
Effects of the Oral Angiotensin II Type 2 Receptor Agonist C21 in Sugen-Hypoxia Induced Pulmonary Hypertension in Rats

Abstract
:1. Introduction
2. Results
2.1. Hemodynamic Assessments by Echocardiography on Day 0, Day 21, and Day 56
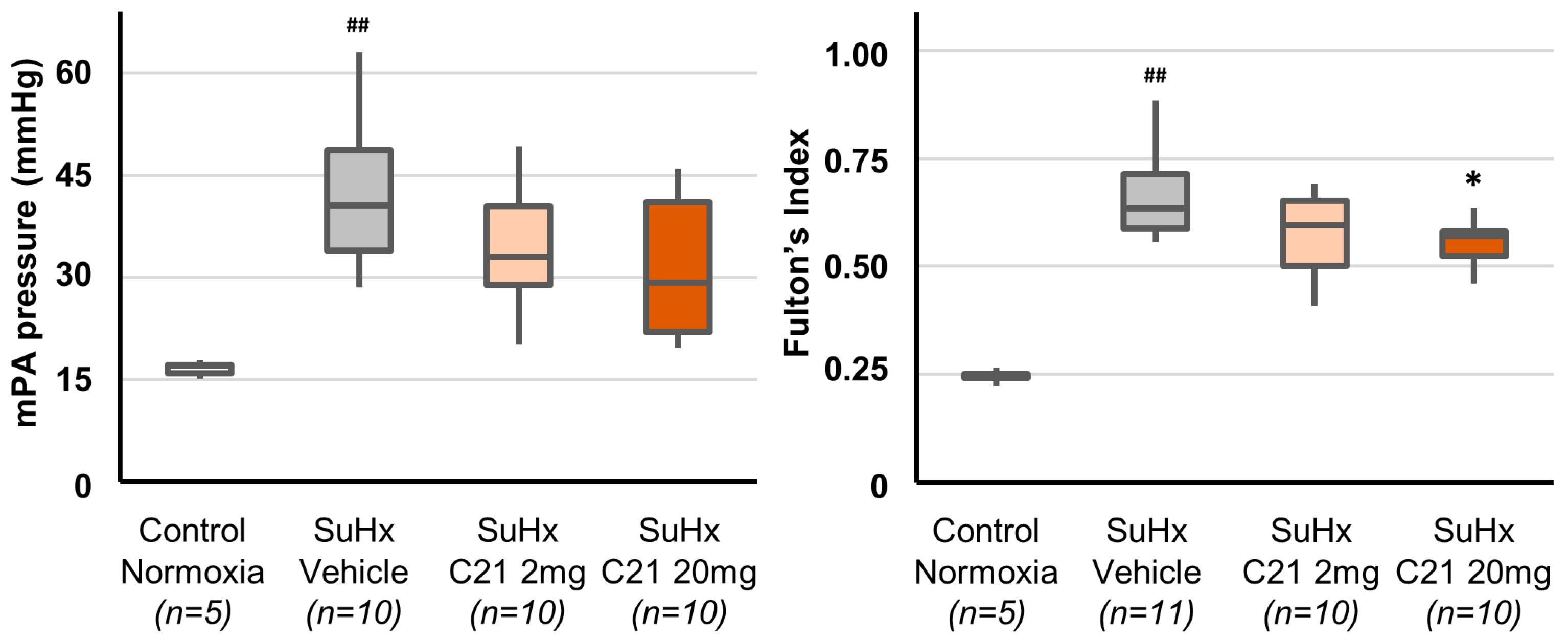
2.2. Hemodynamic Assessments by Catheterization on Day 56
2.3. Right Ventricle Hypertrophy
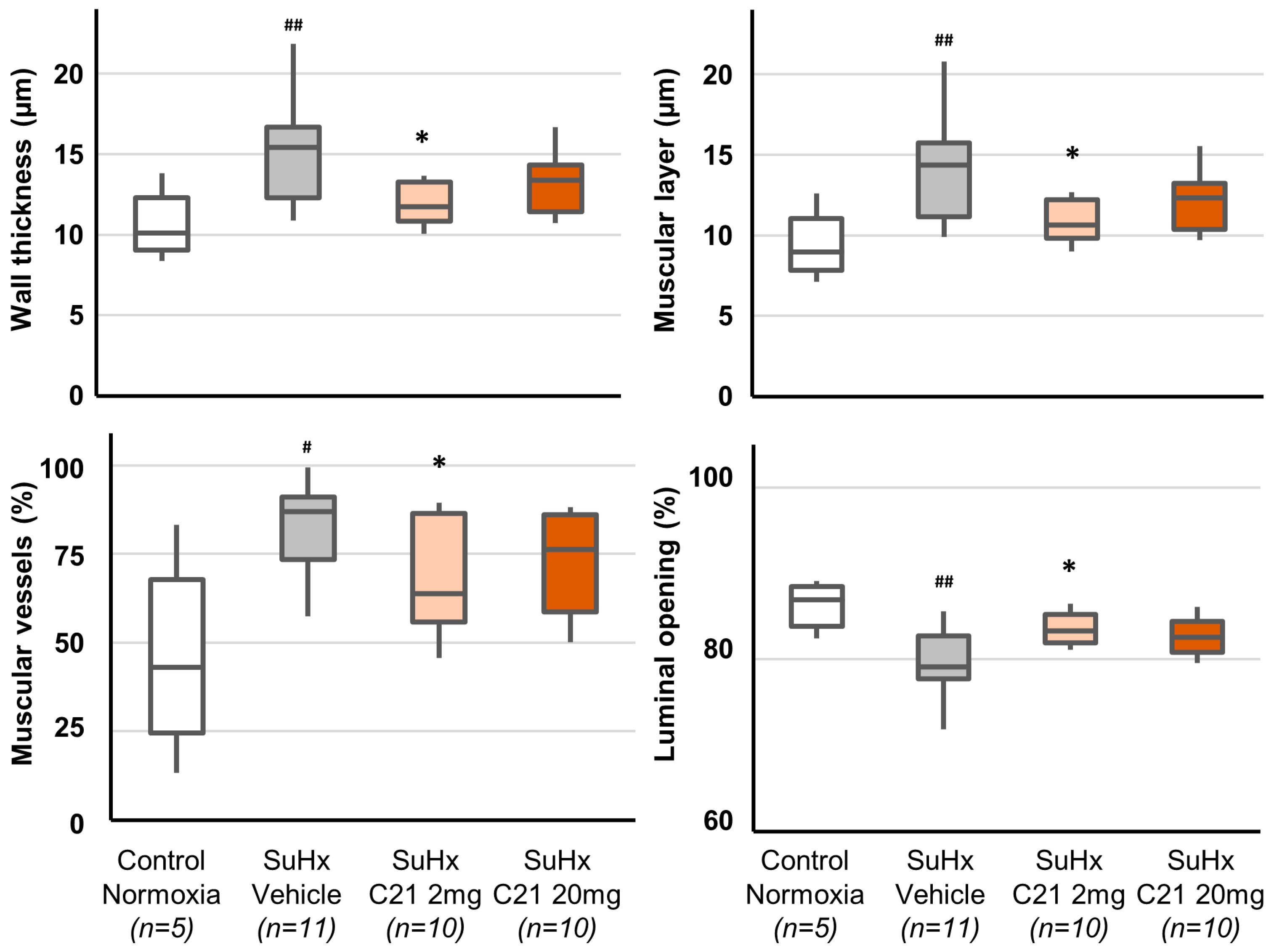
2.4. Vascular Remodeling
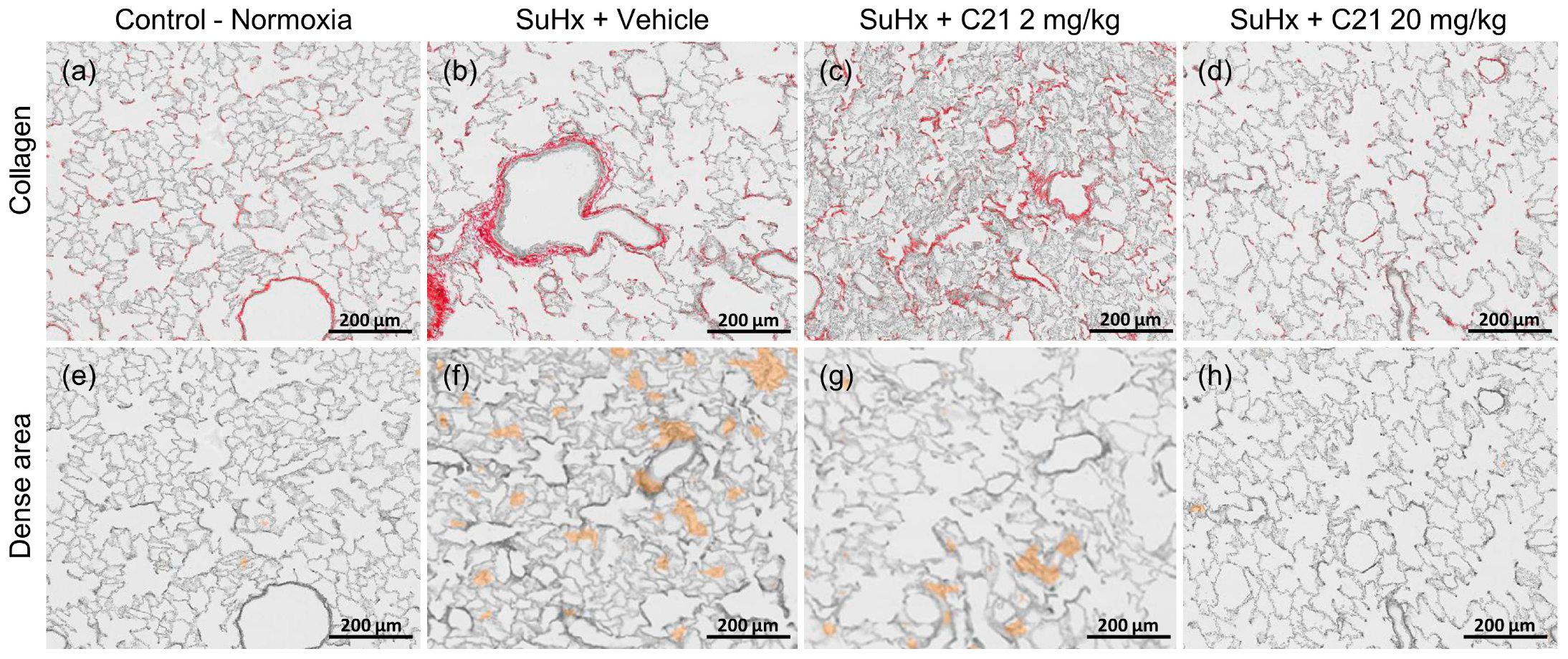
2.5. Collagen Deposition and Dense Areas in the Lungs
3. Discussion
4. Materials and Methods
4.1. Animals and Treatments
4.2. Hemodynamic Measurements
4.3. Tissue Sampling and Histology
4.4. Quantification of Lung Hydroxyproline Content
4.5. Statistics
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | Group | RVWT (mm) | PAD (cm) | HR (bpm) | Vmax (cm/s) | VTI (cm) | PAAT (ms) | ET (ms) | CO (mL/min) | SV (mL) |
|---|---|---|---|---|---|---|---|---|---|---|
| Day 0 | All (n = 45) | 0.44 [0.44;0.53] | 0.24 [023;0.24] | 377 [361;396] | 84.5 [81.7;88.8] | 5.20 [5.08;5.42] | 29.6 [22.2;29.6] | 81 [74;89] | 85.9 [81.9;89.7] | 0.23 [0.22;0.24] |
| Day 21 | Control-Normoxia (n = 5) | 0.50 [0.44;0.53] | 0.24 [0.24;0.25] | 355 [345;361] | 95.8 [92.5;96.5] | 5.42 [5.29;5.79] | 29.6 [29.4;29.6] | 81 [81;81] | 87.1 [86.8;89.9] | 0.25 [0.24;0.26] |
| SuHx (n = 37) | 1.13 ### [0.98;1.20] | 0.25 # [0.24;0.26] | 338 [323;353] | 61.3 ### [58.0;66.5] | 3.26 ### [2.83;3.64] | 18.4 ## [14.8;22.2] | 81 [77;84] | 55.5 ### [46.5;62.3] | 0.16 ### [0.14;0.18] | |
| Day 56 | Control-Normoxia (n = 5) | 0.53 [0.53;0.53] | 0.25 [0.25;0.25] | 312 [306;338] | 93.7 [92.3;95.1] | 5.56 [5.52;5.86] | 37.0 [37.0;37.0] | 96 [89;96] | 93.9 [85.1;95.2] | 0.27 [0.27;0.29] |
| SuHx and Vehicle (n = 11) | 1.24 ## [1.20;1.29] | 0.25 [0.24;0.25] | 306 [306;328] | 66.2 ## [60.5;71.5] | 3.58 ## [3.18;3.74] | 22.2 ## [22.2;22.2] | 89 [81;89] | 53.7 ## [47.2;58.0] | 0.16 ## [0.15;0.18] | |
| SuHx and 2 mg/kg C21 (n = 10) | 1.11 [0.98;1.31] | 0.25 [0.25;0.26] | 328 [301;343] | 65.8 [57.7;68.8] | 3.83 [3.21;4.44] | 25.9 [16.6;29.6] | 93 [89;96] | 62.7 [53.6;70.5] | 0.18 [0.16;0.22] | |
| SuHx and 20 mg/kg C21 (n = 11) | 1.06 [1.02;1.38] | 0.25 * [0.25;0.26] | 325 [304;345] | 71.1 [65.1;78.5] | 4.01 [3.56;4.53] | 22.2 [22.2;25.9] | 89 [81;96] | 66.8 * [55.5;74.3] | 0.21 * [0.18:0.23] | |
| SuHx and All C21 (n = 21) | 1.06 [0.98;1.33] | 0.25 § [0.25;0.26] | 325 [301;345] | 68.3 [61.3;76.1] | 4.01 [3.46;4.51] | 22.2 [22.2;29.6] | 89 [81;96] | 65.5 § [54.6;73.7] | 0.20 § [0.16;0.22] |
| Control Normoxia (n = 5) | SuHx Vehicle (n = 11) | SuHx C21 2 mg/kg (n = 10) | SuHx C21 20 mg/kg (n = 10) | SuHx All C 21 (n = 20) | |
|---|---|---|---|---|---|
| Saturation (%) | 98 (96;98) | 94 (91;96) # | 97 (94;97) | 96 (93;98) | 97 (94;98) § |
| Arterial pressure (mmHg) | |||||
| Diastolic | 95.5 [68.2;110.5] | 93.5 [72.5;104.4] | 104.2 [79.4;112.4] | 103.2 [85.7;118.3] | 103.2 [81.9;1116.1] |
| Systolic | 126.9 [93.5;141.1] | 116.9 [101.3;134.1] | 133.5 [108.6;146.9] | 130.9 [113.9;147.3] | 130.9 [112.9;145.9] |
| Mean | 106.0 [76.6;120.7] | 102.0 [82.1;114.6] | 114.6 [89.1;122.4] | 112.9 [95.1;128.5] | 112.9 [92.3;126.1] |
| Right ventricular pressure (mmHg) | |||||
| Diastolic | 3.8 [3.6:5.1] | 4.3 [3.2;5.2] | 2.5 [1.5;4.0] | 2.4 [1.3;4.0] | 2.5 [1.4;3.9] § |
| Systolic | 22.4 [21.3;24.5] | 62.0 [46.3;82.3] ## | 50.3 [43.7;58.9] | 48.4 [32.3;63.0] | 49.5 [41.0;61.4] |
| Mean | 10.3 [9.9;11.0] | 24.0 [18.3;30.4] ## | 18.8 [16.1;22.0] | 17.4 [12.0;24.8] | 17.9 [14.4;22.9] § |
| Pulmonary artery pressure (mmHg) | |||||
| Diastolic | 13.4 [12.4;14.2] | 28.4 [24.5;33.3] ## | 24.7 [17.1;31.7] | 20.1 [14.1;30.7] | 22.6 [15.3;31.0] § |
| Systolic | 23.2 [21.7;24.8] | 65.0 [47.2;83.9] ## | 51.6 [44.0;61.6] | 47.3 [32.6;62.8] | 49.0 [41.7;61.8] |
| Mean | 17.1 [15.5;17.5] | 40.6 [32.8;50.0] ## | 33.0 [26.9;42.5] | 29.2 [21.4;41.7] | 30.5 [22.3;41.9] § |
| Control Normoxia (n = 5) | SuHx Vehicle (n = 11) | SuHx C21 2 mg/kg (n = 10) | SuHx C21 20 mg/kg (n = 10) | SuHx All C21 (n = 20) | |
|---|---|---|---|---|---|
| vWF Area (%) | 1.22 [1.17;1.72] | 1.94 [1.87;2.62] ## | 1.90 [1.76;2.03] | 1.75 [1.69;1.89] * | 1.85 [1.70;2.03] |
| Vessel Wall (µm) | |||||
| Small vessels | 5.87 [5.00;5.98] | 7.40 [6.78;7.76] ## | 6.88 [6.44;7.10] | 7.01 [6.41;7.31] | 6.93 [6.46;7.21] § |
| Medium vessels | 8.20 [7.93;9.40] | 12.17 [10.84;13.15] ## | 10.99 [10.34;11.47] | 11.15 [10.52;12.13] | 10.99 [10.47;12.01] § |
| Large vessels | 10.11 [9.05;12.28] | 15.42 [12.28;16.68] ## | 11.75 [10.83;13.28] * | 13.39 [11.42;14.33] | 12.42 [10.92;13.68] § |
| Endothelial Layer (µm) | |||||
| Small vessels | 0.88 [0.86;0.90] | 0.79 [0.78;0.85] ## | 0.82 [0.78;0.84] | 0.83 [0.80;0.87] | 0.83 [0.80;0.86] |
| Medium vessels | 1.03 [0.96;1.07] | 0.84 [0.82;0.87] ## | 0.86 [0.82;0.89] | 0.90 [0.85;0.96] | 0.88 [0.83;0.91] |
| Large vessels | 1.23 [1.19;1.23] | 1.05 [1.00;1.08] ## | 1.06 [1.00;1.12] | 1.07 [1.03;1.14] | 1,06 [1.03;1.13] |
| Muscular Layer (µm) | |||||
| Small vessels | 4.98 [4.13;5.09] | 6.65 [5.92;6.98] ## | 6.05 [5.63;6.29] | 6.13 [5.59;6.51] | 6.06 [5.64;6.41] § |
| Medium vessels | 7.25 [6.89;8.38] | 11.33 [10.02;12.32] ## | 10.15 [9.45;10.66] | 10.22 [9.56;11.30] | 10.15 [9.56;11.16] § |
| Large vessels | 8.95 [7.82;11.06] | 14.37 [11.14;15.75] ## | 10.66 [9.83;12.22] * | 12.32 [10.38;13.24] | 11.33 [9.88;12.64] §§ |
| Muscular Vessels (%) | |||||
| Small vessels | 1.2 [0.4;2.0] | 17.6 [12.6;22.3] ## | 13.3 [10.9;16.3] | 15.1 [10.2;17.7] | 14.1 [11.2;17.0] § |
| Medium vessels | 11.1 [8.2;33.3] | 65.9 [54.7;74.2] ## | 56.4 [50.8;62.3] | 63.1 [53.9;72.7] | 57.9 [52.0;740.5] |
| Large vessels | 43.1 [24.5;67.8] | 87.0 [73.4;91.1] # | 63.9 [55.9;86.3] * | 76.2 [58.7;86.0] | 65.2 [57.7;85.7] § |
| Luminal Opening (%) | |||||
| Small vessels | 65.5 [65.0;69.5] | 58.4 [56.8;61.1] ## | 60.6 [59.6;62.3] | 59.9 [58.4;62.6] | 60.2 [59.1;62.1] § |
| Medium vessels | 75.5 [72.4;76.8] | 65.5 [62.1;67.2] ## | 67.9 [66.7;69.2] | 67.6 [65.2;69.3] | 67.9 [65.6;69.0] § |
| Large vessels | 86.9 [83.9;88.4] | 79.1 [77.8;82.8] ## | 83.3 [81.9;85.2] * | 82.6 [80.8;84.4] | 82.9 [81.5;85.0] §§ |
| Non-obliterated Vessels (%) | |||||
| Small vessels | 80.0 [76.2;91.8] | 43.5 [36.1;55.8] ## | 54.1 [49.1;59.5] | 51.1 [46.6;64.7] | 52.1 [47.5;62.1] § |
| Medium vessels | 98.9 [94.2;99.8] | 68.7 [59.4;72.8] ## | 76.3 [72.7;80.6] | 77.7 [72.5;84.3] * | 76.8 [72.9;81.6] §§ |
| Large vessels | 100.0 [100.0;100.0] | 98.8 [94.3;100.0] | 99.6 [98.7;100.0] | 100.0 [99.1;100.0] | 100 [99.1;100.0] |
| Semi-obliterated Vessels (%) | |||||
| Small vessels | 19.5 [8.2;23.0] | 42.0 [37.5;52.7] ## | 39.2 [34.4;42.1] | 40.6 [29.7;46.4] | 40.3 [32.6;43.7] |
| Medium vessels | 1.1 [0.2;5.3] | 23.4 [19.8;27.8] ## | 17.2 [15.4;20.4] | 15.6 [12.5;20.3] * | 17.2 [14.0;19.6] §§ |
| Large vessels | 0.0 [0.0;0.0] | 1.2 [0.0;3.9] | 0.4 [0.0;1.3] | 0.0 [0.0;0.9] | 0.0 [0.0;0.9] |
| Obliterated Vessels (%) | |||||
| Small vessels | 0.4 [0.0;0.8] | 8.8 [6.7;12.3] ## | 6.4 [5.8;9.5] | 7.9 [4.3;10.0] | 7.1 [5.4:9.8] |
| Medium vessels | 0.0 [0.0;0.4] | 7.1 [6.0;11.6] ## | 5.0 [4.0;9.3] | 4.0 [3.1;6.5] | 4.7 [3.4;8.1] § |
| Large vessels | 0.0 [0.0;0.0] | 0.0 [0.0;0.0] | 0.0 [0.0;0.0] | 0.0 [0.0;0.0] | 0.0 [0.0;0.0] |
| Control Normoxia (n = 5) | SuHx Vehicle (n = 11) | SuHx C21 2 mg/kg (n = 10) | SuHx C21 20 mg/kg (n = 10) | SuHx All C 21 (n = 20) | |
|---|---|---|---|---|---|
| Fulton’s index | 0.24 [0.23;0.26] | 0.63 [0.58;0.72] ## | 0.60 [0.49;0.65] | 0.57 [0.51;0.59] * | 0.57 [0.50;0.64] § |
| Left ventricular weight (g) | 1.14 [1.03;1.28] | 1.09 [1.01;1.20] | 1.20 [1.06;1.32] | 1.16 [1.04;1.19] | 1.17 [1.05;1.23] |
| Right ventricular weight (g) | 0.28 [0.26;0.30] | 0.74 [0.64;0.81] ## | 0.67 [0.59;0.75] | 0.59 [0.54;0.74] | 0.63 [0.56;0.74] |
| Right ventricle collagen (mg) | 2.06 [1.79;2.24] | 4.90 [3.66;5.31] ## | 4.18 [3.72;4.76] | 4.05 [3.28;5.20] | 4.18 [3.72;4.76] |
| Vascular Remodeling | rho | Hemodynamic Parameters | rho |
|---|---|---|---|
| VWF Area (%) | 0.411 * | Saturation (%) | −0.299 |
| Vessel wall thickness (µm) | Systemic arterial pressure (mmHg) | ||
| Small vessels | 0.434 * | Diastolic | −0.163 |
| Medium vessels | 0.480 ** | Systolic | −0.237 |
| Large vessels | 0.432 * | Mean | −0.209 |
| Endothelial layer (µm) | Right ventricular pressure (mmHg) | ||
| Small vessels | −0.204 | Diastolic | 0.341 |
| Medium vessels | −0.292 | Systolic | 0.455 * |
| Large vessels | −0.193 | Mean | 0.501 ** |
| Muscle layer (µm) | Pulmonary artery pressure (mmHg) | ||
| Small vessels | 0.450 * | Diastolic | 0.475 ** |
| Medium vessels | 0.504 ** | Systolic | 0.439 * |
| Large vessels | 0.444 * | Mean | 0.485 ** |
| Luminal opening (%) | Stroke volume (mL) | −0.560 ** | |
| Small vessels | −0.477 ** | Vmax (cm/s) | −0.630 *** |
| Medium vessels | −0.529 ** | Cardiac output (mL/min) | −0.537 ** |
| Large vessels | −0.471 ** | Stroke volume (mL) | −0.560 ** |
| Obliterated vessels (%) | |||
| Small vessels | 0.598 *** | ||
| Medium vessels | 0.420 * | ||
| Large vessels | 0.354 |
References
- Hoeper, M.M.; Humbert, M.; Souza, R.; Idrees, M.; Kawut, S.M.; Sliwa-Hahnle, K.; Jing, Z.C.; Gibbs, J.S. A global view of pulmonary hypertension. Lancet Respir. Med. 2016, 4, 306–322. [Google Scholar] [CrossRef] [PubMed]
- Hoeper, M.M.; Humbert, M. The new haemodynamic definition of pulmonary hypertension: Evidence prevails, finally! Eur. Respir. J. 2019, 53, 1900038. [Google Scholar] [CrossRef]
- Galie, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [CrossRef] [PubMed]
- Humbert, M.; Guignabert, C.; Bonnet, S.; Dorfmuller, P.; Klinger, J.R.; Nicolls, M.R.; Olschewski, A.J.; Pullamsetti, S.S.; Schermuly, R.T.; Stenmark, K.R.; et al. Pathology and pathobiology of pulmonary hypertension: State of the art and research perspectives. Eur. Respir. J. 2019, 53, 1801887. [Google Scholar] [CrossRef]
- Tuder, R.M.; Marecki, J.C.; Richter, A.; Fijalkowska, I.; Flores, S. Pathology of pulmonary hypertension. Clin. Chest Med. 2007, 28, 23–42. [Google Scholar] [CrossRef] [PubMed]
- Dotan, Y.; Stewart, J.; Gangemi, A.; Wang, H.; Aneja, A.; Chakraborty, B.; Dass, C.; Zhao, H.; Marchetti, N.; D’Alonzo, G.; et al. Pulmonary vasculopathy in explanted lungs from patients with interstitial lung disease undergoing lung transplantation. BMJ Open Respir. Res. 2020, 7, e000532. [Google Scholar] [CrossRef]
- Waxman, A.; Restrepo-Jaramillo, R.; Thenappan, T.; Ravichandran, A.; Engel, P.; Bajwa, A.; Allen, R.; Feldman, J.; Argula, R.; Smith, P.; et al. Inhaled Treprostinil in Pulmonary Hypertension Due to Interstitial Lung Disease. N. Engl. J. Med. 2021, 384, 325–334. [Google Scholar] [CrossRef]
- Lee, J.; Song, J.U. The Clinical Efficacy of Pulmonary Hypertension-Specific Agents in Idiopathic Pulmonary Fibrosis: Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials. J. Korean Med. Sci. 2020, 35, e48. [Google Scholar] [CrossRef]
- Rajagopal, K.; Bryant, A.J.; Sahay, S.; Wareing, N.; Zhou, Y.; Pandit, L.M.; Karmouty-Quintana, H. Idiopathic pulmonary fibrosis and pulmonary hypertension: Heracles meets the Hydra. Br. J. Pharmacol. 2021, 178, 172–186. [Google Scholar] [CrossRef]
- Maron, B.A.; Leopold, J.A. The role of the renin-angiotensin-aldosterone system in the pathobiology of pulmonary arterial hypertension (2013 Grover Conference series). Pulm. Circ. 2014, 4, 200–210. [Google Scholar] [CrossRef] [PubMed]
- de Man, F.S.; Tu, L.; Handoko, M.L.; Rain, S.; Ruiter, G.; Francois, C.; Schalij, I.; Dorfmuller, P.; Simonneau, G.; Fadel, E.; et al. Dysregulated renin-angiotensin-aldosterone system contributes to pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 2012, 186, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumi, Y.; Matsubara, H.; Ohkubo, N.; Mori, Y.; Nozawa, Y.; Murasawa, S.; Kijima, K.; Maruyama, K.; Masaki, H.; Moriguchi, Y.; et al. Angiotensin II type 2 receptor is upregulated in human heart with interstitial fibrosis, and cardiac fibroblasts are the major cell type for its expression. Circ. Res. 1998, 83, 1035–1046. [Google Scholar] [CrossRef] [PubMed]
- Wagenaar, G.T.; Laghmani El, H.; Fidder, M.; Sengers, R.M.; de Visser, Y.P.; de Vries, L.; Rink, R.; Roks, A.J.; Folkerts, G.; Walther, F.J. Agonists of MAS oncogene and angiotensin II type 2 receptors attenuate cardiopulmonary disease in rats with neonatal hyperoxia-induced lung injury. Am. J. Physiol. Cell Mol. Physiol. 2013, 305, L341–L351. [Google Scholar] [CrossRef] [PubMed]
- Matavelli, L.C.; Siragy, H.M. AT2 receptor activities and pathophysiological implications. J. Cardiovasc. Pharmacol. 2015, 65, 226–232. [Google Scholar] [CrossRef]
- Sumners, C.; de Kloet, A.D.; Krause, E.G.; Unger, T.; Steckelings, U.M. Angiotensin type 2 receptors: Blood pressure regulation and end organ damage. Curr. Opin. Pharmacol. 2015, 21, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Barber, M.N.; Sampey, D.B.; Widdop, R.E. AT(2) receptor stimulation enhances antihypertensive effect of AT(1) receptor antagonist in hypertensive rats. Hypertension 1999, 34, 1112–1116. [Google Scholar] [CrossRef]
- Ferreira, A.J.; Shenoy, V.; Yamazato, Y.; Sriramula, S.; Francis, J.; Yuan, L.; Castellano, R.K.; Ostrov, D.A.; Oh, S.P.; Katovich, M.J.; et al. Evidence for angiotensin-converting enzyme 2 as a therapeutic target for the prevention of pulmonary hypertension. Am. J. Respir. Crit. Care Med. 2009, 179, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, V.; Kwon, K.C.; Rathinasabapathy, A.; Lin, S.; Jin, G.; Song, C.; Shil, P.; Nair, A.; Qi, Y.; Li, Q.; et al. Oral delivery of Angiotensin-converting enzyme 2 and Angiotensin-(1-7) bioencapsulated in plant cells attenuates pulmonary hypertension. Hypertension 2014, 64, 1248–1259. [Google Scholar] [CrossRef]
- Breitling, S.; Krauszman, A.; Parihar, R.; Walther, T.; Friedberg, M.K.; Kuebler, W.M. Dose-dependent, therapeutic potential of angiotensin-(1-7) for the treatment of pulmonary arterial hypertension. Pulm. Circ. 2015, 5, 649–657. [Google Scholar] [CrossRef]
- Rathinasabapathy, A.; Bryant, A.J.; Suzuki, T.; Moore, C.; Shay, S.; Gladson, S.; West, J.D.; Carrier, E.J. rhACE2 Therapy Modifies Bleomycin-Induced Pulmonary Hypertension via Rescue of Vascular Remodeling. Front. Physiol. 2018, 9, 271. [Google Scholar] [CrossRef]
- Santos, R.A.; Simoes e Silva, A.C.; Maric, C.; Silva, D.M.; Machado, R.P.; de Buhr, I.; Heringer-Walther, S.; Pinheiro, S.V.; Lopes, M.T.; Bader, M.; et al. Angiotensin-(1-7) is an endogenous ligand for the G protein-coupled receptor Mas. Proc. Natl. Acad. Sci. USA 2003, 100, 8258–8263. [Google Scholar] [CrossRef] [PubMed]
- Bosnyak, S.; Jones, E.S.; Christopoulos, A.; Aguilar, M.I.; Thomas, W.G.; Widdop, R.E. Relative affinity of angiotensin peptides and novel ligands at AT1 and AT2 receptors. Clin. Sci. 2011, 121, 297–303. [Google Scholar] [CrossRef]
- Steckelings, U.M.; Widdop, R.E.; Sturrock, E.D.; Lubbe, L.; Hussain, T.; Kaschina, E.; Unger, T.; Hallberg, A.; Carey, R.M.; Sumners, C. The Angiotensin AT2 Receptor: From a Binding Site to a Novel Therapeutic Target. Pharmacol. Rev. 2022, 74, 1051–1135. [Google Scholar] [CrossRef] [PubMed]
- Raud, J. (VicorePharma AB, Stockholm, Sweden). Unpublished work. 2022. [Google Scholar]
- Tornling, G.; Batta, R.; Porter, J.C.; Williams, B.; Bengtsson, T.; Parmar, K.; Kashiva, R.; Hallberg, A.; Cohrt, A.K.; Westergaard, K.; et al. Seven days treatment with the angiotensin II type 2 receptor agonist C21 in hospitalized COVID-19 patients; a placebo-controlled randomised multi-centre double-blind phase 2 trial. EClinicalMedicine 2021, 41, 101152. [Google Scholar] [CrossRef]
- VicorePharma. Safety, Efficacy and Pharmacokinetics of C21 in Subjects With IPF. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04533022 (accessed on 28 October 2022).
- Bruce, E.; Shenoy, V.; Rathinasabapathy, A.; Espejo, A.; Horowitz, A.; Oswalt, A.; Francis, J.; Nair, A.; Unger, T.; Raizada, M.K.; et al. Selective activation of angiotensin AT2 receptors attenuates progression of pulmonary hypertension and inhibits cardiopulmonary fibrosis. Br. J. Pharmacol. 2015, 172, 2219–2231. [Google Scholar] [CrossRef] [PubMed]
- Rathinasabapathy, A.; Horowitz, A.; Horton, K.; Kumar, A.; Gladson, S.; Unger, T.; Martinez, D.; Bedse, G.; West, J.; Raizada, M.K.; et al. The Selective Angiotensin II Type 2 Receptor Agonist, Compound 21, Attenuates the Progression of Lung Fibrosis and Pulmonary Hypertension in an Experimental Model of Bleomycin-Induced Lung Injury. Front. Physiol. 2018, 9, 180. [Google Scholar] [CrossRef]
- Abe, K.; Toba, M.; Alzoubi, A.; Ito, M.; Fagan, K.A.; Cool, C.D.; Voelkel, N.F.; McMurtry, I.F.; Oka, M. Formation of plexiform lesions in experimental severe pulmonary arterial hypertension. Circulation 2010, 121, 2747–2754. [Google Scholar] [CrossRef]
- Colvin, K.L.; Yeager, M.E. Animal Models of Pulmonary Hypertension: Matching Disease Mechanisms to Etiology of the Human Disease. J. Pulm. Respir. Med. 2014, 4, 198. [Google Scholar] [CrossRef]
- Derrett-Smith, E.C.; Dooley, A.; Gilbane, A.J.; Trinder, S.L.; Khan, K.; Baliga, R.; Holmes, A.M.; Hobbs, A.J.; Abraham, D.; Denton, C.P. Endothelial injury in a transforming growth factor beta-dependent mouse model of scleroderma induces pulmonary arterial hypertension. Arthritis Rheum. 2013, 65, 2928–2939. [Google Scholar] [CrossRef]
- Farkas, L.; Gauldie, J.; Voelkel, N.F.; Kolb, M. Pulmonary hypertension and idiopathic pulmonary fibrosis: A tale of angiogenesis, apoptosis, and growth factors. Am. J. Respir. Cell Mol. Biol. 2011, 45, 1–15. [Google Scholar] [CrossRef]
- Derrett-Smith, E.; Clark, K.E.N.; Shiwen, X.; Abraham, D.J.; Hoyles, R.K.; Lacombe, O.; Broqua, P.; Junien, J.L.; Konstantinova, I.; Ong, V.H.; et al. The pan-PPAR agonist lanifibranor reduces development of lung fibrosis and attenuates cardiorespiratory manifestations in a transgenic mouse model of systemic sclerosis. Arthritis Res. Ther. 2021, 23, 234. [Google Scholar] [CrossRef] [PubMed]
- Denton, C.P.; Spierings, J. Combining Data Sets as Well as Therapies Shows Improved Outcome in Connective Tissue Disease-Associated Pulmonary Hypertension. Arthritis Rheumatol. 2021, 73, 725–727. [Google Scholar] [CrossRef] [PubMed]
- Khanna, D.; Zhao, C.; Saggar, R.; Mathai, S.C.; Chung, L.; Coghlan, J.G.; Shah, M.; Hartney, J.; McLaughlin, V. Long-Term Outcomes in Patients With Connective Tissue Disease-Associated Pulmonary Arterial Hypertension in the Modern Treatment Era: Meta-Analyses of Randomized, Controlled Trials and Observational Registries. Arthritis Rheumatol. 2021, 73, 837–847. [Google Scholar] [CrossRef]
- Blagojevic, J.; Abignano, G.; Avouac, J.; Cometi, L.; Frerix, M.; Bellando-Randone, S.; Guiducci, S.; Bruni, C.; Huscher, D.; Jaeger, V.K.; et al. Use of vasoactive/vasodilating drugs for systemic sclerosis (SSc)-related digital ulcers (DUs) in expert tertiary centres: Results from the analysis of the observational real-life DeSScipher study. Clin. Rheumatol. 2020, 39, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Jaeger, V.K.; Wirz, E.G.; Allanore, Y.; Rossbach, P.; Riemekasten, G.; Hachulla, E.; Distler, O.; Airo, P.; Carreira, P.E.; Balbir Gurman, A.; et al. Incidences and Risk Factors of Organ Manifestations in the Early Course of Systemic Sclerosis: A Longitudinal EUSTAR Study. PLoS ONE 2016, 11, e0163894. [Google Scholar] [CrossRef] [PubMed]
- Puchtler, H.; Waldrop, F.S.; Valentine, L.S. Polarization microscopic studies of connective tissue stained with picro-sirius red FBA. Beitr. Pathol. 1973, 150, 174–187. [Google Scholar] [CrossRef]
- Gilhodes, J.C.; Jule, Y.; Kreuz, S.; Stierstorfer, B.; Stiller, D.; Wollin, L. Quantification of Pulmonary Fibrosis in a Bleomycin Mouse Model Using Automated Histological Image Analysis. PLoS ONE 2017, 12, e0170561. [Google Scholar] [CrossRef]
- Testa, L.C.; Jule, Y.; Lundh, L.; Bertotti, K.; Merideth, M.A.; O’Brien, K.J.; Nathan, S.D.; Venuto, D.C.; El-Chemaly, S.; Malicdan, M.C.V.; et al. Automated Digital Quantification of Pulmonary Fibrosis in Human Histopathology Specimens. Front. Med. 2021, 8, 607720. [Google Scholar] [CrossRef]


| Control Normoxia (n = 5) | SuHx Vehicle (n = 11) | SuHx C21 2 mg/kg (n = 10) | SuHx C21 20 mg/kg (n = 10) | |
|---|---|---|---|---|
| Collagen content [%] | 5.21 [5.08;5.57] | 6.27 [5.75;7.34] # | 6.39 [6.04;7.22] | 5.19 [4.92;5.41] **,§§§ |
| Dense area [%] | 2.63 [2.08;2.84] | 4.81 [3.76;5.96] ## | 4.65 [4.44;6.33] | 3.01 [2.66;4.37] *,§§ |
| Hydroxyproline [μm/mg tissue] | 60 [51;74] | 64 [57;81] | 55 [51;68] | 63 [58;70] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tornling, G.; Batta, R.; Salvail, D.; Raud, J.; Denton, C.P. Effects of the Oral Angiotensin II Type 2 Receptor Agonist C21 in Sugen-Hypoxia Induced Pulmonary Hypertension in Rats. Int. J. Mol. Sci. 2023, 24, 7478. https://doi.org/10.3390/ijms24087478
Tornling G, Batta R, Salvail D, Raud J, Denton CP. Effects of the Oral Angiotensin II Type 2 Receptor Agonist C21 in Sugen-Hypoxia Induced Pulmonary Hypertension in Rats. International Journal of Molecular Sciences. 2023; 24(8):7478. https://doi.org/10.3390/ijms24087478
Chicago/Turabian StyleTornling, Göran, Rohit Batta, Dan Salvail, Johan Raud, and Christopher P. Denton. 2023. "Effects of the Oral Angiotensin II Type 2 Receptor Agonist C21 in Sugen-Hypoxia Induced Pulmonary Hypertension in Rats" International Journal of Molecular Sciences 24, no. 8: 7478. https://doi.org/10.3390/ijms24087478