
Paradoxical Psoriasis in Patients Receiving Therapy with Tumor Necrosis Factor Inhibitors: Potential Pathogenic Mechanisms and the Role of Genetic Factors

 , , ,
, , ,  , ,
, , 
Abstract
1. Introduction
2. Paradoxical Psoriasis Induced by TNFi
2.1. Definition and General Considerations

{kind=link}
| Mechanism | Palmoplantar Pustulosis (PPP) | Classic Psoriasis | Paradoxical Psoriasis (PP) |
|---|---|---|---|
| Genetic Factors | Variants in IL36RN, ASP1S3 (rs2241880G and rs2241879A), and CARD14 genes [28,29]. | Variants in HLA-Cw6, TNF, IL23R, IL12B, ERAP1, CARD14, TNFAIP3, and NFKBIA [9,32]. | Certain SNPs in genes like IL23R, FBXL19, CTLA4, SLC12A8, TAP1, and others predispose individuals to paradoxical psoriasis [22]. |
| Immunological pathways | 1. Dysregulation of multiple immunological pathways:
| A dysregulation of certain immunological pathways, particularly the TNF/IL-23/IL-17 axis [9] | 1. Cytokine dysregulation: TNFi blocks TNFα, which inhibits the maturation of cDCs and pDC, leading to an increased production of IFNα. The overexpression of IFNα leads to the failure of activation of autoimmune T cells and memory T cells [9,13,33,34]. 2. JAK-STAT pathway: TNFi blocks TNFα, leading to an overexpression of IFNα, which activates JAK1 and TYK2 and leads to the phosphorylation and activation of STAT1 and STAT2. Also, the elevated levels of IL-23 activate JAK2/TYK2, which activates STAT3, leading to Th17 cell differentiation and subsequent inflammation. This activation may have a potential role in the pathogenesis of PP [35,36]. 3. IL-23/Th17 axis involvement [33,37]. 4. TNF inhibitors may cause aberrant lymphocyte movement and increase CXCR3 ligands, such as CXCL9, CXCL10, and CXCL11, supporting a Th1-skewed inflammatory response and contributing to psoriasis lesions [38]. 5. Role of T cells and dendritic cells in the development of in paradoxical adverse events [39]. 6. Microbiota involvement and dysbiosis [40]. |
| Cytokine involved | Increase in TNF-α, IL-22, IL17, and IFN-γ and increased expression of IL 8 [29]. | Increased levels of TNF-α, IL-17, IL-23, and IL-22 [9]. | Increased IFN-α, IL-17, and IL-22 [9]. |
| Environmental Triggers | Smoking, stress, infections female sex, and autoimmune thyroid disease [29]. | Trauma (Koebner phenomenon), infections, stress, and medications [41]. | Infections, stress, smoking, female sex, and reaction to TNF inhibitors [42,43,44]. |
| Immune Cell Involvement: | IL-17 plays an important role in the inflammation in PPP. Neutrophils are attracted to the skin by chemokines like IL-8 and play a significant role in the formation of pustules [45]. | Hyperproliferation of keratinocytes; involvement of Th1, Th17, and Th22 cells, dendritic cells, and neutrophils [46]. |
|
| Clinic presentation | Sterile pustules on palms and soles [28]. | Erythematous plaques characterized by silvery-white scales commonly on elbows, knees, scalp, and lower back [9]. | Presence of different psoriatic patterns including plaque-type, guttate, and pustular forms [26]. |
2.2. Mechanisms Involved in PP
3. Genetic Factors and Paradoxical Psoriasis
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gawdzik, A.; Ponikowska, M.; Jankowska-Konsur, A.; Woźniak, Z.; Maj, J.; Szepietowski, J.C. Paradoxical Skin Reaction to Certolizumab, an Overlap of Pyoderma Gangrenosum and Psoriasis in a Young Woman Treated for Ankylosing Spondylitis: Case Report with Literature Review. Dermatol. Ther. 2020, 10, 869–879. [Google Scholar] [CrossRef] [PubMed]
- García-Lagunar, M.H.; Gutiérrez-Cívicos, M.R.; García-Simón, M.S.; Conesa-Zamora, P.; Jiménez-Santos, E.; Cano-Vivar, P.; García-Márquez, A.; Muñoz-García, I.; Viney, A. Reasons for discontinuation and adverse effects of TNFA inhibitors in a cohort of patients with rheumatoid arthritis and ankylosing spondylitis. Ann. Pharmacother. 2016, 51, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Bucalo, A.; Rega, F.; Zangrilli, A.; Silvestri, V.; Valentini, V.; Scafetta, G.; Marraffa, F.; Grassi, S.; Rogante, E.; Piccolo, A.; et al. Paradoxical psoriasis induced by Anti-TNFA treatment: Evaluation of Disease-Specific Clinical and Genetic markers. Int. J. Mol. Sci. 2020, 21, 7873. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, R.H.A.; Essam, M.; Anwar, I.; Shehab, H.; El-Komy, M.H.M. Psoriasis paradox—Infliximab-induced psoriasis in a patient with Crohn’s disease: A case report and mini-review. J. Int. Med. Res. 2023, 51, 3000605231200270. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, J.J.; Gadina, M.; Siegel, R.M. Cytokines and Cytokine Receptors; Elsevier eBooks: Amsterdam, The Netherlands, 2019; pp. 127–155.e1. [Google Scholar] [CrossRef]
- Liu, C.; Chu, D.; Kalantar-Zadeh, K.; George, J.; Young, H.A.; Liu, G. Cytokines: From clinical significance to quantification. Adv. Sci. 2021, 8, e202004433. [Google Scholar] [CrossRef] [PubMed]
- Johnston, G.R.; Webster, N.R. Cytokines and the immunomodulatory function of the vagus nerve. Br. J. Anaesth. 2009, 102, 453–462. [Google Scholar] [CrossRef]
- Kyttaris, V.C. Targeting cytokines to treat autoimmunity. Clin. Immunol. 2019, 206, 108251. [Google Scholar] [CrossRef]
- Mylonas, A.; Conrad, C. Psoriasis: Classical vs. Paradoxical. The Yin-Yang of TNF and Type I Interferon. Front. Immunol. 2018, 9, 2746. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, F. Pathogenesis of Paradoxical Reactions Associated with Targeted Biologic Agents for Inflammatory Skin Diseases. Biomedicines 2022, 10, 1485. [Google Scholar] [CrossRef] [PubMed]
- Olteanu, R.; Zota, A. Paradoxical reactions induced by tumor necrosis factor-alpha antagonists: A literature review based on 46 cases. Indian J. Dermatol. Venereol. Leprol. 2016, 82, 7. [Google Scholar] [CrossRef]
- Mohammed, J.; Mahmmod, Z.; Mathkhor, A.J. Adalimumab-Induced erythema multiforme in a patient with rheumatoid arthritis: A case report. Curēus 2022, 14, e21126. [Google Scholar] [CrossRef]
- Toussirot, É.; Aubin, F. Paradoxical reactions under TNF-α blocking agents and other biological agents given for chronic immune-mediated diseases: An analytical and comprehensive overview. RMD Open 2016, 2, e000239. [Google Scholar] [CrossRef]
- Puig, L. Paradoxical reactions: Anti-Tumor Necrosis Factor Alpha agents, ustekinumab, secukinumab, ixekizumab, and others. In Current Problems in Dermatology; Karger: Basel, Switzerland, 2017; pp. 49–63. [Google Scholar] [CrossRef]
- Terreaux, W.; Masson, C.; Eschard, J.-P.; Bardin, T.; Constantin, A.; Dantec, L.L.; Marcelli, C.; Perdriger, A.; Di Fazano, C.S.; Wendling, D.; et al. Incidence of paradoxical reactions in patients treated with tocilizumab for rheumatoid arthritis: Data from the French registry REGATE. Jt. Bone Spine 2018, 85, 53–57. [Google Scholar] [CrossRef]
- Romagnuolo, M.; Moltrasio, C.; Iannone, C.; Gattinara, M.; Cambiaghi, S.; Marzano, A.V. Pyoderma gangrenosum following anti-TNF therapy in chronic recurrent multifocal osteomyelitis: Drug reaction or cutaneous manifestation of the disease? A critical review on the topic with an emblematic case report. Front. Med. 2023, 10, 1197273. [Google Scholar] [CrossRef]
- Vorčáková, K.; Juraj, P.; Péčová, T.; Klára, M. Immune-Mediated Skin Reactions Induced by Recombinant Antibodies and Other TNF-Alpha Inhibitors; IntechOpen: London, UK, 2018. [Google Scholar] [CrossRef]
- İbiş, N.; Hocaoglu, S.; Çebiçci, M.A.; Sütbeyaz, S.T.; Çalış, H.T. Palmoplantar pustular psoriasis induced by adalimumab: A case report and literature review. Immunotherapy 2015, 7, 717–720. [Google Scholar] [CrossRef]
- Mir-Bonafé, J.F.; López-Ferrer, A.; Laíz, A.; Puig, L. Triple paradoxical reaction due to adalimumab. J. Eur. Acad. Dermatol. Venereol. 2016, 31, e71–e73. [Google Scholar] [CrossRef]
- Pérez-De-Lis, M.; Retamozo, S.; Flores-Chávez, A.; Kostov, B.; Pérez-Álvarez, R.; Brito-Zerón, P.; Ramos-Casals, M. Autoimmune diseases induced by biological agents. A review of 12,731 cases (BIOGEAS Registry). Expert Opin. Drug Saf. 2017, 16, 1255–1271. [Google Scholar] [CrossRef]
- Ya, J.; Hu, J.; Nowacki, A.S.; Khanna, U.; Mazloom, S.; Kabbur, G.; Husni, M.E.; Fernandez, A.P. Family history of psoriasis, psychological stressors, and tobacco use are associated with the development of tumor necrosis factor-α inhibitor-induced psoriasis: A case-control study. J. Am. Acad. Dermatol. 2020, 83, 1599–1605. [Google Scholar] [CrossRef]
- Cabaleiro, T.; Prieto-Pérez, R.; Navarro, R.; Solano, G.; Román, M.; Ochoa, D.; Abad-Santos, F.; Daudén, E. Paradoxical psoriasiform reactions to anti-TNFα drugs are associated with genetic polymorphisms in patients with psoriasis. Pharmacogenomics J. 2015, 16, 336–340. [Google Scholar] [CrossRef]
- Vedak, P.; Kroshinsky, D.; St John, J.; Xavier, R.J.; Yajnik, V.; Ananthakrishnan, A.N. Genetic basis of TNF-α antagonist associated psoriasis in inflammatory bowel diseases: A genotype-phenotype analysis. Aliment. Pharmacol. Ther. 2016, 43, 697–704. [Google Scholar] [CrossRef]
- Garcovich, S.; De Simone, C.; Genovese, G.; Berti, E.; Cugno, M.; Marzano, A.V. Paradoxical skin reactions to biologics in patients with rheumatologic disorders. Front. Pharmacol. 2019, 10, 282. [Google Scholar] [CrossRef]
- Navarro, R.; Daudén, E. Reacciones psoriasiformes paradójicas durante el tratamiento con terapia anti-factor de necrosis tumoral. Manejo clínico. Actas Dermo-Sifiliogr. 2014, 105, 752–761. [Google Scholar] [CrossRef]
- Li, S.J.; Perez-Chada, L.M.; Merola, J.F. TNF Inhibitor-Induced Psoriasis: Proposed Algorithm for Treatment and Management. J. Psoriasis Psoriatic. Arthritis 2019, 4, 70–80. [Google Scholar] [CrossRef]
- Navarini, A.A.; Burden, A.D.; Capon, F.; Mrowietz, U.; Puig, L.; Köks, S.; Kingo, K.; Smith, C.; Barker, J.N.; ERASPEN Network. European consensus statement on phenotypes of pustular psoriasis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1792–1799. [Google Scholar] [CrossRef] [PubMed]
- Freitas, E.; Rodrigues, M.A.; Torres, T. Diagnosis, Screening and Treatment of Patients with Palmoplantar Pustulosis (PPP): A Review of Current Practices and Recommendations. Clin. Cosmet. Investig. Dermatol. 2020, 13, 561–578. [Google Scholar] [CrossRef] [PubMed]
- Misiak-Galazka, M.; Zozula, J.; Rudnicka, L. Palmoplantar Pustulosis: Recent Advances in Etiopathogenesis and Emerging Treatments. Am. J. Clin. Dermatol. 2020, 21, 355–370. [Google Scholar] [CrossRef]
- Baeten, D.; Kruithof, E.; Van Den Bosch, F.; Van Den Bossche, N.; Herssens, A.; Mielants, H.; De Keyser, F.; Veys, E. Systematic safety follow up in a cohort of 107 patients with spondyloarthropathy treated with infliximab: A new perspective on the role of host defence in the pathogenesis of the disease? Ann. Rheum. Dis. 2003, 62, 829–834. [Google Scholar] [CrossRef]
- Sektaoui, S.; Mehsas, Z.; Benzekri, L. Psoriasis induced by anti-TNF-alpha agents in a patient with Crohn’s disease: A case report and review of the literature. Nasza Dermatol. 2023, 14. [Google Scholar] [CrossRef]
- Dand, N.; Mahil, S.K.; Capon, F.; Smith, C.H.; Simpson, M.A.; Barker, J.N. Psoriasis and Genetics. Acta Derm. Venereol. 2020, 100, adv00030. [Google Scholar] [CrossRef]
- Lu, J.; Lu, Y. Paradoxical psoriasis: The flip side of idiopathic psoriasis or an autocephalous reversible drug reaction? J. Transl. Autoimmun. 2023, 7, 100211. [Google Scholar] [CrossRef]
- Conrad, C.; Di Domizio, J.; Mylonas, A.; Belkhodja, C.; Demaria, O.; Navarini, A.A.; Lapointe, A.-K.; French, L.E.; Vernez, M.; Gilliet, M. TNF blockade induces a dysregulated type I interferon response without autoimmunity in paradoxical psoriasis. Nat. Commun. 2018, 9, 25. [Google Scholar] [CrossRef] [PubMed]
- Woodbury, M.J.; Grant, C.; Perez-Chada, L.; LaChance, A.H.; Merola, J.F. A Case Series of TNF Inhibitor-Induced Psoriasis Successfully Treated With Upadacitinib. J. Drugs Dermatol. 2024, 23, e60–e63. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Jiang, G. Application of JAK inhibitors in paradoxical reaction through immune-related dermatoses. Front. Immunol. 2024, 20, 1341632. [Google Scholar] [CrossRef] [PubMed]
- Wasilewska, A.; Chmielowska-Trybek, M.; Sładek, M. Successful treatment of infliximab-induced psoriasiform skin lesions despite biologic therapy intensification in a paediatric patient with Crohn’s disease and primary sclerosing cholangitis. Pediatr. Pol. 2021, 96, 143–147. [Google Scholar] [CrossRef]
- Tillack, C.; Ehmann, L.M.; Friedrich, M.; Laubender, R.P.; Papay, P.; Vogelsang, H.; Stallhofer, J.; Beigel, F.; Bedynek, A.; Wetzke, M.; et al. Anti-TNF antibody-induced psoriasiform skin lesions in patients with inflammatory bowel disease are characterised by interferon-γ-expressing Th1 cells and IL-17A/IL-22-expressing Th17 cells and respond to anti-IL-12/IL-23 antibody treatment. Gut 2013, 63, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.V.; Connors, T.J.; Farber, D.L. Human T Cell Development, Localization, and Function throughout Life. Immun. Camb. Mass. 2018, 48, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Zákostelská, Z.J.; Reiss, Z.; Tlaskalová-Hogenová, H.; Rob, F. Paradoxical reactions to Anti-TNFA and Anti-IL-17 treatment in psoriasis patients: Are skin and/or gut microbiota involved? Dermatol. Ther. 2023, 13, 911–933. [Google Scholar] [CrossRef] [PubMed]
- Roszkiewicz, M.; Dopytalska, K.; Szymańska, E.; Jakimiuk, A.; Walecka, I. Environmental risk factors and epigenetic alternations in psoriasis. Ann. Agric. Environ. Med. 2020, 27, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Xiao, S.; Huang, H.; Zhang, Z. Incidence of and risk factors for paradoxical psoriasis or psoriasiform lesions in inflammatory bowel disease patients receiving Anti-TNF therapy: Systematic Review with Meta-Analysis. Front. Immunol. 2022, 13, 847160. [Google Scholar] [CrossRef]
- Munera-Campos, M.; Ballescà, F.; Carrascosa, J.M. Reacciones paradójicas de los tratamientos biológicos utilizados en psoriasis: Revisión de la literatura. Actas Dermo-Sifiliográficas/Actas Dermo-Sifiliogr. 2018, 109, 791–800. [Google Scholar] [CrossRef]
- Baganz, L.; Listing, J.; Kekow, J.; Eisterhues, C.; Wassenberg, S.; Zink, A.; Strangfeld, A. Different risk profiles of biologic agents for new-onset psoriasis in patients with rheumatoid arthritis. Semin. Arthritis Rheum. 2020, 50, 36–41. [Google Scholar] [CrossRef]
- Brunasso, A.M.G.; Massone, C. Recent advances in palmoplantar pustulosis. Fac. Rev. 2021, 10, 62. [Google Scholar] [CrossRef]
- Hu, P.; Wang, M.; Gao, H.; Zheng, A.; Li, J.; Mu, D.; Tong, J. The Role of Helper T Cells in Psoriasis. Front. Immunol. 2021, 12, 788940. [Google Scholar] [CrossRef]
- Yang, M.; Liu, W.; Deng, Q.; Liang, Z.; Wang, Q. The incidence of psoriasis among smokers and/or former smokers inflammatory bowel diseases patients treated with tumor necrosis factor antagonist. Medicine 2021, 100, e27510. [Google Scholar] [CrossRef]
- Grine, L.; Dejager, L.; Libert, C.; Vandenbroucke, R.E. An inflammatory triangle in psoriasis: TNF, type I IFNs and IL-17. Cytokine Growth Factor Rev. 2015, 26, 25–33. [Google Scholar] [CrossRef]
- Lian, N.; Zhang, L.; Chen, M. Tumor necrosis factors-α inhibition-induced paradoxical psoriasis: A case series and literature review. Dermatol. Ther. 2020, 33, e14225. [Google Scholar] [CrossRef]
- Joyau, C.; Veyrac, G.; Dixneuf, V.; Jolliet, P. Anti-tumour necrosis factor alpha therapy and increased risk of de novo psoriasis: Is it really a paradoxical side effect? Clin. Exp. Rheumatol. 2012, 30, 700–706. [Google Scholar]
- Lopetuso, L.R.; Cuomo, C.; Mignini, I.; Gasbarrini, A.; Papa, A. Focus on Anti-Tumour Necrosis Factor (TNF)-A-Related autoimmune diseases. Int. J. Mol. Sci. 2023, 24, 8187. [Google Scholar] [CrossRef]
- Ruggiero, A.; Fabbrocini, G.; Picone, V.; Marano, L.; Fabbrocini, G.; Marasca, C. Paradoxical Hidradenitis Suppurativa during Biologic Therapy, an Emerging Challenge: A Systematic Review. Biomedicines 2022, 10, 455. [Google Scholar] [CrossRef]
- Hausmann, J. Targeting cytokines to treat autoinflammatory diseases. Clin. Immunol. 2019, 206, 23–32. [Google Scholar] [CrossRef]
- Her, M.; Kavanaugh, A. Alterations in immune function with biologic therapies for autoimmune disease. J. Allergy Clin. Immunol. 2016, 137, 19–27. [Google Scholar] [CrossRef]
- Fania, L.; Morelli, M.; Scarponi, C.; Mercurio, L.; Scopelliti, F.; Cattani, C.; Scaglione, G.L.; Tonanzi, T.; Pilla, M.; Pagnanelli, G.; et al. Paradoxical psoriasis induced by TNF-α blockade shows immunological features typical of the early phase of psoriasis development. J. Pathol. Clin. Res. 2019, 6, 55–68. [Google Scholar] [CrossRef]
- Morelli, M.; Scarponi, C.; Madonna, S.; Albanesi, C. Experimental methods for the immunological characterization of paradoxical psoriasis reactions induced by TNF-A biologics. In Methods in Molecular Biology; Springer: Berlin/Heidelberg, Germany, 2020; pp. 155–165. [Google Scholar] [CrossRef]
- De Vasconcellos, J.B.; Pereira, D.Q.; De Sousa Vargas, T.J.; Levy, R.A.; Da Rocha Castelar Pinheiro, G.; Cursi, Í.B. Paradoxical psoriasis after the use of anti-TNF in a patient with rheumatoid arthritis. An. Bras. Dermatol. 2016, 91 (Suppl. 1), 137–139. [Google Scholar] [CrossRef]
- Chokshi, A.; Beckler, M.D.; Laloo, A.; Kesselman, M.M. Paradoxical Tumor Necrosis Factor-Alpha (TNF-A) Inhibitor-Induced Psoriasis: A Systematic Review of Pathogenesis, clinical presentation, and treatment. Curēus, 2023. [Google Scholar] [CrossRef]
- Moy, A.P.; Murali, M.R.; Kroshinsky, D.; Horn, T.; Nazarian, R.M. T-helper immune phenotype may underlie ‘paradoxical’ tumour necrosis factor-α inhibitor therapy-related psoriasiform dermatitis. Clin. Exp. Dermatol. 2017, 43, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Wendling, D.; Prati, C. Paradoxical effects of anti-TNF-α agents in inflammatory diseases. Expert Rev. Clin. Immunol. 2013, 10, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Sénéschal, J.; Milpied, B.; Vergier, B.; Lepreux, S.; Schaeverbeke, T.; TaiEb, A. Cytokine imbalance with increased production of interferon-α in psoriasiform eruptions associated with antitumour necrosis factor-α treatments. Br. J. Dermatol. 2009, 161, 1081–1088. [Google Scholar] [CrossRef]
- Mehta, A.; Gracias, D.T.; Croft, M. TNF activity and T cells. Cytokine 2018, 101, 14–18. [Google Scholar] [CrossRef]
- Davignon, J.; Rauwel, B.; Degboé, Y.; Constantin, A.; Boyer, J.; Kruglov, A.; Cantagrel, A. Modulation of T-cell responses by anti-tumor necrosis factor treatments in rheumatoid arthritis: A review. Arthritis Res. Ther. 2018, 20. [Google Scholar] [CrossRef]
- Wang, A.; Bai, Y. Dendritic cells: The driver of psoriasis. J. Dermatol. 2019, 47, 104–113. [Google Scholar] [CrossRef]
- Kremenevski, I.; Sander, O.; Sticherling, M.; Raithel, M. Paradoxical reactions to biologicals in chronic inflammatory systemic diseases. Dtsch. Ärzteblatt Int. 2022. [Google Scholar] [CrossRef]
- Fry, L.; Baker, B.S.; Powles, A.V.; Fahlén, A.; Engstrand, L. Is chronic plaque psoriasis triggered by microbiota in the skin? Br. J. Dermatol. Suppl. 2013, 169, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Zákostelská, Z.J.; Málková, J.; Klimešová, K.; Rossmann, P.; Hornová, M.; Novosádová, I.; Stehlíková, Z.; Kostovčík, M.; Hudcovic, T.; Štěpánková, R.; et al. Intestinal microbiota promotes Psoriasis-Like skin inflammation by enhancing TH17 response. PLoS ONE 2016, 11, e0159539. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, H.; Ebrahimi, E.; Daneshpazhooh, M.; Balighi, K.; Mirzazadeh, A.; Behjati, S.E.; Tavakolpour, S. Single-nucleotide polymorphisms associated with pemphigus vulgaris: Potent markers for better treatment and personalized medicine. Int. J. Immunogenet. 2019, 47, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Berna-Rico, E.; Perez-Bootello, J.; De Aragón, C.A.; González-Cantero, Á. Genetic Influence on Treatment Response in Psoriasis: New Insights into Personalized Medicine. Int. J. Mol. Sci. 2023, 24, 9850. [Google Scholar] [CrossRef] [PubMed]
- Sherlock, M.; Walters, T.D.; Tabbers, M.M.; Frost, K.; Zachos, M.; Muise, A.M.; Pope, E.; Griffiths, A.M. Infliximab-Induced psoriasis and psoriasiform skin lesions in pediatric Crohn disease and a potential association with IL-23 receptor polymorphisms. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 512–518. [Google Scholar] [CrossRef]
- Butler, J.M. Single Nucleotide Polymorphisms and Applications; Elsevier eBooks: Amsterdam, The Netherlands, 2012; pp. 347–369. [Google Scholar] [CrossRef]
- Børsting, C.; Pereira, V.; Andersen, J.D.; Morling, N. Single nucleotide polymorphism. Forensic Sci. 2014. [Google Scholar] [CrossRef]
| Mechanism | Description | References |
|---|---|---|
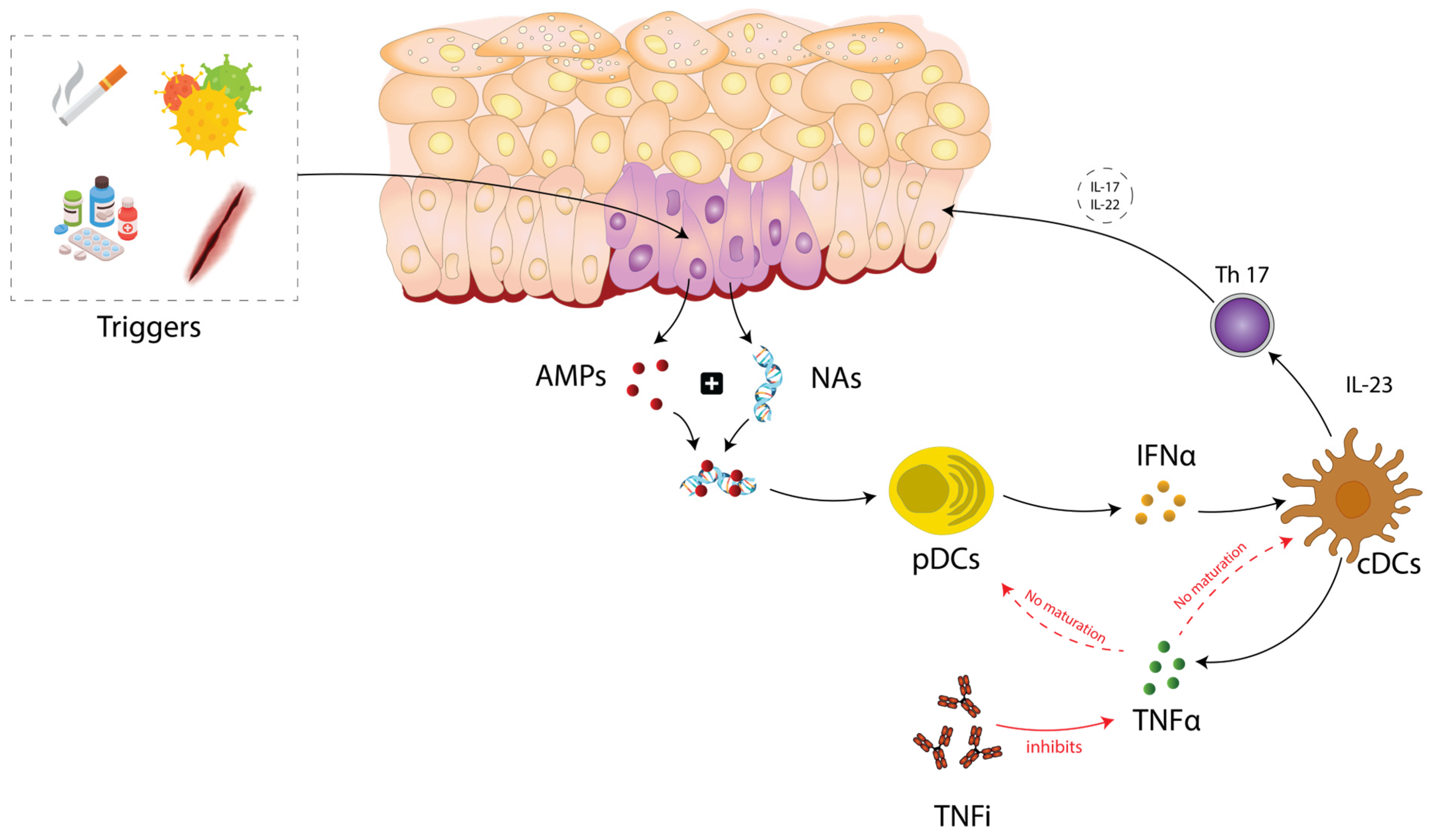
| Cytokine dysregulation | Dysregulation in cytokine balance is one of the most common and most accepted theories. In PP, TNFi blocks TNFα, which inhibits the maturation of conventional dendritic cells (cDCs) and pDC, leading to an increased production of IFNα. As a result, the overexpression of IFNα leads to the failure of activation of autoimmune T cells and memory T cells. | Mylonas A et al., 2018 [9] Toussirot É et al., 2016 [13] Lu J et al., 2023 [33] Conrad C et al., 2018 [34] |
| JAK-STAT pathway | TNFi blocks TNFα, leading to an overexpression of IFNα, which binds to its specific receptors on cells, activates JAK1 and TYK2, and leads to the phosphorylation and activation of STAT1 and STAT2. These induce the expression of proinflammatory genes, resulting in amplified inflammation and potentially explaining the development of psoriasis. Also, the elevated levels of IL-23 activate JAK2/TYK2, which activates STAT3, leading to Th17 cell differentiation and subsequent inflammation. This activation may have a potential role in the pathogenesis of PP. | Woodbury MJ et al., 2024 [35] Zhang Y et al., 2024 [36] |
| IL-23/Th17 axis involvement | IL-23 promotes the activation of Th17 cells, which produce IL-17 and IL-22. Blocking the IL-23/Th17 axis with anti-IL-12/IL-23 antibodies like ustekinumab can resolve skin lesions in IBD patients with paradoxical psoriasis. | Lu J et al., 2023 [33] Wasilewska A et al., 2021 [37] |
| CXCR3 ligands and T cell migration | TNF inhibitors may cause aberrant lymphocyte movement and increase CXCR3 ligands, such as CXCL9, CXCL10, and CXCL11, supporting a Th1-skewed inflammatory response and contributing to psoriasis lesions. | Tillack C et al., 2013 [38] |
| Role of T cells and dendritic cells | T cells produce cytokines such as TNFα and IL-17, sustaining inflammation, while dendritic cells produce IFNα. Both play crucial roles in paradoxical adverse events. | Kumar BV et al., 2018 [39] |
| Genetic factors | Certain SNPs in genes like IL23R, FBXL19, CTLA4, SLC12A8, TAP1, and others predispose individuals to paradoxical psoriasis. | Cabaleiro T et al., 2015 [22] |
| Microbiota involvement and dysbiosis | Changes in the gut or skin microbiota might influence systemic inflammation, contribute to the pathogenesis and progression of IBD or psoriasis, and could trigger or exacerbate psoriasis, including paradoxical forms. Certain modifications in the composition of the microbiota can potentially result in an immune system response alteration, ultimately leading to the development of an inflammatory response. | Zákostelská Z J et al., 2023 [40] |
| Article | Patients | Number of Patients | Treatment | Gene | SNPs | Association with PP |
|---|---|---|---|---|---|---|
| Sherlock M.E et al., 2013 [69] | Pediatric patients with IBD and psoriasis | Total of 234 IBD patients (147 with CD, 87 with UC). Total of 35 patients used Infliximab treatment. Total of 10 developed PP under Infliximab. | IFX | IL23R | rs2201841 rs10489628 rs10789229 rs11209026 rs1343151 | Not associated Associated Associated Not associated Associated |
| Tillack C et al., 2014 [38] * | IBD patients | Total of 434 patients with IBD. Total of 21 develop PP (16 under IFX, 5 under ADA). | IFX or ADA | IL23R IL12B IL23A | rs1004819 rs7517847 rs10489629 rs2201841 rs11465804 rs11209026 (p.Arg381Gln) rs1343151 rs10889677 rs11209032 rs1495965 rs12131065 rs7530511 (p.Leu310Pro) rs3212227 rs6887695 rs2082412 rs10045431 rs2066808 | Not associated Not associated No association No association No association Disease-modifying effects No association No association No association No association No association Disease-modifying effects No association No association No association No association No association |
| Cabaleiro T et al., 2015 [22] | Psoriasis patients | Total of 161 patients with moderate to severe plaque psoriasis. Total of 25 develop PP (18 under ETA, 5 under ADA, 2 under IFX). | TNFi (ETA, ADA, IFX) | IL23R | rs11209026 | Associated |
| FBXL19 | rs10782001 | Associated | ||||
| CTLA4 | rs3087243 | Associated | ||||
| SLC12A8 | rs651630 | Associated | ||||
| TAP1 | rs1800453 | Associated | ||||
| Fania L et al., 2019 [55] ** | HS | patients with HS | ADA | ERAP1 | rs30187 | Possibly associated |
| rs30186 | Possibly associated | |||||
| rs26653 | Possibly associated | |||||
| rs11743410 | Possibly associated | |||||
| HLA-C | rs114395371 | Possibly associated | ||||
| rs2524095 | Possibly associated | |||||
| rs2853922 | Possibly associated | |||||
| rs386698994 | Possibly associated | |||||
| rs28383849 | Possibly associated | |||||
| rs10484554 | Possibly associated | |||||
| rs147538049 | Possibly associated | |||||
| rs9264944 | Possibly associated | |||||
| rs9264946 | Possibly associated | |||||
| HLA-Cw6 2v | rs79709508 | Possibly associated | ||||
| HLA-Cw6 | rs17192540 | No association | ||||
| IL23R | rs72676067 | Possibly associated | ||||
| rs1004819 | Possibly associated | |||||
| rs41313262 | Possibly associated | |||||
| rs11209026 | No association | |||||
| NFKBIZ | rs3217713 | Associated | ||||
| rs7637230 | Possibly associated | |||||
| IL12B | rs2546890 | Possibly associated | ||||
| TNF α | rs1800610 | Possibly associated | ||||
| IL17F | rs2397084 | Possibly associated | ||||
| TRAF3IP2 | rs71562288 | Possibly associated | ||||
| rs33980500 | Possibly associated | |||||
| TNFAIP3 | rs610604 | Possibly associated | ||||
| TYK2 | rs12720356 | Possibly associated | ||||
| rs280519 | Possibly associated | |||||
| IL17RA | rs4819554 | Possibly associated | ||||
| CDSN | rs3132554 | Possibly associated | ||||
| rs1042127 | Possibly associated | |||||
| rs1042126 | Possibly associated | |||||
| rs1062470 | Possibly associated | |||||
| rs707913 | Possibly associated | |||||
| rs3130983 | Possibly associated | |||||
| CCHCR1 | rs1576 | Possibly associated | ||||
| rs130079 | Possibly associated | |||||
| rs746647 | Possibly associated | |||||
| rs130075 | Possibly associated | |||||
| Bucalo A et al., 2020 [3] | IBD and psoriasis patients | Total of 53 IBD patients. Total of 16 develop PP (11 under ADA, 5 under IFX). Total of 108 psoriatic patients. Total of 23 develop PP under ADA. | TNFi (ADA, IFX, ETA) | HLA-Cw06 | rs10484554 | Not associated |
| IL23R | rs11209026 | Associated | ||||
| rs10789229 | Not associated | |||||
| TNFα | rs1799964 | Associated | ||||
| rs1800629 | No association | |||||
| IFIH1 | rs1990760 | No association |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costin, D.; Burlui, A.M.; Cardoneanu, A.; Macovei, L.A.; Rezus, C.; Bratoiu, I.; Richter, P.; Mihai, I.R.; Gherasim, A.; Danielescu, C.; et al. Paradoxical Psoriasis in Patients Receiving Therapy with Tumor Necrosis Factor Inhibitors: Potential Pathogenic Mechanisms and the Role of Genetic Factors. Int. J. Mol. Sci. 2024, 25, 7018. https://doi.org/10.3390/ijms25137018
Costin D, Burlui AM, Cardoneanu A, Macovei LA, Rezus C, Bratoiu I, Richter P, Mihai IR, Gherasim A, Danielescu C, et al. Paradoxical Psoriasis in Patients Receiving Therapy with Tumor Necrosis Factor Inhibitors: Potential Pathogenic Mechanisms and the Role of Genetic Factors. International Journal of Molecular Sciences. 2024; 25(13):7018. https://doi.org/10.3390/ijms25137018
Chicago/Turabian StyleCostin, Damiana, Alexandra Maria Burlui, Anca Cardoneanu, Luana Andreea Macovei, Ciprian Rezus, Ioana Bratoiu, Patricia Richter, Ioana Ruxandra Mihai, Andreea Gherasim, Ciprian Danielescu, and et al. 2024. "Paradoxical Psoriasis in Patients Receiving Therapy with Tumor Necrosis Factor Inhibitors: Potential Pathogenic Mechanisms and the Role of Genetic Factors" International Journal of Molecular Sciences 25, no. 13: 7018. https://doi.org/10.3390/ijms25137018
APA StyleCostin, D., Burlui, A. M., Cardoneanu, A., Macovei, L. A., Rezus, C., Bratoiu, I., Richter, P., Mihai, I. R., Gherasim, A., Danielescu, C., & Rezus, E. (2024). Paradoxical Psoriasis in Patients Receiving Therapy with Tumor Necrosis Factor Inhibitors: Potential Pathogenic Mechanisms and the Role of Genetic Factors. International Journal of Molecular Sciences, 25(13), 7018. https://doi.org/10.3390/ijms25137018