
Long-Term Remission with Novel Combined Immune-Targeted Treatment for Histiocytic Sarcoma Accompanied by Follicular Lymphoma: Case Report and Literature Review
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
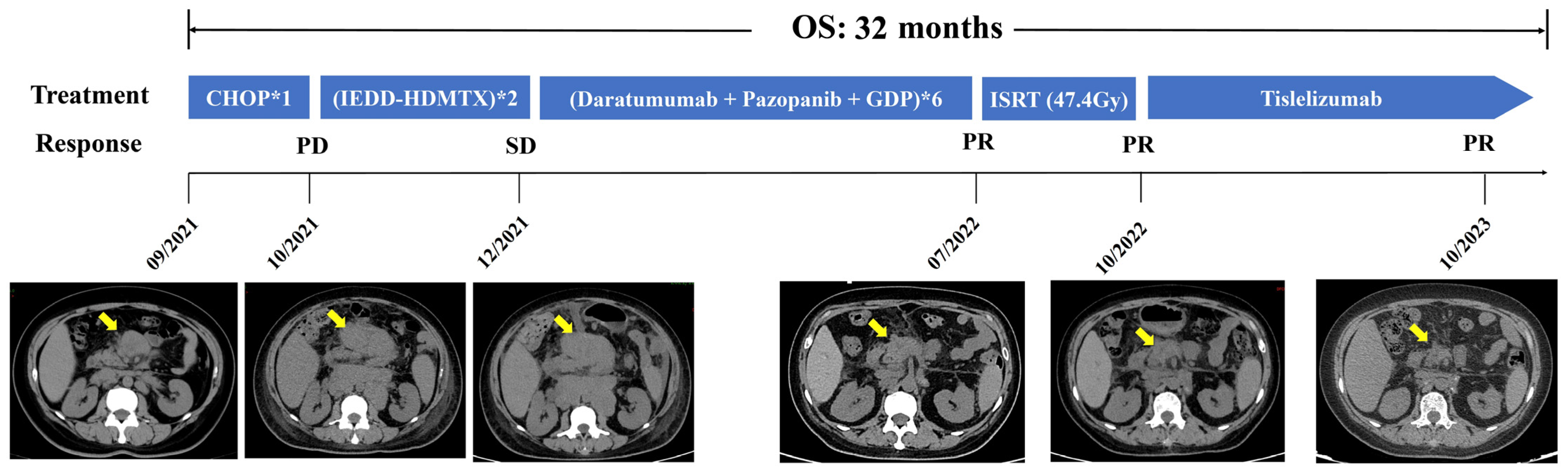
2. Case Presentation
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khoury, J.D.; Solary, E.; Abla, O.; Akkari, Y.; Alaggio, R.; Apperley, J.F.; Bejar, R.; Berti, E.; Busque, L.; Chan, J.K.C.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia 2022, 36, 1703–1719. [Google Scholar] [CrossRef]
- Feldman, A.L.; Arber, D.A.; Pittaluga, S.; Martinez, A.; Burke, J.S.; Raffeld, M.; Camos, M.; Warnke, R.; Jaffe, E.S. Clonally related follicular lymphomas and histiocytic/dendritic cell sarcomas: Evidence for transdifferentiation of the follicular lymphoma clone. Blood 2008, 111, 5433–5439. [Google Scholar] [CrossRef]
- Wang, E.; Hutchinson, C.B.; Huang, Q.; Sebastian, S.; Rehder, C.; Kanaly, A.; Moore, J.; Datto, M. Histiocytic sarcoma arising in indolent small B-cell lymphoma: Report of two cases with molecular/genetic evidence suggestive of a ‘transdifferentiation’ during the clonal evolution. Leuk. Lymphoma 2010, 51, 802–812. [Google Scholar] [CrossRef]
- Hure, M.C.; Elco, C.P.; Ward, D.; Hutchinson, L.; Meng, X.; Dorfman, D.M.; Yu, H. Histiocytic sarcoma arising from clonally related mantle cell lymphoma. J. Clin. Oncol. 2012, 30, e49–e53. [Google Scholar] [CrossRef]
- Kommalapati, A.; Tella, S.H.; Durkin, M.; Go, R.S.; Goyal, G. Histiocytic sarcoma: A population-based analysis of incidence, demographic disparities, and long-term outcomes. Blood 2018, 131, 265–268. [Google Scholar] [CrossRef]
- Gupta, D.; Gupta, A.; Nalwa, A.; Yadav, T.; Chaudhary, R.; Rao, M. Cytopathologic findings in histiocytic sarcoma of thyroid mimicking as anaplastic carcinoma: A report of a rare case with review of literature. Diagn. Cytopathol. 2021, 49, E218–E221. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, K.; Delgado, R.; Kochiyil, J.; Medina, A.M. Primary Histiocytic Sarcoma in Adult Polycystic Kidney Disease: Case Report and Review of Literature. Int. J. Surg. Pathol. 2021, 29, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, R.; Kanazawa, Y.; Matsuno, K.; Kakinuma, D.; Tokura, T.; Marumo, A.; Yui, S.; Ando, F.; Masuda, Y.; Hagiwara, N.; et al. An advanced case of gastric histiocytic sarcoma treated with chemotherapy and gastrectomy: A case report and review of literature. Clin. J. Gastroenterol. 2021, 14, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Montalvo, N.; Lara-Endara, J.; Redrobán, L.; Leiva, M.; Armijos, C.; Russo, L. Primary splenic histiocytic sarcoma associated with hemophagocytic lymphohistiocytosis: A case report and review of literature of next-generation sequencing involving FLT3, NOTCH2, and KMT2A mutations. Cancer Rep. 2022, 5, e1496. [Google Scholar] [CrossRef]
- Péricart, S.; Waysse, C.; Siegfried, A.; Struski, S.; Delabesse, E.; Laurent, C.; Evrard, S. Subsequent development of histiocytic sarcoma and follicular lymphoma: Cytogenetics and next-generation sequencing analyses provide evidence for transdifferentiation of early common lymphoid precursor—A case report and review of literature. Virchows Arch. 2020, 476, 609–614. [Google Scholar] [CrossRef]
- Wang, W.; Zhang, Y.; Dong, Y.; Li, S.; Qin, H. Primary central nervous system histiocytic sarcoma with somatic NF2 mutation: Case report and review of literature. Clin. Neuropathol. 2022, 41, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Pol, S.; Bangs, C.D.; Cherry, A.; Arber, D.A.; Gratzinger, D. Two cases of histiocytic sarcoma with BCL2 translocations and occult or subsequent follicular lymphoma. Hum. Pathol. 2016, 55, 39–43. [Google Scholar] [CrossRef]
- Sabatini, P.J.B.; Tremblay-Lemay, R.; Ahmadi Moghaddam, P.; Delabie, J.M.A.; Sakhdari, A. Marginal zone lymphoma transdifferentiated to histiocytic sarcoma. Br. J. Haematol. 2021, 194, 1090–1094. [Google Scholar] [CrossRef] [PubMed]
- Bassarova, A.; Trøen, G.; Fosså, A.; Ikonomou, I.M.; Beiske, K.; Nesland, J.M.; Delabie, J. Transformation of B cell lymphoma to histiocytic sarcoma: Somatic mutations of PAX-5 gene with loss of expression cannot explain transdifferentiation. J. Hematop. 2009, 2, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Brunner, P.; Rufle, A.; Dirnhofer, S.; Lohri, A.; Willi, N.; Cathomas, G.; Tzankov, A.; Juskevicius, D. Follicular lymphoma transformation into histiocytic sarcoma: Indications for a common neoplastic progenitor. Leukemia 2014, 28, 1937–1940. [Google Scholar] [CrossRef] [PubMed]
- Etancelin, P.; Boussaid, I. Two sides of the same coin: Transdifferentiation from Burkitt lymphoma to histiocytic sarcoma. Blood 2023, 142, 1576. [Google Scholar] [CrossRef] [PubMed]
- Cheon, M.; Yoo, J.; Kim, H.S.; Lee, M. Enhanced Computed Tomography and (18)F-fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in the Uncommon Histiocytic Sarcoma of Small Intestine Arising after Gastric Large B-Cell Lymphoma. Diagnostics 2023, 13, 3189. [Google Scholar] [CrossRef] [PubMed]
- Farris, M.; Hughes, R.T.; Lamar, Z.; Soike, M.H.; Menke, J.R.; Ohgami, R.S.; Winkfield, K. Histiocytic Sarcoma Associated with Follicular Lymphoma: Evidence for Dramatic Response with Rituximab and Bendamustine Alone and a Review of the Literature. Clin. Lymphoma Myeloma Leuk. 2019, 19, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.; Al-Kawaaz, M.; Martin, B.A.; Hegazi, M.M.; Tan, B.; Gratzinger, D. Histiocytic Sarcoma with CCND1 Gene Rearrangement Clonally Related and Transdifferentiated from Mantle Cell Lymphoma. Am. J. Clin. Pathol. 2022, 158, 449–455. [Google Scholar] [CrossRef]
- Shao, H.; Xi, L.; Raffeld, M.; Feldman, A.L.; Ketterling, R.P.; Knudson, R.; Rodriguez-Canales, J.; Hanson, J.; Pittaluga, S.; Jaffe, E.S. Clonally related histiocytic/dendritic cell sarcoma and chronic lymphocytic leukemia/small lymphocytic lymphoma: A study of seven cases. Mod. Pathol. 2011, 24, 1421–1432. [Google Scholar] [CrossRef]
- Cheng, F.; Yu, F.; Wang, X.; Huang, K.; Lu, H.; Wang, Z. A Pedigree Analysis and Clonal Correlations of the Coexistence of B-Cell Lymphoma and Histiocytic/Dendritic Cell Tumor. Int. J. Surg. Pathol. 2021, 29, 906–914. [Google Scholar] [CrossRef]
- D’amore, E.S.; Mainardi, C.; Mussolin, L.; Carraro, E.; Alaggio, R.; Lazzari, E.; Fusetti, S.; Ghirotto, C.; Marzollo, A.; Biddeci, G.; et al. Histiocytic sarcoma arising in a child affected by Burkitt lymphoma, with t(8;14)(q24;q32) positivity in both tumors. Pediatr. Hematol. Oncol. 2021, 38, 1–7. [Google Scholar] [CrossRef]
- Zhang, D.; McGuirk, J.; Ganguly, S.; Persons, D.L. Histiocytic/dendritic cell sarcoma arising from follicular lymphoma involving the bone: A case report and review of literature. Int. J. Hematol. 2009, 89, 529–532. [Google Scholar] [CrossRef]
- Schünemann, C.; Göhring, G.; Behrens, Y.L.; Kreipe, H.-H.; Ganser, A.; Thol, F. Histiocytic sarcoma progressing from follicular lymphoma and mimicking acquired hemophagocytic lymphohistiocytosis. Ann. Hematol. 2020, 99, 2441–2443. [Google Scholar] [CrossRef]
- Shi, C.M.; Lytle, A.M.; Milman, T.; Penne, R.; Bagg, A. Composite Histiocytic Sarcoma and Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma of the Ocular Adnexa. Ophthalmic Plast. Reconstr. Surg. 2024, 10, 1097. [Google Scholar] [CrossRef] [PubMed]
- Egan, C.; Lack, J.; Skarshaug, S.; Pham, T.A.; Abdullaev, Z.; Xi, L.; Pack, S.; Pittaluga, S.; Jaffe, E.S.; Raffeld, M. The mutational landscape of histiocytic sarcoma associated with lymphoid malignancy. Mod. Pathol. 2020, 34, 336–347. [Google Scholar] [CrossRef]
- Hung, Y.P.; Qian, X. Histiocytic Sarcoma. Arch. Pathol. Lab. Med. 2020, 144, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Tocut, M.; Vaknine, H.; Potachenko, P.; Elias, S.; Zandman-Goddard, G. Histiocytic Sarcoma. Isr. Med. Assoc. J. 2020, 22, 645–647. [Google Scholar] [PubMed]
- Campedel, L.; Kharroubi, D.; Vozy, A.; Spano, J.P.; Emile, J.F.; Haroche, J. Malignant Histiocytosis With PD-L1 Expression-Dramatic Response to Nivolumab. Mayo Clin. Proc. 2022, 97, 1401–1403. [Google Scholar] [CrossRef]
- Imataki, O.; Uemura, M.; Fujita, H.; Kadowaki, N. Application of PD-L1 blockade in refractory histiocytic sarcoma: A case report. Mol. Clin. Oncol. 2022, 17, 1–6. [Google Scholar] [CrossRef]
- May, J.M.; Waddle, M.R.; Miller, D.H.; Stross, W.C.; Kaleem, T.A.; May, B.C.; Miller, R.C.; Jiang, L.; Strong, G.W.; Trifiletti, D.M.; et al. Primary histiocytic sarcoma of the central nervous system: A case report with platelet derived growth factor receptor mutation and PD-L1/PD-L2 expression and literature review. Radiat. Oncol. 2018, 13, 167. [Google Scholar] [CrossRef]
- Zhao, Y.; Deng, Y.; Jiang, Y.; Zheng, W.; Tan, Y.; Yang, Z.; Wang, Z.; Xu, F.; Cheng, Z.; Yuan, L.; et al. Case report: Targeting the PD-1 receptor and genetic mutations validated in primary histiocytic sarcoma with hemophagocytic lymphohistiocytosis. Front. Immunol. 2023, 14, 1127599. [Google Scholar] [CrossRef]
- Zhao, J.; Niu, X.; Wang, Z.; Lu, H.; Lin, X.; Lu, Q. Histiocytic sarcoma combined with acute monocytic leukemia: A case report. Diagn. Pathol. 2015, 10, 1–6. [Google Scholar] [CrossRef]
- Michonneau, D.; Kaltenbach, S.; Derrieux, C.; Trinquand, A.; Brouzes, C.; Gibault, L.; North, M.O.; Delarue, R.; Varet, B.; Emile, J.F.; et al. BRAF(V600E) mutation in a histiocytic sarcoma arising from hairy cell leukemia. J. Clin. Oncol. 2014, 32, e117–e121. [Google Scholar] [CrossRef]
- Shanmugam, V.; Griffin, G.K.; Jacobsen, E.D.; Fletcher, C.D.M.; Sholl, L.M.; Hornick, J.L. Identification of diverse activating mutations of the RAS-MAPK pathway in histiocytic sarcoma. Mod. Pathol. 2019, 32, 830–843. [Google Scholar] [CrossRef]
- Egan, C.; Nicolae, A.; Lack, J.; Chung, H.-J.; Skarshaug, S.; Pham, T.A.; Navarro, W.; Abdullaev, Z.; Aguilera, N.S.; Xi, L.; et al. Genomic profiling of primary histiocytic sarcoma reveals two molecular subgroups. Haematologica 2020, 105, 951–960. [Google Scholar] [CrossRef]
- Hung, Y.P.; Lovitch, S.B.; Qian, X. Histiocytic sarcoma: New insights into FNA cytomorphology and molecular characteristics. Cancer Cytopathol. 2017, 125, 604–614. [Google Scholar] [CrossRef]
- Narita, K.; Noro, R.; Seike, M.; Matsumoto, M.; Fujita, K.; Matsumura, J.; Takahashi, M.; Kawamoto, M.; Gemma, A. Successful treatment of histiocytic sarcoma and concurrent HIV infection using a combination of CHOP and antiretroviral therapy. Intern. Med. 2013, 52, 2805–2809. [Google Scholar] [CrossRef]
- Philip, D.S.J.; Sherief, A.; Narayanan, G.; Nair, S.G.; Av, J. Histiocytic Sarcoma: Clinical Features and Outcomes of Patients Treated at a Tertiary Cancer Care Center. Cureus 2022, 14, e25814. [Google Scholar] [CrossRef]
- Tsujimura, H.; Miyaki, T.; Yamada, S.; Sugawara, T.; Ise, M.; Iwata, S.; Yonemoto, T.; Ikebe, D.; Itami, M.; Kumagai, K. Successful treatment of histiocytic sarcoma with induction chemotherapy consisting of dose-escalated CHOP plus etoposide and upfront consolidation auto-transplantation. Int. J. Hematol. 2014, 100, 507–510. [Google Scholar] [CrossRef]
- Zeidan, A.; Bolaños-Meade, J.; Kasamon, Y.; Aoki, J.; Borowitz, M.; Swinnen, L.; Symons, H.; Luznik, L.; Fuchs, E.; Jones, R.; et al. Human leukocyte antigen-haploidentical hematopoietic stem cell transplant for a patient with histiocytic sarcoma. Leuk. Lymphoma 2012, 54, 655–657. [Google Scholar] [CrossRef] [PubMed]
- Schlick, K.; Aigelsreiter, A.; Pichler, M.; Reitter, S.; Neumeister, P.; Hoefler, G.; Beham-Schmid, C.; Linkesch, W. Histiocytic sarcoma—Targeted therapy: Novel therapeutic options? A series of 4 cases. Onkologie 2012, 35, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Gounder, M.M.; Solit, D.B.; Tap, W.D. Trametinib in Histiocytic Sarcoma with an Activating MAP2K1 (MEK1) Mutation. N. Engl. J. Med. 2018, 378, 1945–1947. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Patel, J.L.; Tao, R.; Cannon, R.B.; Monroe, M.; Goyal, G. Near Complete Response to Trametinib Treatment in Histiocytic Sarcoma Harboring a Somatic KRAS Mutation. J. Natl. Compr. Cancer Netw. 2022, 20, 618–621. [Google Scholar] [CrossRef] [PubMed]
- Idbaih, A.; Mokhtari, K.; Emile, J.-F.; Galanaud, D.; Belaid, H.; de Bernard, S.; Benameur, N.; Barlog, V.-C.; Psimaras, D.; Donadieu, J.; et al. Dramatic response of a BRAF V600E-mutated primary CNS histiocytic sarcoma to vemurafenib. Neurology 2014, 83, 1478–1480. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, J.L.; Freitag, C.E.; Hemminger, J.A.; Jones, J.A. BRAF V600E expression in histiocytic sarcoma associated with splenic marginal zone lymphoma: A case report. J. Med. Case Rep. 2017, 11, 92. [Google Scholar] [CrossRef] [PubMed]
- Furui, Y.; Kurata, T.; Komori, K.; Uchida, E.; Miyairi, Y.; Chiba, A.; Ogiso, Y.; Sakashita, K. A case of recurrent refractory cervical primary histiocytic sarcoma treated with pembrolizumab. Int. Cancer Conf. J. 2022, 11, 280–285. [Google Scholar] [CrossRef]
- Frampton, J.E. Pazopanib: A Review in Advanced Renal Cell Carcinoma. Target. Oncol. 2017, 12, 543–554. [Google Scholar] [CrossRef]
- Ward, J.E.; Stadler, W.M. Pazopanib in renal cell carcinoma. Clin. Cancer Res. 2010, 16, 5923–5927. [Google Scholar] [CrossRef]
- Kommalapati, A.; Tella, S.H.; Go, R.S.; Goyal, G. Predictors of survival, treatment patterns, and outcomes in histiocytic sarcoma. Leuk. Lymphoma 2018, 60, 553–555. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, M.; Xiao, F.; Fang, J.; Liu, Z.; Shen, Y.; Zhu, D.; Zhang, Y.; Hou, J.; Huang, H. Long-Term Remission with Novel Combined Immune-Targeted Treatment for Histiocytic Sarcoma Accompanied by Follicular Lymphoma: Case Report and Literature Review. Int. J. Mol. Sci. 2024, 25, 7293. https://doi.org/10.3390/ijms25137293
Zhang M, Xiao F, Fang J, Liu Z, Shen Y, Zhu D, Zhang Y, Hou J, Huang H. Long-Term Remission with Novel Combined Immune-Targeted Treatment for Histiocytic Sarcoma Accompanied by Follicular Lymphoma: Case Report and Literature Review. International Journal of Molecular Sciences. 2024; 25(13):7293. https://doi.org/10.3390/ijms25137293
Chicago/Turabian StyleZhang, Minyue, Fei Xiao, Jianchen Fang, Zebing Liu, Yanying Shen, Di Zhu, Yiwei Zhang, Jian Hou, and Honghui Huang. 2024. "Long-Term Remission with Novel Combined Immune-Targeted Treatment for Histiocytic Sarcoma Accompanied by Follicular Lymphoma: Case Report and Literature Review" International Journal of Molecular Sciences 25, no. 13: 7293. https://doi.org/10.3390/ijms25137293