
Stress-Related Chronic Fatigue Syndrome: A Case Report with a Positive Response to Alpha-Methyl-P-Tyrosine (AMPT) Treatment

Abstract
:1. Introduction
2. Case Description
2.1. Diagnostic Timeline
2.2. Biochemical and Genetic Analyses
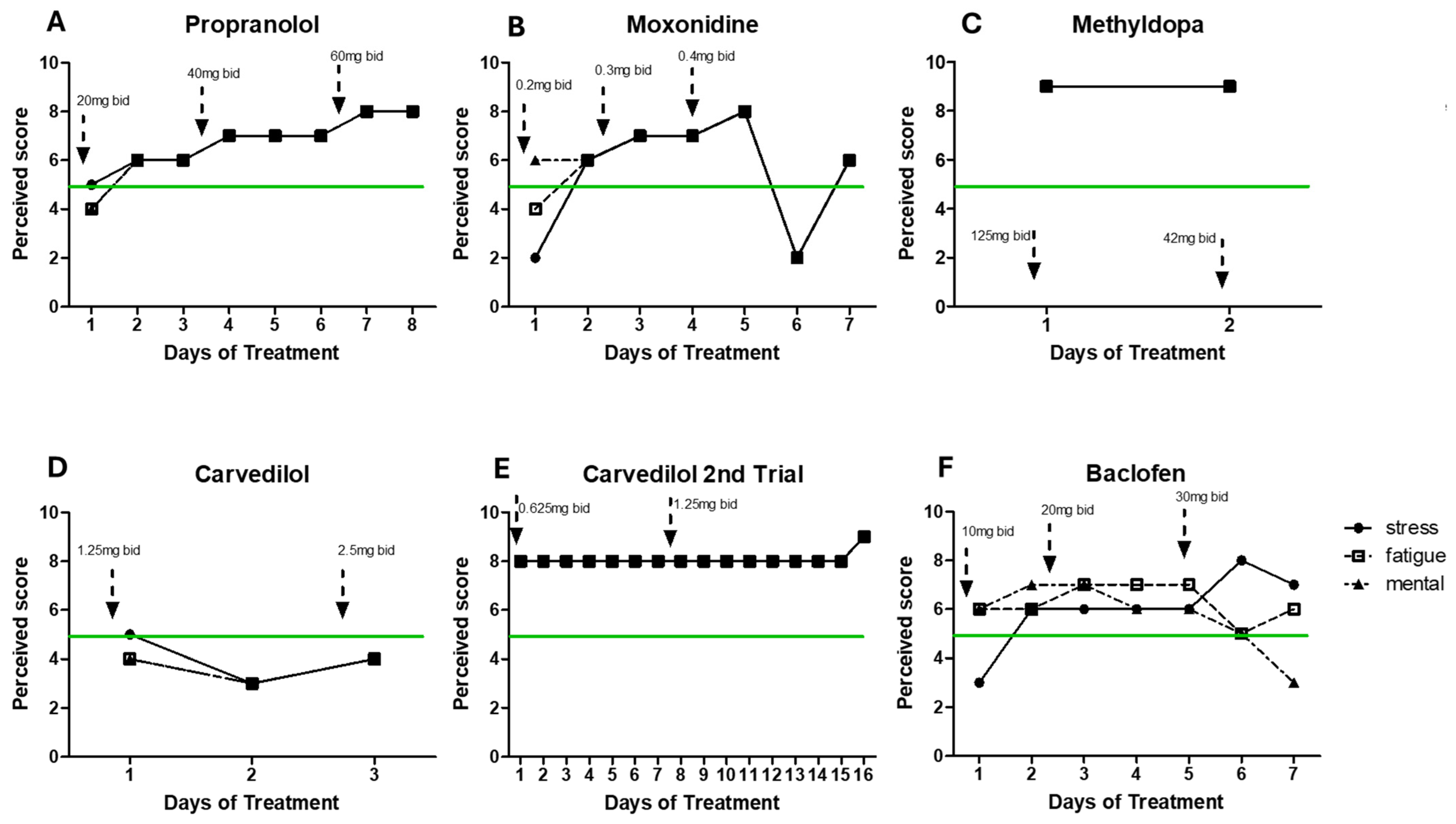
3. Treatment and Course of Symptoms
4. Materials and Methods
4.1. Clinical Analysis
4.2. Self-Evaluation Assessment of Symptoms
5. Summary and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harrison, J.E.; Weber, S.; Jakob, R.; Chute, C.G. ICD-11: An international classification of diseases for the twenty-first century. BMC Med. Inform. Decis. Mak. 2021, 21 (Suppl. S6), 206. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, B.M.; van De Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International consensus criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Sapra, A.; Bhandari, P. Chronic fatigue syndrome. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557676/ (accessed on 25 November 2023).
- Abdulla, J.; Torpy, B.D.J. Chronic fatigue syndrome. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., et al., Eds.; MDText.com, Inc.: Dartmouth, MA, USA, 2000. [Google Scholar]
- de Vega, W.C.; Herrera, S.; Vernon, S.D.; McGowan, P.O. Epigenetic modifications and glucocorticoid sensitivity in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). BMC Med. Genom. 2017, 10, 11. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.D. Use of Low-Dose Beta-Blockers to Treat Symptoms of Chronic Fatigue Syndrome. Master’s Thesis, The University of Utah, Salt Lake City, UT, USA, 2014. [Google Scholar]
- Montoya, J.G.; Holmes, T.H.; Anderson, J.N.; Maecker, H.T.; Rosenberg-Hasson, Y.; Valencia, I.J.; Chu, L.; Younger, J.W.; Tato, C.M.; Davis, M.M. Cytokine signature associated with disease severity in chronic fatigue syndrome patients. Proc. Natl. Acad. Sci. USA 2017, 114, E7150–E7158. [Google Scholar] [CrossRef]
- Brenu, E.W.; Hardcastle, S.L.; Atkinson, G.M.; van Driel, M.L.; Kreijkamp-Kaspers, S.; Ashton, K.J.; Staines, D.R.; Marshall-Gradisnik, S.M. Natural killer cells in patients with severe chronic fatigue syndrome. Autoimmun. Highlights 2013, 4, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Janal, M.N.; Ciccone, D.S.; Natelson, B.H. Sub-typing CFS patients on the basis of ‘minor’ symptoms. Biol. Psychol. 2006, 73, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Gimeno Pi, I.; Guitard Sein-Echaluce, M.L.; Rosselló Aubach, L.; Torres Puig-Gros, J.; Fernández Solà, J. Stressful events in the onset of chronic fatigue syndrome. Rev. Española De Salud Pública 2016, 90, e1–e7. [Google Scholar] [PubMed]
- Borsini, A.; Hepgul, N.; Mondelli, V.; Chalder, T.; Pariante, C.M. Childhood stressors in the development of fatigue syndromes: A review of the past 20 years of research. Psychol. Med. 2014, 44, 1809–1823. [Google Scholar] [CrossRef] [PubMed]
- Hall, D.L.; Lattie, E.G.; Milrad, S.F.; Czaja, S.; Fletcher, M.A.; Klimas, N.; Perdomo, D.; Antoni, M.H. Telephone-administered versus live group cognitive behavioral stress management for adults with CFS. J. Psychosom. Res. 2017, 93, 41–47. [Google Scholar] [CrossRef]
- Hall, D.L.; Lattie, E.G.; Antoni, M.H.; Fletcher, M.A.; Czaja, S.; Perdomo, D.; Klimas, N.G. Stress management skills, cortisol awakening response, and post-exertional malaise in chronic fatigue syndrome. Psychoneuroendocrinology 2014, 49, 26–31. [Google Scholar] [CrossRef]
- Powell, D.J.; Liossi, C.; Moss-Morris, R.; Schlotz, W. Unstimulated cortisol secretory activity in everyday life and its relationship with fatigue and chronic fatigue syndrome: A systematic review and subset meta-analysis. Psychoneuroendocrinology 2013, 38, 2405–2422. [Google Scholar] [CrossRef] [PubMed]
- Rajeevan, M.S.; Smith, A.K.; Dimulescu, I.; Unger, E.R.; Vernon, S.D.; Heim, C.; Reeves, W.C. Glucocorticoid receptor polymorphisms and haplotypes associated with chronic fatigue syndrome. Genes Brain Behav. 2007, 6, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Wyller, V.B.; Eriksen, H.R.; Malterud, K. Can sustained arousal explain the chronic fatigue syndrome? Behav. Brain Funct. 2009, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- Mar, P.L.; Raj, S.R. Postural orthostatic tachycardia syndrome: Mechanisms and new therapies. Annu. Rev. Med. 2020, 71, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Clinician Coalition ME/CFS Treatment Recommendations US ME/CFS Version 1. Bateman Horne Center, 2021. Available online: https://batemanhornecenter.org/wp-content/uploads/filebase/Treatment-Recs-MECFS-Clinician-Coalition-V1-Feb.-2021.pdf (accessed on 27 November 2023).
- Sommerfeldt, L.; Portilla, H.; Jacobsen, L.; Gjerstad, J.; Wyller, V.B. Polymorphisms of adrenergic cardiovascular control genes are associated with adolescent chronic fatigue syndrome. Acta Paediatr. 2011, 100, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.T.; Kossowsky, J.; Oberlander, T.F.; Kaptchuk, T.J.; Saul, J.P.; Wyller, V.B.; Fagermoen, E.; Sulheim, D.; Gjerstad, J.; Winger, A.; et al. Genetic variation in catechol-O-methyltransferase modifies effects of clonidine treatment in chronic fatigue syndrome. Pharmacogenomics J. 2016, 16, 454–460. [Google Scholar] [CrossRef]
- Polli, A.; Hendrix, J.; Ickmans, K.; Bakusic, J.; Ghosh, M.; Monteyne, D.; Velkeniers, B.; Bekaert, B.; Nijs, J.; Godderis, L. Genetic and epigenetic regulation of catechol-O-methyltransferase in relation to inflammation in chronic fatigue syndrome and fibromyalgia. J. Transl. Med. 2022, 20, 487. [Google Scholar] [CrossRef]
- Riley, D.S.; Barber, M.S.; Kienle, G.S.; Aronson, J.K.; von Schoen-Angerer, T.; Tugwell, P.; Kiene, H.; Helfand, M.; Altman, D.G.; Sox, H.; et al. CARE guidelines for case reports: Explanation and elaboration document. J. Clin. Epidemiol. 2017, 89, 218–235. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, S.Y.; Wang, D.; Wu, M.Z.; He, J.K.; Zhang, J.L.; Zhao, B.; Hou, L.W.; Wang, J.Y.; Wang, L.; et al. Transcutaneous Auricular Vagus Nerve Stimulation: From Concept to Application. Neurosci. Bull. 2021, 37, 853–862. [Google Scholar] [CrossRef]
- Jiménez, K.M.; Pereira-Morales, A.J.; Forero, D.A. MTHFR gene methylation is associated with perceived stress in healthy young adults. Psychiatr. Genet. 2018, 28, 41–46. [Google Scholar] [CrossRef]
- Wang, T.; Yin, J.; Miller, A.H.; Xiao, C. A systematic review of the association between fatigue and genetic polymorphisms. Brain Behav. Immun. 2017, 62, 230–244. [Google Scholar] [CrossRef] [PubMed]
- Prichard, B.N.; Owens, C.W.; Graham, B.R. Pharmacology and clinical use of moxonidine, a new centrally acting sympatholytic antihypertensive agent. J. Hum. Hypertens. 1997, 11 (Suppl. S1), S29–S45. [Google Scholar] [PubMed]
- Boot, E.; Booij, J.; Hasler, G.; Zinkstok, J.R.; de Haan, L.; Linszen, D.H.; van Amelsvoort, T.A. AMPT-induced monoamine depletion in humans: Evaluation of two alternative [123I]IBZM SPECT procedures. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Ballester-Servera, C.; Cañes, L.; Alonso, J.; Puertas, L.; Taurón, M.; Rodríguez, C.; Martínez-González, J. Nuclear receptor NOR-1 (Neuron-derived Orphan Receptor-1) in pathological vascular remodelling and vascular remodelling. Clínica E Investig. En Arterioscler. 2022, 34, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Graf, W.D.; Unis, A.S.; Yates, C.M.; Sulzbacher, S.; Dinulos, M.B.; Jack, R.M.; Dugaw, K.A.; Paddock, M.N.; Parson, W.W. Catecholamines in patients with 22q11.2 deletion syndrome and the low-activity COMT polymorphism. Neurology 2001, 57, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Longhurst, J.G.; Carpenter, L.L.; Epperson, C.; Price, L.H.; McDougle, C.J. Effects of catecholamine depletion with AMPT (alpha-methyl-para-tyrosine) in obsessive-compulsive disorder. Biol. Psychiatry 1999, 46, 573–576. [Google Scholar] [CrossRef]
- Voruganti, L.; Slomka, P.; Zabel, P.; Costa, G.; So, A.; Mattar, A.; Awad, A.G. Subjective effects of AMPT-induced dopamine depletion in schizophrenia: Correlation between dysphoric responses and striatal D(2) binding ratios on SPECT imaging. Neuropsychopharmacology 2001, 25, 642–650. [Google Scholar] [CrossRef] [PubMed]
- da Silva Alves, F.; Bakker, G.; Schmitz, N.; Abeling, N.; Hasler, G.; van der Meer, J.; Nederveen, A.; de Haan, L.; Linszen, D.; van Amelsvoort, T. Dopaminergic modulation of the reward system in schizophrenia: A placebo-controlled dopamine depletion fMRI study. Eur. Neuropsychopharmacol. 2013, 23, 1577–1586. [Google Scholar] [CrossRef]
- Miller, H.L.; Delgado, P.L.; Salomon, R.M.; Heninger, G.R.; Charney, D.S. Effects of alpha-methyl-para-tyrosine (AMPT) in drug-free depressed patients. Neuropsychopharmacology 1996, 14, 151–157. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biochemical Target | Normal Range | Unit | Level | Value | Date of Measurement |
|---|---|---|---|---|---|
| 5-HIAA (5-hydroxyindoleacetic acid) | <2.40 | mg/g | High | 3.05 * | November 2021 |
| Adrenaline | <20 | μg | Normal | 11 | August 2012 |
| Normal | 3.5 | July 2022 | |||
| Normal | 10.22 | March 2023 | |||
| B1 adrenergic receptor autoantibody | <15 | U/mL | High | 17.9 * | July 2021 |
| B2 adrenergic receptor autoantibody | <8 | U/mL | High | 13.5 * | July 2021 |
| Dopamine (plasma) | <85 | ng/L | Normal | 81 | March 2023 |
| GABA urine/creatinine | 3–13.6 | μmol/g | High | 15.4 * | July 2022 |
| Glutamate urine/creatinine | 8–25 | μmol/gCrea | High | 42.4 * | July 2022 |
| M3-muscarinic autoantibodies AChR | <6 | U/mL | High | 8.4 * | July 2021 |
| Metanephrine | <350 | μg | Normal | 78 | August 2012 |
| High | 427 * | March 2023 | |||
| Noradrenaline | <90 | μg | Normal | 77 | August 2012 |
| Normal | 19.5 | July 2022 | |||
| Noradrenaline | 70–750 (lying) | ng/L | Normal | 167 | March 2023 |
| Noradrenaline | 200–1700 (standing) | ng/L | Normal | 518 | March 2023 |
| Noradrenaline urine/creatinine | 32–58 | μg/gCrea | High | 64.9 * | July 2022 |
| Noradrenaline/adrenaline | 3–6 | quotient | Normal | 5.6 | July 2022 |
| Normetanephrine | <600 | μg | Normal | 270 | August 2012 |
| Quinolinic acid | <5.50 | mg/g | High | 6.11 * | November 2021 |
| Serotonin | 50–20 | μg/L | Normal | 39.7 | July 2022 |
| Serotonin urine/creatinine | 148–230 | μg/gCrea | Low | 131.9 * | July 2022 |
| Taurine | 5.4–31.3 | mg/L | Low | 4.8 * | July 2022 |
| Tryptophan | 7.30–12.50 | mg/g | Normal | 9.86 | November 2021 |
| Normal | 10.5 | July 2022 | |||
| Tyrosine | 38.5–84.3 | μmol/L | Low | 35.18 * | November 2021 |
| Low | 36.43 * | July 2022 | |||
| VMA (vanillyl mandelic acid) | <3 | mg/g | High | 3.14 * | November 2021 |
| Gene Target | Locus (GRCh38) | rs ID | Genotype | Gene Region |
|---|---|---|---|---|
| COMT | 22q11.21 | rs4680 | A/A homozygote | coding |
| MAOA | Xp11.3 | VNTR30bp | High copy number | promoter |
| MAOB | Xp11.3 | rs1799836 | T/T homozygote | intron |
| FKBP5 | 6p21.31 | rs1360780 | C/T heterozygote | intron |
| FKBP5 | 6p21.31 | rs9470080 | C/T heterozygote | intron |
| FKBP5 | 6p21.31 | rs4713916 | G/A heterozygote | intron |
| FKBP5 | 6p21.31 | rs9296158 | G/A heterozygote | intron |
| NR3C1 | 5q31.3 | rs6198 | G/A heterozygote | 3´UTR |
| MTHFR | 1p36.22 | rs1801133 | C/T heterozygote | coding |
| SOD2 | 6q25.3 | rs4880 | C/T heterozygote | coding |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ljungström, M.; Oltra, E.; Pardo, M. Stress-Related Chronic Fatigue Syndrome: A Case Report with a Positive Response to Alpha-Methyl-P-Tyrosine (AMPT) Treatment. Int. J. Mol. Sci. 2024, 25, 7778. https://doi.org/10.3390/ijms25147778
Ljungström M, Oltra E, Pardo M. Stress-Related Chronic Fatigue Syndrome: A Case Report with a Positive Response to Alpha-Methyl-P-Tyrosine (AMPT) Treatment. International Journal of Molecular Sciences. 2024; 25(14):7778. https://doi.org/10.3390/ijms25147778
Chicago/Turabian StyleLjungström, Maria, Elisa Oltra, and Marta Pardo. 2024. "Stress-Related Chronic Fatigue Syndrome: A Case Report with a Positive Response to Alpha-Methyl-P-Tyrosine (AMPT) Treatment" International Journal of Molecular Sciences 25, no. 14: 7778. https://doi.org/10.3390/ijms25147778