

Common Clinical and Molecular Pathways between Migraine and Sarcoidosis


 ,
, 
 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Epidemiological Impact of Migraine and Sarcoidosis
2.1. Burden of Migraine in Terms of Work Loss and Impaired Quality of Life and Functioning
2.2. Burden of Sarcoidosis and Headache-Related Pain
3. Headache in Migraine versus Sarcoidosis
3.1. Characteristics of Migraine
3.2. Migraine in Patients with Sarcoidosis
3.3. Headache as Clinical Manifestation of NS
4. Imaging Diagnosis of NS
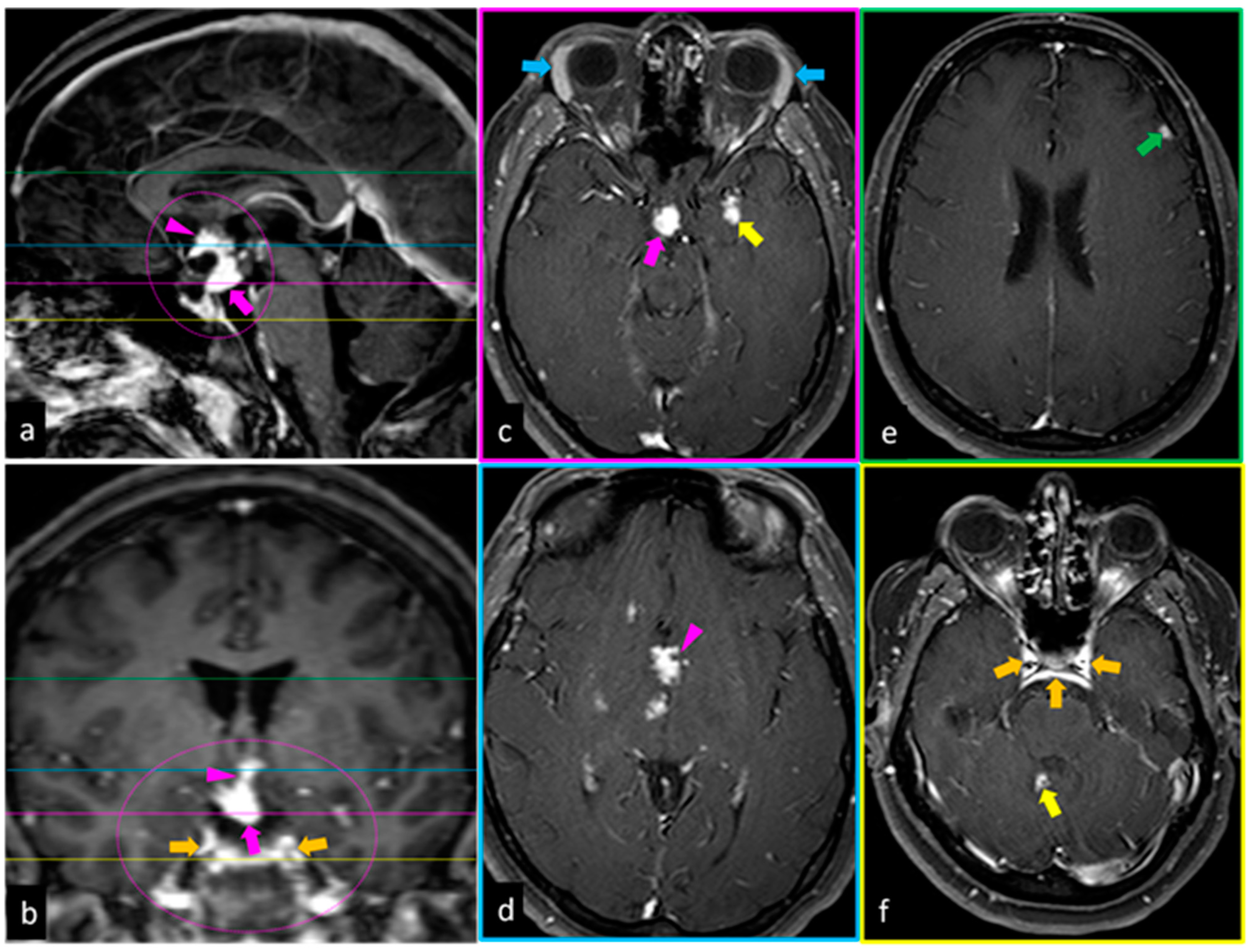
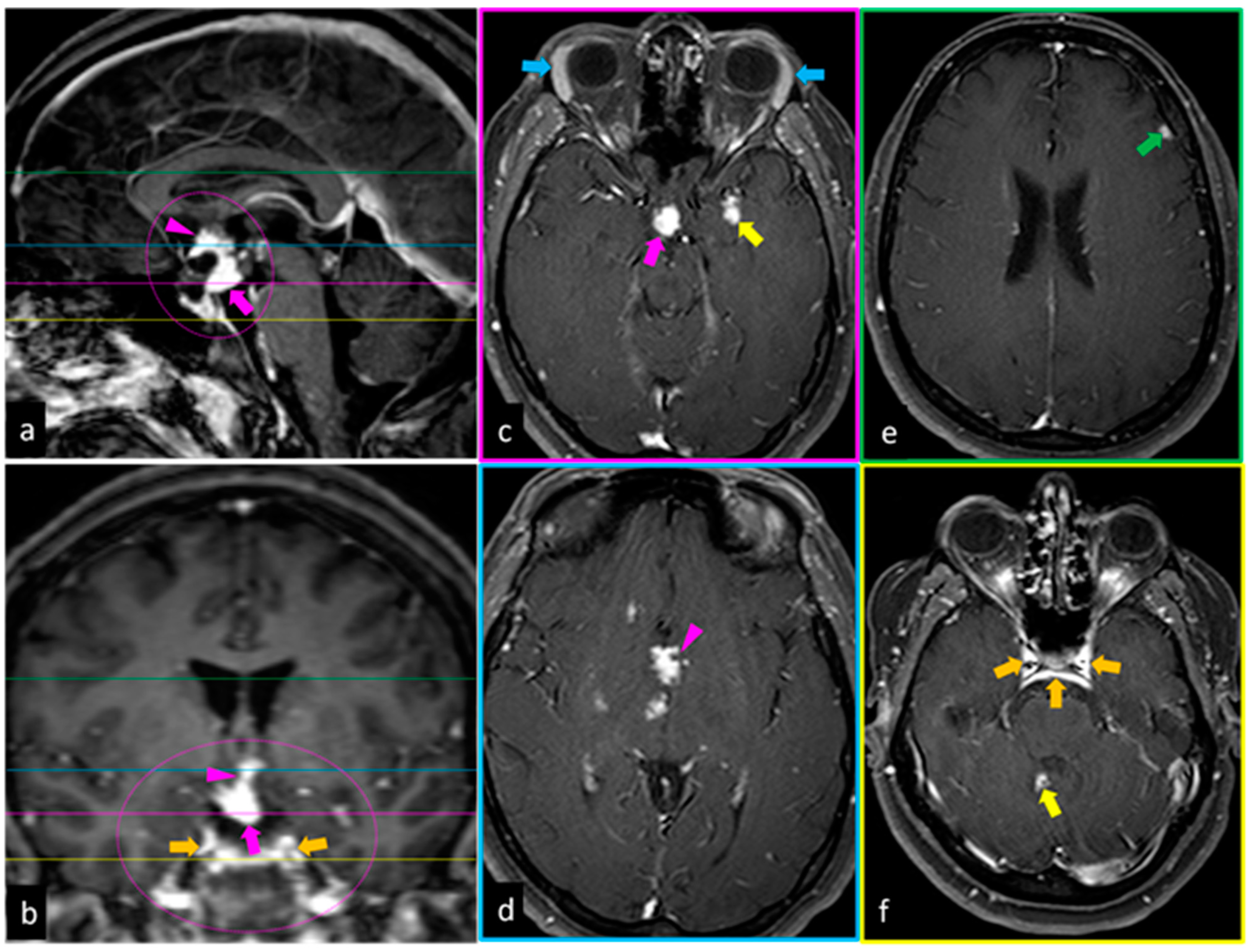
4.1. Magnetic Resonance Imaging
4.2. PET-CT
5. Shared Molecular Mechanisms between Migraine and Sarcoidosis
6. Common Ways of Treatment and Strategies of Approach on Disease Severity
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef]
- Holroyd, K.A.; Drew, J.B.; Cottrell, C.K.; Romanek, K.M.; Heh, V. Impaired functioning and quality of life in severe migraine: The role of catastrophizing and associated symptoms. Cephalalgia 2007, 27, 1156–1165. [Google Scholar] [CrossRef]
- Steiner, T.J.; Stovner, L.J.; Jensen, R.; Uluduz, D.; Katsarava, Z. Lifting The Burden: The Global Campaign against Headache. Migraine remains second among the world’s causes of disability, and first among young women: Findings from GBD2019. J. Headache Pain 2020, 21, 137. [Google Scholar] [CrossRef] [PubMed]
- Tana, C.; Iannetti, G.; Mezzetti, A.; Schiavone, C. Splenic sarcoidosis remains a diagnostic challenge. J. Clin. Ultrasound 2014, 42, 156. [Google Scholar] [CrossRef] [PubMed]
- Tana, C.; Silingardi, M.; Dietrich, C.F. New trends in ultrasound of hepatosplenic sarcoidosis. Z. Gastroenterol. 2015, 53, 283–284. [Google Scholar] [CrossRef] [PubMed]
- Tana, C.; Schiavone, C. The Chameleon Behavior of Sarcoidosis. J. Clin. Med. 2021, 10, 2780. [Google Scholar] [CrossRef]
- Tchernev, G.; Tana, C.; Schiavone, C.; Cardoso, J.C.; Ananiev, J.; Wollina, U. Sarcoidosis vs. Sarcoid-like reactions: The Two Sides of the same Coin? Wien. Med. Wochensschrift 2014, 164, 247–259. [Google Scholar] [CrossRef]
- Gelfand, J.M.; Gelfand, A.A.; Goadsby, P.J.; Benn, B.S.; Koth, L.L. Migraine is common in patients with sarcoidosis. Cephalalgia 2018, 38, 2079–2082. [Google Scholar] [CrossRef]
- Stovner, L.J.; Hagen, K.; Linde, M.; Steiner, T.J. The global prevalence of headache: An update, with analysis of the influences of methodological factors on prevalence estimates. J. Headache Pain 2022, 23, 34. [Google Scholar] [CrossRef]
- Ashina, M.; Katsarava, Z.; Do, T.P.; Buse, D.C.; Pozo-Rosich, P.; Özge, A.; Krymchantowski, A.V.; Lebedeva, E.R.; Ravishankar, K.; Yu, S.; et al. Migraine: Epidemiology and systems of care. Lancet 2021, 397, 1485–1495. [Google Scholar] [CrossRef]
- Burch, R.C.; Buse, D.C.; Lipton, R.B. Migraine: Epidemiology, Burden, and Comorbidity. Neurol. Clin. 2019, 37, 631–649. [Google Scholar] [CrossRef] [PubMed]
- Amiri, P.; Kazeminasab, S.; Nejadghaderi, S.A.; Mohammadinasab, R.; Pourfathi, H.; Araj-Khodaei, M.; Sullman, M.J.M.; Kolahi, A.A.; Safiri, S. Migraine: A Review on Its History, Global Epidemiology, Risk Factors, and Comorbidities. Front. Neurol. 2022, 12, 800605. [Google Scholar] [CrossRef]
- Safiri, S.; Pourfathi, H.; Eagan, A.; Mansournia, M.A.; Khodayari, M.T.; Sullman, M.J.M.; Kaufman, J.; Collins, G.; Dai, H.; Bragazzi, N.L.M.; et al. Global, regional, and national burden of migraine in 204 countries and territories, 1990 to 2019. Pain 2022, 163, e293–e309. [Google Scholar] [CrossRef] [PubMed]
- Ornello, R.; Caponnetto, V.; Frattale, I.; Sacco, S. Patterns of migraine in postmenopausal women: A systematic review. Neuropsychiatr. Dis. Treat. 2021, 17, 859–871. [Google Scholar] [CrossRef] [PubMed]
- Lui, J.Z.; Young, N.P.; Ebbert, J.O.; Rosedahl, J.K.; Philpot, L.M. Loneliness and Migraine Self-Management: A Cross-Sectional Assessment. J. Prim. Care Commun. Health 2020, 11, 2150132720924874. [Google Scholar] [CrossRef]
- Shimizu, T.; Sakai, F.; Miyake, H.; Sone, T.; Sato, M.; Tanabe, S.; Azuma, Y.; Dodick, D.W. Disability, quality of life, productivity impairment and employer costs of migraine in the workplace. J. Headache Pain 2021, 22, 29. [Google Scholar] [CrossRef]
- Yucel, A.; Thach, A.; Kumar, S.; Loden, C.; Bensink, M.; Goldfarb, N. Estimating the economic burden of migraine on US employers. Am. J. Manag. Care 2020, 26, e403–e408. [Google Scholar]
- Raggi, A.; Giovannetti, A.M.; Quintas, R.; D’Amico, D.; Cieza, A.; Sabariego, C.; Bickenbach, J.E.; Leonardi, M. A systematic review of the psychosocial difficulties relevant to patients with migraine. J. Headache Pain 2012, 13, 595–606. [Google Scholar] [CrossRef]
- Rybicki, B.A.; Major, M.; Popovich, J., Jr.; Maliarik, M.J.; Iannuzzi, M.C. Racial differences in sarcoidosis incidence: A 5-year study in a health maintenance organization. Am. J. Epidemiol. 1997, 145, 234–241. [Google Scholar] [CrossRef]
- Brennan, M.; Breen, D. Sarcoidosis in the older person: Diagnostic challenges and treatment consideration. Age Ageing 2022, 51, afac203. [Google Scholar] [CrossRef]
- Gerke, A.K.; Judson, M.A.; Cozier, Y.C.; Culver, D.A.; Koth, L.L. Disease Burden and Variability in Sarcoidosis. Ann. Am. Thorac. Soc. 2017, 14 (Suppl. S6), S421–S428. [Google Scholar] [CrossRef]
- Baughman, R.P.; Teirstein, A.S.; Judson, M.A.; Rossman, M.D.; Yeager, H., Jr.; Bresnitz, E.A.; DePalo, L.; Hunninghake, G.; Iannuzzi, M.C.; Johns, C.J.; et al. Case Control Etiologic Study of Sarcoidosis (ACCESS) Research Group. Clinical characteristics of patients in a case control study of sarcoidosis. Am. J. Respir. Crit. Care Med. 2001, 164, 1885–1889. [Google Scholar] [CrossRef]
- Hena, K.M. Sarcoidosis Epidemiology: Race Matters. Front. Immunol. 2020, 11, 537382. [Google Scholar] [CrossRef]
- Gerke, A.K. Morbidity and mortality in sarcoidosis. Curr. Opin. Pulm. Med. 2014, 20, 472–478. [Google Scholar] [CrossRef]
- Tchernev, G.; Chokoeva, A.A.; Tana, M.; Tana, C. Transcriptional blood signatures of sarcoidosis, sarcoid-like reactions and tubercolosis and their diagnostic implications. Sarcoidosis Vasc. Diffus. Lung Dis. 2016, 33, 5030. [Google Scholar]
- Tana, C.; Wegener, S.; Borys, E.; Pambuccian, S.; Tchernev, G.; Tana, M.; Giamberardino, M.A.; Silingardi, M. Challenges in the diagnosis and treatment of neurosarcoidosis. Ann. Med. 2015, 47, 576–591. [Google Scholar] [CrossRef]
- Heij, L.; Dahan, A.; Hoitsma, E. Sarcoidosis and pain caused by small-fiber neuropathy. Pain Res. Treat. 2012, 2012, 256024. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.P.; Judson, M.A.; Teirstein, A.; Yeager, H.; Rossman, M.; Knatterud, G.L.; Thompson, B. Presenting characteristics as predictors of duration of treatment in sarcoidosis. QJM 2006, 99, 307–315. [Google Scholar] [CrossRef]
- Drent, M.; Marcellis, R.; Lenssen, A.; De Vries, J. Association between physical functions and quality of life in sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2014, 31, 117–128. [Google Scholar]
- Tana, C.; Drent, M.; Nunes, H.; Kouranos, V.; Cinetto, F.; Jessurun, N.T.; Spagnolo, P. Comorbidities of sarcoidosis. Ann. Med. 2022, 54, 1014–1035. [Google Scholar] [CrossRef] [PubMed]
- Al-Kofahi, K.; Korsten, P.; Ascoli, C.; Virupannavar, S.; Mirsaeidi, M.; Chang, I.; Qaqish, N.; Saketkoo, L.A.; Baughman, R.P.; Sweiss, N.J. Management of extrapulmonary sarcoidosis: Challenges and solutions. Ther. Clin. Risk Manag. 2016, 12, 1623–1634. [Google Scholar] [CrossRef] [PubMed]
- Rota, E.; Mongini, F. Muscle tenderness and psychiatric comorbidity: A vicious cycle in migraine chronicization. Front. Neurol. 2014, 5, 148. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013, 33, 629–808. [Google Scholar] [CrossRef]
- Rapoport, A.M.; Bigal, M.E. ID-migraine. Neurol. Sci. 2004, 25 (Suppl. S3), S258–S260. [Google Scholar] [CrossRef]
- Dizdarevi, K.; Dizdarevi, S.; Dizdarevi, Z. Neurosarkoidoza prezentirana tranzitornim neurodeficitom i generaliziranim epileptickim napadima i udruzena sa migrenom [Neurosarcoidosis presenting with transitory neurodeficit and generalized epileptic seizures associated with migraine]. Med. Arch. 1998, 52, 159–162. [Google Scholar]
- Ray, B.K.; Thakur, R.K.; Shah, A.K.; Adhikari, B.; Mandal, D.K.; Pandey, R. Neurosarcoidosis Presenting as Young-Onset Chronic Headache: A Case Report. Case Rep. Neurol. 2021, 13, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Stefani, L.; Corsani, I.; Manetti, P.; Ciullini, G.; Galanti, G. Sarcoidosis in an athlete. Asian J. Sport. Med. 2011, 2, 57–62. [Google Scholar] [CrossRef]
- Medhat, B.M.; Behiry, M.E.; Fateen, M.; El-Ghobashy, N.; Fouda, R.; Embaby, A.; Seif, E.M.; Taha, M.M.; Hasswa, M.K.; Sobhy, D.; et al. Sarcoidosis beyond pulmonary involvement: A case series of unusual presentations. Respir. Med. Case Rep. 2021, 34, 101495. [Google Scholar] [CrossRef]
- Campbell, J.; Kee, R.; Bhattacharya, D.; Flynn, P.; McCarron, M.; Fulton, A. Systemic Sarcoidosis Presenting with Headache and Stroke-Like Episodes. Case Rep. Immunol. 2015, 2015, 619867. [Google Scholar] [CrossRef]
- Do, T.P.; Remmers, A.; Schytz, H.W.; Schankin, C.; Nelson, S.E.; Obermann, M.; Hansen, J.M.; Sinclair, A.J.; Gantenbein, A.R.; Schoonman, G.G. Red and orange flags for secondary headaches in clinical practice: SNNOOP10 list. Neurology 2019, 92, 134–144. [Google Scholar] [CrossRef]
- García-Azorín, D.; Abelaira-Freire, J.; González-García, N.; Rodriguez-Adrada, E.; Schytz, H.W.; Barloese, M.; Guerrero, Á.L.; Porta-Etessam, J.; Martín-Sánchez, F.J. Sensitivity of the SNNOOP10 list in the high-risk secondary headache detection. Cephalalgia 2022, 42, 1521–1531. [Google Scholar] [CrossRef]
- Oksanen, V. Neurosarcoidosis: Clinical presentations and course in 50 patients. Acta Neurol. Scand. 1986, 73, 283–290. [Google Scholar] [CrossRef]
- Lacomis, D. Neurosarcoidosis. Curr Neuropharmacol. 2011, 9, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Chapelon, C.; Ziza, J.M.; Piette, J.C.; Levy, Y.; Raguin, G.; Wechsler, B.; Bitker, M.O.; Bletry, O.; Laplane, D.; Bousser, M.G.; et al. Neurosarcoidosis: Signs, course and treatment in 35 confirmed cases. Medicine 1990, 69, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Joseph, F.G.; Scolding, N.J. Neurosarcoidosis: A study of 30 new cases. J. Neurol. Neurosurg. Psychiatry 2009, 80, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Fritz, D.; van de Beek, D.; Brouwer, M.C. Clinical features, treatment and outcome in neurosarcoidosis: Systematic review and meta-analysis. BMC Neurol. 2016, 16, 220. [Google Scholar] [CrossRef]
- Curone, M.; Tullo, V.; Peccarisi, C.; Bussone, G.; D’Amico, D. Headache as presenting symptom of neurosarcoidosis. Neurol. Sci. 2013, 34 (Suppl. S1), S183–S185. [Google Scholar] [CrossRef]
- Chokoeva, A.A.; Tchernev, G.; Tana, M.; Tana, C. Exclusion criteria for sarcoidosis: A novel approach for an ancient disease? Eur. J. Intern. Med. 2014, 25, e120. [Google Scholar] [CrossRef]
- Vukojevic, Z. EHMTI-0060. Neurosarcoidosis and chronic headache—Case report. J. Headache Pain 2014, 15 (Suppl. S1), C63. [Google Scholar] [CrossRef]
- Sambon, P.; Sellimi, A.; Kozyreff, A.; Gheysens, O.; Pothen, L.; Yildiz, H.; van Pesch, V. Epidemiology, clinical presentation, treatment, and outcome of neurosarcoidosis: A mono-centric retrospective study and literature review. Front. Neurol. 2022, 13, 970168. [Google Scholar] [CrossRef]
- Lord, J.; Paz Soldan, M.M.; Galli, J.; Salzman, K.L.; Kresser, J.; Bacharach, R.; DeWitt, L.D.; Klein, J.; Rose, J.; Greenlee, J.; et al. Neurosarcoidosis: Longitudinal experience in a single-center, academic healthcare system. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e743. [Google Scholar] [CrossRef]
- Chakales, P.A.; Herman, M.C.; Chien, L.C.; Hutto, S.K. Pachymeningitis in Biopsy-Proven Sarcoidosis: Clinical Course, Radiographic Findings, Response to Treatment, and Long-term Outcomes. Neurol. Neuroimmunol. Neuroinflamm. 2022, 9, e200028. [Google Scholar] [CrossRef] [PubMed]
- Hayes, W.S.; Sherman, J.L.; Stern, B.J.; Citrin, C.M.; Pulaski, P.D. MR and CT evaluation of intracranial sarcoidosis. AJR Am. J. Roentgenol. 1987, 149, 1043–1049. [Google Scholar] [CrossRef]
- Nowak, D.A.; Widenka, D.C. Neurosarcoidosis: A review of its intracranial manifestation. J. Neurol. 2001, 248, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.K.; Matheus, M.G.; Castillo, M. Imaging manifestations of neurosarcoidosis. AJR Am. J. Roentgenol. 2004, 182, 289–295. [Google Scholar] [CrossRef]
- Shah, R.; Roberson, G.H.; Curé, J.K. Correlation of MR imaging findings and clinical manifestations in neurosarcoidosis. AJNR Am. J. Neuroradiol. 2009, 30, 953–961. [Google Scholar] [CrossRef]
- Valeyre, D.; Prasse, A.; Nunes, H.; Uzunhan, Y.; Brillet, P.Y.; Muller-Quernheim, J. Sarcoidosis. Lancet 2014, 383, 1155–1167. [Google Scholar] [CrossRef]
- Mostard, R.L.; van Kroonenburgh, M.J.; Drent, M. The role of the PET scan in the management of sarcoidosis. Curr. Opin. Pulm. Med. 2013, 19, 538–544. [Google Scholar] [CrossRef]
- Tana, C. FDG-PET Imaging in Sarcoidosis. Curr. Med. Imaging Rev. 2019, 15, 2–3. [Google Scholar] [CrossRef]
- Tana, C.; Mantini, C.; Donatiello, I.; Mucci, L.; Tana, M.; Ricci, F.; Cipollone, F.; Giamberardino, M.A. Clinical Features and Diagnosis of Cardiac Sarcoidosis. J. Clin. Med. 2021, 10, 1941. [Google Scholar] [CrossRef] [PubMed]
- Cinetto, F.; Agostini, C. Advances in understanding the immunopathology of sarcoidosis and implications on therapy. Expert Rev. Clin. Immunol. 2016, 12, 973–988. [Google Scholar] [CrossRef] [PubMed]
- Stern, B.J.; Royal, W., 3rd; Gelfand, J.M.; Clifford, D.B.; Tavee, J.; Pawate, S.; Berger, J.R.; Aksamit, A.J.; Krumholz, A.; Pardo, C.A.; et al. Definition and Consensus Diagnostic Criteria for Neurosarcoidosis: From the Neurosarcoidosis Consortium Consensus Group. JAMA Neurol. 2018, 75, 1546–1553. [Google Scholar] [CrossRef] [PubMed]
- Chazal, T.; Costopoulos, M.; Maillart, E.; Fleury, C.; Psimaras, D.; Legendre, P.; Pineton de Chambrun, M.; Haroche, J.; Lubetzki, C.; Amoura, Z.; et al. The cerebrospinal fluid CD4/CD8 ratio and interleukin-6 and -10 levels in neurosarcoidosis: A multicenter, pragmatic, comparative study. Eur. J. Neurol. 2019, 26, 1274–1280. [Google Scholar] [CrossRef] [PubMed]
- Greco, R.; Demartini, C.; De Icco, R.; Martinelli, D.; Putortì, A.; Tassorelli, C. Migraine neuroscience: From experimental models to target therapy. Neurol. Sci. 2020, 41 (Suppl. S2), 351–361. [Google Scholar] [CrossRef]
- Byg, K.E.; Illes, Z.; Sejbaek, T.; Lambertsen, K.L.; Ellingsen, T.; Nielsen, H.H. Inflammatory profiles in plasma and cerebrospinal fluid of patients with neurosarcoidosis. J. Neuroimmunol. 2022, 367, 577849. [Google Scholar] [CrossRef]
- Cowan, R.P.; Gross, N.B.; Sweeney, M.D.; Sagare, A.P.; Montagne, A.; Arakaki, X.; Fonteh, A.N.; Zlokovic, B.V.; Pogoda, J.M.; Harrington, M.G. Evidence that blood-CSF barrier transport, but not inflammatory biomarkers, change in migraine, while CSF sVCAM1 associates with migraine frequency and CSF fibrinogen. Headache 2021, 61, 536–545. [Google Scholar] [CrossRef]
- Cseh, A.; Farkas, K.M.; Derzbach, L.; Muller, K.; Vasarhelyi, B.; Szalay, B.; Treszl, A.; Farkas, V. Lymphocyte subsets in pediatric migraine. Neurol. Sci. 2013, 34, 1151–1155. [Google Scholar] [CrossRef]
- Pavelek, Z.; Souček, O.; Krejsek, J.; Sobíšek, L.; Klímová, B.; Masopust, J.; Kuča, K.; Vališ, M. The role of the immune system and the biomarker CD3+CD4+CD45RA-CD62L- in the pathophysiology of migraine. Sci. Rep. 2020, 10, 12277. [Google Scholar] [CrossRef]
- Arumugam, M.; Parthasarathy, V. Reduction of CD4(+)CD25(+) regulatory T-cells in migraine: Is migraine an autoimmune disorder? J. Neuroimmunol. 2016, 290, 54–59. [Google Scholar] [CrossRef]
- Faraji, F.; Shojapour, M.; Farahani, I.; Ganji, A.; Mosayebi, G. Reduced regulatory T lymphocytes in migraine patients. Neurol. Res. 2021, 43, 677–682. [Google Scholar] [CrossRef]
- Zhang, J.; Czerpaniak, K.; Huang, L.; Liu, X.; Cloud, M.E.; Unsinger, J.; Hotchkiss, R.S.; Li, D.; Cao, Y.Q. Low-dose interleukin-2 reverses behavioral sensitization in multiple mouse models of headache disorders. Pain 2020, 161, 1381–1398. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Zhang, J.; Liu, X.; Unsinger, J.; Hotchkiss, R.S.; Cao, Y.Q. Low-dose interleukin-2 reverses chronic migraine-related sensitizations through peripheral interleukin-10 and transforming growth factor beta-1 signaling. Neurobiol. Pain 2022, 12, 100096. [Google Scholar] [CrossRef]
- Arumugam, M.; Sugin Lal Jabaris, S. Recent preclinical study offers a promising clue: Role of regulatory T cells as biomarkers in migraine. Immunol. Lett. 2021, 240, 9–11. [Google Scholar] [CrossRef]
- Taheri, M.; Nicknafs, F.; Hesami, O.; Javadi, A.; Arsang-Jang, S.; Sayad, A.; Ghafouri-Fard, S. Differential Expression of Cytokine-Coding Genes among Migraine Patients with and without Aura and Normal Subjects. J. Mol. Neurosci. 2021, 71, 1197–1204. [Google Scholar] [CrossRef]
- Sabri, M.R.; Dehghan, B.; Yaghini, O.; Nasiri, J.; Mansourian, M.; Khalifehsoltani, S. Endothelial dysfunction state in migraine headache and neutrally mediated syncope in children and young adults. J. Res. Med. Sci. 2015, 20, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Kelishadi, M.R.; Naeini, A.A.; Khorvash, F.; Askari, G.; Heidari, Z. The beneficial effect of Alpha-lipoic acid supplementation as a potential adjunct treatment in episodic migraines. Sci. Rep. 2022, 12, 271. [Google Scholar] [CrossRef] [PubMed]
- Ceylan, M.; Bayraktutan, O.F.; Becel, S.; Atis, Ö.; Yalcin, A.; Kotan, D. Serum levels of pentraxin-3 and other inflammatory biomarkers in migraine: Association with migraine characteristics. Cephalalgia 2016, 36, 518–525. [Google Scholar] [CrossRef]
- Vural, S.; Albayrak, L. Can calcitonin gene-related peptide (CGRP) and pentraxin-3 (PTX-3) be useful in diagnosing acute migraine attack? J. Recept. Signal Transduct. Res. 2022, 42, 562–566. [Google Scholar] [CrossRef]
- Gonçales, R.A.; Bastos, H.N.; Duarte-Oliveira, C.; Antunes, D.; Sokhatska, O.; Jacob, M.; Rolo, R.; Campos, C.F.; Sasaki, S.D.; Donato, A.; et al. Pentraxin 3 Inhibits Complement-driven Macrophage Activation to Restrain Granuloma Formation in Sarcoidosis. Am. J. Respir. Crit. Care Med. 2022, 206, 1140–1152. [Google Scholar] [CrossRef]
- Tana, C.; Bentivegna, E.; Cho, S.J.; Harriott, A.M.; García-Azorín, D.; Labastida-Ramirez, A.; Ornello, R.; Raffaelli, B.; Beltrán, E.R.; Ruscheweyh, R.; et al. Long COVID headache. J. Headache Pain 2022, 23, 93. [Google Scholar] [CrossRef] [PubMed]
- VanderPluym, J.H.; Halker Singh, R.B.; Urtecho, M.; Morrow, A.S.; Nayfeh, T.; Torres Roldan, V.D.; Farah, M.H.; Hasan, B.; Saadi, S.; Shah, S.; et al. Acute Treatments for Episodic Migraine in Adults: A Systematic Review and Meta-analysis. JAMA 2021, 325, 2357–2369. [Google Scholar] [CrossRef]
- Derry, S.; Moore, R.A. Paracetamol (acetaminophen) with or without an antiemetic for acute migraine headaches in adults. Cochrane Database Syst. Rev. 2013, 2013, CD008040. [Google Scholar] [CrossRef] [PubMed]
- Pope, J.V.; Edlow, J.A. Favorable response to analgesics does not predict a benign etiology of headache. Headache 2008, 48, 944–950. [Google Scholar] [CrossRef]
- Moore, R.A.; Derry, S.; Aldington, D.; Cole, P.; Wiffen, P.J. Amitriptyline for neuropathic pain in adults. Cochrane Database Syst. Rev. 2015, 2015, CD008242. [Google Scholar] [CrossRef]
- Gonzalez-Martinez, A.; Guerrero-Peral, Á.L.; Arias-Rivas, S.; Silva, L.; Sierra, Á.; Gago-Veiga, A.B.; García-Azorín, D. Amitriptyline for post-COVID headache: Effectiveness, tolerability, and response predictors. J. Neurol. 2022, 269, 5702–5709. [Google Scholar] [CrossRef]
- Spagnolo, P.; Rossi, G.; Trisolini, R.; Sverzellati, N.; Baughman, R.P.; Wells, A.U. Pulmonary sarcoidosis. Lancet Respir. Med. 2018, 6, 389–402. [Google Scholar] [CrossRef] [PubMed]
- Gosselin, J.; Roy-Hewitson, C.; Bullis, S.S.M.; DeWitt, J.C.; Soares, B.P.; Dasari, S.; Nevares, A. Neurosarcoidosis: Phenotypes, Approach to Diagnosis and Treatment. Curr. Rheumatol. Rep. 2022, 24, 371–382. [Google Scholar] [CrossRef]
- Pawate, S. Sarcoidosis and the Nervous System. Continuum 2020, 26, 695–715. [Google Scholar] [CrossRef] [PubMed]
- Bitoun, S.; Bouvry, D.; Borie, R.; Mahevas, M.; Sacre, K.; Haroche, J.; Psimaras, D.; Pottier, C.; Mathian, A.; Hie, M.; et al. Treatment of neurosarcoidosis: A comparative study of methotrexate and mycophenolate mofetil. Neurology 2016, 87, 2517–2521. [Google Scholar] [CrossRef]
- Gelfand, J.M.; Bradshaw, M.J.; Stern, B.J.; Clifford, D.B.; Wang, Y.; Cho, T.A.; Koth, L.L.; Hauser, S.L.; Dierkhising, J.; Vu, N.; et al. Infliximab for the treatment of CNS sarcoidosis: A multi-institutional series. Neurology 2017, 89, 2092–2100. [Google Scholar] [CrossRef]
- Fritz, D.; Timmermans, W.M.C.; van Laar, J.A.M.; van Hagen, P.M.; Siepman, T.A.M.; van de Beek, D.; Brouwer, M.C. Infliximab treatment in pathology-confirmed neurosarcoidosis. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e847. [Google Scholar] [CrossRef]
- Cohen Aubart, F.; Bouvry, D.; Galanaud, D.; Dehais, C.; Mathey, G.; Psimaras, D.; Haroche, J.; Pottier, C.; Hie, M.; Mathian, A.; et al. Long-term outcomes of refractory neurosarcoidosis treated with infliximab. J. Neurol. 2017, 264, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Moravan, M.; Segal, B.M. Treatment of CNS sarcoidosis with infliximab and mycophenolate mofetil. Neurology 2009, 72, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Riller, Q.; Cotteret, C.; Junot, H.; Benameur, N.; Haroche, J.; Mathian, A.; Hie, M.; Miyara, M.; Tilleul, P.; Amoura, Z.; et al. Infliximab biosimilar for treating neurosarcoidosis: Tolerance and efficacy in a retrospective study including switch from the originator and initiation of treatment. J. Neurol. 2019, 266, 1073–1078. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Central Nervous System Involvement | Peripheral Nervous System Disease | Myopathy |
|---|---|---|
| Non-specific symptoms (headache, fatigue, cognitive dysfunction with decline, fever, nausea and vomiting, mood disorders). Cranial neuropathy (II, III, VI, VII nerve involvement). Seizures and focal neurological deficits (hemiparesis) from brain tumor-like masses. Endocrine dysfunction (diabetes insipidus, hyperprolactinemia, TSH or gonadotropin deficiency). Ischemic or hemorrhagic stroke with focal deficits. Involvement of spinal cord, most often thoracic, with paresthesia and lower extremities weakness. | Mono- or multifocal neuropathy with or without conduction blocks. Poly-radiculoneuropathy (Guillain–Barre’-like syndrome). Asymmetrical sensory motor polyneuropathy. Less frequently patterns: atypical chronic inflammatory demyelinating polyneuropathy, small-fiber neuropathy, or involvement of autonomic fibers with pain or restless leg syndrome. | Non-specific, pain, muscle weakness, and atrophy. Acute myositis with fever, fatigue, disabling pain, muscle swelling, and sometimes contractures. Chronic myositis presenting as multiple tumor-like nodules found on physical examination. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tana, C.; Azorin, D.G.; Cinetto, F.; Mantini, C.; Tana, M.; Caulo, M.; Ricci, F.; Martelletti, P.; Cipollone, F.; Giamberardino, M.A. Common Clinical and Molecular Pathways between Migraine and Sarcoidosis. Int. J. Mol. Sci. 2023, 24, 8304. https://doi.org/10.3390/ijms24098304
Tana C, Azorin DG, Cinetto F, Mantini C, Tana M, Caulo M, Ricci F, Martelletti P, Cipollone F, Giamberardino MA. Common Clinical and Molecular Pathways between Migraine and Sarcoidosis. International Journal of Molecular Sciences. 2023; 24(9):8304. https://doi.org/10.3390/ijms24098304
Chicago/Turabian StyleTana, Claudio, David Garcia Azorin, Francesco Cinetto, Cesare Mantini, Marco Tana, Massimo Caulo, Fabrizio Ricci, Paolo Martelletti, Francesco Cipollone, and Maria Adele Giamberardino. 2023. "Common Clinical and Molecular Pathways between Migraine and Sarcoidosis" International Journal of Molecular Sciences 24, no. 9: 8304. https://doi.org/10.3390/ijms24098304
APA StyleTana, C., Azorin, D. G., Cinetto, F., Mantini, C., Tana, M., Caulo, M., Ricci, F., Martelletti, P., Cipollone, F., & Giamberardino, M. A. (2023). Common Clinical and Molecular Pathways between Migraine and Sarcoidosis. International Journal of Molecular Sciences, 24(9), 8304. https://doi.org/10.3390/ijms24098304