

The Role of MicroRNA in the Pathogenesis of Duchenne Muscular Dystrophy
 ,
,  ,
,
Abstract
1. Introduction
2. Duchenne Muscular Dystrophy: Pathogenesis and Epidemiology
3. MicroRNAs in the Pathogenesis of Duchenne Muscular Dystrophy
3.1. MicroRNAs Regulating Muscle and Satellite Cells
3.2. MicroRNAs Regulating DMD-Associated Cardiomyopathy
4. MicroRNA Alterations in Duchenne Muscular Dystrophy
4.1. Diagnostic Potential of microRNAs
4.2. MicroRNA Levels in Ambulant versus Non-Ambulant Patients
4.3. The Role of microRNAs in Detecting Carriers
5. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bez Batti Angulski, A.; Hosny, N.; Cohen, H.; Martin, A.A.; Hahn, D.; Bauer, J.; Metzger, J.M. Duchenne muscular dystrophy: Disease mechanism and therapeutic strategies. Front. Physiol. 2023, 14, 1183101. [Google Scholar] [CrossRef] [PubMed]
- Duan, D.; Goemans, N.; Takeda, S.; Mercuri, E.; Aartsma-Rus, A. Duchenne muscular dystrophy. Nat. Rev. Dis. Primers 2021, 7, 13. [Google Scholar] [CrossRef] [PubMed]
- Suthar, R.; Sankhyan, N. Duchenne Muscular Dystrophy: A Practice Update. Indian J. Pediatr. 2018, 85, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Birnkrant, D.J.; Bushby, K.; Bann, C.M.; Apkon, S.D.; Blackwell, A.; Colvin, M.K.; Cripe, L.; Herron, A.R.; Kennedy, A.; Kinnett, K.; et al. Diagnosis and management of Duchenne muscular dystrophy, part 3: Primary care, emergency management, psychosocial care, and transitions of care across the lifespan. Lancet Neurol. 2018, 17, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Broomfield, J.; Hill, M.; Guglieri, M.; Crowther, M.; Abrams, K. Life Expectancy in Duchenne Muscular Dystrophy: Reproduced Individual Patient Data Meta-Analysis. Neurology 2021, 97, e2304–e2314. [Google Scholar] [CrossRef] [PubMed]
- Molinaro, M.; Torrente, Y.; Villa, C.; Farini, A. Advancing Biomarker Discovery and Therapeutic Targets in Duchenne Muscular Dystrophy: A Comprehensive Review. Int. J. Mol. Sci. 2024, 25, 631. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; Xu, L.; Zhang, R.; Jin, Y.; Jiang, P.; Wei, K.; Shi, Y.; Zhao, J.; Xiong, M.; Guo, S.; et al. MicroRNA-Mediated Epigenetic Regulation of Rheumatoid Arthritis Susceptibility and Pathogenesis. Front. Immunol. 2022, 13, 838884. [Google Scholar] [CrossRef] [PubMed]
- Krauze, A.; Procyk, G.; Gąsecka, A.; Garstka-Pacak, I.; Wrzosek, M. The Role of MicroRNAs in Aortic Stenosis-Lessons from Recent Clinical Research Studies. Int. J. Mol. Sci. 2023, 24, 13095. [Google Scholar] [CrossRef] [PubMed]
- Kiełbowski, K.; Ptaszyński, K.; Wójcik, J.; Wojtyś, M.E. The role of selected non-coding RNAs in the biology of non-small cell lung cancer. Adv. Med. Sci. 2023, 68, 121–137. [Google Scholar] [CrossRef]
- Procyk, G.; Klimczak-Tomaniak, D.; Sygitowicz, G.; Tomaniak, M. Circulating and Platelet MicroRNAs in Cardiovascular Risk Assessment and Antiplatelet Therapy Monitoring. J. Clin. Med. 2022, 11, 1763. [Google Scholar] [CrossRef]
- Procyk, G.; Grodzka, O.; Procyk, M.; Gąsecka, A.; Głuszek, K.; Wrzosek, M. MicroRNAs in Myocarditis—Review of the Preclinical In Vivo Trials. Biomedicines 2023, 11, 2723. [Google Scholar] [CrossRef] [PubMed]
- Siracusa, J.; Koulmann, N.; Banzet, S. Circulating myomiRs: A new class of biomarkers to monitor skeletal muscle in physiology and medicine. J. Cachexia Sarcopenia Muscle 2018, 9, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Maggio, I.; Chen, X.; Gonçalves, M.A. The emerging role of viral vectors as vehicles for DMD gene editing. Genome Med. 2016, 8, 59. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.C.; Sheehan, D.W.; Prochoroff, A.; Birnkrant, D.J. Muscular Dystrophies. Clin. Chest Med. 2018, 39, 377–389. [Google Scholar] [CrossRef] [PubMed]
- Vincik, L.Y.; Dautel, A.D.; Staples, A.A.; Lauck, L.V.; Armstrong, C.J.; Howard, J.T.; McGregor, D.; Ahmadzadeh, S.; Shekoohi, S.; Kaye, A.D. Evolving Role of Viltolarsen for Treatment of Duchenne Muscular Dystrophy. Adv. Ther. 2024, 41, 1338–1350. [Google Scholar] [CrossRef] [PubMed]
- Pilgram, G.S.; Potikanond, S.; Baines, R.A.; Fradkin, L.G.; Noordermeer, J.N. The roles of the dystrophin-associated glycoprotein complex at the synapse. Mol. Neurobiol. 2010, 41, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Huard, J.; Côté, P.Y.; Parent, A.; Bouchard, J.P.; Tremblay, J.P. Dystrophin-like immunoreactivity in monkey and human brain areas involved in learning and motor functions. Neurosci. Lett. 1992, 141, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Keegan, N.P. Pseudoexons of the DMD Gene. J. Neuromuscul. Dis. 2020, 7, 77–95. [Google Scholar] [CrossRef] [PubMed]
- Ervasti, J.M. Dystrophin, its interactions with other proteins, and implications for muscular dystrophy. Biochim. Biophys. Acta 2007, 1772, 108–117. [Google Scholar] [CrossRef]
- Gao, Q.Q.; McNally, E.M. The Dystrophin Complex: Structure, Function, and Implications for Therapy. Compr. Physiol. 2015, 5, 1223–1239. [Google Scholar] [CrossRef]
- Le, S.; Yu, M.; Hovan, L.; Zhao, Z.; Ervasti, J.; Yan, J. Dystrophin As a Molecular Shock Absorber. ACS Nano 2018, 12, 12140–12148. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, C.L.; Winder, S.J. Sparks, signals and shock absorbers: How dystrophin loss causes muscular dystrophy. Trends Cell Biol. 2006, 16, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Fortunato, F.; Rossi, R.; Falzarano, M.S.; Ferlini, A. Innovative Therapeutic Approaches for Duchenne Muscular Dystrophy. J. Clin. Med. 2021, 10, 820. [Google Scholar] [CrossRef] [PubMed]
- Mirouse, V. Evolution and developmental functions of the dystrophin-associated protein complex: Beyond the idea of a muscle-specific cell adhesion complex. Front. Cell Dev. Biol. 2023, 11, 1182524. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, E.P.; Brown, R.H.; Kunkel, L.M. Dystrophin: The protein product of the Duchenne muscular dystrophy locus. Cell 1987, 51, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Lorin, C.; Vögeli, I.; Niggli, E. Dystrophic cardiomyopathy: Role of TRPV2 channels in stretch-induced cell damage. Cardiovasc. Res. 2015, 106, 153–162. [Google Scholar] [CrossRef]
- Klingler, W.; Jurkat-Rott, K.; Lehmann-Horn, F.; Schleip, R. The role of fibrosis in Duchenne muscular dystrophy. Acta Myol. 2012, 31, 184–195. [Google Scholar] [PubMed]
- Houang, E.M.; Sham, Y.Y.; Bates, F.S.; Metzger, J.M. Muscle membrane integrity in Duchenne muscular dystrophy: Recent advances in copolymer-based muscle membrane stabilizers. Skelet. Muscle 2018, 8, 31. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, E.; Seferian, A.M.; Servais, L.; Deconinck, N.; Stevenson, H.; Ni, X.; Zhang, W.; East, L.; Yonren, S.; Muntoni, F.; et al. Safety, tolerability and pharmacokinetics of eteplirsen in young boys aged 6-48 months with Duchenne muscular dystrophy amenable to exon 51 skipping. Neuromuscul. Disord. 2023, 33, 476–483. [Google Scholar] [CrossRef]
- Law, M.L.; Cohen, H.; Martin, A.A.; Angulski, A.B.B.; Metzger, J.M. Dysregulation of Calcium Handling in Duchenne Muscular Dystrophy-Associated Dilated Cardiomyopathy: Mechanisms and Experimental Therapeutic Strategies. J. Clin. Med. 2020, 9, 520. [Google Scholar] [CrossRef]
- Stedman, H.H.; Sweeney, H.L.; Shrager, J.B.; Maguire, H.C.; Panettieri, R.A.; Petrof, B.; Narusawa, M.; Leferovich, J.M.; Sladky, J.T.; Kelly, A.M. The mdx mouse diaphragm reproduces the degenerative changes of Duchenne muscular dystrophy. Nature 1991, 352, 536–539. [Google Scholar] [CrossRef] [PubMed]
- Aartsma-Rus, A.; Van Deutekom, J.C.; Fokkema, I.F.; Van Ommen, G.J.; Den Dunnen, J.T. Entries in the Leiden Duchenne muscular dystrophy mutation database: An overview of mutation types and paradoxical cases that confirm the reading-frame rule. Muscle Nerve 2006, 34, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Poyatos-García, J.; Martí, P.; Liquori, A.; Muelas, N.; Pitarch, I.; Martinez-Dolz, L.; Rodríguez, B.; Gonzalez-Quereda, L.; Damiá, M.; Aller, E.; et al. Dystrophinopathy Phenotypes and Modifying Factors in DMD Exon 45–55 Deletion. Ann. Neurol. 2022, 92, 793–806. [Google Scholar] [CrossRef] [PubMed]
- Monaco, A.P.; Bertelson, C.J.; Liechti-Gallati, S.; Moser, H.; Kunkel, L.M. An explanation for the phenotypic differences between patients bearing partial deletions of the DMD locus. Genomics 1988, 2, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Flanigan, K.M.; Dunn, D.M.; von Niederhausern, A.; Soltanzadeh, P.; Gappmaier, E.; Howard, M.T.; Sampson, J.B.; Mendell, J.R.; Wall, C.; King, W.M.; et al. Mutational spectrum of DMD mutations in dystrophinopathy patients: Application of modern diagnostic techniques to a large cohort. Hum. Mutat. 2009, 30, 1657–1666. [Google Scholar] [CrossRef] [PubMed]
- Aartsma-Rus, A.; Ginjaar, I.B.; Bushby, K. The importance of genetic diagnosis for Duchenne muscular dystrophy. J. Med. Genet. 2016, 53, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Takeshima, Y.; Yagi, M.; Okizuka, Y.; Awano, H.; Zhang, Z.; Yamauchi, Y.; Nishio, H.; Matsuo, M. Mutation spectrum of the dystrophin gene in 442 Duchenne/Becker muscular dystrophy cases from one Japanese referral center. J. Hum. Genet. 2010, 55, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Sarker, S.; Eshaque, T.B.; Soorajkumar, A.; Nassir, N.; Zehra, B.; Kanta, S.I.; Rahaman, M.A.; Islam, A.; Akter, S.; Ali, M.K.; et al. Mutational spectrum and phenotypic variability of Duchenne muscular dystrophy and related disorders in a Bangladeshi population. Sci. Rep. 2023, 13, 21547. [Google Scholar] [CrossRef] [PubMed]
- Iannone, F.; Montesanto, A.; Cione, E.; Crocco, P.; Caroleo, M.C.; Dato, S.; Rose, G.; Passarino, G. Expression Patterns of Muscle-Specific miR-133b and miR-206 Correlate with Nutritional Status and Sarcopenia. Nutrients 2020, 12, 297. [Google Scholar] [CrossRef]
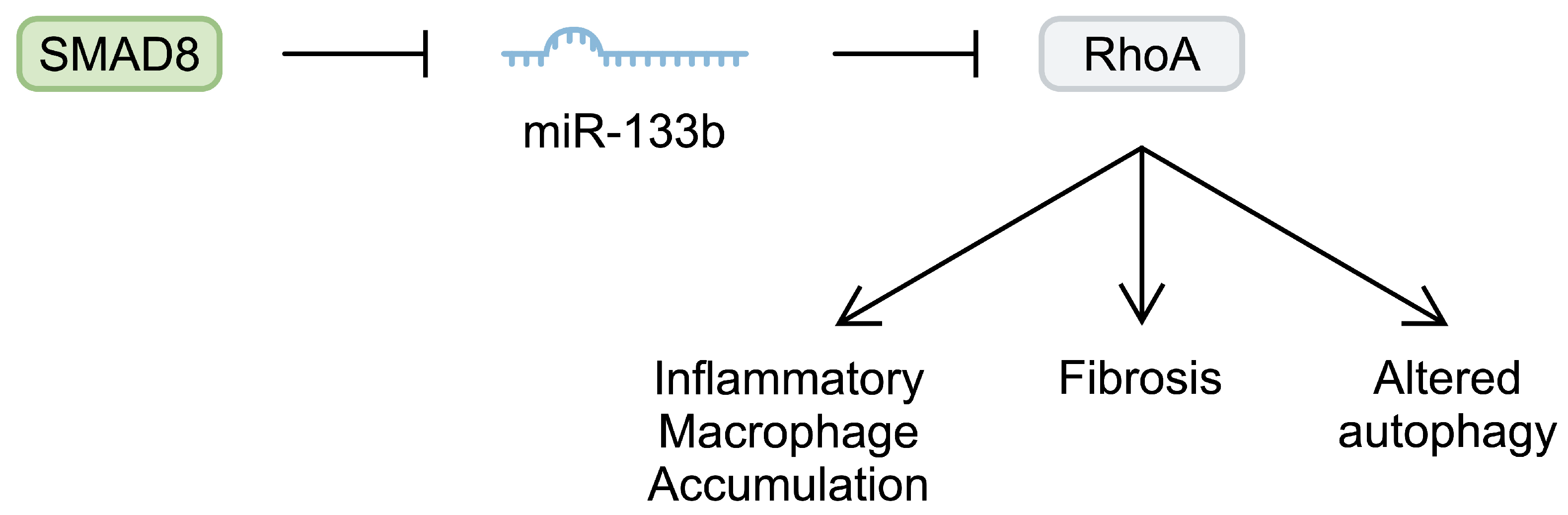
- Taetzsch, T.; Shapiro, D.; Eldosougi, R.; Myers, T.; Settlage, R.E.; Valdez, G. The microRNA miR-133b functions to slow Duchenne muscular dystrophy pathogenesis. J. Physiol. 2021, 599, 171–192. [Google Scholar] [CrossRef]
- Mu, X.; Usas, A.; Tang, Y.; Lu, A.; Wang, B.; Weiss, K.; Huard, J. RhoA mediates defective stem cell function and heterotopic ossification in dystrophic muscle of mice. FASEB J. 2013, 27, 3619–3631. [Google Scholar] [CrossRef] [PubMed]
- Mu, X.; Lin, C.Y.; Hambright, W.S.; Tang, Y.; Ravuri, S.; Lu, A.; Matre, P.; Chen, W.; Gao, X.; Cui, Y.; et al. Aberrant RhoA activation in macrophages increases senescence-associated secretory phenotypes and ectopic calcification in muscular dystrophic mice. Aging 2020, 12, 24853–24871. [Google Scholar] [CrossRef]
- Fernández-Simón, E.; Suárez-Calvet, X.; Carrasco-Rozas, A.; Piñol-Jurado, P.; López-Fernández, S.; Pons, G.; Bech Serra, J.J.; de la Torre, C.; de Luna, N.; Gallardo, E.; et al. RhoA/ROCK2 signalling is enhanced by PDGF-AA in fibro-adipogenic progenitor cells: Implications for Duchenne muscular dystrophy. J. Cachexia Sarcopenia Muscle 2022, 13, 1373–1384. [Google Scholar] [CrossRef] [PubMed]
- You, J.S.; Kim, Y.; Lee, S.; Bashir, R.; Chen, J. RhoA/ROCK signalling activated by ARHGEF3 promotes muscle weakness via autophagy in dystrophic mdx mice. J. Cachexia Sarcopenia Muscle 2023, 14, 1880–1893. [Google Scholar] [CrossRef]
- Lopez, M.A.; Si, Y.; Hu, X.; Williams, V.; Qushair, F.; Carlyle, J.; Alesce, L.; Conklin, M.; Gilbert, S.; Bamman, M.M.; et al. Smad8 Is Increased in Duchenne Muscular Dystrophy and Suppresses miR-1, miR-133a, and miR-133b. Int. J. Mol. Sci. 2022, 23, 7515. [Google Scholar] [CrossRef]
- Liu, N.; Williams, A.H.; Maxeiner, J.M.; Bezprozvannaya, S.; Shelton, J.M.; Richardson, J.A.; Bassel-Duby, R.; Olson, E.N. microRNA-206 promotes skeletal muscle regeneration and delays progression of Duchenne muscular dystrophy in mice. J. Clin. Investig. 2012, 122, 2054–2065. [Google Scholar] [CrossRef]
- Amirouche, A.; Jahnke, V.E.; Lunde, J.A.; Koulmann, N.; Freyssenet, D.G.; Jasmin, B.J. Muscle-specific microRNA-206 targets multiple components in dystrophic skeletal muscle representing beneficial adaptations. Am. J. Physiol. Cell Physiol. 2017, 312, C209–C221. [Google Scholar] [CrossRef] [PubMed]
- Soblechero-Martín, P.; López-Martínez, A.; de la Puente-Ovejero, L.; Vallejo-Illarramendi, A.; Arechavala-Gomeza, V. Utrophin modulator drugs as potential therapies for Duchenne and Becker muscular dystrophies. Neuropathol. Appl. Neurobiol. 2021, 47, 711–723. [Google Scholar] [CrossRef]
- Gurpur, P.B.; Liu, J.; Burkin, D.J.; Kaufman, S.J. Valproic acid activates the PI3K/Akt/mTOR pathway in muscle and ameliorates pathology in a mouse model of Duchenne muscular dystrophy. Am. J. Pathol. 2009, 174, 999–1008. [Google Scholar] [CrossRef]
- Boppart, M.D.; Burkin, D.J.; Kaufman, S.J. Activation of AKT signaling promotes cell growth and survival in α7β1 integrin-mediated alleviation of muscular dystrophy. Biochim. Biophys. Acta 2011, 1812, 439–446. [Google Scholar] [CrossRef]
- Yazid, M.D.; Hung-Chih, C. Perturbation of PI3K/Akt signaling affected autophagy modulation in dystrophin-deficient myoblasts. Cell Commun. Signal. 2021, 19, 105. [Google Scholar] [CrossRef] [PubMed]
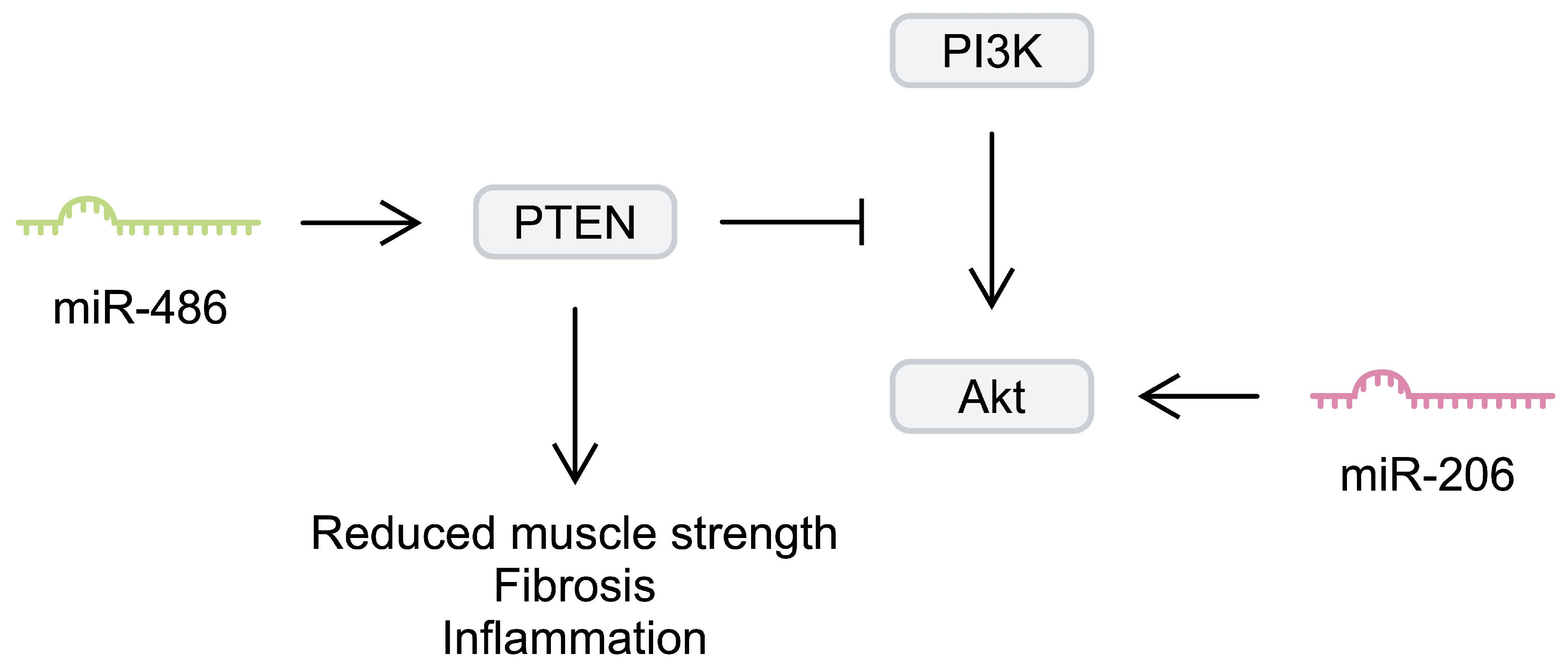
- Yue, F.; Song, C.; Huang, D.; Narayanan, N.; Qiu, J.; Jia, Z.; Yuan, Z.; Oprescu, S.N.; Roseguini, B.T.; Deng, M.; et al. PTEN Inhibition Ameliorates Muscle Degeneration and Improves Muscle Function in a Mouse Model of Duchenne Muscular Dystrophy. Mol. Ther. 2021, 29, 132–148. [Google Scholar] [CrossRef] [PubMed]
- Go, G.Y.; Jo, A.; Seo, D.W.; Kim, W.Y.; Kim, Y.K.; So, E.Y.; Chen, Q.; Kang, J.S.; Bae, G.U.; Lee, S.J. Ginsenoside Rb1 and Rb2 upregulate Akt/mTOR signaling-mediated muscular hypertrophy and myoblast differentiation. J. Ginseng Res. 2020, 44, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.S.; Casar, J.C.; Motohashi, N.; Vieira, N.M.; Eisenberg, I.; Marshall, J.L.; Gasperini, M.J.; Lek, A.; Myers, J.A.; Estrella, E.A.; et al. MicroRNA-486-dependent modulation of DOCK3/PTEN/AKT signaling pathways improves muscular dystrophy-associated symptoms. J. Clin. Investig. 2014, 124, 2651–2667. [Google Scholar] [CrossRef] [PubMed]
- Park, S.E.; Jeong, J.B.; Oh, S.J.; Kim, S.J.; Kim, H.; Choi, A.; Choi, S.J.; Oh, S.Y.; Ryu, G.H.; Lee, J.; et al. Wharton’s Jelly-Derived Mesenchymal Stem Cells Reduce Fibrosis in a Mouse Model of Duchenne Muscular Dystrophy by Upregulating microRNA 499. Biomedicines 2021, 9, 1089. [Google Scholar] [CrossRef] [PubMed]
- Ismaeel, A.; Kim, J.S.; Kirk, J.S.; Smith, R.S.; Bohannon, W.T.; Koutakis, P. Role of Transforming Growth Factor-β in Skeletal Muscle Fibrosis: A Review. Int. J. Mol. Sci. 2019, 20, 2446. [Google Scholar] [CrossRef] [PubMed]
- Mázala, D.A.; Novak, J.S.; Hogarth, M.W.; Nearing, M.; Adusumalli, P.; Tully, C.B.; Habib, N.F.; Gordish-Dressman, H.; Chen, Y.W.; Jaiswal, J.K.; et al. TGF-β-driven muscle degeneration and failed regeneration underlie disease onset in a DMD mouse model. JCI Insight 2020, 5, e135703. [Google Scholar] [CrossRef]
- Bakinowska, E.; Kiełbowski, K.; Pawlik, A. The Role of Extracellular Vesicles in the Pathogenesis and Treatment of Rheumatoid Arthritis and Osteoarthritis. Cells 2023, 12, 2716. [Google Scholar] [CrossRef]
- Bier, A.; Berenstein, P.; Kronfeld, N.; Morgoulis, D.; Ziv-Av, A.; Goldstein, H.; Kazimirsky, G.; Cazacu, S.; Meir, R.; Popovtzer, R.; et al. Placenta-derived mesenchymal stromal cells and their exosomes exert therapeutic effects in Duchenne muscular dystrophy. Biomaterials 2018, 174, 67–78. [Google Scholar] [CrossRef]
- Sengupta, K.; Mishra, M.K.; Loro, E.; Spencer, M.J.; Pyle, A.D.; Khurana, T.S. Genome Editing-Mediated Utrophin Upregulation in Duchenne Muscular Dystrophy Stem Cells. Mol. Ther. Nucleic Acids 2020, 22, 500–509. [Google Scholar] [CrossRef]
- Bostock, E.L.; Edwards, B.T.; Jacques, M.F.; Pogson, J.T.S.; Reeves, N.D.; Onambele-Pearson, G.L.; Morse, C.I. Impaired Glucose Tolerance in Adults with Duchenne and Becker Muscular Dystrophy. Nutrients 2018, 10, 1947. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Cai, X.; Xu, K.; Wu, Q.; Xu, B. The metabolomic plasma profile of patients with Duchenne muscular dystrophy: Providing new evidence for its pathogenesis. Orphanet J. Rare Dis. 2023, 18, 273. [Google Scholar] [CrossRef] [PubMed]
- Podkalicka, P.; Mucha, O.; Kaziród, K.; Szade, K.; Stępniewski, J.; Ivanishchuk, L.; Hirao, H.; Pośpiech, E.; Józkowicz, A.; Kupiec-Weglinski, J.W.; et al. miR-378 affects metabolic disturbances in the mdx model of Duchenne muscular dystrophy. Sci. Rep. 2022, 12, 3945. [Google Scholar] [CrossRef] [PubMed]
- Casati, S.R.; Cervia, D.; Roux-Biejat, P.; Moscheni, C.; Perrotta, C.; De Palma, C. Mitochondria and Reactive Oxygen Species: The Therapeutic Balance of Powers for Duchenne Muscular Dystrophy. Cells 2024, 13, 574. [Google Scholar] [CrossRef] [PubMed]
- Vu Hong, A.; Bourg, N.; Sanatine, P.; Poupiot, J.; Charton, K.; Gicquel, E.; Massourides, E.; Spinazzi, M.; Richard, I.; Israeli, D. Dlk1-Dio3 cluster miRNAs regulate mitochondrial functions in the dystrophic muscle in Duchenne muscular dystrophy. Life Sci. Alliance 2023, 6, e202201506. [Google Scholar] [CrossRef] [PubMed]
- Cardone, N.; Taglietti, V.; Baratto, S.; Kefi, K.; Periou, B.; Gitiaux, C.; Barnerias, C.; Lafuste, P.; Pharm, F.L.; Pharm, J.N.; et al. Myopathologic trajectory in Duchenne muscular dystrophy (DMD) reveals lack of regeneration due to senescence in satellite cells. Acta Neuropathol. Commun. 2023, 11, 167. [Google Scholar] [CrossRef] [PubMed]
- Pietraszek-Gremplewicz, K.; Kozakowska, M.; Bronisz-Budzynska, I.; Ciesla, M.; Mucha, O.; Podkalicka, P.; Madej, M.; Glowniak, U.; Szade, K.; Stepniewski, J.; et al. Heme Oxygenase-1 Influences Satellite Cells and Progression of Duchenne Muscular Dystrophy in Mice. Antioxid. Redox Signal. 2018, 29, 128–148. [Google Scholar] [CrossRef]
- Chen, J.F.; Tao, Y.; Li, J.; Deng, Z.; Yan, Z.; Xiao, X.; Wang, D.Z. microRNA-1 and microRNA-206 regulate skeletal muscle satellite cell proliferation and differentiation by repressing Pax7. J. Cell Biol. 2010, 190, 867–879. [Google Scholar] [CrossRef]
- Crist, C.G.; Montarras, D.; Pallafacchina, G.; Rocancourt, D.; Cumano, A.; Conway, S.J.; Buckingham, M. Muscle stem cell behavior is modified by microRNA-27 regulation of Pax3 expression. Proc. Natl. Acad. Sci. USA 2009, 106, 13383–13387. [Google Scholar] [CrossRef]
- Shen, J.; Wang, J.; Zhen, H.; Liu, Y.; Li, L.; Luo, Y.; Hu, J.; Liu, X.; Li, S.; Hao, Z.; et al. MicroRNA-381 Regulates Proliferation and Differentiation of Caprine Skeletal Muscle Satellite Cells by Targeting. Int. J. Mol. Sci. 2022, 23, 13587. [Google Scholar] [CrossRef]
- Li, H.; Kang, L.; Wu, R.; Li, C.; Zhang, Q.; Zhong, R.; Jia, L.; Zhu, D.; Zhang, Y. miR-378-mediated glycolytic metabolism enriches the Pax7. Cell Regen. 2022, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Li, P.; Dan, X.; Kang, X.; Ma, Y.; Shi, Y. Inhibits Proliferation and Differentiation of Bovine Skeletal Muscle Satellite Cells by Targeting. Genes 2022, 13, 947. [Google Scholar] [CrossRef] [PubMed]
- Kamdar, F.; Garry, D.J. Dystrophin-Deficient Cardiomyopathy. J. Am. Coll. Cardiol. 2016, 67, 2533–2546. [Google Scholar] [CrossRef] [PubMed]
- Fayssoil, A.; Nardi, O.; Orlikowski, D.; Annane, D. Cardiomyopathy in Duchenne muscular dystrophy: Pathogenesis and therapeutics. Heart Fail. Rev. 2010, 15, 103–107. [Google Scholar] [CrossRef]
- Morales, E.D.; Yue, Y.; Watkins, T.B.; Han, J.; Pan, X.; Gibson, A.M.; Hu, B.; Brito-Estrada, O.; Yao, G.; Makarewich, C.A.; et al. Dwarf Open Reading Frame (DWORF) Gene Therapy Ameliorated Duchenne Muscular Dystrophy Cardiomyopathy in Aged mdx Mice. J. Am. Heart Assoc. 2023, 12, e027480. [Google Scholar] [CrossRef]
- Gartz, M.; Beatka, M.; Prom, M.J.; Strande, J.L.; Lawlor, M.W. Cardiomyocyte-produced miR-339-5p mediates pathology in Duchenne muscular dystrophy cardiomyopathy. Hum. Mol. Genet. 2021, 30, 2347–2361. [Google Scholar] [CrossRef]
- Kyrychenko, S.; Kyrychenko, V.; Badr, M.A.; Ikeda, Y.; Sadoshima, J.; Shirokova, N. Pivotal role of miR-448 in the development of ROS-induced cardiomyopathy. Cardiovasc. Res. 2015, 108, 324–334. [Google Scholar] [CrossRef]
- Gonzalez, D.R.; Treuer, A.V.; Lamirault, G.; Mayo, V.; Cao, Y.; Dulce, R.A.; Hare, J.M. NADPH oxidase-2 inhibition restores contractility and intracellular calcium handling and reduces arrhythmogenicity in dystrophic cardiomyopathy. Am. J. Physiol. Heart Circ. Physiol. 2014, 307, H710–H721. [Google Scholar] [CrossRef]
- Kepreotis, S.V.; Oh, J.G.; Park, M.; Yoo, J.; Lee, C.; Mercola, M.; Hajjar, R.J.; Jeong, D. Inhibition of miR-25 ameliorates cardiac and skeletal muscle dysfunction in aged. Mol. Ther. Nucleic Acids 2024, 35, 102174. [Google Scholar] [CrossRef]
- Abdel-Salam, E.; Abdel-Meguid, I.; Korraa, S.S. Markers of degeneration and regeneration in Duchenne muscular dystrophy. Acta Myol. 2009, 28, 94–100. [Google Scholar]
- Toivonen, J.M.; Manzano, R.; Oliván, S.; Zaragoza, P.; García-Redondo, A.; Osta, R. MicroRNA-206: A potential circulating biomarker candidate for amyotrophic lateral sclerosis. PLoS ONE 2014, 9, e89065. [Google Scholar] [CrossRef] [PubMed]
- Greco, S.; De Simone, M.; Colussi, C.; Zaccagnini, G.; Fasanaro, P.; Pescatori, M.; Cardani, R.; Perbellini, R.; Isaia, E.; Sale, P.; et al. Common micro-RNA signature in skeletal muscle damage and regeneration induced by Duchenne muscular dystrophy and acute ischemia. FASEB J. 2009, 23, 3335–3346. [Google Scholar] [CrossRef]
- Jeanson-Leh, L.; Lameth, J.; Krimi, S.; Buisset, J.; Amor, F.; Le Guiner, C.; Barthélémy, I.; Servais, L.; Blot, S.; Voit, T.; et al. Serum profiling identifies novel muscle miRNA and cardiomyopathy-related miRNA biomarkers in Golden Retriever muscular dystrophy dogs and Duchenne muscular dystrophy patients. Am. J. Pathol. 2014, 184, 2885–2898. [Google Scholar] [CrossRef] [PubMed]
- Coenen-Stass, A.M.L.; Sork, H.; Gatto, S.; Godfrey, C.; Bhomra, A.; Krjutškov, K.; Hart, J.R.; Westholm, J.O.; O’Donovan, L.; Roos, A.; et al. Comprehensive RNA-Sequencing Analysis in Serum and Muscle Reveals Novel Small RNA Signatures with Biomarker Potential for DMD. Mol. Ther. Nucleic Acids 2018, 13, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Trifunov, S.; Natera-de Benito, D.; Exposito Escudero, J.M.; Ortez, C.; Medina, J.; Cuadras, D.; Badosa, C.; Carrera, L.; Nascimento, A.; Jimenez-Mallebrera, C. Longitudinal Study of Three microRNAs in Duchenne Muscular Dystrophy and Becker Muscular Dystrophy. Front. Neurol. 2020, 11, 304. [Google Scholar] [CrossRef] [PubMed]
- García-Giménez, J.L.; García-Trevijano, E.R.; Avilés-Alía, A.I.; Ibañez-Cabellos, J.S.; Bovea-Marco, M.; Bas, T.; Pallardó, F.V.; Viña, J.R.; Zaragozá, R. Identification of circulating miRNAs differentially expressed in patients with Limb-girdle, Duchenne or facioscapulohumeral muscular dystrophies. Orphanet J. Rare Dis. 2022, 17, 450. [Google Scholar] [CrossRef]
- Cacchiarelli, D.; Legnini, I.; Martone, J.; Cazzella, V.; D’Amico, A.; Bertini, E.; Bozzoni, I. miRNAs as serum biomarkers for Duchenne muscular dystrophy. EMBO Mol. Med. 2011, 3, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Zaharieva, I.T.; Calissano, M.; Scoto, M.; Preston, M.; Cirak, S.; Feng, L.; Collins, J.; Kole, R.; Guglieri, M.; Straub, V.; et al. Dystromirs as serum biomarkers for monitoring the disease severity in Duchenne muscular Dystrophy. PLoS ONE 2013, 8, e80263. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Kong, M.; Ye, Y.; Hong, S.; Cheng, L.; Jiang, L. Serum miR-206 and other muscle-specific microRNAs as non-invasive biomarkers for Duchenne muscular dystrophy. J. Neurochem. 2014, 129, 877–883. [Google Scholar] [CrossRef]
- Li, X.; Li, Y.; Zhao, L.; Zhang, D.; Yao, X.; Zhang, H.; Wang, Y.C.; Wang, X.Y.; Xia, H.; Yan, J.; et al. Circulating Muscle-specific miRNAs in Duchenne Muscular Dystrophy Patients. Mol. Ther. Nucleic Acids 2014, 3, e177. [Google Scholar] [CrossRef]
- Llano-Diez, M.; Ortez, C.I.; Gay, J.A.; Álvarez-Cabado, L.; Jou, C.; Medina, J.; Nascimento, A.; Jimenez-Mallebrera, C. Digital PCR quantification of miR-30c and miR-181a as serum biomarkers for Duchenne muscular dystrophy. Neuromuscul. Disord. 2017, 27, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Meng, Q.; Zhang, J.; Zhong, J.; Zeng, D.; Lan, D. Novel miRNA Biomarkers for Patients With Duchenne Muscular Dystrophy. Front. Neurol. 2022, 13, 921785. [Google Scholar] [CrossRef] [PubMed]
- Catapano, F.; Domingos, J.; Perry, M.; Ricotti, V.; Phillips, L.; Servais, L.; Seferian, A.; Groot, I.; Krom, Y.D.; Niks, E.H.; et al. Downregulation of miRNA-29, -23 and -21 in urine of Duchenne muscular dystrophy patients. Epigenomics 2018, 10, 875–889. [Google Scholar] [CrossRef] [PubMed]
- Catapano, F.; Scaglioni, D.; Maresh, K.; Ala, P.; Domingos, J.; Selby, V.; Ricotti, V.; Phillips, L.; Servais, L.; Seferian, A.; et al. Novel free-circulating and extracellular vesicle-derived miRNAs dysregulated in Duchenne muscular dystrophy. Epigenomics 2020, 12, 1899–1915. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Becerril, T.; Rodríguez-Cruz, M.; Hernández-Cruz, S.Y.; Ruiz-Cruz, E.D.; Mendoza, C.R.S.; Cárdenas-Conejo, A.; Escobar-Cedillo, R.E.; Ávila-Moreno, F.; Aquino-Jarquin, G. Natural history of circulating miRNAs in Duchenne disease: Association with muscle injury and metabolic parameters. Acta Neurol. Scand. 2022, 146, 512–524. [Google Scholar] [CrossRef] [PubMed]
- Anaya-Segura, M.A.; Rangel-Villalobos, H.; Martínez-Cortés, G.; Gómez-Díaz, B.; Coral-Vázquez, R.M.; Zamora-González, E.O.; García, S.; López-Hernández, L.B. Serum Levels of MicroRNA-206 and Novel Mini-STR Assays for Carrier Detection in Duchenne Muscular Dystrophy. Int. J. Mol. Sci. 2016, 17, 1334. [Google Scholar] [CrossRef] [PubMed]
- Mousa, N.O.; Abdellatif, A.; Fahmy, N.; Zada, S.; El-Fawal, H.; Osman, A. Circulating MicroRNAs in Duchenne Muscular Dystrophy. Clin. Neurol. Neurosurg. 2020, 189, 105634. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Meng, Q.; Zhong, J.; Zhang, M.; Qin, X.; Ni, X.; Ma, J.; He, Y.; Zeng, D.; Lan, D. Serum MyomiRs as Biomarkers for Female Carriers of Duchenne/Becker Muscular Dystrophy. Front. Neurol. 2020, 11, 563609. [Google Scholar] [CrossRef] [PubMed]
- Sandonà, M.; Consalvi, S.; Tucciarone, L.; De Bardi, M.; Scimeca, M.; Angelini, D.F.; Buffa, V.; D’Amico, A.; Bertini, E.S.; Cazzaniga, S.; et al. HDAC inhibitors tune miRNAs in extracellular vesicles of dystrophic muscle-resident mesenchymal cells. EMBO Rep. 2020, 21, e50863. [Google Scholar] [CrossRef]
- Xu, X.; Hao, Y.; Xiong, S.; He, Z. Comprehensive Analysis of Long Non-coding RNA-Associated Competing Endogenous RNA Network in Duchenne Muscular Dystrophy. Interdiscip. Sci. 2020, 12, 447–460. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, Y.; Hu, Q.; Xi, Y.; Xing, Z.; Zhang, Z.; Huang, L.; Wu, J.; Liang, K.; Nguyen, T.K.; et al. The lncRNA H19 alleviates muscular dystrophy by stabilizing dystrophin. Nat. Cell Biol. 2020, 22, 1332–1345. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Molecule | Mechanism | Reference |
|---|---|---|
| miR-133b. | Deletion of miR-133b was associated with reduced cross-sectional area, fewer satellite cells, and decreased muscle regenerative capabilities. | [40] |
| miR-206. | Knockdown of miR-206 in mdx mice further exacerbated dystrophic alterations. | [46] |
| Overexpression of miR-206 enhanced the expression of myogenic regulatory factors and utrophin A. | [47] | |
| miR-486 | Overexpression of miR-486 in dystrophin-deficient murine models improved muscle histology, strength, and physiology. | [54] |
| miR-499-5p | Administration of Wharton’s jelly mesenchymal stem cells into mdx mice increase the expression of miR-499-5p, which has anti-fibrotic effects. | [55] |
| miR-29c | Exosomes from placenta-derived mesenchymal stem cells can transfer miR-29c to myoblasts, thus reducing fibrosis and inflammation. | [59] |
| miR-378 | Mdx mice lacking miR-378 demonstrated improved glucose tolerance, reduced expression of inflammatory mediators in the liver, and altered expression of lipid metabolism–related genes. | [63] |
| miR-339-5p | DMD-derived cardiomyocytes secrete exosomes containing miR-339-5p that impairs the response of other cardiac cells to stress. | [76] |
| miR-448-3p | Downregulation of miR-448-3p, which is observed in dystrophic hearts, was associated with the induction of fibrosis and cardiac remodelling. | [77] |
| miR-25 | Suppression of overexpressed miR-25 in DMD animal models was associated with improved myocyte contractility and enhanced survival. | [79] |
| Ref. | Year | Population | Comparison | Assessed miRNAs | Outcome | Methodology |
|---|---|---|---|---|---|---|
| [82] | 2009 | 12 patients with DMD | 10 age- and sex-matched controls | miR-1, miR-29c, miR-124a, miR-135a, miR-516-3p, miR-31, miR-43c, miR-206, miR-222, miR-223, miR-335, miR-449, and miR-494 | ↑ miR-31, miR-43c, miR-206, miR-222, miR-223, miR-335, miR-449, and miR-494 in patients with DMD ↓ miR-1, miR-29c, and miR-135a in patients with DMD | miRNAs in human quadriceps femoris biopsies by qPCR |
| [83] | 2014 | 5 patients with DMD (serum) 3 patients with DMD (muscle biopsy) | 3 age-matched controls | miR-95, miR-208a, miR-208b, miR-410, miR-433, miR-494, miR-495, miR-499, and miR-539 | ↑ miR-95, miR-208b, and miR-499 and ↓ miR-539 in serum of patients with DMD ↓ miR-499 in muscle of patients with DMD | miRNAs in serum and paravertebral/dorsal muscle biopsies by qRT-PCR |
| [84] | 2018 | 28 patients with DMD | 16 HCs | miR-1a-3p, miR-133a-3p, miR-206-3p, miR-483-5p, and miR-483-3p | ↑ miR-1a-3p, miR-133a-3p, miR-206-3p, and miR-483-5p in patients with DMD ROC analysis showed significant values for DMD vs HCs (AUC)—miR-1a-3p: (0.980); miR-133a-3p: (0.915); miR-206-3p: (0.998); miR-483-5p: (0.819); miR-483-3p: (0.531) | miRNAs in serum by qRT-PCR |
| [85] | 2020 | 13 patients with DMD | 13 HCs | miR-181a-5p, miR-30c-5p, and miR-206 | ↑ miR-30c-5p and miR-206 in patients with DMD over the entire study length ROC analysis DMD vs BMD (AUC)—miR-206: (0.82), (0.95), and (0.75) at the first, second, and third timepoints, respectively | miRNAs in serum by ddPCR at the three timepoints over 4 years |
| [86] | 2022 | 5 patients with DMD | 5 HCs | miR-122-5p, miR-192-5p, miR-19b-3p, miR-323b-3p, and miR-206 | ↑ miR-122-5p, miR-192-5p, miR-19b-3p, miR-323b-3p, and miR-206 in patients with DMD ROC analysis DMD vs HCs—AUC > 0.9 for all miRNAs | miRNAs in plasma by qPCR |
| [87] | 2011 | 26 patients with DMD | 7 HCs | miR-1, miR-133, miR-206, and miR-233 | ↑ miR-1, miR-133, and miR-206 in patients with DMD ROC analysis DMD vs. BMD and DMD vs. HCs– miR-206: AUC always > 0.94, p < 0.001 miR-1: AUC always > 0.84, p < 0.01 miR-133: AUC always > 0.76, p < 0.01 Inverse correlation between miR-1, miR-133, and miR-206 and NSAA scores | miRNAs in serum by qRT-PCR |
| [88] | 2013 | 44 patients with DMD | 14 HCs | miR-1, miR-206, miR-31, miR-133a, and miR-133b | ↑ miR-1, miR-206, miR-31, and miR-133b in patients with DMD ↑ miR-1, miR-206, miR-31, miR-133a, and miR-133b in ambulant patients with DMD compared with non-ambulant patients with DMD No correlation between miRNAs and NSAA scores Positive correlation between miR-1 and miR-133b and FVC values | miRNAs in serum by qRT-PCR |
| [89] | 2014 | 39 patients with DMD | 36 HCs | miR-1, miR-133, and miR-206 | ↑ miR-1, miR-133b, and miR-206 in patients with DMD Inverse correlations between miR-1 and miR-206 and muscle strength; miR-1, miR-133, and miR-206 and muscle function; miR-1, miR-133, and miR-206 and QoL ROC analysis DMD vs HCs (AUC)—miR-1: (0.93); miR-133: (0.90); miR-206: (0.96) | miRNAs in serum by qRT-PCR |
| [90] | 2014 | 52 patients with DMD | 23 HCs | miR-1, miR-133, miR-206, miR-208a, miR-208b, and miR-499 | ↑ miR-1, miR-133, miR-206, miR-208a, miR-208b, and miR-499 in patients with DMD ROC analysis showed significant values for DMD vs HCs (AUC), DMD vs BMD [AUC]—miR-1: (0.8227); miR-133: (0.8119), [0.6756]; miR-206: (0.9156), [0.7090]; miR-208a: (0.8127); miR-208b: (0.9323), [0.7115]; miR-499: (0.9900), [0.6987] Positive correlation between miR-206, miR-208b, and miR-499 and both age and type IIc muscle fibre content in patients with DMD | miRNAs in serum by qRT-PCR |
| [91] | 2017 | 21 patients with DMD | 22 age-matched HCs | miR-30c-5p and miR-181a-5p | ↑ miR-30c-5p and miR-181a-5p in patients with DMD No correlation between miR-30c-5p and miR-181a-5p and NSAA scores | miRNAs in serum by ddPCR |
| [92] | 2022 | 48 patients with DMD | 53 HCs | miR-1, miR-133a, miR-133b, miR-206, miR-208a, miR-208b, and miR-499 | ↑ miR-1, miR-133a, miR-133b, miR-206, miR-208a, miR-208b, and miR-499 in patients with DMD ROC analysis DMD vs HCs—AUC > 0.747 for all miRNAs Positive correlation between all miRNAs and lower limb distal muscle strength Negative correlation between miR-499, miR-208b, miR-133a, and miR-133b and Gowers’ time | miRNAs in serum by qPCR |
| [93] | 2018 | 54 patients with DMD: ambulant (n = 31) non-ambulant (n = 23) | 20 age-matched HCs | miR-21-5p, miR-22-3p, miR-23b-3p, miR-29c-3p and miR-103a-3p | ↓ miR-29c-3p in patients with DMD compared with HCs and in ambulant patients with DMD compared with HCs ↓ miR-21-5p and miR-23b-3p in non-ambulant patients with DMD compared with HCs | miRNAs in urinary exosomes by qPCR |
| [94] | 2020 | 28 patients with DMD: ambulant (n = 15) non-ambulant (n = 13) | 8 HCs | miR-1-3p, miR-133a-3p, miR-133b, miR-200c-3p, miR-660-5p, miR-29c-3p and miR-136-5p | ↑ miR-1-3p, miR-133a-3p, and miR-29c-3p in patients with DMD compared with HCs ↑ miR-1-3p, miR-133a-3p, miR-133b and miR-136-5p in ambulant patients with DMD compared with HCs ↑ miR-133a-3p in non-ambulant patients with DMD compared with HCs ↑ miR-660-5p and miR-29c-3p in ambulant patients with DMD compared with non-ambulant patients with DMD | Free circulating miRNAs in serum by qRT-PCR |
| 16 patients with DMD: ambulant (n = 8) non-ambulant (n = 8) | 8 HCs | miR-1-3p, miR-133a-3p, miR-133b, miR-199a-5p, miR-33a-5p, miR-660-5p, and miR-29c-3p | ↑ miR-133a-3p and ↓ miR-29c-3p in patients with DMD compared with HCs ↑ miR-133a-3p and miR-199a-5p in ambulant patients with DMD compared with HCs ↑ miR-133a-3p in non-ambulant patients with DMD compared with HCs | EV-derived miRNAs in serum by qRT-PCR | ||
| [95] | 2022 | 28 patients with DMD: ambulant (n = 18) non-ambulant (n = 6) | miRNA correlation with muscle injury and circulating metabolic parameters | miR-1-3p, miR-133a-3p, miR-206, miR-21-5p, miR-31-5p, miR-128-3p, and miR-144-3p | ↑ miR-133a-3p, miR-206, miR-21-5p, miR-31-5p, miR-128-3p, and miR-144-3p in ambulant compared with non-ambulant patients with DMD Positive correlation between all miRNAs and ALT, AST, and CK Negative correlation between miR-133a-3p, miR-206, miR-21-5p, miR-31-5p, miR-128-3p, and miR-144-3p and the Vignos scale score | miRNAs in serum by qRT-PCR |
| [96] | 2016 | 23 DMD carriers | 24 control women | miR-206 | ↑ miR-206 in DMD carriers ROC analysis for DMD carriers vs control women (AUC)—miR-206: (0.803), p < 0.0001 | miRNAs in serum by qRT-PCR |
| [97] | 2020 | 29 patients with DMD 29 DMD carriers | 10 HCs for each group | miR-499, miR-103a-3p, miR-223, miR-208a, miR-103a-5p, miR-206 and miR-191-5p | ↑ miR-499, miR-103a-3p and ↓ miR-208a, miR-103a-5p, miR-206, and miR-191-5p in patients with DMD compared with HCs ↑ miR-499 and miR-103a-3p and ↓ miR-208a, miR-103a-5p, miR-206, and miR-191-5p in DMD carriers compared with HCs ROC analysis showed significant values for patients with DMD vs HCs (AUC) and DMD carriers vs HCs [AUC]—miR-499: (1.000), [1.000]; miR-206: (0.887), [0.918]; miR-191-5p: (0.887), [0.932] | miRNAs in plasma by qPCR |
| [98] | 2020 | 34 DMD carriers | 33 control women | miR-1, miR-133a, miR-133b, miR-206, miR-208a, miR-208b, and miR-499 | ↑ miR-1, miR-133a, miR-133b, miR-206, miR-208a, miR-208b, and miR-499 in DMD carriers ROC analysis showed significant values for DMD carriers vs control women (AUC)—miR-1: (0.771); miR-133a: (0.701); miR-133b: (0.779); miR-206: (0.655); miR-208b: (0.730), and miR-499 (0.786) | miRNAs in serum by qRT-PCR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiełbowski, K.; Bakinowska, E.; Procyk, G.; Ziętara, M.; Pawlik, A. The Role of MicroRNA in the Pathogenesis of Duchenne Muscular Dystrophy. Int. J. Mol. Sci. 2024, 25, 6108. https://doi.org/10.3390/ijms25116108
Kiełbowski K, Bakinowska E, Procyk G, Ziętara M, Pawlik A. The Role of MicroRNA in the Pathogenesis of Duchenne Muscular Dystrophy. International Journal of Molecular Sciences. 2024; 25(11):6108. https://doi.org/10.3390/ijms25116108
Chicago/Turabian StyleKiełbowski, Kajetan, Estera Bakinowska, Grzegorz Procyk, Marta Ziętara, and Andrzej Pawlik. 2024. "The Role of MicroRNA in the Pathogenesis of Duchenne Muscular Dystrophy" International Journal of Molecular Sciences 25, no. 11: 6108. https://doi.org/10.3390/ijms25116108
APA StyleKiełbowski, K., Bakinowska, E., Procyk, G., Ziętara, M., & Pawlik, A. (2024). The Role of MicroRNA in the Pathogenesis of Duchenne Muscular Dystrophy. International Journal of Molecular Sciences, 25(11), 6108. https://doi.org/10.3390/ijms25116108