
Exploring the Role of Vitamin D, Vitamin D-Dependent Proteins, and Vitamin D Receptor Gene Variation in Lung Cancer Risk
 , , , and
, , , and
Abstract
:1. Introduction
2. The Role of Vitamin D and Vitamin D Receptor in Immunity and Carcinogenesis
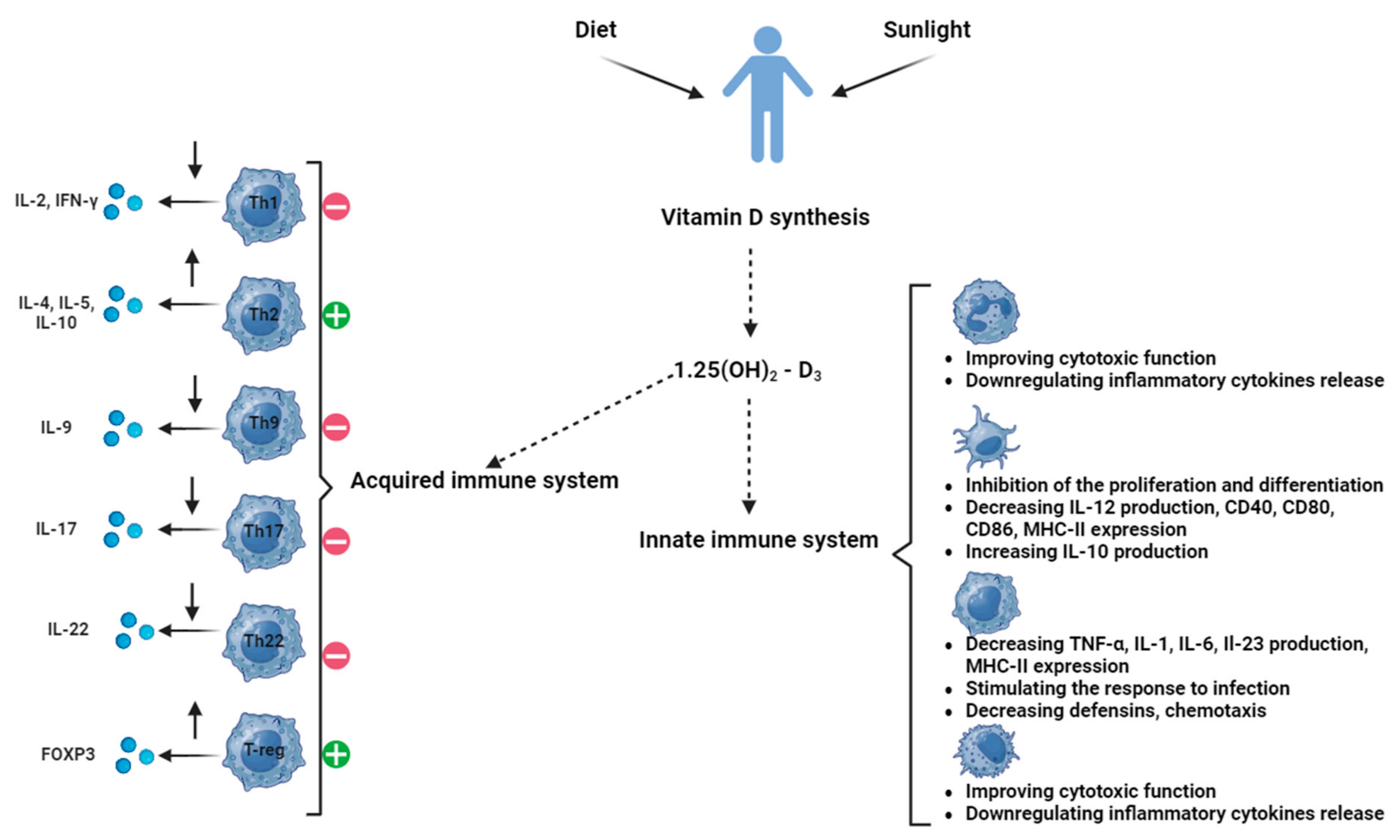
2.1. Vitamin D and Its Role in Immunity and Carcinogenesis
2.2. Vitamin D-Dependent Proteins in Lung Cancer
2.3. Vitamin D Receptor in Lung Pathology
3. Vitamin D Receptor Gene Variation and Lung Cancer Risk
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- INSP Profil de Țară Privind Cancerul. Available online: https://insp.gov.ro/wp-content/uploads/2024/03/Profil-de-tara-privind-cancerul-2023.pdf (accessed on 4 June 2024).
- Smith, R.A.; Andrews, K.S.; Brooks, D.; Fedewa, S.A.; Manassaram-Baptiste, D.; Saslow, D.; Brawley, O.W.; Wender, R.C. Cancer Screening in the United States, 2018: A Review of Current American Cancer Society Guidelines and Current Issues in Cancer Screening. CA Cancer J. Clin. 2018, 68, 297–316. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Newman, T.G.; Aronow, W.S. Lung Cancer Screening: History, Current Perspectives, and Future Directions. Arch. Med. Sci. 2015, 11, 1033–1043. [Google Scholar] [CrossRef] [PubMed]
- Wolf, A.M.D.; Oeffinger, K.C.; Tina, Y.-C.S.; Walter, L.C.; Church, T.R.; Fontham, E.T.H.; Elkin, E.B.; Ruth, R.D.; Guerra, C.E.; Perkins, R.B.; et al. Screening for Lung Cancer: 2023 Guideline Update from the American Cancer Society. CA Cancer J. Clin. 2024, 74, 50–81. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, J.; Malvezzi, M.; Negri, E.; La Vecchia, C.; Boffetta, P. Risk Factors for Lung Cancer Worldwide. Eur. Respir. J. 2016, 48, 889–902. [Google Scholar] [CrossRef] [PubMed]
- Pesch, B.; Kendzia, B.; Gustavsson, P.; Jöckel, K.H.; Johnen, G.; Pohlabeln, H.; Olsson, A.; Ahrens, W.; Gross, I.M.; Brüske, I.; et al. Cigarette Smoking and Lung Cancer—Relative Risk Estimates for the Major Histological Types from a Pooled Analysis of Case—Control Studies. Int. J. Cancer 2012, 131, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, N.; Bansal, J.G. Risk Factors of Lung Cancer in Nonsmoker. Curr. Probl. Cancer 2017, 41, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Pan, Z.; Cai, X.; Wang, W.; Guo, C.; He, J.; Chen, Y.; Liu, Z.; Wang, B.; He, J.; et al. The Association between Human Papillomavirus Presence and Epidermal Growth Factor Receptor Mutations in Asian Patients with Non-Small Cell Lung Cancer. Transl. Lung Cancer Res. 2018, 7, 397–403. [Google Scholar] [CrossRef]
- Thanoon, M.A.; Zulkifley, M.A.; Mohd Zainuri, M.A.A.; Abdani, S.R. A Review of Deep Learning Techniques for Lung Cancer Screening and Diagnosis Based on CT Images. Diagnostics 2023, 13, 2617. [Google Scholar] [CrossRef]
- Manser, R.; Lethaby, A.; Irving, L.B.; Stone, C.; Byrnes, G.; Abramson, M.J.; Campbell, D. Screening for Lung Cancer. Cochrane Database Syst. Rev. 2013, 2013. [Google Scholar] [CrossRef]
- Nooreldeen, R.; Bach, H. Current and Future Development in Lung Cancer Diagnosis. Int. J. Mol. Sci. 2021, 22, 8661. [Google Scholar] [CrossRef]
- Knight, S.B.; Crosbie, P.A.; Balata, H.; Chudziak, J.; Hussell, T.; Dive, C. Progress and Prospects of Early Detection in Lung Cancer. Open Biol. 2017, 7, 170070. [Google Scholar] [CrossRef] [PubMed]
- Currie, G.P.; Kennedy, A.M.; Denison, A.R. Tools Used in the Diagnosis and Staging of Lung Cancer: What’s Old and What’s New? QJM Int. J. Med. 2009, 102, 443–448. [Google Scholar] [CrossRef]
- Park, H.J.; Lee, S.H.; Chang, Y.S. Recent Advances in Diagnostic Technologies in Lung Cancer. Korean J. Intern. Med. 2020, 35, 257. [Google Scholar] [CrossRef]
- Yup Lee, S.; Kang, H.G.; Eun Choi, J.; Kju Jung, D.; Kee Lee, W.; Chul Lee, H.; Lee, S.Y.; Soo Yoo, S.; Lee, J.; Seok, Y.; et al. Polymorphisms in Cancer-Related Pathway Genes and Lung Cancer. Eur. Respir. J. 2016, 48, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Weissfeld, J.L.; Lin, Y.; Lin, H.M.; Kurland, B.F.; Wilson, D.O.; Fuhrman, C.R.; Pennathur, A.; Romkes, M.; Nukui, T.; Yuan, J.M.; et al. Lung Cancer Risk Prediction Using Common SNPs Located in GWAS-Identified Susceptibility Regions. J. Thorac. Oncol. 2015, 10, 1538. [Google Scholar] [CrossRef]
- Wang, Y.; Ma, R.; Liu, B.; Kong, J.; Lin, H.; Yu, X.; Wang, R.; Li, L.; Gao, M.; Zhou, B.; et al. SNP Rs17079281 Decreases Lung Cancer Risk through Creating an YY1-Binding Site to Suppress DCBLD1 Expression. Oncogene 2020, 39, 4092–4102. [Google Scholar] [CrossRef]
- Bernig, T.; Chanock, S.J. Challenges of SNP Genotyping and Genetic Variation: Its Future Role in Diagnosis and Treatment of Cancer. Expert Rev. Mol. Diagn. 2006, 6, 319–331. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Gao, G.; Li, X.; Ren, S.; Li, A.; Xu, J.; Zhang, J.; Zhou, C. Association between Single Nucleotide Polymorphisms (SNPs) and Toxicity of Advanced Non-Small-Cell Lung Cancer Patients Treated with Chemotherapy. PLoS ONE 2012, 7, e48350. [Google Scholar] [CrossRef]
- Sapkota, Y.; Mackey, J.R.; Lai, R.; Franco-Villalobos, C.; Lupichuk, S.; Robson, P.J.; Kopciuk, K.; Cass, C.E.; Yasui, Y.; Damaraju, S. Assessing SNP-SNP Interactions among DNA Repair, Modification and Metabolism Related Pathway Genes in Breast Cancer Susceptibility. PLoS ONE 2013, 8, e64896. [Google Scholar] [CrossRef]
- Goodman, J.E.; Mechanic, L.E.; Luke, B.T.; Ambs, S.; Chanock, S.; Harris, C.C. Exploring SNP-SNP Interactions and Colon Cancer Risk Using Polymorphism Interaction Analysis. Int. J. Cancer 2006, 118, 1790–1797. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, S.; Che, X.; Li, X. Vitamin D and Lung Cancer Risk: A Comprehensive Review and Meta-Analysis. Cell. Physiol. Biochem. 2015, 36, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Fleet, J.C. Molecular Actions of Vitamin D Contributing to Cancer Prevention. Mol. Asp. Med. 2008, 29, 388–396. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D: Its Role in Cancer Prevention and Treatment. Prog. Biophys. Mol. Biol. 2006, 92, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Hu, W.; Xue, S.; Chen, Q.; Jiang, Y.; Zhang, H.; Zuo, W. Vitamin D and Lung Cancer; Association, Prevention, and Treatment. Nutr. Cancer 2021, 73, 2188–2200. [Google Scholar] [CrossRef] [PubMed]
- Fleet, J.C.; Desmet, M.; Johnson, R.; Li, Y. Vitamin D and Cancer: A Review of Molecular Mechanisms. Biochem. J. 2012, 441, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Tagliabue, E.; Raimondi, S.; Gandini, S. Vitamin D, Cancer Risk, and Mortality. Adv. Food Nutr. Res. 2015, 75, 1–52. [Google Scholar] [CrossRef]
- Miraglia del Giudice, M.; Indolfi, C.; Strisciuglio, C. Vitamin D. J. Clin. Gastroenterol. 2018, 52, S86–S88. [Google Scholar] [CrossRef]
- Armas, L.A.G.; Hollis, B.W.; Heaney, R.P. Vitamin D2 Is Much Less Effective than Vitamin D3 in Humans. J. Clin. Endocrinol. Metab. 2004, 89, 5387–5391. [Google Scholar] [CrossRef] [PubMed]
- Ao, T.; Kikuta, J.; Ishii, M. The Effects of Vitamin D on Immune System and Inflammatory Diseases. Biomolecules 2021, 11, 1624. [Google Scholar] [CrossRef]
- Carlberg, C. Vitamin D Signaling in the Context of Innate Immunity: Focus on Human Monocytes. Front. Immunol. 2019, 10, 2211. [Google Scholar] [CrossRef]
- Skrobot, A.; Demkow, U.; Wachowska, M. Immunomodulatory Role of Vitamin D: A Review. Adv. Exp. Med. Biol. 2018, 1108, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Penna, G.; Adorini, L. 1α,25-Dihydroxyvitamin D3 Inhibits Differentiation, Maturation, Activation, and Survival of Dendritic Cells Leading to Impaired Alloreactive T Cell Activation. J. Immunol. 2000, 164, 2405–2411. [Google Scholar] [CrossRef] [PubMed]
- Urry, Z.; Chambers, E.S.; Xystrakis, E.; Dimeloe, S.; Richards, D.F.; Gabryšová, L.; Christensen, J.; Gupta, A.; Saglani, S.; Bush, A.; et al. The Role of 1α,25-Dihydroxyvitamin D3 and Cytokines in the Promotion of Distinct Foxp3+and IL-10+ CD4+ T Cells. Eur. J. Immunol. 2012, 42, 2697–2708. [Google Scholar] [CrossRef] [PubMed]
- Menezes, R.J.; Cheney, R.T.; Husain, A.; Tretiakova, M.; Loewen, G.; Johnson, C.S.; Jayaprakash, V.; Moysich, K.B.; Salgia, R.; Reid, M.E. Vitamin D Receptor Expression in Normal, Premalignant, and Malignant Human Lung Tissue. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1104. [Google Scholar] [CrossRef] [PubMed]
- Sirajudeen, S.; Shah, I.; Al Menhali, A. A Narrative Role of Vitamin d and Its Receptor: With Current Evidence on the Gastric Tissues. Int. J. Mol. Sci. 2019, 20, 3832. [Google Scholar] [CrossRef] [PubMed]
- DeLuca, H.F. Overview of General Physiologic Features and Functions of Vitamin D. Am. J. Clin. Nutr. 2004, 80, 1689S–1696S. [Google Scholar] [CrossRef] [PubMed]
- Pop, T.L.; Sîrbe, C.; Benţa, G.; Mititelu, A.; Grama, A. The Role of Vitamin D and Vitamin D Binding Protein in Chronic Liver Diseases. Int. J. Mol. Sci. 2022, 23, 10705. [Google Scholar] [CrossRef] [PubMed]
- Zmijewski, M.A. Vitamin D and Human Health. Int. J. Mol. Sci. 2019, 20, 145. [Google Scholar] [CrossRef] [PubMed]
- Norton, R. Effects of Vitamin D on Inflammation and Oxidative Stress in Airway Epithelial Cells. Ph.D. Thesis, University of East Anglia, Norwich, UK, 2012. [Google Scholar]
- Boughanem, H.; Canudas, S.; Hernandez-Alonso, P.; Becerra-tomás, N.; Babio, N.; Salas-Salvadó, J.; Macias-Gonzalez, M. Vitamin D Intake and the Risk of Colorectal Cancer: An Updated Meta-analysis and Systematic Review of Case-control and Prospective Cohort Studies. Cancers 2021, 13, 2814. [Google Scholar] [CrossRef]
- Norton, R.; O’connell, M.A. Vitamin D and Cancer Vitamin D: Potential in the Prevention and Treatment of Lung Cancer. Anticancer Res. 2012, 32, 211–221. [Google Scholar]
- Zhan, R.; Shen, X.; Ma, Z.; Li, S.; Liang, J.; Zhang, W. Dietary Vitamin D Intake and Risk of Non-Small Cell Lung Cancer: A Matched Case-Control Study. Transl. Cancer Res. 2016, 5, 470–475. [Google Scholar] [CrossRef]
- Ramnath, N.; Kim, S.H.; Christensen, P.J. Vitamin D and Lung Cancer. Expert Rev. Respir. Med. 2011, 5, 305–309. [Google Scholar] [CrossRef] [PubMed]
- McFarland, D.C.; Fernbach, M.; Breitbart, W.S.; Nelson, C. Prognosis in Metastatic Lung Cancer: Vitamin D Deficiency and Depression—A Cross-Sectional Analysis. BMJ Support. Palliat. Care 2022, 12, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Autier, P.; Boniol, M.; Pizot, C.; Mullie, P. Vitamin D Status and Ill Health: A Systematic Review. Lancet Diabetes Endocrinol. 2014, 2, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Dong, Y.; Lu, C.; Wang, Y.; Peng, L.; Jiang, M.; Tang, Y.; Zhao, Q. Meta-Analysis of the Correlation between Vitamin D and Lung Cancer Risk and Outcomes. Oncotarget 2017, 8, 81040. [Google Scholar] [CrossRef] [PubMed]
- Herr, C.; Greulich, T.; Koczulla, R.A.; Meyer, S.; Zakharkina, T.; Branscheidt, M.; Eschmann, R.; Bals, R. The Role of Vitamin D in Pulmonary Disease: COPD, Asthma, Infection, and Cancer. Respir. Res. 2011, 12, 31. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Sung, H.C.; Chuang, T.Y.; Lai, T.C.; Lee, T.L.; Lee, C.W.; Lee, I.T.; Chen, Y.L. Vitamin D3 Decreases TNF-α-Induced Inflammation in Lung Epithelial Cells through a Reduction in Mitochondrial Fission and Mitophagy. Cell Biol. Toxicol. 2022, 38, 427–450. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.R.; Chiappinelli, K.B. Protein Exaptation by Endogenous Retroviral Elements Shapes Tumor Cell Senescence and Downstream Immune Signaling. Cancer Res. 2023, 83, 2640–2642. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.S.; Son, D.S.; Kim, S.H.; Lee, J.; Jo, J.; Han, J.; Kim, H.; Hyun, J.L.; Hye, Y.C.; Jung, Y.; et al. Prediction of Recurrence-Free Survival in Postoperative Non–Small Cell Lung Cancer Patients by Using an Integrated Model of Clinical Information and Gene Expression. Clin. Cancer Res. 2008, 14, 7397–7404. [Google Scholar] [CrossRef]
- Christakos, S.; Barletta, F.; Huening, M.; Dhawan, P.; Liu, Y.; Porta, A.; Peng, X. Vitamin D Target Proteins: Function and Regulation. J. Cell. Biochem. 2003, 88, 238–244. [Google Scholar] [CrossRef]
- Jin, C.; Lin, T.; Shan, L. Downregulation of Calbindin 1 by MiR-454-3p Suppresses Cell Proliferation in Nonsmall Cell Lung Cancer In Vitro. Cancer Biother. Radiopharm. 2019, 34, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Castro, C.Y.; Stephenson, M.; Gondo, M.M.; Medeiros, L.J.; Cagle, P.T. Prognostic Implications of Calbindin-D28k Expression in Lung Cancer: Analysis of 452 Cases. Mod. Pathol. 2000, 13, 808–813. [Google Scholar] [CrossRef]
- Mingxia, D. MiR-186-5p Inhibits Talignant Phenotypes of Prostate Cancer by Regulating CALB1 Clinics of Oncology. Clin. Oncol. 2022, 6, 1–8. [Google Scholar]
- Dowd, D.R.; MacDonald, P.N.; Komm, B.S.; Haussler, M.R.; Miesfeld, R.L. Stable Expression of the Calbindin-D28K Complementary DNA Interferes with the Apoptotic Pathway in Lymphocytes. Mol. Endocrinol. 1992, 6, 1843–1848. [Google Scholar] [CrossRef] [PubMed]
- Blum, W.; Pecze, L.; Rodriguez, J.W.; Steinauer, M.; Schwaller, B. Regulation of Calretinin in Malignant Mesothelioma Is Mediated by Septin 7 Binding to the CALB2 Promoter. BMC Cancer 2018, 18, 475. [Google Scholar] [CrossRef]
- Liu, C.; Chen, J.; Liao, J.; Li, Y.; Yu, H.; Zhao, X.; Sun, S.; Hu, Z.; Zhang, Y.; Zhu, Z.; et al. Plasma Extracellular Vesicle Long RNA in Diagnosis and Prediction in Small Cell Lung Cancer. Cancers 2022, 14, 5493. [Google Scholar] [CrossRef] [PubMed]
- Gueugnon, F.; Leclercq, S.; Blanquart, C.; Sagan, C.; Cellerin, L.; Padieu, M.; Perigaud, C.; Scherpereel, A.; Gregoire, M. Identification of Novel Markers for the Diagnosis of Malignant Pleural Mesothelioma. Am. J. Pathol. 2011, 178, 1033–1042. [Google Scholar] [CrossRef]
- Liu, Y.; Cui, J.; Tang, Y.L.; Huang, L.; Zhou, C.Y.; Xu, J.X. Prognostic Roles of MRNA Expression of S100 in Non-Small-Cell Lung Cancer. Biomed. Res. Int. 2018, 2018, 9815806. [Google Scholar] [CrossRef]
- Allgower, C.; Kretz, A.-L.; von Karstedt, S.; Wittau, M.; Henne-Bruns, D.; Lemke, J. Friend or Foe: S100 Proteins in Cancer. Cancers 2020, 12, 2037. [Google Scholar] [CrossRef]
- Acharya, M.; Singh, N.; Gupta, G.; Tambuwala, M.M.; Aljabali, A.A.A.; Chellappan, D.K.; Dua, K.; Goyal, R. Vitamin D, Calbindin, and Calcium Signaling: Unraveling the Alzheimer’s Connection. Cell Signal. 2024, 116, 111043. [Google Scholar] [CrossRef]
- Cao, L.Q.; Wang, Y.N.; Liang, M.; Pan, M.Z. CALB1 Enhances the Interaction between P53 and MDM2, and Inhibits the Senescence of Ovarian Cancer Cells. Mol. Med. Rep. 2019, 19, 5097–5104. [Google Scholar] [CrossRef] [PubMed]
- Jurutka, P.W.; Remus, L.S.; Whitfield, G.K.; Thompson, P.D.; Hsieh, J.C.; Zitzer, H.; Tavakkoli, P.; Galligan, M.A.; Dang, H.T.L.; Haussler, C.A.; et al. The Polymorphic N Terminus in Human Vitamin D Receptor Isoforms Influences Transcriptional Activity by Modulating Interaction with Transcription Factor IIB. Mol. Endocrinol. 2000, 14, 401–420. [Google Scholar] [CrossRef] [PubMed]
- Tamura, M.; Ishizawa, M.; Isojima, T.; Özen, S.; Oka, A.; Makishima, M.; Kitanaka, S. Functional Analyses of a Novel Missense and Other Mutations of the Vitamin D Receptor in Association with Alopecia. Sci. Rep. 2017, 7, 5102. [Google Scholar] [CrossRef]
- Goltzman, D. Functions of Vitamin D in Bone. Histochem. Cell Biol. 2018, 149, 305–312. [Google Scholar] [CrossRef]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2015, 96, 365–408. [Google Scholar] [CrossRef]
- Zhang, Y.G.; Wu, S.; Lu, R.; Zhou, D.; Zhou, J.; Carmeliet, G.; Petrof, E.; Claud, E.C.; Sun, J. Tight Junction CLDN2 Gene Is a Direct Target of the Vitamin D Receptor. Sci. Rep. 2015, 5, 10642. [Google Scholar] [CrossRef]
- Vaughan-Shaw, P.G.; O’Sullivan, F.; Farrington, S.M.; Theodoratou, E.; Campbell, H.; Dunlop, M.G.; Zgaga, L. The Impact of Vitamin D Pathway Genetic Variation and Circulating 25-HydroxyVitamin D on Cancer Outcome: Systematic Review and Meta-Analysis. Br. J. Cancer 2017, 116, 1095–1110. [Google Scholar] [CrossRef]
- Deuster, E.; Jeschke, U.; Ye, Y.; Mahner, S.; Czogalla, B. Vitamin D and VDR in Gynecological Cancers-A Systematic Review. Int. J. Mol. Sci. 2017, 18, 2328. [Google Scholar] [CrossRef] [PubMed]
- Gheliji, T.; Oskooei, V.K.; Ashrafi Hafez, A.; Taheri, M.; Ghafouri-Fard, S. Evaluation of Expression of Vitamin D Receptor Related LncRNAs in Lung Cancer. Noncoding RNA Res. 2020, 5, 83. [Google Scholar] [CrossRef]
- Fathi, N.; Ahmadian, E.; Shahi, S.; Roshangar, L.; Khan, H.; Kouhsoltani, M.; Maleki Dizaj, S.; Sharifi, S. Role of Vitamin D and Vitamin D Receptor (VDR) in Oral Cancer. Biomed. Pharmacother. 2019, 109, 391–401. [Google Scholar] [CrossRef]
- Duan, G.Q.; Zheng, X.; Li, W.K.; Zhang, W.; Li, Z.; Tan, W. The Association between VDR and GC Polymorphisms and Lung Cancer Risk: A Systematic Review and Meta-Analysis. Genet. Test Mol. Biomark. 2020, 24, 285–295. [Google Scholar] [CrossRef]
- Kim, S.H.; Chen, G.; King, A.N.; Jeon, C.K.; Christensen, P.J.; Zhao, L.; Simpson, R.U.; Thomas, D.G.; Giordano, T.J.; Brenner, D.E.; et al. Characterization of Vitamin D Receptor (VDR) in Lung Adenocarcinoma. Lung Cancer 2012, 77, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Gromowski, T.; Gapska, P.; Scott, R.J.; Kąklewski, K.; Marciniak, W.; Durda, K.; Lener, M.; Górski, B.; Cybulski, C.; Sukiennicki, G.; et al. Serum 25(OH)D Concentration, Common Variants of the VDR Gene and Lung Cancer Occurrence. Int. J. Cancer 2017, 141, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Xiong, L.; Cheng, J.; Gao, J.; Wang, J.; Liu, X.; Wang, L. Vitamin D Receptor Genetic Variants Are Associated With Chemotherapy Response and Prognosis in Patients With Advanced Non–Small-Cell Lung Cancer. Clin. Lung Cancer 2013, 14, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.X.; Yang, J.X.; Hu, X.; Li, M.; Wang, Q.; Dancer, R.C.A.; Parekh, D.; Gao-Smith, F.; Thickett, D.R.; Jin, S.W. Vitamin D Attenuates Lung Injury via Stimulating Epithelial Repair, Reducing Epithelial Cell Apoptosis and Inhibits TGF-β Induced Epithelial to Mesenchymal Transition. Biochem. Pharmacol. 2020, 177, 113955. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.-H.; Chen, M.; Zhang, Q.-Q.; Hu, X. The Association of Vitamin D Receptor Gene Polymorphism with Lung Cancer Risk: An Update Meta-Analysis. Comb. Chem. High Throughput Screen 2019, 21, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Dogan, I.; Ilke Onen, H.; Yurdakul, A.; Selim Yurdakul, A.; Konac, E.; Ozturk, C.; Varol, A.; Ekmekci, A. Polymorphisms in the Vitamin D Receptor Gene and Risk of Lung Cancer. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2009, 15, BR242–BR248. [Google Scholar]
- Rai, V.; Abdo, J.; Agrawal, S.; Agrawal, D.K. Vitamin D Receptor Polymorphism and Cancer: An Update. Anticancer Res. 2017, 37, 3991. [Google Scholar] [PubMed]
- Zhong, H.; Zhou, R.; Feng, Y.; Zheng, G.X.; Liang, Y.; Zhang, J.Y.; Qin, X.Q.; Chen, W.; Wu, J.Q.; Zhong, Y.H. Association of Vitamin D Receptor Gene Polymorphism with the Risk of Lung Cancer: A Meta-Analysis. J. Recept. Signal Transduct. 2014, 34, 500–505. [Google Scholar] [CrossRef]
- Ingles, S.A.; Haile, R.W.; Henderson, B.E.; Kolonel, L.N.; Nakaichi, G.; Shi, C.Y.; Yu, M.C.; Ross, R.K.; Coetzee, G.A. Strength of Linkage Disequilibrium between Two Vitamin D Receptor Markers in Five Ethnic Groups: Implications for Association Studies. Cancer Epidemiol. Biomark. Prev. 1997, 6, 93–98. [Google Scholar]
- Raimondi, S.; Pasquali, E.; Gnagnarella, P.; Serrano, D.; Disalvatore, D.; Johansson, H.A.; Gandini, S. BsmI Polymorphism of Vitamin D Receptor Gene and Cancer Risk: A Comprehensive Meta-Analysis. Mutat. Res. Fundam. Mol. Mech. Mutagen. 2014, 769, 17–34. [Google Scholar] [CrossRef] [PubMed]
- Underwood, J.M.; Townsend, J.S.; Tai, E.; Davis, S.P.; Stewart, S.L.; White, A.; Momin, B.; Fairley, T.L. Racial and Regional Disparities in Lung Cancer Incidence. Cancer 2012, 118, 1910–1918. [Google Scholar] [CrossRef] [PubMed]
- Kaabachi, W.; Kaabachi, S.; Rafrafi, A.; ben Amor, A.; Tizaoui, K.; Haj Sassi, F.; Hamzaoui, K. Association of Vitamin D Receptor FokI and ApaI Polymorphisms with Lung Cancer Risk in Tunisian Population. Mol. Biol. Rep. 2014, 41, 6545–6553. [Google Scholar] [CrossRef] [PubMed]
- Pineda-Lancheros, L.E.; Gálvez-Navas, J.M.; Rojo-Tolosa, S.; Membrive-Jiménez, C.; Valverde-Merino, M.I.; Martínez-Martínez, F.; Sánchez-Martín, A.; Ramírez-Tortosa, M.; Pérez-Ramírez, C.; Jiménez-Morales, A. Polymorphisms in VDR, CYP27B1, CYP2R1, GC and CYP24A1 Genes as Biomarkers of Survival in Non-Small Cell Lung Cancer: A Systematic Review. Nutrients 2023, 15, 1525. [Google Scholar] [CrossRef] [PubMed]
- Rajiyalakshmi, G.; Suresh, A.; Muninathan, N.; Baskaran, K.; Gopikrishnan, V. Association between Polymorphisms of Vitamin D Receptor and Lung Cancer Susceptibility: A Systematic Review and Meta-Analysis. Korean J. Physiol. Pharmacol. 2023, 27, 78–88. [Google Scholar] [CrossRef]
- Turna, A.; Pekçolaklar, A.; Metin, M.; Yaylim, I.; Gurses, A. The Effect of Season of Operation on the Survival of Patients with Resected Non-Small Cell Lung Cancer. Interact. Cardiovasc. Thorac. Surg. 2012, 14, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Liu, X.; Liu, N.; Yang, T.; Shi, P.; He, R.; Chen, M. Association between Polymorphisms of Vitamin D Receptor and Lung Cancer Susceptibility: Evidence from an Updated Meta-Analysis. J. Cancer 2019, 10, 3639. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Tian, M.; Ma, M.; Pei, J.; Song, Y.; Han, B. Five Vitamin D Receptor Polymorphisms (FokI, BsmI, Apa1, Taq1, and Cdx2) and Lung Cancer Risk. J. Clin. Oncol. 2012, 30, e12013. [Google Scholar] [CrossRef]
- Maj, E.; Trynda, J.; Maj, B.; Gębura, K.; Bogunia-Kubik, K.; Chodyński, M.; Kutner, A.; Wietrzyk, J. Differential Response of Lung Cancer Cell Lines to Vitamin D Derivatives Depending on EGFR, KRAS, P53 Mutation Status and VDR Polymorphism. J. Steroid Biochem. Mol. Biol. 2019, 193, 105431. [Google Scholar] [CrossRef]
- Anderson, M.G.; Nakane, M.; Ruan, X.; Kroeger, P.E.; Wu-Wong, J.R. Expression of VDR and CYP24A1 MRNA in Human Tumors. Cancer Chemother. Pharmacol. 2006, 57, 234–240. [Google Scholar] [CrossRef]
- Kaiser, U.; Schilli, M.; Wegmann, B.; Barth, P.; Wedel, S.; Hofmann, J.; Havemann, K. Expression of Vitamin D Receptor in Lung Cancer. J. Cancer Res. Clin. Oncol. 1996, 122, 356–359. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Protein | Expression in Tumoral Cells | Lung Cancer Association | References |
|---|---|---|---|
| CALB1 | Overexpression | Non-small cell lung cancer | [63] |
| CALB2 | Overexpression | Not associated with cancer but with malignant pleural mesothelioma | [57] |
| S100-G | Overexpression | Non-small cell lung cancer | [58] |
| Gene Polymorphism | Genotype/Allele/rs Variant | Ethnicity | Lung Cancer Risk | References |
|---|---|---|---|---|
| TaqI | t allele and TT genotype | Overall population | High risk (especially in Caucasians) t allele was associated with s reduced risk in one study | [74,79] |
| rs731236 | Asian | High risk | [81] | |
| African | No correlation | [79] | ||
| Bsml | B allele, BB and bb genotype | Asian | High risk | [82] |
| B allele and bb genotype | Overall population | High risk | [82] | |
| bb genotype | Caucasian/overall population | High risk | [83] | |
| rs1544410 | Overall population | No correlation, even if a dominant allele may decrease the risk of lung cancer | [81,82] | |
| Asian | High risk | [82,84] | ||
| ApaI | Aa and aa genotypes | Overall population | High risk | [81] |
| rs7975232 | African | High risk | [85] | |
| FokI | rs2228570 | Overall population | High risk | [86] |
| African | High risk | [85] | ||
| f allele | Overall population | Weak correlation with high risk | [87] | |
| F allele | Overall population | High risk | [88] | |
| Cdx-2 | rs11568820 | Caucasian | Protective factor against lung cancer | [89] |
| TT and TT+TC genotypes | Overall population | Low risk | [75] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciocarlie, T.; Motofelea, A.C.; Motofelea, N.; Dutu, A.G.; Crăciun, A.; Costachescu, D.; Roi, C.I.; Silaghi, C.N.; Crintea, A. Exploring the Role of Vitamin D, Vitamin D-Dependent Proteins, and Vitamin D Receptor Gene Variation in Lung Cancer Risk. Int. J. Mol. Sci. 2024, 25, 6664. https://doi.org/10.3390/ijms25126664
Ciocarlie T, Motofelea AC, Motofelea N, Dutu AG, Crăciun A, Costachescu D, Roi CI, Silaghi CN, Crintea A. Exploring the Role of Vitamin D, Vitamin D-Dependent Proteins, and Vitamin D Receptor Gene Variation in Lung Cancer Risk. International Journal of Molecular Sciences. 2024; 25(12):6664. https://doi.org/10.3390/ijms25126664
Chicago/Turabian StyleCiocarlie, Tudor, Alexandru Cătălin Motofelea, Nadica Motofelea, Alina Gabriela Dutu, Alexandra Crăciun, Dan Costachescu, Ciprian Ioan Roi, Ciprian Nicolae Silaghi, and Andreea Crintea. 2024. "Exploring the Role of Vitamin D, Vitamin D-Dependent Proteins, and Vitamin D Receptor Gene Variation in Lung Cancer Risk" International Journal of Molecular Sciences 25, no. 12: 6664. https://doi.org/10.3390/ijms25126664