
Angiogenesis and Ovarian Cancer: What Potential Do Different Subtypes of Circulating Endothelial Cells Have for Clinical Application?



Abstract
:1. Introduction
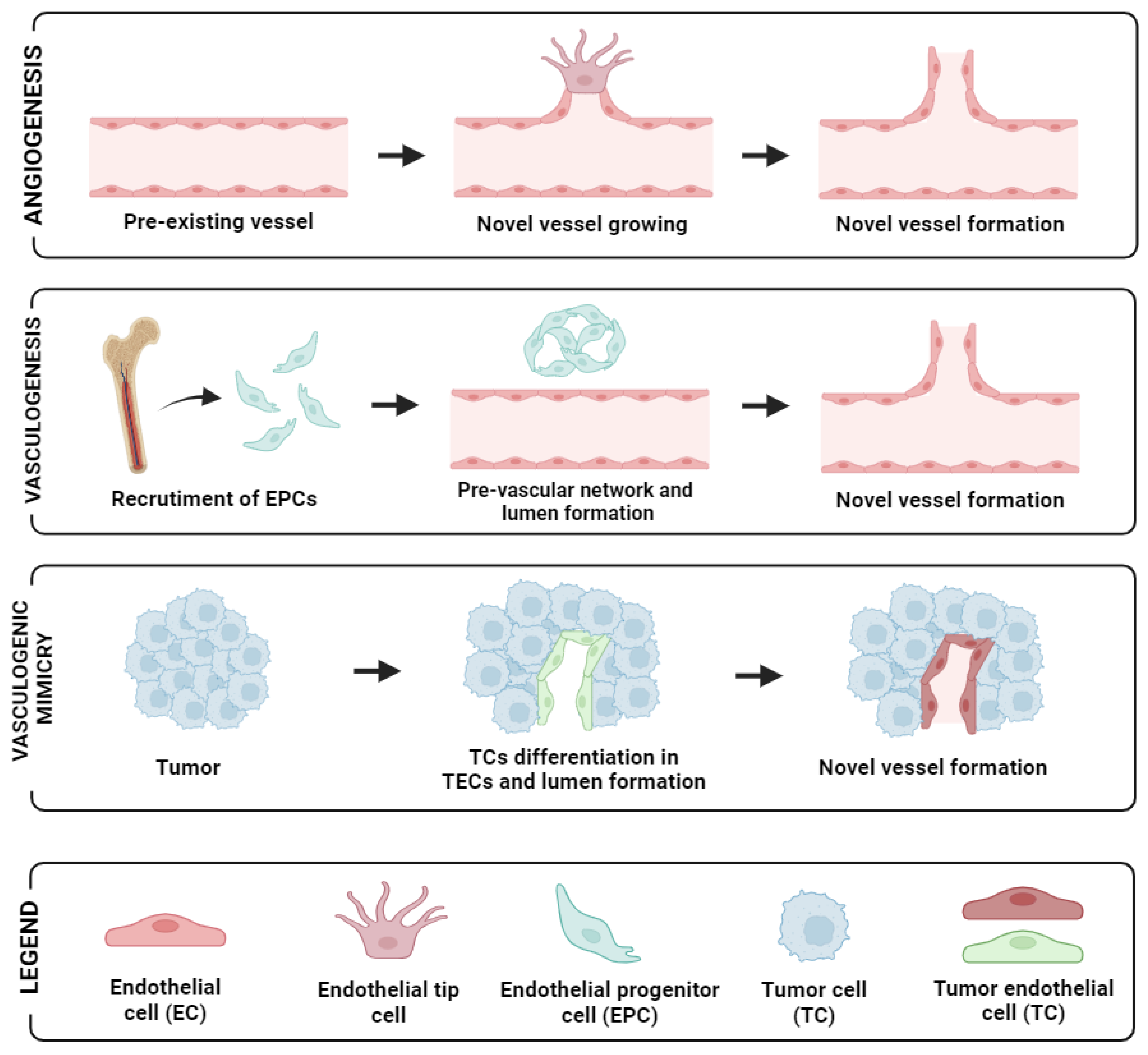
2. Endothelial Cells and Neovascularisation Process
3. Circulating Endothelial Cell Subtypes
3.1. Circulating Endothelial Cells in OC
3.2. Potential Biomarkers for the Detection of the CECs/CEPCs
3.3. Isolation Platform and Detection Method
3.4. Potential of CECs/CEPCs/CTECs as Biomarkers in Ovarian Cancer
4. Perspectives
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhang, S.; Cheng, C.; Lin, Z.; Xiao, L.; Su, X.; Zheng, L.; Mu, Y.; Liao, M.; Ouyang, R.; Li, W.; et al. The Global Burden and Associated Factors of Ovarian Cancer in 1990-2019: Findings from the Global Burden of Disease Study 2019. BMC Public Health 2022, 22, 1455. [Google Scholar] [CrossRef] [PubMed]
- Havasi, A.; Cainap, S.S.; Havasi, A.T.; Cainap, C. Ovarian Cancer—Insights into Platinum Resistance and Overcoming It. Medicina 2023, 59, 544. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Gong, Y.; Wang, Y.; Xie, J.; Cheng, J.; Huang, Q. Comprehensive Atlas of Circulating Rare Cells Detected by SE-IFISH and Image Scanning Platform in Patients with Various Diseases. Front. Oncol. 2022, 12, 821454. [Google Scholar] [CrossRef] [PubMed]
- Kraan, J.; Sleijfer, S.; Foekens, J.A.; Gratama, J.W. Clinical Value of Circulating Endothelial Cell Detection in Oncology. Drug Discov. Today 2012, 17, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, F.; Shaked, Y.; Mancuso, P.; Kerbel, R.S. The Multifaceted Circulating Endothelial Cell in Cancer: Towards Marker and Target Identification. Nat. Rev. Cancer 2006, 6, 835–845. [Google Scholar] [CrossRef] [PubMed]
- Cima, I.; Kong, S.L.; Sengupta, D.; Tan, I.B.; Phyo, W.M.; Lee, D.; Hu, M.; Iliescu, C.; Alexander, I.; Goh, W.L.; et al. Tumor-Derived Circulating Endothelial Cell Clusters in Colorectal Cancer. Sci. Transl. Med. 2016, 8, 345ra89. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J. Role of Angiogenesis in Tumor Growth and Metastasis. Semin. Oncol. 2002, 29, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Alix-Panabières, C.; Marchetti, D.; Lang, J.E. Liquid Biopsy: From Concept to Clinical Application. Sci. Rep. 2023, 13, 21685. [Google Scholar] [CrossRef] [PubMed]
- Asante, D.B.; Calapre, L.; Ziman, M.; Meniawy, T.M.; Gray, E.S. Liquid Biopsy in Ovarian Cancer Using Circulating Tumor DNA and Cells: Ready for Prime Time? Cancer Lett. 2020, 468, 59–71. [Google Scholar] [CrossRef]
- Su, Y.; Zheng, L.; Wang, Q.; Li, W.; Cai, Z.; Xiong, S.; Bao, J. Quantity and Clinical Relevance of Circulating Endothelial Progenitor Cells in Human Ovarian Cancer. J. Exp. Clin. Cancer Res. 2010, 29, 27. [Google Scholar] [CrossRef]
- Lee, J.M.; Trepel, J.B.; Choyke, P.; Cao, L.; Sissung, T.; Houston, N.; Yu, M.; Figg, W.D.; Turkbey, I.B.; Steinberg, S.M.; et al. CECs and IL-8 Have Prognostic and Predictive Utility in Patients with Recurrent Platinum-Sensitive Ovarian Cancer: Biomarker Correlates from the Randomized Phase-2 Trial of Olaparib and Cediranib Compared with Olaparib in Recurrent Platinum-Sensitive Ovarian Cancer. Front. Oncol. 2015, 5, 123. [Google Scholar] [CrossRef] [PubMed]
- Jakobsson, L.; Franco, C.A.; Bentley, K.; Collins, R.T.; Ponsioen, B.; Aspalter, I.M.; Rosewell, I.; Busse, M.; Thurston, G.; Medvinsky, A.; et al. Endothelial Cells Dynamically Compete for the Tip Cell Position during Angiogenic Sprouting. Nat. Cell Biol. 2010, 12, 943–953. [Google Scholar] [CrossRef] [PubMed]
- Donnem, T.; Reynolds, A.R.; Kuczynski, E.A.; Gatter, K.; Vermeulen, P.B.; Kerbel, R.S.; Harris, A.L.; Pezzella, F. Non-Angiogenic Tumours and Their Influence on Cancer Biology. Nat. Rev. Cancer 2018, 18, 323–336. [Google Scholar] [CrossRef] [PubMed]
- De Spiegelaere, W.; Casteleyn, C.; Van Den Broeck, W.; Plendl, J.; Bahramsoltani, M.; Simoens, P.; Djonov, V.; Cornillie, P. Intussusceptive Angiogenesis: A Biologically Relevant Form of Angiogenesis. J. Vasc. Res. 2012, 49, 390–404. [Google Scholar] [CrossRef] [PubMed]
- Gao, D.; Nolan, D.; McDonnell, K.; Vahdat, L.; Benezra, R.; Altorki, N.; Mittal, V. Bone Marrow-Derived Endothelial Progenitor Cells Contribute to the Angiogenic Switch in Tumor Growth and Metastatic Progression. Biochim. Biophys. Acta Rev. Cancer 2009, 1796, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Ronca, R.; Giacomini, A.; Rusnati, M.; Presta, M. The Potential of Fibroblast Growth Factor/Fibroblast Growth Factor Receptor Signaling as a Therapeutic Target in Tumor Angiogenesis. Expert. Opin. Ther. Targets 2015, 19, 1361–1377. [Google Scholar] [CrossRef] [PubMed]
- Krishna Priya, S.; Nagare, R.P.; Sneha, V.S.; Sidhanth, C.; Bindhya, S.; Manasa, P.; Ganesan, T.S. Tumour Angiogenesis—Origin of Blood Vessels. Int. J. Cancer 2016, 139, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Huang, J.; Sun, Y.; Guo, Q. Long-Term Progression-Free Survival of Apatinib Monotherapy for Relapsed Ovarian Cancer: A Case Report and Literature Review. Oncol. Targets Ther. 2019, 12, 3635–3644. [Google Scholar] [CrossRef] [PubMed]
- Dewhirst, M.W.; Secomb, T.W. Transport of Drugs from Blood Vessels to Tumour Tissue. Nat. Rev. Cancer 2017, 17, 738–750. [Google Scholar] [CrossRef]
- Finger, E.C.; Giaccia, A.J. Hypoxia, Inflammation, and the Tumor Microenvironment in Metastatic Disease. Cancer Metastasis Rev. 2010, 29, 285–293. [Google Scholar] [CrossRef]
- Brown, J.M. Vasculogenesis: A Crucial Player in the Resistance of Solid Tumours to Radiotherapy. Br. J. Radiol. 2014, 87. [Google Scholar] [CrossRef] [PubMed]
- Alvero, A.B.; Fu, H.H.; Holmberg, J.; Visintin, I.; Mor, L.; Marquina, C.C.; Oidtman, J.; Silasi, D.A.; Mor, G. Stem-like Ovarian Cancer Cells Can Serve as Tumor Vascular Progenitors. Stem Cells 2009, 27, 2405–2413. [Google Scholar] [CrossRef] [PubMed]
- Baba, F.; Yajid, A.I.; Nafi, S.N.M.; Hamid, S.A.A.; Adnan, W.N.A.W.; Jalil, N.A.C. Endocan-Microvascular Density in Primary Ovarian Carcinoma. Asian Pac. J. Cancer Prev. 2022, 23, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Luo, Q.; Wang, J.; Zhao, W.; Peng, Z.; Liu, X.; Li, B.; Zhang, H.; Shan, B.; Zhang, C.; Duan, C. Vasculogenic Mimicry in Carcinogenesis and Clinical Applications. J. Hematol. Oncol. 2020, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- Millimaggi, D.; Mari, M.; D’Ascenzo, S.; Giusti, I.; Pavan, A.; Dolo, V. Vasculogenic Mimicry of Human Ovarian Cancer Cells: Role of CD147. Int. J. Oncol. 2009, 35, 1423–1428. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Chen, Y.; Zhang, M.; Zhou, H.; Wu, H. Relationship between Cd177 and the Vasculogenic Mimicry, Clinicopathological Parameters, and Prognosis of Epithelial Ovarian Cancer. Ann. Palliat. Med. 2020, 9, 3985–3992. [Google Scholar] [CrossRef] [PubMed]
- Onyeisi, J.O.S.; Pernambuco Filho, P.C.D.A.; Mesquita, A.P.D.S.; de Azevedo, L.C.; Nader, H.B.; Lopes, C.C. Effects of Syndecan-4 Gene Silencing by Micro RNA Interference in Anoikis Resistant Endothelial Cells: Syndecan-4 Silencing and Anoikis Resistance. Int. J. Biochem. Cell Biol. 2020, 128, 105848. [Google Scholar] [CrossRef]
- Pyaskovskaya, O.N.; Kolesnik, D.L.; Garmanchouk, L.V.; Yanish, Y.V.; Solyanik, G.I. Role of Tumor/Endothelial Cell Interactions in Tumor Growth and Metastasis. Exp. Oncol. 2021, 43, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Rowand, J.L.; Martin, G.; Doyle, G.V.; Miller, M.C.; Pierce, M.S.; Connelly, M.C.; Rao, C.; Terstappen, L.W.M.M. Endothelial Cells in Peripheral Blood of Healthy Subjects and Patients with Metastatic Carcinomas. Cytom. Part A 2007, 71, 105–113. [Google Scholar] [CrossRef]
- Yu, H.K.; Lee, H.J.; Choi, H.N.; Ahn, J.H.; Choi, J.Y.; Song, H.S.; Lee, K.H.; Yoon, Y.; Yi, L.S.H.; Kim, J.S.; et al. Characterization of CD45-/CD31+/CD105+ Circulating Cells in the Peripheral Blood of Patients with Gynecologic Malignancies. Clin. Cancer Res. 2013, 19, 5340–5350. [Google Scholar] [CrossRef]
- Zhang, J.; Hong, Y.; Wang, L.; Hu, W.; Tian, G.; Wu, D.; Wang, Y.; Dai, L.; Zhang, Z.; Yang, Y.; et al. Aneuploid Subtypes of Circulating Tumor Cells and Circulating Tumor-Derived Endothelial Cells Predict the Overall Survival of Advanced Lung Cancer. Front. Oncol. 2023, 13, 829054. [Google Scholar] [CrossRef] [PubMed]
- Beerepoot, L.V.; Mehra, N.; Vermaat, J.S.P.; Zonnenberg, B.A.; Gebbink, M.F.G.B.; Voest, E.E. Increased Levels of Viable Circulating Endothelial Cells Are an Indicator of Progressive Disease in Cancer Patients. Ann. Oncol. 2004, 15, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Wang, S.; Luan, W.; Ye, X.; Dou, S.; Tang, Z.; Zhu, H.; Ping Lin, P.; Li, Y.; Cui, H.; et al. Combined Detection and Subclass Characteristics Analysis of CTCs and CTECs by SE-IFISH in Ovarian Cancer. Chin. J. Cancer Res. 2021, 33, 256–270. [Google Scholar] [CrossRef]
- Kim, Y.B.; Chung, Y.W.; Bae, H.S.; Lee, J.K.; Lee, N.W.; Lee, K.W.; Song, J.Y. Circulating Endothelial Progenitor Cells in Gynaecological Cancer. J. Int. Med. Res. 2013, 41, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Po, J.W.; Roohullah, A.; Lynch, D.; DeFazio, A.; Harrison, M.; Harnett, P.R.; Kennedy, C.; de Souza, P.; Becker, T.M. Improved Ovarian Cancer EMT-CTC Isolation by Immunomagnetic Targeting of Epithelial EpCAM and Mesenchymal N-Cadherin. J. Circ. Biomark. 2018, 7, 1849454418782617. [Google Scholar] [CrossRef]
- Qiu, H.; Cao, L.; Wang, D.; Xu, H.; Liang, Z. High Levels of Circulating CD34+/VEGFR3+ Lymphatic/Vascular Endothelial Progenitor Cells Is Correlated with Lymph Node Metastasis in Patients with Epithelial Ovarian Cancer. J. Obstet. Gynaecol. Res. 2013, 39, 1268–1275. [Google Scholar] [CrossRef]
- Schilder, R.J.; Sill, M.W.; Lankes, H.A.; Gold, M.A.; Mannel, R.S.; Modesitt, S.C.; Hanjani, P.; Bonebrake, A.J.; Sood, A.K.; Godwin, A.K.; et al. A Phase II Evaluation of Motesanib (AMG 706) in the Treatment of Persistent or Recurrent Ovarian, Fallopian Tube and Primary Peritoneal Carcinomas: A Gynecologic Oncology Group Study. Gynecol. Oncol. 2013, 129, 86–91. [Google Scholar] [CrossRef]
- Su, Y.; Zheng, L.; Wang, Q.; Bao, J.; Cai, Z.; Liu, A. The PI3K/Akt Pathway Upregulates Id1 and Integrin A4 to Enhance Recruitment of Human Ovarian Cancer Endothelial Progenitor Cells. BMC Cancer 2010, 10, 459. [Google Scholar] [CrossRef]
- Su, Y.; Gao, L.; Teng, L.; Wang, Y.; Cui, J.; Peng, S.; Fu, S. Id1 Enhances Human Ovarian Cancer Endothelial Progenitor Cell Angiogenesis via PI3K/Akt and NF-ΚB/MMP-2 Signaling Pathways. J. Transl. Med. 2013, 11, 132–138. [Google Scholar] [CrossRef]
- Asante, D.B.; Morici, M.; Mohan, G.R.K.A.; Acheampong, E.; Spencer, I.; Lin, W.; van Miert, P.; Gibson, S.; Beasley, A.B.; Ziman, M.; et al. Multi-Marker Immunofluorescent Staining and Pd-L1 Detection on Circulating Tumour Cells from Ovarian Cancer Patients. Cancers 2021, 13, 6225. [Google Scholar] [CrossRef]
- Lin, P.P.; Gires, O.; Wang, D.D.; Li, L.; Wang, H. Comprehensive in Situ Co-Detection of Aneuploid Circulating Endothelial and Tumor Cells. Sci. Rep. 2017, 7, 9789. [Google Scholar] [CrossRef]
- Rabascio, C.; Muratori, E.; Mancuso, P.; Calleri, A.; Raia, V.; Foutz, T.; Cinieri, S.; Veronesi, G.; Pruneri, G.; Lampertico, P.; et al. Assessing Tumor Angiogenesis: Increased Circulating VE-Cadherin RNA in Patients with Cancer Indicates Viability of Circulating Endothelial Cells. Cancer Res. 2004, 64, 4373–4377. [Google Scholar] [CrossRef]
- Ostrand-Rosenberg, S.; Horn, L.A.; Haile, S.T. The Programmed Death-1 Immune-Suppressive Pathway: Barrier to Antitumor Immunity. J. Immunol. 2014, 193, 3835–3841. [Google Scholar] [CrossRef]
- Romano, S.; Tufano, M.; D’Arrigo, P.; Vigorito, V.; Russo, S.; Romano, M.F. Cell Stemness, Epithelial-to-Mesenchymal Transition, and Immunoevasion: Intertwined Aspects in Cancer Metastasis. Semin. Cancer Biol. 2020, 60, 181–190. [Google Scholar] [CrossRef]
- Georganaki, M.; van Hooren, L.; Dimberg, A. Vascular Targeting to Increase the Efficiency of Immune Checkpoint Blockade in Cancer. Front. Immunol. 2018, 9, 3081. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, X.; Liu, Y.; Zhang, T.; Wang, Z.; Gu, M.; Li, Y.; Wang, D.D.; Li, W.; Lin, P.P. PD-L1+ Aneuploid Circulating Tumor Endothelial Cells (CTECs) Exhibit Resistance to the Checkpoint Blockade Immunotherapy in Advanced NSCLC Patients. Cancer Lett. 2020, 469, 355–366. [Google Scholar] [CrossRef]
- Musso, N.; Romano, A.; Bonacci, P.G.; Scandura, G.; Pandino, C.; Camarda, M.; Russo, G.I.; Di Raimondo, F.; Cacciola, E.; Cacciola, R. Label-Free Enrichment of Circulating Tumor Plasma Cells: Future Potential Applications of Dielectrophoresis in Multiple Myeloma. Int. J. Mol. Sci. 2022, 23, 12052. [Google Scholar] [CrossRef]
- Asante, D.B.; Mohan, G.R.K.A.; Acheampong, E.; Ziman, M.; Calapre, L.; Meniawy, T.M.; Gray, E.S.; Beasley, A.B. Genetic Analysis of Heterogeneous Subsets of Circulating Tumour Cells from High Grade Serous Ovarian Carcinoma Patients. Sci. Rep. 2023, 13, 2552. [Google Scholar] [CrossRef]
- Mehran, R.; Nilsson, M.; Khajavi, M.; Du, Z.; Cascone, T.; Wu, H.K.; Cortes, A.; Xu, L.; Zurita, A.; Schier, R.; et al. Tumor Endothelial Markers Define Novel Subsets of Cancer-Specific Circulating Endothelial Cells Associated with Antitumor Efficacy. Cancer Res. 2014, 74, 2731–2741. [Google Scholar] [CrossRef]
- Mancuso, P.; Burlini, A.; Pruneri, G.; Goldhirsch, A.; Martinelli, G.; Bertolini, F. Resting and Activated Endothelial Cells Are Increased in the Peripheral Blood of Cancer Patients. Blood 2001, 97, 3658–3661. [Google Scholar] [CrossRef]
- Ronzoni, M.; Manzoni, M.; Mariucci, S.; Loupakis, F.; Brugnatelli, S.; Bencardino, K.; Rovati, B.; Tinelli, C.; Falcone, A.; Villa, E.; et al. Circulating Endothelial Cells and Endothelial Progenitors as Predictive Markers of Clinical Response to Bevacizumab-Based First-Line Treatment in Advanced Colorectal Cancer Patients. Ann. Oncol. 2010, 21, 2382–2389. [Google Scholar] [CrossRef]
- Adams, D.L.; Alpaugh, R.K.; Tsai, S.; Tang, C.M.; Stefansson, S. Multi-Phenotypic Subtyping of Circulating Tumor Cells Using Sequential Fluorescent Quenching and Restaining. Sci. Rep. 2016, 6, 33488. [Google Scholar] [CrossRef]
- Waldman, A.D.; Fritz, J.M.; Lenardo, M.J. A Guide to Cancer Immunotherapy: From T Cell Basic Science to Clinical Practice. Nat. Rev. Immunol. 2020, 20, 651–668. [Google Scholar] [CrossRef]
- Yang, C.; Xia, B.R.; Zhang, Z.C.; Zhang, Y.J.; Lou, G.; Jin, W.L. Immunotherapy for Ovarian Cancer: Adjuvant, Combination, and Neoadjuvant. Front. Immunol. 2020, 11, 577869. [Google Scholar] [CrossRef]
- Mei, C.; Gong, W.; Wang, X.; Lv, Y.; Zhang, Y.; Wu, S.; Zhu, C. Anti-Angiogenic Therapy in Ovarian Cancer: Current Understandings and Prospects of Precision Medicine. Front. Pharmacol. 2023, 14, 1147717. [Google Scholar] [CrossRef]
- Arend, R.C.; Jackson-Fisher, A.; Jacobs, I.A.; Chou, J.; Monk, B.J. Ovarian Cancer: New Strategies and Emerging Targets for the Treatment of Patients with Advanced Disease. Cancer Biol. Ther. 2021, 22, 89–105. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Subtypes (Stage) | Isolation Platform | Method of Detection | Biomarkers Used for Detection | CECs/CEPCs/CTECs | Cit. |
|---|---|---|---|---|---|
| HGSOC (III-IV) | Parsortix (Microfluidics) | Immunofluerescence | CD31 | CECs | [40] |
| / | Immunomagnetic | Immunostaining and fluorescence in situ hybridisation (iFISH) | CD31 aneuploidy | CTECs | [33] |
| HGSOC, clear cell carcinoma | Immunomagnetic cell surface target | Immunofluorescence | VE-cad | CECs | [35] |
| HGSOC (platinum sensitive) | Density gradient centrifugation | Flow cytometry | CD31, CD146 CD133 | CECs, CEPCS | [11] |
| Serous and mucinous (IB, IIA, IIB, IIIC) | Density gradient centrifugation | Quadruple immunofluorescence | CD34, CD133 | CEPCs | [34] |
| Serous, endometroid, and mucinous (FIGO I-IV) and clear cell | Density centrifugation | Flow cytometry | CD34 | CEPCs | [36] |
| Serous, mucinous, and endometroid | Density gradient centrifugation | Immunofluorescence | CD31 | CEPCs | [39] |
| Clear cell, endometroid, and serous | Immunomagnetic | Immunofluorescence | CD34, CD-133 CD-146 | CEPCs, CECs | [37] |
| Serous, mucinous and endometrioid (I–IV) | Immunomagnetic | Flow cytometry, RT-PCR | CD34 | CEPCs | [38] |
| Serous, mucinous and endometroid | Density gradient centrifugation | Immunofluorescence | CD31 | CEPCs | [10] |
| / | Immunomagnetic | Immunofluorescence | CD31 | CECs | [32] |
| Patients/ Control (n/n) | Stage | Circulating Endothelial Cell Types/Clinical Value | Markers of Therapeutic Importance | Main Clinical Findings | Cit. |
|---|---|---|---|---|---|
| P/HC(16/5) | I-IV | CECs Diagnostic, Predictive | PD-L1 | Subsets of CD31+ in OC patients were PD-L1+/CK+/EpCAM+. | [40] |
| P/HC(20/36) | NR | CTECs Diagnostic | / | CTEC levels were higher in OC patients than in benign cases. However, the difference was not significant. | [33] |
| P(13) | NR | CECs and CEPCs Prognostic | / | Patients who received a combination of Olaparib and Cediranib had significant decrease in IL-8 concentration and CECs numbers, compared with patients who received Olaparib alone. | [11] |
| P/HC(14/14) | IB, IIA, IIB, IIIC | CEPCs Diagnostic, Prognostic | VEGFR-2 | Patients who underwent chemoradiation therapy or surgery had a reduced frequency and number of CEPCs compared to pre-treatment values. | [34] |
| P/HC(54/31) | I–IV | CEPCs Diagnostic, Predictive | VEGFR-3 | CEPC levels were higher in OC patients compared with healthy controls, and the increase in CEPC levels correlated with lymph node metastasis. | [36] |
| P(22) | NR | CECs and CEPCs / | vWF, VEGFR-2 | CPEC/CEC levels were higher in second/third cycles of treatments compared to the first one. This could be due to the side-effects of Motesanib. | [37] |
| P/HC(22/15) | NR | CEPCs Diagnostic | VEGFR-2 | CEPCs from OC patients showed increased expression of Id1 and MMP-2 compared to those from healthy controls. Id1 was involved in stimulation of angiogenesis, tumour proliferation and migration via PIK3CA/Akt and NF-kB/MMP2 pathway. | [39] |
| P/HC(42/25) | I–IV | CEPCs Diagnostic, Prognostic | VEGFR-2 | CEPCs levels significantly increased in in OC patients compared to healthy control. Higher levels in stages III and IV compared to stages I and II. High CEPCs count correlated with poor overall survival. | [10] |
| P/HC(20/25) | NR | CEPCs Diagnostic, Predictive | vWF, VEGFR-2 | CEPCs from OC patients showed an increased expression of Id1 and integrin α4 compared to those from healthy controls. Id1 mediated CEPCs mobilisation and recruitment. Inhibition of PI3K/Akt of cultured CEPCs from OC patients, down-regulated the expression of Id1 and integrin α4, inhibiting CEPCs mobilisation. | [38] |
| P/HC(95/46) | NR | CECs Diagnostic, Predictive | VEGFR-2 | Compared to healthy cohort, OC patients with progressing disease exhibited an average of 3.6 times higher CECs. CECs levels in OC patients with stable disease were similar to those of healthy controls. | [32] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asante, D.-B.; Tierno, D.; Woode, M.; Scaggiante, B. Angiogenesis and Ovarian Cancer: What Potential Do Different Subtypes of Circulating Endothelial Cells Have for Clinical Application? Int. J. Mol. Sci. 2024, 25, 6283. https://doi.org/10.3390/ijms25116283
Asante D-B, Tierno D, Woode M, Scaggiante B. Angiogenesis and Ovarian Cancer: What Potential Do Different Subtypes of Circulating Endothelial Cells Have for Clinical Application? International Journal of Molecular Sciences. 2024; 25(11):6283. https://doi.org/10.3390/ijms25116283
Chicago/Turabian StyleAsante, Du-Bois, Domenico Tierno, Michael Woode, and Bruna Scaggiante. 2024. "Angiogenesis and Ovarian Cancer: What Potential Do Different Subtypes of Circulating Endothelial Cells Have for Clinical Application?" International Journal of Molecular Sciences 25, no. 11: 6283. https://doi.org/10.3390/ijms25116283
APA StyleAsante, D.-B., Tierno, D., Woode, M., & Scaggiante, B. (2024). Angiogenesis and Ovarian Cancer: What Potential Do Different Subtypes of Circulating Endothelial Cells Have for Clinical Application? International Journal of Molecular Sciences, 25(11), 6283. https://doi.org/10.3390/ijms25116283