
Eicosapentaenoic and Docosahexaenoic Acid Supplementation Increases HDL Content in n-3 Fatty Acids and Improves Endothelial Function in Hypertriglyceridemic Patients
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
2.1. Patients Included in the Study
2.2. Anthropometric and Biochemical Characteristics during EPA and DHA Supplementation
2.3. HDL Characterization
2.3.1. HDL Subclasses and Lipid Content
2.3.2. HDL Stability
2.4. Effect n-3 Supplementation on Vascular Function
2.4.1. Flow-Mediated Vasodilation In Vivo
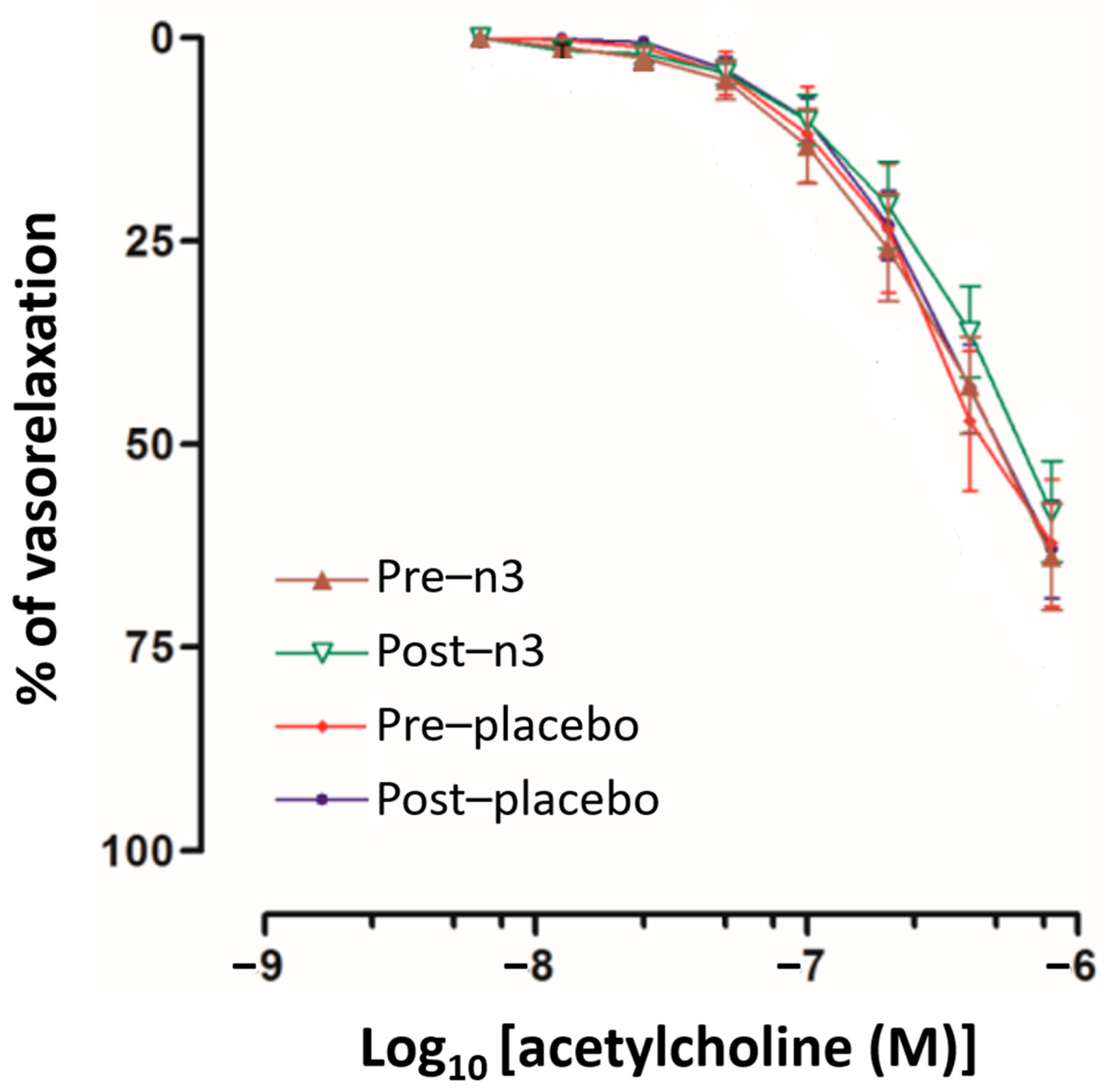
2.4.2. Endothelial-Mediated Vasodilation In Vitro
3. Discussion
4. Materials and Methods
4.1. Patients and Study Design
4.2. Laboratory Analysis
4.3. HDL Subclasses Composition Assessment
4.4. HDL Stability
4.5. Flow-Mediated Vasodilation
4.6. Vascular Reactivity of Aorta Rings
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wiest, E.F.; Walsh-Wilcox, M.T.; Walker, M.K. Omega-3 Polyunsaturated Fatty Acids Protect Against Cigarette Smoke-Induced Oxidative Stress and Vascular Dysfunction. Toxicol. Sci. 2017, 156, 300–310. [Google Scholar] [CrossRef] [PubMed]
- Goodfellow, J.; Bellamy, M.F.; Ramsey, M.W.; Jones, C.J.; Lewis, M.J. Dietary supplementation with marine omega-3 fatty acids improve systemic large artery endothelial function in subjects with hypercholesterolemia. J. Am. Coll. Cardiol. 2000, 35, 265–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siasos, G.; Tousoulis, D.; Oikonomou, E.; Zaromitidou, M.; Verveniotis, A.; Plastiras, A.; Kioufis, S.; Maniatis, K.; Miliou, A.; Siasou, Z.; et al. Effects of Ω-3 fatty acids on endothelial function, arterial wall properties, inflammatory and fibrinolytic status in smokers: A cross over study. Int. J. Cardiol. 2013, 166, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Hoshi, T.; Wissuwa, B.; Tian, Y.; Tajima, N.; Xu, R.; Bauer, M.; Heinemann, S.H.; Hou, S. Omega-3 fatty acids lower blood pressure by directly activating large-conductance Ca2⁺-dependent K⁺ channels. Proc. Natl. Acad. Sci. USA 2013, 110, 4816–4821. [Google Scholar] [CrossRef] [Green Version]
- Miller, P.E.; Van Elswyk, M.; Alexander, D.D. Long-chain omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid and blood pressure: A meta-analysis of randomized controlled trials. Am. J. Hypertens. 2014, 27, 885–896. [Google Scholar] [CrossRef]
- Zehr, K.R.; Walker, M.K. Omega-3 polyunsaturated fatty acids improve endothelial function in humans at risk for atherosclerosis: A review. Prostaglandins Other Lipid Mediat. 2018, 134, 131–140. [Google Scholar] [CrossRef]
- Bockus, L.; Kim, F. Coronary endothelial dysfunction: From pathogenesis to clinical implications. Open Heart 2022, 9, e002200. [Google Scholar] [CrossRef]
- Rossi, R.; Nuzzo, A.; Origliani, G.; Modena, M.G. Prognostic role of flow-mediated dilation and cardiac risk factors in post-menopausal women. J. Am. Coll. Cardiol. 2008, 51, 997–1002. [Google Scholar] [CrossRef] [Green Version]
- Shechter, M.; Issachar, A.; Marai, I.; Koren-Morag, N.; Freinark, D.; Shahar, Y.; Shechter, A.; Feinberg, M.S. Long-term association of brachial artery flow-mediated vasodilation and cardiovascular events in middle-aged subjects with no apparent heart disease. Int. J. Cardiol. 2009, 134, 52–58. [Google Scholar] [CrossRef]
- Witte, D.R.; Westerink, J.; de Koning, E.J.; van der Graaf, Y.; Grobbee, D.E.; Bots, M.L. Is the association between flow-mediated dilation and cardiovascular risk limited to low-risk populations? J. Am. Coll. Cardiol. 2005, 45, 1987–1993. [Google Scholar] [CrossRef] [Green Version]
- Modena, M.G.; Bonetti, L.; Coppi, F.; Bursi, F.; Rossi, R. Prognostic role of reversible endothelial dysfunction in hypertensive postmenopausal women. J. Am. Coll. Cardiol. 2002, 40, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Del Gaudio, I.; Rubinelli, L.; Sasset, L.; Wadsack, C.; Hla, T.; Di Lorenzo, A. Endothelial Spns2 and ApoM Regulation of Vascular Tone and Hypertension Via Sphingosine-1-Phosphate. J. Am. Heart Assoc. 2021, 10, e021261. [Google Scholar] [CrossRef]
- Takaeko, Y.; Matsui, S.; Kajikawa, M.; Maruhashi, T.; Yamaji, T.; Harada, T.; Han, Y.; Hashimoto, H.; Kihara, Y.; Hida, E.; et al. Relationship between high-density lipoprotein cholesterol levels and endothelial function in women: A cross-sectional study. BMJ Open 2020, 10, e038121. [Google Scholar] [CrossRef] [PubMed]
- Acikgoz, N.; Kurtoğlu, E.; Yagmur, J.; Kapicioglu, Y.; Cansel, M.; Ermis, N. Elevated Monocyte to High-Density Lipoprotein Cholesterol Ratio and Endothelial Dysfunction in Behçet Disease. Angiology 2018, 69, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Cartolano, F.C.; Dias, G.D.; Miyamoto, S.; Damasceno, N.R.T. Omega-3 Fatty Acids Improve Functionality of High-Density Lipoprotein in Individuals With High Cardiovascular Risk: A Randomized, Parallel, Controlled and Double-Blind Clinical Trial. Front. Nutr. 2022, 8, 767535. [Google Scholar] [CrossRef]
- Luna-Luna, M.; Niesor, E.; Pérez-Méndez, Ó. HDL as Bidirectional Lipid Vectors: Time for New Paradigms. Biomedicines 2022, 10, 1180. [Google Scholar] [CrossRef]
- Kratzer, A.; Giral, H.; Landmesser, U. High-density lipoproteins as modulators of endothelial cell functions: Alterations in patients with coronary artery disease. Cardiovasc. Res. 2014, 103, 350–361. [Google Scholar] [CrossRef] [Green Version]
- Muñoz-Vega, M.; Massó, F.; Páez, A.; Vargas-Alarcón, G.; Coral-Vázquez, R.; Mas-Oliva, J.; Carreón-Torres, E.; Pérez-Méndez, Ó. HDL-Mediated Lipid Influx to Endothelial Cells Contributes to Regulating Intercellular Adhesion Molecule (ICAM)-1 Expression and eNOS Phosphorylation. Int. J. Mol. Sci. 2018, 19, 3394. [Google Scholar] [CrossRef] [Green Version]
- López-Olmos, V.; Luna-Luna, M.; Carreón-Torres, E.; González-Pacheco, H.; Bautista-Pérez, R.; Posadas-Sánchez, R.; Fragoso, J.M.; Vargas-Alarcón, G.; Pérez-Méndez, Ó. Trp Fluorescence Redshift during HDL Apolipoprotein Denaturation Is Increased in Patients with Coronary Syndrome in Acute Phase: A New Assay to Evaluate HDL Stability. Int. J. Mol. Sci. 2021, 22, 7819. [Google Scholar] [CrossRef]
- Tousoulis, D.; Plastiras, A.; Siasos, G.; Oikonomou, E.; Verveniotis, A.; Kokkou, E.; Maniatis, K.; Gouliopoulos, N.; Miliou, A.; Paraskevopoulos, T.; et al. Omega-3 PUFAs improved endothelial function and arterial stiffness with a parallel antiinflammatory effect in adults with metabolic syndrome. Atherosclerosis 2014, 232, 10–16. [Google Scholar] [CrossRef]
- Siniarski, A.; Haberka, M.; Mostowik, M.; Gołębiowska-Wiatrak, R.; Poręba, M.; Malinowski, K.P.; Gąsior, Z.; Konduracka, E.; Nessler, J.; Gajos, G. Treatment with omega-3 polyunsaturated fatty acids does not improve endothelial function in patients with type 2 diabetes and very high cardiovascular risk: A randomized, double-blind, placebo-controlled study (Omega-FMD). Atherosclerosis 2018, 271, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Sherratt, S.C.R.; Libby, P.; Budoff, M.J.; Bhatt, D.L.; Mason, R.P. Role of Omega-3 Fatty Acids in Cardiovascular Disease: The Debate Continues. Curr. Atheroscler. Rep. 2023, 25, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Khorshidi, M.; Sayyari, A.; Aryaeian, N.; Olang, B.; Alaei, M.; Khalili, M.; Hosseini, A.; Salehi, M. Effects of omega-3 supplementation on endothelial function, vascular structure, and metabolic parameters in adolescents with type 1 diabetes mellitus: A randomized clinical trial. Front. Nutr. 2022, 9, 962773. [Google Scholar] [CrossRef] [PubMed]
- Fabian, C.J.; Kimler, B.F.; Hursting, S.D. Omega-3 fatty acids for breast cancer prevention and survivorship. Breast Cancer Res. 2015, 17, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, J.; Shan, K.; Yang, Q.; Qi, Y.; Qu, H.; Li, J.; Wang, R.; Jia, L.; Chen, W.; Feng, N.; et al. Prostaglandin E3 attenuates macrophage-associated inflammation and prostate tumour growth by modulating polarization. J. Cell Mol. Med. 2021, 25, 5586–5601. [Google Scholar] [CrossRef]
- Endres, S.; Ghorbani, R.; Kelley, V.E.; Georgilis, K.; Lonnemann, G.; van der Meer, J.W.; Cannon, J.G.; Rogers, T.S.; Klempner, M.S.; Weber, P.C. The effect of dietary supplementation with n-3 polyunsaturated fatty acids on the synthesis of interleukin-1 and tumor necrosis factor by mononuclear cells. N. Engl. J. Med. 1989, 320, 265–271. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Sun, L.; Wen, W.; Qiu, M.; Luo, J.; Li, W.; Hao, S.; He, M.; Wu, J.; Hu, Y.; et al. Association between the ratio of serum eicosapentaenoic acid to arachidonic acid and risk of coronary artery disease in young Chinese patients. Front. Nutr. 2022, 9, 1019058. [Google Scholar] [CrossRef]
- Koivuniemi, A.; Sysi-Aho, M.; Orešič, M.; Ollila, S. Interfacial properties of high-density lipoprotein-like lipid droplets with different lipid and apolipoprotein A-I compositions. Biophys. J. 2013, 104, 2193–2201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, R.P.; Jacob, R.F.; Shrivastava, S.; Sherratt, S.C.R.; Chattopadhyay, A. Eicosapentaenoic acid reduces membrane fluidity, inhibits cholesterol domain formation, and normalizes bilayer width in atherosclerotic-like model membranes. Biochim. Biophys. Acta 2016, 1858, 3131–3140. [Google Scholar] [CrossRef] [Green Version]
- Bautista, R.; Carreón-Torres, E.; Luna-Luna, M.; Komera-Arenas, Y.; Franco, M.; Fragoso, J.M.; López-Olmos, V.; Cruz-Robles, D.; Vargas-Barrón, J.; Vargas-Alarcón, G.; et al. Early endothelial nitrosylation and increased abdominal adiposity in Wistar rats after long-term consumption of food fried in canola oil. Nutrition 2014, 30, 1055–1060. [Google Scholar] [CrossRef]
- James, G.; Bohannan, W.; Adewunmi, E.; Schmidt, K.; Park, H.G.; Shchepinov, M.S.; Agbaga, M.P.; Brenna, J.T. Pharmacokinetics and metabolism in mouse retina of bis-allylic deuterated docosahexaenoic acid (D-DHA), a new dry AMD drug candidate. Exp. Eye Res. 2022, 222, 109193. [Google Scholar] [CrossRef] [PubMed]
- Quintanilla-Cantú, A.; Peña-de-la-Sancha, P.; Flores-Castillo, C.; Mejía-Domínguez, A.M.; Posadas-Sánchez, R.; Pérez-Hernández, N.; Bautista-Pérez, R.; Enriquez-Calderón, R.E.; Juárez-Oropeza, M.A.; Fragoso, J.M.; et al. Small HDL subclasses become cholesterol-poor during postprandial period after a fat diet intake in subjects with high triglyceridemia increases. Clin. Chim. Acta 2017, 464, 98–105. [Google Scholar] [CrossRef]
- Estrada-Luna, D.; Martínez-Hinojosa, E.; Cancino-Diaz, J.C.; Belefant-Miller, H.; López-Rodríguez, G.; Betanzos-Cabrera, G. Daily supplementation with fresh pomegranate juice increases paraoxonase 1 expression and activity in mice fed a high-fat diet. Eur. J. Nutr. 2018, 57, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Johnston, D.T.; Deuster, P.A.; Harris, W.S.; Macrae, H.; Dretsch, M.N. Red blood cell omega-3 fatty acid levels and neurocognitive performance in deployed U.S. Servicemembers. Nutr. Neurosci. 2013, 16, 30–38. [Google Scholar] [CrossRef]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meléndez-Ramírez, G.; Pérez-Méndez, O.; López-Osorio, C.; Kuri-Alfaro, J.; Espinola-Zavaleta, N. Effect of the treatment with allopurinol on the endothelial function in patients with hyperuricemia. Endocr. Res. 2012, 37, 1–6. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Pre-n-3 | Post-n-3 | Pre-Placebo | Post-Placebo | |
|---|---|---|---|---|
| Age (years) | 42.5 ± 6.2 | |||
| SBP (mmHg) | 117.0 ± 8.2 | 115.8 ± 7.9 | 119.8 ± 8.0 | 115.9 ± 10.5 |
| DBP (mmHg) | 81.3 ± 4.2 | 80.4 ± 5.8 | 81.1 ± 4.0 | 81.1 ± 3.3 |
| Body fatty mass (%) | 30.6 ± 4.9 | 29.4 ± 4.0 * | 30.2 ± 4.7 | 29.6 ± 4.6 |
| Waist (cm) | 102.3 ± 10.2 | 98.9 ± 9.1 | 101.1 ± 9.5 | 99.4 ± 9.1 |
| BMI (kg/m2) | 30.9 ± 4.2 | 30.4 ± 3.9 * | 30.6 ± 4.2 | 30.4 ± 4.0 |
| Glucose (mg/dL) | 98.2 ± 13.1 | 97.8 ± 15.0 | 97.9 ± 12.6 | 100.0 ± 13.3 |
| Triglycerides (mg/dL) | 316.4 [257.3–633.9] | 235.3 [176.5–300.4] ** | 287.5 [206.6–418.4] | 261.7 [221.9–395.7] |
| Cholesterol (mg/dL) | 199.0 ± 39.1 | 215.9 ± 53.5 | 213.4 ± 67.7 | 206.8 ± 37.6 |
| Non-HDL-cholesterol (mg/dL) | 157.3 ± 42.0 | 170.2 ± 55.2 | 171.8 ± 69.0 | 164.9 ± 37.2 |
| HDL-cholesterol (mg/dL) | 41.8 ± 8.2 | 49.2 ± 10.5 * | 41.8 ± 9.3 | 42.3 ± 9.4 |
| HDL-phospholipids (mg/dL) | 56.2 ± 17.9 | 71.5 ± 21.3 * | 55.0 ± 17.8 | 55.3 ± 20.8 |
| HDL-triglycerides (mg/dL) | 11.2 [8.0–13.8] | 7.32 [5.3–10.9] ** | 10.9 [7.3–13.9] | 10.5 [8.5–12.9] |
| HDL Subclass * | Pre-n-3 | Post-n-3 | Pre-Placebo | Post-Placebo |
|---|---|---|---|---|
| HDL2b | 14.2 ± 9.6 | 15.5 ± 12.1 | 13.0 ± 9.9 | 13.5 ± 10.7 |
| HDL2a | 6.9 ± 2.3 | 7.4 ± 3.0 | 7.2 ± 3.1 | 6.9 ± 2.5 |
| HDL3a | 30.2 ± 6.2 | 29.9 ± 6.4 | 29.4 ± 8.8 | 31.9 ± 6.4 |
| HDL3b | 19.0 ± 5.3 | 18.9 ± 5.9 | 20.5 ± 4.6 | 20.4 ± 6.7 |
| HDL3c | 29.5 ± 11.2 | 28.3 ± 13.4 | 30.2 ± 12.7 | 27.2 ± 10.9 |
| Pre-n-3 | Post-n-3 | Δ | % Change | p * | |
|---|---|---|---|---|---|
| Saturated | |||||
| 14:0 | 0.61 ± 0.17 | 0.59 ± 0.21 | −0.02 | −3.3 | 0.08 |
| 16:0 | 23.55 ± 1.73 | 23.18 ± 1.03 | −0.37 | −1.7 | 0.766 |
| 18:0 | 10.03 ± 1.33 | 9.70 ± 0.99 | −0.33 | −3.3 | 0.337 |
| 20:0 | 0.24 ± 0.05 | 0.22 ± 0.06 | −0.02 | −8.3 | 0.328 |
| 22:0 | 0.88 ± 0.24 | 0.82 ± 0.23 | −0.06 | −6.8 | 0.388 |
| Monounsaturated | |||||
| 18:1 n-9 | 18.21 ± 2.34 | 17.29 ± 2.44 | −0.93 | −5.1 | 0.877 |
| 20:1 n-9 | 0.16 ± 0.03 | 0.15 ± 0.04 | −0.01 | −6.3 | 0.157 |
| 24:1 n-9 | 0.24 ± 0.08 | 0.27 ± 0.09 | 0.03 | 12.5 | 0.358 |
| Polyunsaturated | |||||
| n-3 | |||||
| 18:3 n-3 | 0.52 ± 0.14 | 0.59 ± 0.19 | 0.07 | 13.5 | 0.211 |
| 20:5 n-3 | 0.42 ± 0.28 | 0.97 ± 0.68 | 0.55 | 131.0 | 0.002 |
| 22:5 n-3 | 0.59 ± 0.11 | 0.73 ± 0.17 | 0.14 | 23.7 | 0.001 |
| 22:6 n-3 | 1.85 ± 0.60 | 2.99 ± 0.88 | 1.14 | 61.6 | 0.000 |
| n-6 | |||||
| 18:2 n-6 | 28.16 ± 2.98 | 28.87 ± 3.14 | 0.71 | 2.5 | 0.493 |
| 18:3 n-6 | 0.33 ± 0.11 | 0.31 ± 0.12 | −0.02 | −6.1 | 0.431 |
| 20:2 n-6 | 0.24 ± 0.06 | 0.26 ± 0.04 | 0.02 | 8.3 | 0.131 |
| 20:3 n-6 | 2.29 ± 0.48 | 2.00 ± 0.46 | −0.29 | −12.7 | 0.001 |
| 20:4 n-6 | 8.13 ± 1.55 | 7.82 ± 1.55 | −0.31 | −3.8 | 0.309 |
| 22:4 n-6 | 0.37 ± 0.11 | 0.25 ± 0.06 | −0.12 | −32.4 | 0.001 |
| 22:5 n-6 | 0.30 ± 0.08 | 0.23 ± 0.08 | −0.06 | −23.3 | 0.005 |
| Pre-n-3 | Post-n-3 | Pre-Placebo | Post-Placebo | |
|---|---|---|---|---|
| Diameter at rest (mm) | 4.30 ± 0.39 | 4.45 ± 0.42 | 4.23 ± 0.40 | 4.22 ± 0.51 |
| Diameter at 1 min (mm) | 4.72 ± 0.37 | 4.96 ± 0.47 * | 4.60 ± 0.47 | 4.61 ± 0.48 |
| FMD at 1 min (%) | 7.67 ± 2.88 | 10.80 ± 3.99 ** | 8.20 ± 4.38 | 8.58 ± 3.85 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña-de-la-Sancha, P.; Muñoz-García, A.; Espínola-Zavaleta, N.; Bautista-Pérez, R.; Mejía, A.M.; Luna-Luna, M.; López-Olmos, V.; Rodríguez-Pérez, J.-M.; Fragoso, J.-M.; Carreón-Torres, E.; et al. Eicosapentaenoic and Docosahexaenoic Acid Supplementation Increases HDL Content in n-3 Fatty Acids and Improves Endothelial Function in Hypertriglyceridemic Patients. Int. J. Mol. Sci. 2023, 24, 5390. https://doi.org/10.3390/ijms24065390
Peña-de-la-Sancha P, Muñoz-García A, Espínola-Zavaleta N, Bautista-Pérez R, Mejía AM, Luna-Luna M, López-Olmos V, Rodríguez-Pérez J-M, Fragoso J-M, Carreón-Torres E, et al. Eicosapentaenoic and Docosahexaenoic Acid Supplementation Increases HDL Content in n-3 Fatty Acids and Improves Endothelial Function in Hypertriglyceridemic Patients. International Journal of Molecular Sciences. 2023; 24(6):5390. https://doi.org/10.3390/ijms24065390
Chicago/Turabian StylePeña-de-la-Sancha, Paola, Adolfo Muñoz-García, Nilda Espínola-Zavaleta, Rocío Bautista-Pérez, Ana María Mejía, María Luna-Luna, Victoria López-Olmos, José-Manuel Rodríguez-Pérez, José-Manuel Fragoso, Elizabeth Carreón-Torres, and et al. 2023. "Eicosapentaenoic and Docosahexaenoic Acid Supplementation Increases HDL Content in n-3 Fatty Acids and Improves Endothelial Function in Hypertriglyceridemic Patients" International Journal of Molecular Sciences 24, no. 6: 5390. https://doi.org/10.3390/ijms24065390