H.; Miyagi, S.; Ishida, T.; et al. The Anti-Angiogenic Agent Lenvatinib Induces Tumor Vessel Normalization and Enhances Radiosensitivity in Hepatocellular Tumors. Med. Oncol. 2021, 38, 60. [Google Scholar] [CrossRef]
- Sergio, A.; Cristofori, C.; Cardin, R.; Pivetta, G.; Ragazzi, R.; Baldan, A.; Girardi, L.; Cillo, U.; Burra, P.; Giacomin, A.; et al. Transcatheter Arterial Chemoembolization (Tace) in Hepatocellular Carcinoma (Hcc): The Role of Angiogenesis and Invasiveness. Am. J. Gastroenterol. 2008, 103, 914–921. [Google Scholar] [CrossRef]
- Shim, J.H.; Park, J.W.; Kim, J.H.; An, M.; Kong, S.Y.; Nam, B.H.; Choi, J.I.; Kim, H.B.; Lee, W.J.; Kim, C.M. Association between Increment of Serum Vegf Level and Prognosis after Transcatheter Arterial Chemoembolization in Hepatocellular Carcinoma Patients. Cancer Sci. 2008, 99, 2037–2044. [Google Scholar] [CrossRef] [PubMed]
- Quirk, M.; Kim, Y.H.; Saab, S.; Lee, E.W. Management of Hepatocellular Carcinoma with Portal Vein Thrombosis. World J. Gastroenterol. 2015, 21, 3462–3471. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.X.; Shi, J.; Li, N.; Guo, W.X.; Wu, M.C.; Lau, W.Y.; Cheng, S.Q. Portal Vein Tumor Thrombus Is a Bottleneck in the Treatment of Hepatocellular Carcinoma. Cancer Biol. Med. 2016, 13, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, H.; Niizeki, T.; Nagamatsu, H.; Ueshima, K.; Tani, J.; Kuzuya, T.; Kasai, K.; Kooka, Y.; Hiraoka, A.; Sugimoto, R.; et al. The Clinical Impact of Hepatic Arterial Infusion Chemotherapy New-Fp for Hepatocellular Carcinoma with Preserved Liver Function. Cancers 2022, 14, 4873. [Google Scholar] [CrossRef]
- Ueshima, K.; Ogasawara, S.; Ikeda, M.; Yasui, Y.; Terashima, T.; Yamashita, T.; Obi, S.; Sato, S.; Aikata, H.; Ohmura, T.; et al. Hepatic Arterial Infusion Chemotherapy versus Sorafenib in Patients with Advanced Hepatocellular Carcinoma. Liver Cancer 2020, 9, 583–595. [Google Scholar] [CrossRef]
- Long, Y.; Song, X.; Guan, Y.; Lan, R.; Huang, Z.; Li, S.; Zhang, L. Sorafenib Plus Hepatic Arterial Infusion Chemotherapy versus Sorafenib Alone for Advanced Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. J. Gastroenterol. Hepatol. 2023, 38, 486–495. [Google Scholar] [CrossRef]
- Zeng, L.; Kong, L.N.; Fang, Q.; Wang, W.X.; Fan, J.L.; Zhang, X.Q.; Yu, Y.H.; Yuan, S.T. Diagnostic Accuracy of the Frail Scale for Frailty Screening in Community-Dwelling Older Adults with Diabetes: A Cross-Sectional Study. Geriatr. Nurs. 2023, 52, 115–120. [Google Scholar] [CrossRef]
- Hiraoka, A.; Tanizawa, Y.; Huang, Y.J.; Cai, Z.; Sakaguchi, S. Association of Albumin-Bilirubin Grade and Sequential Treatment with Standard Systemic Therapies for Advanced Hepatocellular Carcinoma: A Retrospective Cohort Study Using a Japanese Administrative Database. Drugs Real. World Outcomes 2021, 8, 301–314. [Google Scholar] [CrossRef]
- Tsumura, S.; Shimose, S.; Niizeki, T.; Kuboyama, E.; Iwamoto, H.; Tanaka, M.; Moriyama, E.; Shirono, T.; Takaki, K.; Noda, Y.; et al. Telephone Follow-Up Contributes to Improving Adherence and Treatment Duration in Patients with Hepatocellular Carcinoma Treated with Lenvatinib. J. Gastroenterol. Hepatol. 2023, 38, 1140–1147. [Google Scholar] [CrossRef]
- Iwamoto, H.; Suzuki, H.; Shimose, S.; Niizeki, T.; Nakano, M.; Shirono, T.; Okamura, S.; Noda, Y.; Kamachi, N.; Nakamura, T.; et al. Weekends-Off Lenvatinib for Unresectable Hepatocellular Carcinoma Improves Therapeutic Response and Tolerability toward Adverse Events. Cancers 2020, 12, 1010. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified Recist (Mrecist) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Freites-Martinez, A.; Santana, N.; Arias-Santiago, S.; Viera, A. Using the Common Terminology Criteria for Adverse Events (Ctcae-Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies. Actas Dermosifiliogr. (Engl. Ed.) 2021, 112, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Aino, H.; Sumie, S.; Niizeki, T.; Kuromatsu, R.; Tajiri, N.; Nakano, M.; Satani, M.; Yamada, S.; Okamura, S.; Shimose, S.; et al. Clinical Characteristics and Prognostic Factors for Advanced Hepatocellular Carcinoma with Extrahepatic Metastasis. Mol. Clin. Oncol. 2014, 2, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Han, K.H.; Ye, S.L.; Zhou, J.; Huang, Y.H.; Lin, S.M.; Wang, C.K.; Ikeda, M.; Chan, S.L.; Choo, S.P.; et al. A Changing Paradigm for the Treatment of Intermediate-Stage Hepatocellular Carcinoma: Asia-Pacific Primary Liver Cancer Expert Consensus Statements. Liver Cancer 2020, 9, 245–260. [Google Scholar] [CrossRef] [PubMed]
- Shimose, S.; Kawaguchi, T.; Iwamoto, H.; Niizeki, T.; Shirono, T.; Tanaka, M.; Koga, H.; Torimura, T. Indication of Suitable Transarterial Chemoembolization and Multikinase Inhibitors for Intermediate Stage Hepatocellular Carcinoma. Oncol. Lett. 2020, 19, 2667–2676. [Google Scholar] [CrossRef]
- Niizeki, T.; Iwamoto, H.; Shirono, T.; Shimose, S.; Nakano, M.; Okamura, S.; Noda, Y.; Kamachi, N.; Hiroyuki, S.; Sakai, M.; et al. Clinical Importance of Regimens in Hepatic Arterial Infusion Chemotherapy for Advanced Hepatocellular Carcinoma with Macrovascular Invasion. Cancers 2021, 13, 4450. [Google Scholar] [CrossRef]
- Shimose, S.; Iwamoto, H.; Shirono, T.; Tanaka, M.; Niizeki, T.; Kajiwara, M.; Itano, S.; Yano, Y.; Matsugaki, S.; Moriyama, E.; et al. The Impact of Curative Conversion Therapy Aimed at a Cancer-Free State in Patients with Hepatocellular Carcinoma Treated with Atezolizumab Plus Bevacizumab. Cancer Med. 2023, 12, 12325–12335. [Google Scholar] [CrossRef]
- Niizeki, T.; Tokunaga, T.; Takami, Y.; Wada, Y.; Harada, M.; Shibata, M.; Nakao, K.; Sasaki, R.; Hirai, F.; Shakado, S.; et al. Comparison of Efficacy and Safety of Atezolizumab Plus Bevacizumab and Lenvatinib as First-Line Therapy for Unresectable Hepatocellular Carcinoma: A Propensity Score Matching Analysis. Target Oncol. 2022, 17, 643–653. [Google Scholar] [CrossRef]






| Characteristic | All Patients | LEN Combined with TIT | LEN Monotherapy | p |
|---|---|---|---|---|
| n | 115 | 30 | 85 | |
| Age (years old) | 71 (38–89) | 63 (38–78) | 73 (44–89) | <0.001 |
| Sex (female/male) | 23/92 | 5/25 | 18/67 | 0.590 |
| PS (0/1/2) | 105/8/1 | 28/2/0 | 77/7/1 | 0.475 |
| Etiology (HBV/HCV/Others) | 27/46/42 | 9/8/13 | 18/38/29 | 0.205 |
| ALBI score (Median (range)) | −2.50 (−3.34–−1.49) | −2.66 (−3.34–−1.91) | −2.47 (−3.33–−1.49) | 0.001 |
| m-ALBI grade (1/2a/2b) | 47/34/34 | 18/6/6 | 29/28/28 | 0.047 |
| Tumor size (mm) | 40 (11–190) | 40 (11–190) | 40 (10–135) | 0.396 |
| Number tumors <5/≥5 | 31/84 | 8/22 | 23/62 | 0.966 |
| Macrovascular invasion (No/Yes) | 87/28 | 18/12 | 69/16 | 0.024 |
| Extrahepatic spread (No/Yes) | 27/88 | 10/20 | 17/68 | 0.138 |
| Initial dose of LEN | 0.454 | |||
| 12 mg | 31 | 10 | 21 | |
| 8 mg | 71 | 15 | 56 | |
| 8 mg weekend methods | 3 | 2 | 1 | |
| 4 mg | 8 | 2 | 6 | |
| 4 mg weekend methods | 2 | 1 | 1 | |
| Combination therapy | n.s. | |||
| TACE | 12 | 12 | ||
| HAIC | 18 | 18 | ||
| AFP (ng/mL) | 92.7 (1.0–146,260) | 78.9 (1.7–56,225) | 133.0 (1.0–146,260) | 0.605 |
| Treatment line (1st/2nd/3rd) | 77/27/11 | 21/6/3 | 56/21/8 | 0.869 |
| Characteristic | All Patients | LEN Combined with TIT | LEN Monotherapy | p |
|---|---|---|---|---|
| n | 38 | 19 | 19 | |
| Age (years old) | 67 (44–79) | 68 (44–78) | 66 (44–79) | 0.578 |
| Sex (female/male) | 8/30 | 4/15 | 4/15 | n.s. |
| PS (0/1/2) | 33/5/0 | 17/2/0 | 16/3/0 | 0.305 |
| Etiology (HBV/HCV/Others) | 12/11/15 | 5/5/9 | 7/6/6 | 0.597 |
| ALBI score (Median (range)) | −2.66 (−3.33–−1.91) | −2.69 (−3.06–−1.91) | −2.65 (−3.33–−2.10) | 0.883 |
| m-ALBI grade (1/2a/2b) | 22/8/8 | 11/3/5 | 11/5/3 | 0.603 |
| Tumor size (mm) | 38 (11–131) | 37 (11–131) | 40 (11–92) | 0.770 |
| Number tumors <5/≥5 | 9/29 | 5/14 | 4/15 | 0.702 |
| Macrovascular invasion (No/Yes) | 25/13 | 11/8 | 14/5 | 0.303 |
| Extrahepatic spread (No/Yes) | 12/26 | 7/12 | 5/14 | 0.484 |
| Initial dose of LEN | 0.338 | |||
| 12 mg | 12 | 5 | 7 | |
| 8 mg | 23 | 11 | 12 | |
| 8 mg weekend methods | 1 | 1 | 0 | |
| 4 mg | 1 | 1 | 0 | |
| 4 mg weekend methods | 1 | 1 | 0 | |
| Combination therapy | n.s. | |||
| TACE | 7 | 7 | ||
| HAIC | 12 | 12 | ||
| AFP (ng/mL) | 59.6 (1.6–56,225) | 78.9 (1.7–56,225) | 133.0 (1.0–146,260) | 0.605 |
| Treatment line (1st/2nd/3rd) | 31/4/3 | 15/3/1 | 16/1/2 | 0.492 |
| Variables | LEN Combined with TIT (n = 19) | LEN Monotherapy (n = 19) | p |
|---|---|---|---|
| CR | 1 (5.3%) | 0 (0.0%) | |
| PR | 8 (42.1%) | 3 (15.7%) | |
| SD | 9 (47.3%) | 9 (47.4%) | |
| PD | 1 (5.3%) | 7 (36.9%) | |
| ORR | 9 (47.3%) | 3 (15.7%) | 0.032 |
| DCR | 18 (94.7%) | 12 (63.1%) | 0.017 |
| Variable | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| p-Value | Odds Ratio | 95% CI | p-Value | |
| Age, <75 vs. ≥75 | 0.998 | |||
| Sex, female vs. male | 0.226 | |||
| Etiology, (HBV vs. HCV vs. other) | 0.245 | |||
| ALBI grade, 1 vs. 2 | 0.566 | |||
| Number tumors, <5 vs. ≥5 | 0.681 | |||
| Tumor size, <30 vs. ≥30 | 0.032 | 0.475 | 0.184–1.22 | 0.122 |
| Macrovascular invasion, (No/Yes) | 0.269 | |||
| Extrahepatic spread, (No/Yes) | 0.495 | |||
| LEN combined with TIT, (+/−) | 0.013 | 0.371 | 0.164–0.837 | 0.013 |
| AFP, <200 vs. ≥200 ng/ml | 0.001 | 0.367 | 0.161–0.832 | 0.012 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimose, S.; Iwamoto, H.; Niizeki, T.; Tanaka, M.; Shirono, T.; Moriyama, E.; Noda, Y.; Nakano, M.; Suga, H.; Kuromatsu, R.; et al. Efficacy of Lenvatinib Combined with Transcatheter Intra-Arterial Therapies for Patients with Advanced-Stage of Hepatocellular Carcinoma: A Propensity Score Matching. Int. J. Mol. Sci. 2023, 24, 13715. https://doi.org/10.3390/ijms241813715
Shimose S, Iwamoto H, Niizeki T, Tanaka M, Shirono T, Moriyama E, Noda Y, Nakano M, Suga H, Kuromatsu R, et al. Efficacy of Lenvatinib Combined with Transcatheter Intra-Arterial Therapies for Patients with Advanced-Stage of Hepatocellular Carcinoma: A Propensity Score Matching. International Journal of Molecular Sciences. 2023; 24(18):13715. https://doi.org/10.3390/ijms241813715
Chicago/Turabian StyleShimose, Shigeo, Hideki Iwamoto, Takashi Niizeki, Masatoshi Tanaka, Tomotake Shirono, Etsuko Moriyama, Yu Noda, Masahito Nakano, Hideya Suga, Ryoko Kuromatsu, and et al. 2023. "Efficacy of Lenvatinib Combined with Transcatheter Intra-Arterial Therapies for Patients with Advanced-Stage of Hepatocellular Carcinoma: A Propensity Score Matching" International Journal of Molecular Sciences 24, no. 18: 13715. https://doi.org/10.3390/ijms241813715
APA StyleShimose, S., Iwamoto, H., Niizeki, T., Tanaka, M., Shirono, T., Moriyama, E., Noda, Y., Nakano, M., Suga, H., Kuromatsu, R., Torimura, T., Koga, H., & Kawaguchi, T. (2023). Efficacy of Lenvatinib Combined with Transcatheter Intra-Arterial Therapies for Patients with Advanced-Stage of Hepatocellular Carcinoma: A Propensity Score Matching. International Journal of Molecular Sciences, 24(18), 13715. https://doi.org/10.3390/ijms241813715