
Characterization of Serum Cytokine Profiles of Patients with Active Lupus Nephritis
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Study Population
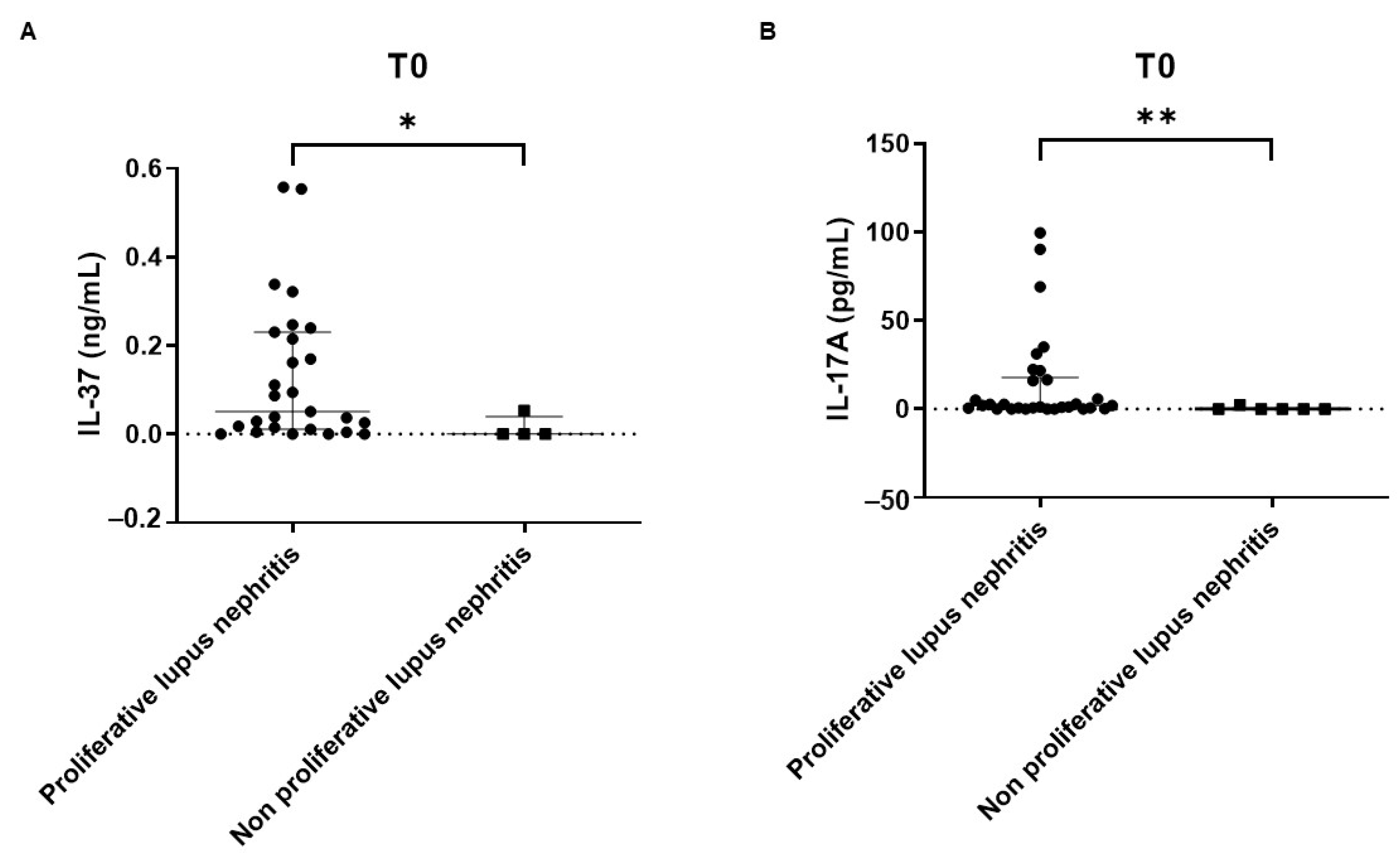
2.2. Cross-Sectional Study
2.3. Prospective Study
2.4. Renal Response
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Study Design
4.2.1. Cross-Sectional Phase
4.2.2. Prospective Phase
4.3. Cytokines and Serology Analysis
4.4. Ethics
4.5. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Doria, A.; Iaccarino, L.; Ghirardello, A.; Zampieri, S.; Arienti, S.; Sarzi-Puttini, P.; Atzeni, F.; Piccoli, A.; Todesco, S. Long-Term Prognosis and Causes of Death in Systemic Lupus Erythematosus. Am. J. Med. 2006, 119, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Gatto, M.; Zen, M.; Ghirardello, A.; Bettio, S.; Bassi, N.; Iaccarino, L.; Punzi, L.; Doria, A. Emerging and critical issues in the pathogenesis of lupus. Autoimmun. Rev. 2013, 12, 523–536. [Google Scholar] [CrossRef] [PubMed]
- Gasparotto, M.; Gatto, M.; Binda, V.; Doria, A.; Moroni, G. Lupus nephritis: Clinical presentations and outcomes in the 21st century. Rheumatol. 2020, 59 (Suppl. S5), v39–v51. [Google Scholar] [CrossRef] [PubMed]
- Yung, S.; Yap, D.Y.; Chan, T.M. A review of advances in the understanding of lupus nephritis pathogenesis as a basis for emerging therapies. F1000Research 2020, 9, 905. [Google Scholar] [CrossRef] [PubMed]
- Doria, A.; Gatto, M. Nephritogenic-antinephritogenic antibody network in lupus glomerulonephritis. Lupus 2012, 21, 1492–1496. [Google Scholar] [CrossRef]
- Marín-Rosales, M.; Palafox-Sánchez, C.A.; Franco-Topete, R.A.; Carrillo-Ballesteros, F.J.; Cruz, A.; Salazar-Camarena, D.C.; Muñoz-Valle, J.F.; Ramos-Solano, F. Renal Tissue Expression of BAFF and BAFF Receptors Is Associated with Proliferative Lupus Nephritis. J. Clin. Med. 2022, 12, 71. [Google Scholar] [CrossRef]
- Tawfik, M.G.; Nasef, S.I.; Omar, H.H.; Ghaly, M.S. Serum Interleukin-37: A new player in Lupus Nephritis? Int. J. Rheum. Dis. 2017, 20, 996–1001. [Google Scholar] [CrossRef]
- Lieberman, L.A.; Tsokos, G.C. The IL-2 Defect in Systemic Lupus Erythematosus Disease Has an Expansive Effect on Host Immunity. J. Biomed. Biotechnol. 2010, 2010, 740619. [Google Scholar] [CrossRef]
- Wei, W.; Zhao, Y.; Zhang, Y.; Jin, H.; Shou, S. The role of IL-10 in kidney disease. Int. Immunopharmacol. 2022, 108, 108917. [Google Scholar] [CrossRef]
- Li, D.; Guo, B.; Wu, H.; Tan, L.; Chang, C.; Lu, Q. Interleukin-17 in systemic lupus erythematosus: A comprehensive review. Autoimmunity 2015, 48, 353–361. [Google Scholar] [CrossRef]
- Wong, C.K.; Ho, C.Y.; Li, E.K.; Tam, L.S.; Lam, C.W.K. Elevated production of interleukin-18 is associated with renal disease in patients with systemic lupus erythematosus. Clin. Exp. Immunol. 2002, 130, 345–351. [Google Scholar] [CrossRef]
- Ye, L.; Ji, L.; Wen, Z.; Zhou, Y.; Hu, D.; Li, Y.; Yu, T.; Chen, B.; Zhang, J.; Ding, L.; et al. IL-37 inhibits the production of inflammatory cytokines in peripheral blood mononuclear cells of patients with systemic lupus erythematosus: Its correlation with disease activity. J. Transl. Med. 2014, 12, 69. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.; Bieber, K.; Manz, R.A. IL-10 revisited in systemic lupus erythematosus. Front. Immunol. 2022, 13, 970906. [Google Scholar] [CrossRef] [PubMed]
- Paquissi, F.C.; Abensur, H. The Th17/IL-17 Axis and Kidney Diseases, With Focus on Lupus Nephritis. Front. Med. 2021, 8, 654912. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.-D.; Pan, H.-F.; Ye, D.-Q. Association of interleukin-18 and systemic lupus erythematosus. Rheumatol. Int. 2013, 33, 3055–3057. [Google Scholar] [CrossRef] [PubMed]
- Ihim, S.A.; Abubakar, S.D.; Zian, Z.; Sasaki, T.; Saffarioun, M.; Maleknia, S.; Azizi, G. Interleukin-18 cytokine in immunity, inflammation, and autoimmunity: Biological role in induction, regulation, and treatment. Front. Immunol. 2022, 13, 919973. [Google Scholar] [CrossRef] [PubMed]
- Möckel, T.; Basta, F.; Weinmann-Menke, J.; Schwarting, A. B cell activating factor (BAFF): Structure, functions, autoimmunity and clinical implications in Systemic Lupus Erythematosus (SLE). Autoimmun. Rev. 2021, 20, 102736. [Google Scholar] [CrossRef]
- Groom, J.R.; Fletcher, C.A.; Walters, S.N.; Grey, S.T.; Watt, S.V.; Sweet, M.J.; Smyth, M.J.; Mackay, C.R.; Mackay, F. BAFF and MyD88 signals promote a lupuslike disease independent of T cells. J. Exp. Med. 2007, 204, 1959–1971. [Google Scholar] [CrossRef]
- Itotagawa, E.; Tomofuji, Y.; Kato, Y.; Konaka, H.; Tsujimoto, K.; Park, J.; Nagira, D.; Hirayama, T.; Jo, T.; Hirano, T.; et al. SLE stratification based on BAFF and IFN-I bioactivity for biologics and implications of BAFF produced by glomeruli in lupus nephritis. Rheumatology 2023, 62, 1988–1997. [Google Scholar] [CrossRef]
- Giordano, D.; Kuley, R.; Draves, K.E.; Elkon, K.B.; Giltiay, N.V.; Clark, E.A. B cell-activating factor (BAFF) from dendritic cells, monocytes and neutrophils is required for B cell maturation and autoantibody production in SLE-like autoimmune disease. Front. Immunol. 2023, 14, 1050528. [Google Scholar] [CrossRef]
- Wu, Y.; Hsing, C.; Chiu, C.; Huang, H.; Hsu, Y. Roles of IL-1 and IL-10 family cytokines in the progression of systemic lupus erythematosus: Friends or foes? IUBMB Life 2022, 74, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Winikajtis-Burzyńska, A.; Brzosko, M.; Przepiera-Będzak, H. Increased Serum Interleukin 10 Levels Are Associated with Increased Disease Activity and Increased Risk of Anti-SS-A/Ro Antibody Positivity in Patients with Systemic Lupus Erythematosus. Biomolecules 2023, 13, 974. [Google Scholar] [CrossRef] [PubMed]
- Parodis, I.; Åkerström, E.; Sjöwall, C.; Sohrabian, A.; Jönsen, A.; Gomez, A.; Frodlund, M.; Zickert, A.; Bengtsson, A.A.; Rönnelid, J.; et al. Autoantibody and Cytokine Profiles during Treatment with Belimumab in Patients with Systemic Lupus Erythematosus. Int. J. Mol. Sci. 2020, 21, 3463. [Google Scholar] [CrossRef] [PubMed]
- Parodis, I.; Gatto, M.; Sjöwall, C. B cells in systemic lupus erythematosus: Targets of new therapies and surveillance tools. Front. Med. 2022, 9, 952304. [Google Scholar] [CrossRef]
- Talaat, R.M.; Mohamed, S.F.; Bassyouni, I.H.; Raouf, A.A. Th1/Th2/Th17/Treg cytokine imbalance in systemic lupus erythematosus (SLE) patients: Correlation with disease activity. Cytokine 2015, 72, 146–153. [Google Scholar] [CrossRef]
- Su, D.-L.; Lu, Z.-M.; Shen, M.-N.; Li, X.; Sun, L.-Y. Roles of Pro- and Anti-Inflammatory Cytokines in the Pathogenesis of SLE. J. Biomed. Biotechnol. 2012, 2012, 347141. [Google Scholar] [CrossRef]
- Nold, M.F.; Nold-Petry, C.A.; Zepp, J.A.; Palmer, B.E.; Bufler, P.; A Dinarello, C. IL-37 is a fundamental inhibitor of innate immunity. Nat. Immunol. 2010, 11, 1014–1022. [Google Scholar] [CrossRef]
- Wu, Q.; Zhou, J.; Yuan, Z.-C.; Lan, Y.-Y.; Xu, W.-D.; Huang, A.-F. Association between IL-37 and Systemic Lupus Erythematosus Risk. Immunol. Investig. 2022, 51, 727–738. [Google Scholar] [CrossRef]
- Moneim, N.H.A.; Hosny, M.M.; Omar, H.H.; Abdelnaby, M.M.; Fouad, M.M.; El-Waheed, W.O.A.; Elmedany, S.H.; Zaki, H.M. Relative CTLA-4, PTPN-22, and interleukin 37 mRNA expressions in patients with lupus nephritis. Reumatol. Clin. 2023, 19, 180–187. [Google Scholar] [CrossRef]
- Zeng, H.; Zhou, K.; Ye, Z. Biology of interleukin-37 and its role in autoimmune diseases (Review). Exp. Ther. Med. 2022, 24, 495. [Google Scholar] [CrossRef]
- Su, Z.; Tao, X. Current Understanding of IL-37 in Human Health and Disease. Front. Immunol. 2021, 12, 696605. [Google Scholar] [CrossRef] [PubMed]
- Larosa, M.; Zen, M.; Gatto, M.; Jesus, D.; Zanatta, E.; Iaccarino, L.; Inês, L.; Doria, A. IL-12 and IL-23/Th17 axis in systemic lupus erythematosus. Exp. Biol. Med. 2019, 244, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Galil, S.M.A.; Ezzeldin, N.; El-Boshy, M.E. The role of serum IL-17 and IL-6 as biomarkers of disease activity and predictors of remission in patients with lupus nephritis. Cytokine 2015, 76, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yan, C.; Yu, L.; Zhang, X.; Shang, J.; Fan, J.; Zhang, R.; Ren, J.; Duan, X. The star target in SLE: IL-17. Inflamm. Res. 2023, 72, 313–328. [Google Scholar] [CrossRef] [PubMed]
- Hristova, M.; Kamenarska, Z.; Dzhebir, G.; Nikolova, S.; Hristova, R.; Mihova, K.; Vinkov, A.; Georgiev, T.; Pozharashka, J.; Kaneva, R.; et al. The role of IL-17 rs2275913, IL-17RC rs708567 and TGFB1 rs1800469 SNPs and IL-17A serum levels in patients with lupus nephritis. Rheumatol. Int. 2021, 41, 2205–2213. [Google Scholar] [CrossRef]
- Park, J.; Yang, S.; Hwang, S.; Choi, J.; Kwok, S.; Kong, Y.; Youn, J.; Cho, M.; Park, S. B Cell–Specific Deletion of CR6-Interacting Factor 1 Drives Lupus-like Autoimmunity by Activation of Interleukin-17, Interleukin-6, and Pathogenic Follicular Helper T Cells in a Mouse Model. Arthritis Rheumatol. 2022, 74, 1211–1222. [Google Scholar] [CrossRef]
- Xiang, M.; Feng, Y.; Wang, Y.; Wang, J.; Zhang, Z.; Liang, J.; Xu, J. Correlation between circulating interleukin-18 level and systemic lupus erythematosus: A meta-analysis. Sci. Rep. 2021, 11, 4707. [Google Scholar] [CrossRef]
- Mende, R.; Vincent, F.B.; Kandane-Rathnayake, R.; Koelmeyer, R.; Lin, E.; Chang, J.; Hoi, A.Y.; Morand, E.F.; Harris, J.; Lang, T. Analysis of Serum Interleukin (IL)-1β and IL-18 in Systemic Lupus Erythematosus. Front. Immunol. 2018, 9, 1250. [Google Scholar] [CrossRef]
- Calvani, N.; Tucci, M.; Richards, H.B.; Tartaglia, P.; Silvestris, F. Th1 cytokines in the pathogenesis of lupus nephritis: The role of IL-18. Autoimmun. Rev. 2005, 4, 542–548. [Google Scholar] [CrossRef]
- Umare, V.; Pradhan, V.; Nath, S.; Rajadhyaksha, A.; Ghosh, K.; Nadkarni, A. Impact of functional IL-18 polymorphisms on genetic predisposition and diverse clinical manifestations of the disease in Indian SLE patients. Lupus 2019, 28, 545–554. [Google Scholar] [CrossRef]
- Mohsen, M.A.; Karim, S.A.A.; Abbas, T.M.; Amin, M. Serum interleukin-18 levels in patients with systemic lupus erythematosus: Relation with disease activity and lupus nephritis. Egypt. Rheumatol. 2013, 35, 45–51. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Rheumatology 2019, 78, 1151–1159. [Google Scholar] [CrossRef]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus ery-thematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef] [PubMed]
- Bajema, I.M.; Wilhelmus, S.; Alpers, C.E.; Bruijn, J.A.; Colvin, R.B.; Cook, H.T.; D’agati, V.D.; Ferrario, F.; Haas, M.; Jennette, J.C.; et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: Clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018, 93, 789–796. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Rheumatol. 2019, 78, 736–745. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | |
|---|---|
| Patients, n | 29 |
| Age at baseline, mean ± SD (years) | 39.7 ± 16.7 |
| Females, n (%) | 19 (65.5) |
| Caucasians n (%) | 24 (82.8) |
| Smokers, n (%) | 5 (17.2) |
| SLE disease duration at baseline, mean ± SD (years) | 9.9 ± 9.2 |
| Histological Class at Renal Biopsy | |
| Proliferative LN, n (%) | 24 (82.8) |
| Non-proliferative LN, n (%) | 5 (17.2) |
| Class II | 2 (6.9) |
| Class III | 2 (6.9) |
| Class IV | 20 (69.0) |
| Class V | 2 (6.9) |
| Mixed class (III + IV, IV + V, III + V) | 2 (6.9) |
| Other (podocytopathy) | 1 (3.4) |
| Clinical Features at Baseline | |
| Chronic kidney disease, n (%) | 5 (17.2) |
| End-stage kidney disease, n (%) | 0 (0) |
| Serology, n (%) | |
| ANA > 1:80 | 29 (100) |
| Anti-dsDNA | 22 (75.9) |
| Anti-Sm | 8 (27.6) |
| Anti-U1RNP | 6 (20.7) |
| Anti-Scl70 | 5 (17.2) |
| Anti-SSA | 18 (62.1) |
| Anti-SSB | 9 (31.0) |
| Anti-phospholipid antibodies | |
| - Single positivity | 9 (31.0) |
| - Double positivity | 2 (6.9) |
| - Triple positivity | 2 (6.9) |
| Active urinary sediment, n (%) | 22 (75.9) |
| Proteinuria > 3 g/24 h, n (%) | 13 (44.8) |
| Low complement, n (%) | 21 (72.4) |
| Anti-dsDNA antibody levels (UI/mL) (mean ± SD) | 420.1 ± 940.4 |
| Hypertension, n (%) | 14 (48.3) |
| Anemia, n (%) | 16 (55.17) |
| Leucopenia, n (%) | 11 (25.6) |
| Thrombocytopenia, n (%) | 9 (31.0) |
| SLEDAI-2K score, mean ± SD | 10.6 ± 5.0 |
| CRP (mg/L), mean ± SD | 2.3 ± 2.7 |
| ESR (mm/h), mean ± SD | 24.2 ± 16.3 |
| Treatment Administered at Baseline | |
| CS pulses, n (%) | 24 (82.8) |
| Oral CS, n (%) | 26 (89.7) |
| MMF, n (%) | 26 (89.7) |
| MMF + CNI, n (%) | 1 (3.4) |
| IV CYC, n (%) | 5 (17.2) |
| RTX, n (%) | 1 (3.4) |
| HCQ, n (%) | 22 (75.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahmé, Z.; Franco, C.; Cruciani, C.; Pettorossi, F.; Zaramella, A.; Realdon, S.; Iaccarino, L.; Frontini, G.; Moroni, G.; Doria, A.; et al. Characterization of Serum Cytokine Profiles of Patients with Active Lupus Nephritis. Int. J. Mol. Sci. 2023, 24, 14883. https://doi.org/10.3390/ijms241914883
Rahmé Z, Franco C, Cruciani C, Pettorossi F, Zaramella A, Realdon S, Iaccarino L, Frontini G, Moroni G, Doria A, et al. Characterization of Serum Cytokine Profiles of Patients with Active Lupus Nephritis. International Journal of Molecular Sciences. 2023; 24(19):14883. https://doi.org/10.3390/ijms241914883
Chicago/Turabian StyleRahmé, Zahrà, Chiara Franco, Claudio Cruciani, Federico Pettorossi, Alice Zaramella, Stefano Realdon, Luca Iaccarino, Giulia Frontini, Gabriella Moroni, Andrea Doria, and et al. 2023. "Characterization of Serum Cytokine Profiles of Patients with Active Lupus Nephritis" International Journal of Molecular Sciences 24, no. 19: 14883. https://doi.org/10.3390/ijms241914883