
Redox Balance and Inflammatory Response in Follicular Fluids of Women Recovered by SARS-CoV-2 Infection or Anti-COVID-19 Vaccinated: A Combined Metabolomics and Biochemical Study

 , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. Patient Data
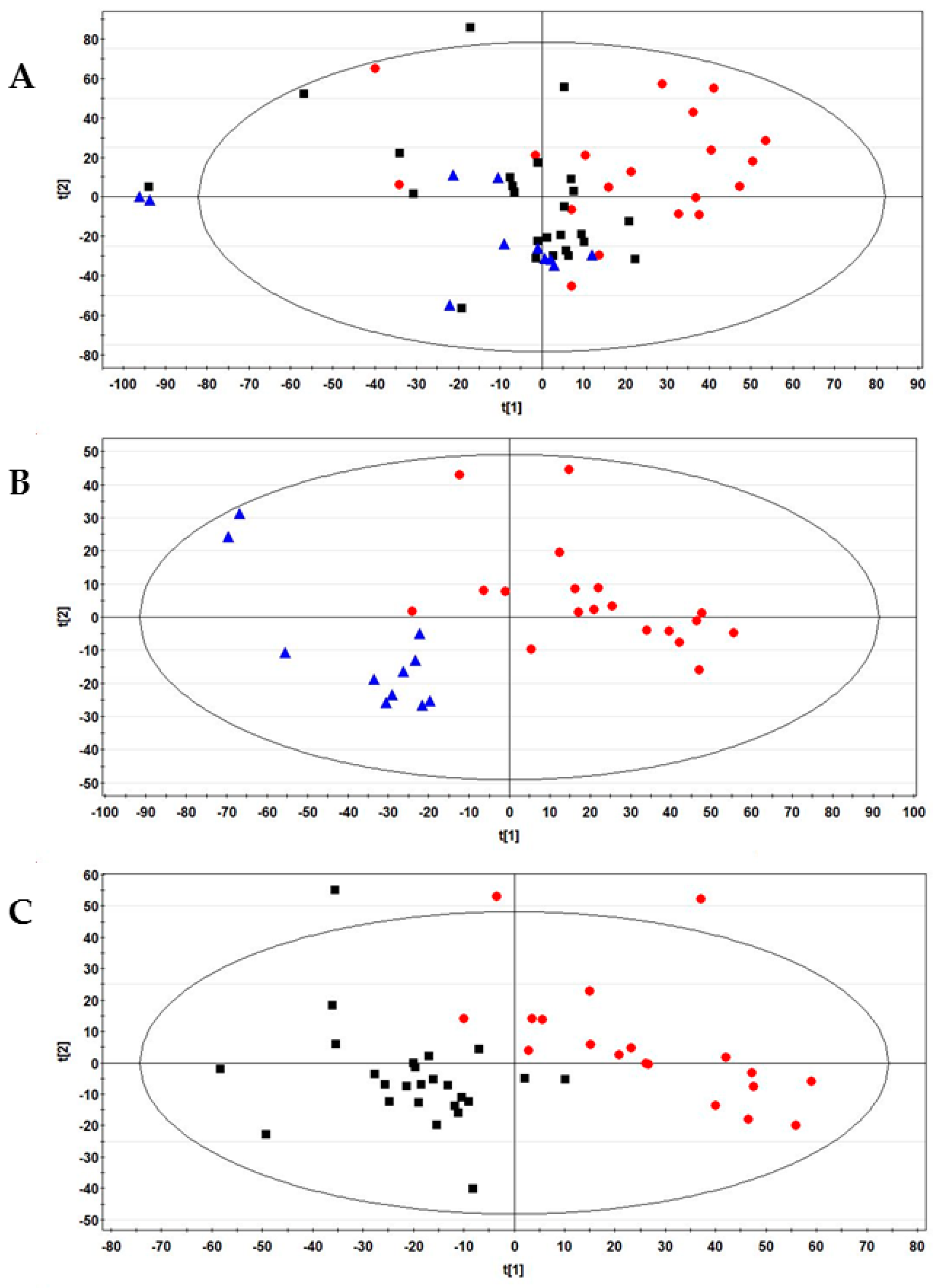
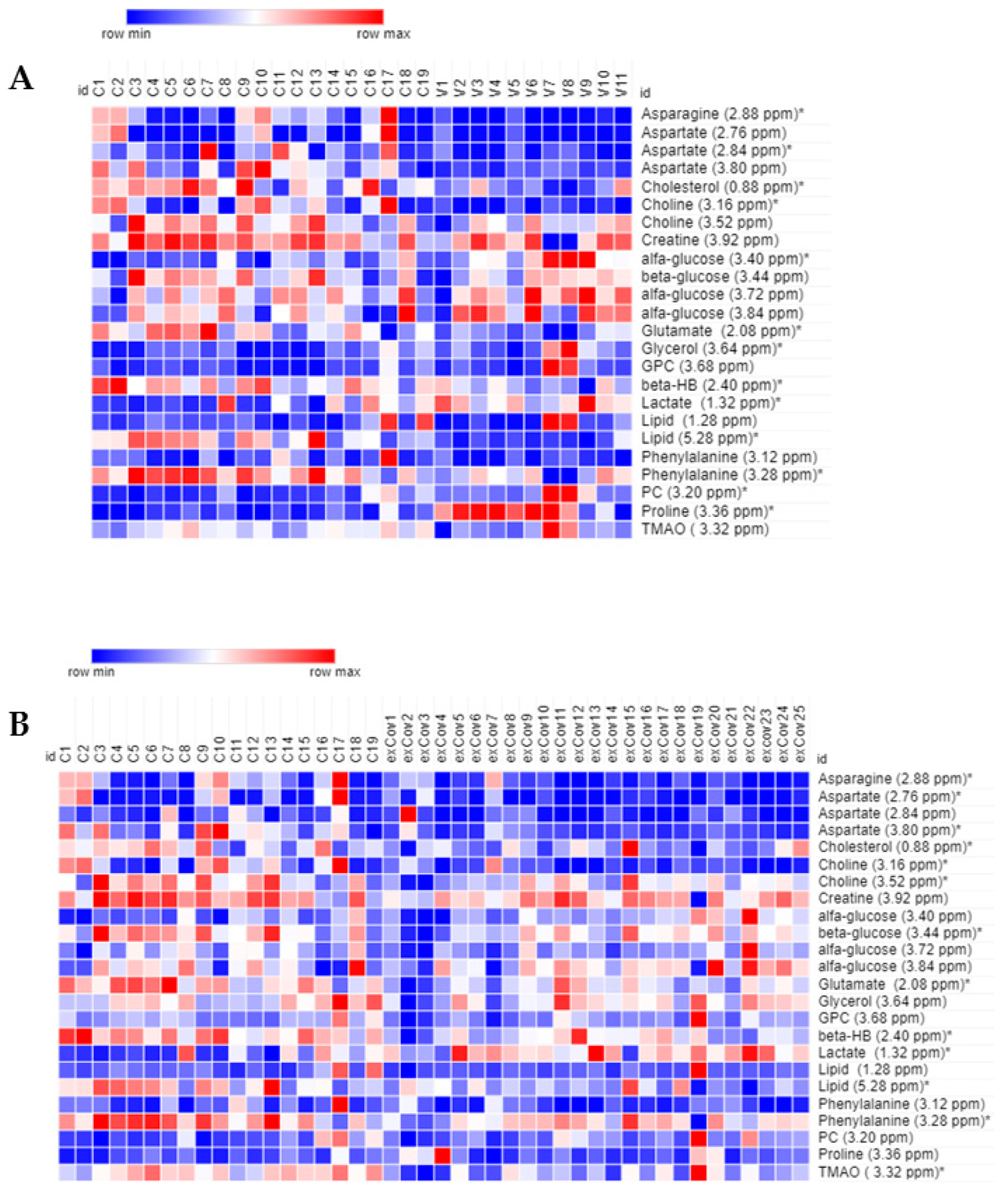
2.2. NMR Results
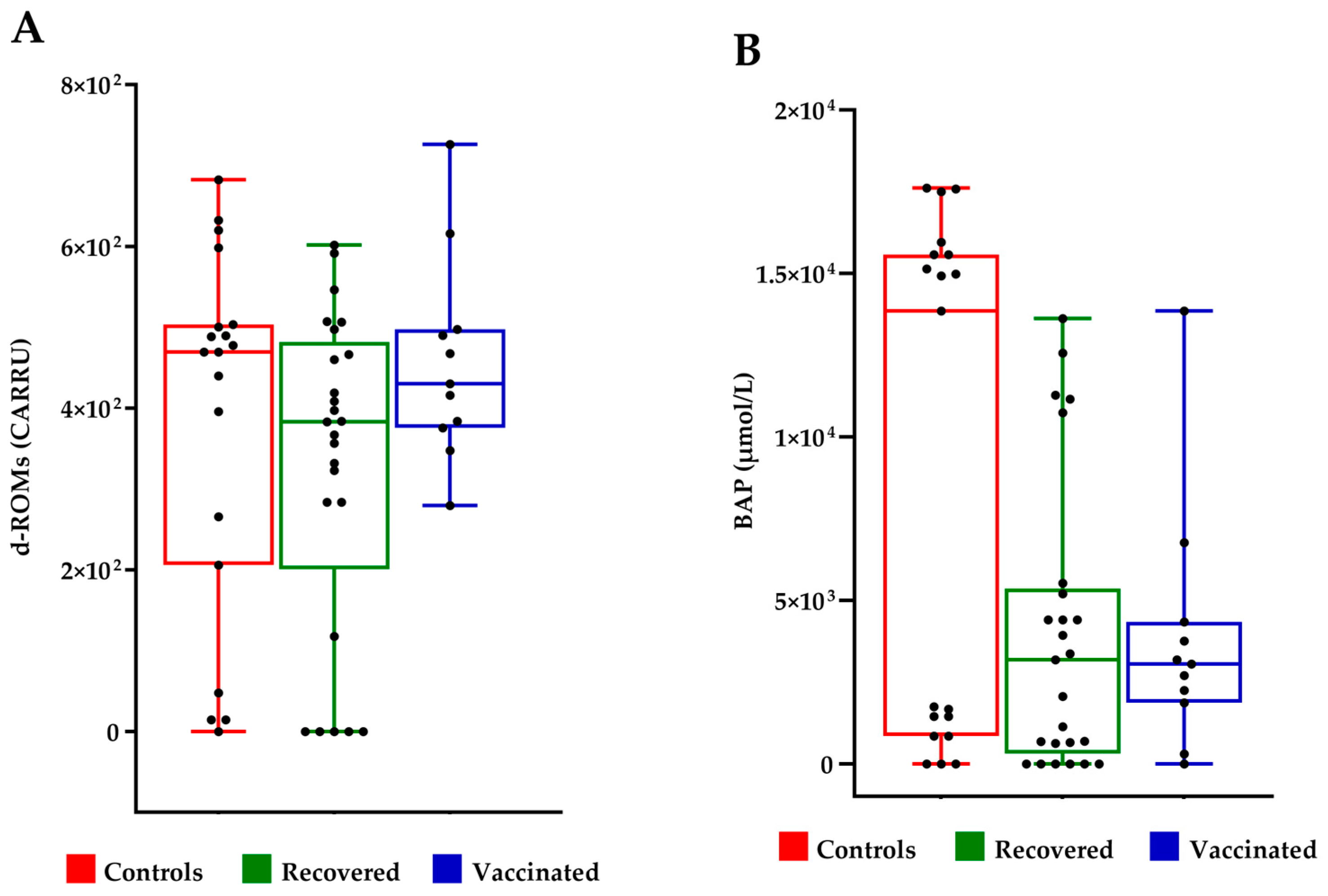
2.3. Evaluation of Oxidative Stress and Antioxidant Capacity
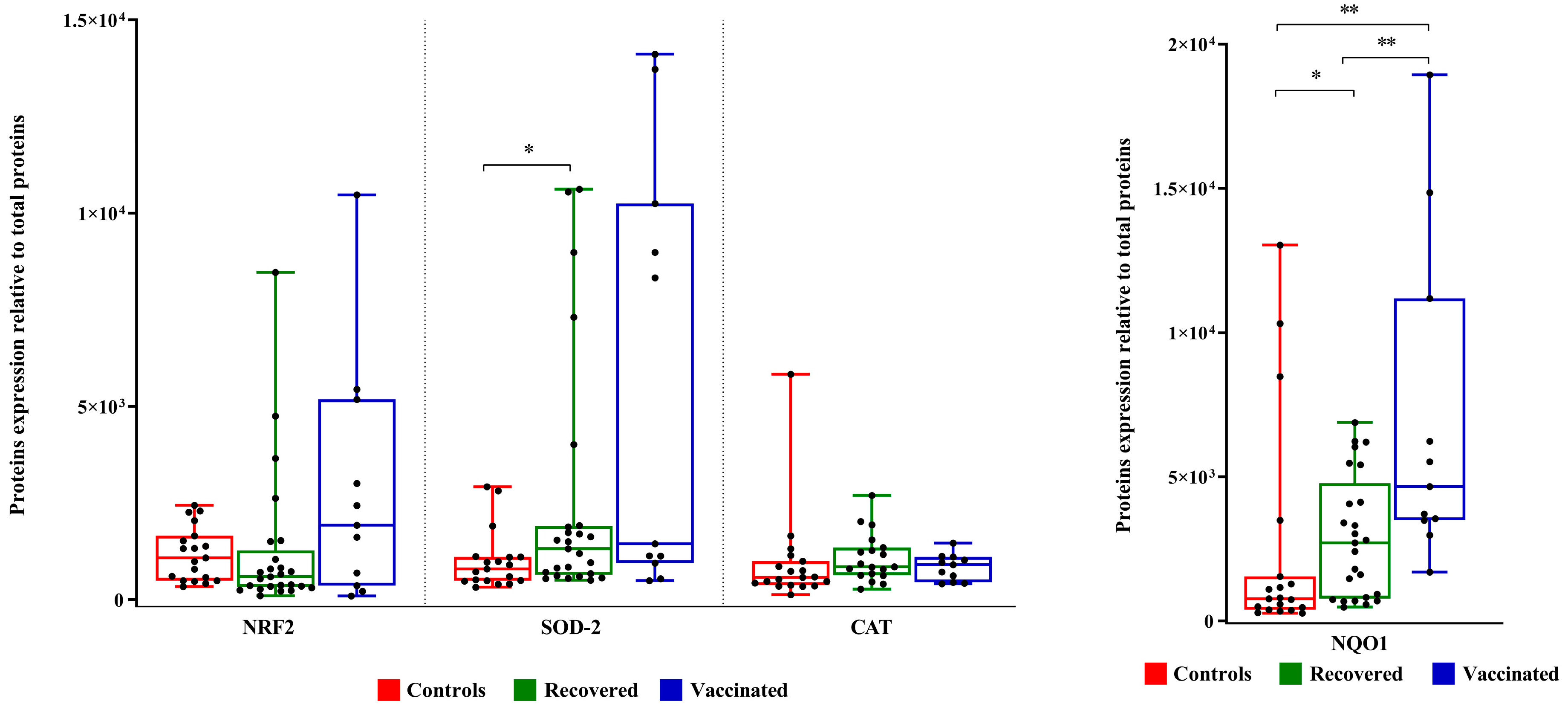
2.4. Expression Analysis of Oxidative Stress Biomarkers
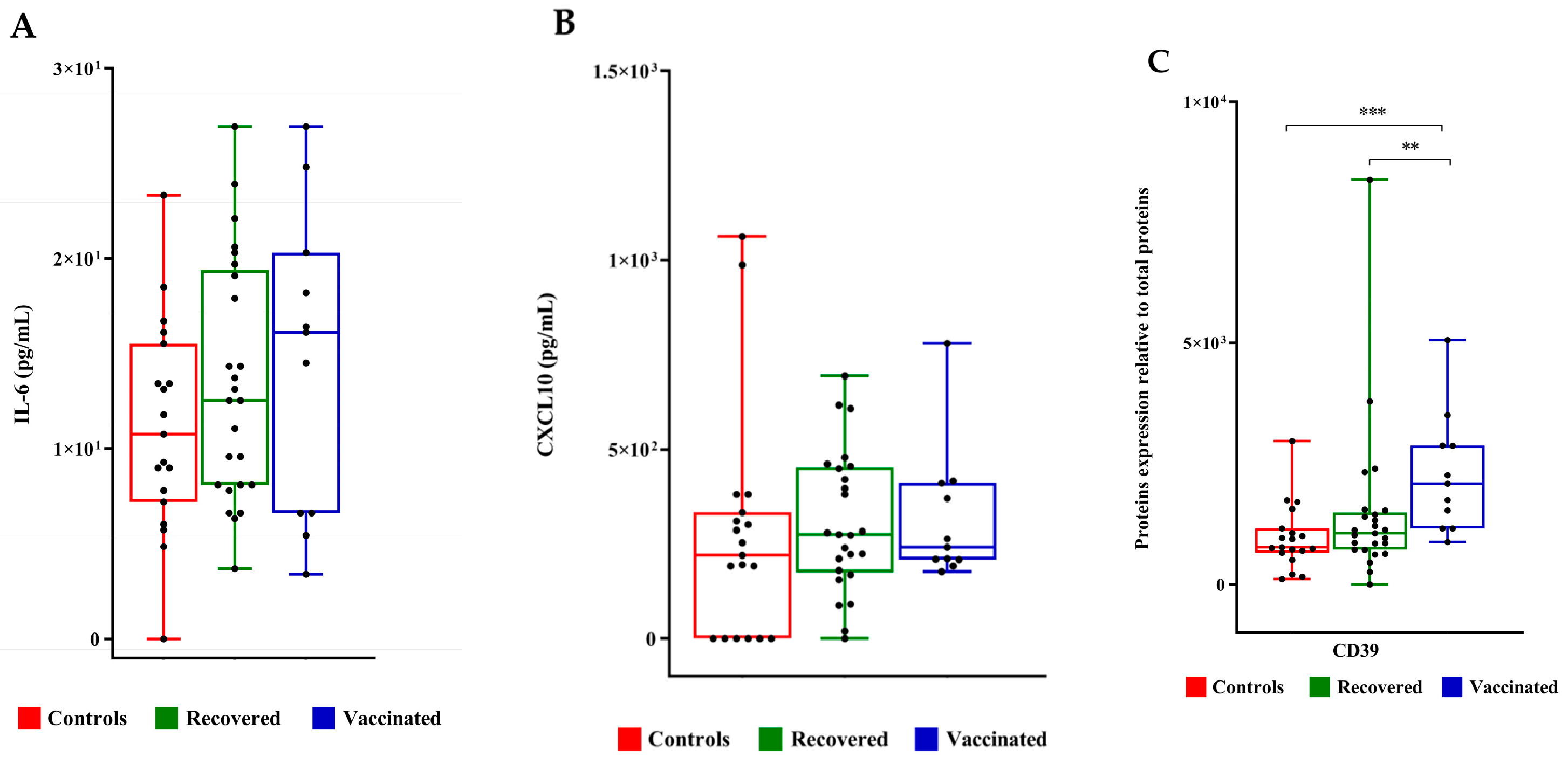
2.5. Analysis of Biomarkers of Inflammation
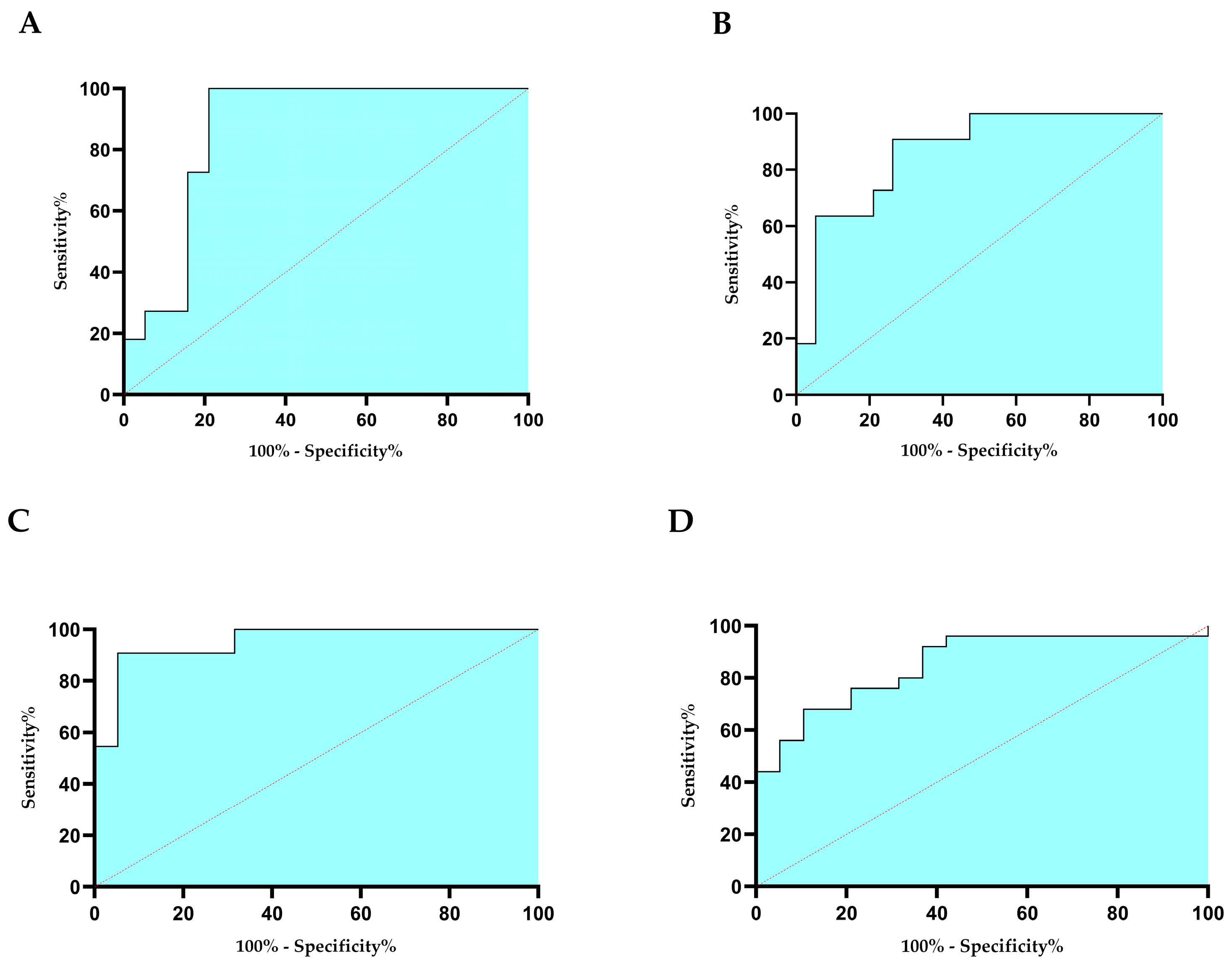
2.6. Evaluation of the Diagnostic Importance of Detected Biomarkers and Metabolites
2.7. Relationships between NMR Variables with Clinical Parameters and Proteins
3. Discussion
4. Materials and Methods
4.1. Study Participants
4.2. NMR Sample Analysis
4.3. Multivariate Analysis
4.4. Oxidative Balance Evaluation
4.5. Western Blot Analysis
4.6. ELISA
4.7. Statistical Analysis
4.8. ROC Analysis
4.9. Correlation Tests
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ata, B.; Vermeulen, N.; Mocanu, E.; Gianaroli, L.; Lundin, K.; Rautakallio-Hokkanen, S.; Tapanainen, J.S.; Veiga, A. SARS-CoV-2, fertility and assisted reproduction. Hum. Reprod. Update. 2023, 29, 177–196. [Google Scholar] [CrossRef]
- Madni, S.A.; Sharma, A.J.; Zauche, L.H.; Waters, A.V.; Nahabedian, J.F., 3rd; Johnson, T.; Olson, C.K. CDC COVID-19 Vaccine Pregnancy Registry Work Group. CDC COVID-19 Vaccine Pregnancy Registry: Design, data collection, response rates, and cohort description. Vaccine. 2023, 42, 1469–1477. [Google Scholar] [CrossRef] [PubMed]
- Alviggi, C.; Esteves, S.C.; Orvieto, R.; Conforti, A.; La Marca, A.; Fischer, R.; Andersen, C.Y.; Bühler, K.; Sunkara, S.K.; Polyzos, N.P.; et al. POSEIDON (Patient-Oriented Strategies Encompassing IndividualizeD Oocyte Number) group. COVID-19 and assisted reproductive technology services: Repercussions for patients and proposal for individualized clinical management. Reprod. Biol. Endocrinol. 2020, 18, 45. [Google Scholar] [CrossRef]
- Madjunkov, M.; Dviri, M.; Librach, C. A comprehensive review of the impact of COVID-19 on human reproductive biology, assisted reproduction care and pregnancy: A Canadian perspective. J. Ovarian Res. 2020, 13, 140. [Google Scholar] [CrossRef] [PubMed]
- Elsaddig, M.; Khalil, A. Effects of the COVID pandemic on pregnancy outcomes. Best. Pract. Res. Clin. Obstet. Gynaecol. 2021, 73, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chen, S.; Chen, M.; Xing, C.; Su, D.; Fan, L.; Xu, D.; Tian, L.; Xia, L.; Zhang, K.; et al. Impact of prior coronavirus disease 2019 infection in females on assisted reproductive outcomes: A systematic review with meta-analysis. Clin Transl Disc. 2023, 3, e251. [Google Scholar] [CrossRef]
- Kaur, H.; Chauhan, A.; Mascarenhas, M. Does SARS Cov-2 infection affect the IVF outcome—A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2024, 292, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Carp-Veliscu, A.; Mehedintu, C.; Frincu, F.; Bratila, E.; Rasu, S.; Iordache, I.; Bordea, A.; Braga, M. The Effects of SARS-CoV-2 Infection on Female Fertility: A Review of the Literature. Int. J. Environ. Res. Public Health 2022, 19, 984. [Google Scholar] [CrossRef] [PubMed]
- Zaçe, D.; La Gatta, E.; Petrella, L.; Di Pietro, M.L. The impact of COVID-19 vaccines on fertility-A systematic review and meta-analysis. Vaccine 2022, 40, 6023–6034. [Google Scholar] [CrossRef]
- Braun, A.S.; Feil, K.; Reiser, E.; Weiss, G.; von Steuben, T.; Pinggera, G.M.; Köhn, F.M.; Toth, B. Corona and Reproduction, or Why the Corona Vaccination Does Not Result in Infertility. Geburtshilfe Frauenheilkd. 2022, 82, 490–500. [Google Scholar] [CrossRef]
- Zhang, X.; Li, X.; Chen, W.; Wu, S.; Qi, X.; Bian, J.; Gao, S.; Lu, Y.; Tan, J. SARS-CoV-2 infection, vaccination and in vitro fertilization treatment: A prospective cohort study. Int. Immunopharmacol. 2024, 135, 112291. [Google Scholar] [CrossRef]
- Youngster, M.; Maman, O.; Kedem, A.; Avraham, S.; Rabbi, M.L.; Gat, I.; Yerushalmi, G.; Baum, M.; Hourvitz, A.; Maman, E. The effect of COVID-19 vaccination during IVF stimulation on cycle outcomes—A retrospective cohort study. J. Reprod. Immunol. 2024, 163, 104246. [Google Scholar] [CrossRef]
- Ba, Z.; Yang, A.; Zhu, S.; Li, Y.; Ma, J.; Zhang, Y.; Li, Z.; Chen, F. Comprehensive evaluation of the effect of inactivated SARS-CoV-2 vaccination on female fertility: A retrospective cohort study. J. Med. Virol. 2023, 95, e29161. [Google Scholar] [CrossRef]
- Castiglione Morelli, M.A.; Iuliano, A.; Schettini, S.C.A.; Ferri, A.; Colucci, P.; Viggiani, L.; Matera, I.; Ostuni, A. Are the Follicular Fluid Characteristics of Recovered Coronavirus Disease 2019 Patients Different From Those of Vaccinated Women Approaching in vitro Fertilization? Front. Physiol. 2022, 13, 840109. [Google Scholar] [CrossRef]
- Morgenstern, C.; Lastres-Becker, I.; Demirdöğen, B.C.; Costa, V.M.; Daiber, A.; Foresti, R.; Motterlini, R.; Kalyoncu, S.; Arioz, B.I.; Genc, S.; et al. Biomarkers of NRF2 signalling: Current status and future challenges. Redox Biol. 2024, 72, 103134. [Google Scholar] [CrossRef]
- Ross, D.; Siegel, D. The diverse functionality of NQO1 and its roles in redox control. Redox Biol. 2021, 41, 101950. [Google Scholar] [CrossRef]
- Morello, S.; Caiazzo, E.; Turiello, R.; Cicala, C. Thrombo-Inflammation: A Focus on NTPDase1/CD39. Cells 2021, 10, 2223. [Google Scholar] [CrossRef]
- Jing, Y.; Run-Qian, L.; Hao-Ran, W.; Hao-Ran, C.; Ya-Bin, L.; Yang, G.; Fei, C. Potential influence of COVID-19/ACE2 on the female reproductive system. Mol. Hum. Reprod. 2020, 26, 367–373. [Google Scholar] [CrossRef]
- Pourmasumi, S.; Kounis, N.G.; Naderi, M.; Hosseinisadat, R.; Khoradmehr, A.; Fagheirelahee, N.; Kouni, S.N.; de Gregorio, C.; Dousdampanis, P.; Mplani, V.; et al. Effects of COVID-19 Infection and Vaccination on the Female Reproductive System: A Narrative Review. Balk. Med. J. 2023, 40, 153–164. [Google Scholar] [CrossRef]
- Li, R.; Yin, T.; Fang, F.; Li, Q.; Chen, J.; Wang, Y.; Hao, Y.; Wu, G.; Duan, P.; Wang, Y.; et al. Potential risks of SARS-CoV-2 infection on reproductive health. Reprod. Biomed. Online 2020, 41, 89–95. [Google Scholar] [CrossRef]
- Harb, J.; Debs, N.; Rima, M.; Wu, Y.; Cao, Z.; Kovacic, H.; Fajloun, Z.; Sabatier, J.-M. SARS-CoV-2, COVID-19, and Reproduction: Effects on Fertility, Pregnancy, and Neonatal Life. Biomedicines 2022, 10, 1775. [Google Scholar] [CrossRef] [PubMed]
- Bentov, Y.; Beharier, O.; Moav-Zafrir, A.; Kabessa, M.; Godin, M.; Greenfield, C.S.; Ketzinel-Gilad, M.; Ash Broder, E.; Holzer, H.E.; Wolf, D.; et al. Ovarian follicular function is not altered by SARS-CoV-2 infection or BNT162b2 mRNA COVID-19 vaccination. Hum Reprod. 2021, 36, 2506–2513. [Google Scholar] [CrossRef] [PubMed]
- Ding, T.; Wang, T.; Zhang, J.; Cui, P.; Chen, Z.; Zhou, S.; Yuan, S.; Ma, W.; Zhang, M.; Rong, Y.; et al. Analysis of Ovarian Injury Associated With COVID-19 Disease in Reproductive-Aged Women in Wuhan, China: An Observational Study. Front Med. 2021, 8, 635255. [Google Scholar] [CrossRef] [PubMed]
- Herrero, Y.; Pascuali, N.; Velazquez, C.; Oubina, G.; Hauk, V.; de Zuniga, I.; Peña, M.G.; Martinez, G.; Lavolpe, M.; Veiga, F.; et al. SARS-CoV-2 infection negatively affects ovarian function in ART patients. Biochim. Biophys. Acta. Mol. Basis Dis. 2022, 1868, 166295. [Google Scholar] [CrossRef] [PubMed]
- Orvieto, R.; Segev-Zahav, A.; Aizer, A. Does COVID-19 infection influence patients’ performance during IVF-ET cycle?: An observational study. Gynecol Endocrinol. 2021, 37, 895–897. [Google Scholar] [CrossRef] [PubMed]
- D’Ippolito, S.; Turchiano, F.; Vitagliano, A.; Scutiero, G.; Lanzone, A.; Scambia, G.; Greco, P. Is There a Role for SARS-CoV-2/COVID-19 on the Female Reproductive System? Front. Physiol. 2022, 13, 845156. [Google Scholar] [CrossRef] [PubMed]
- Hood, R.B.; Liang, D.; Tan, Y.; Ford, J.; Souter, I.; Jones, D.P.; Hauser, R.; Gaskins, A.J. Characterizing the follicular fluid metabolome: Quantifying the correlation across follicles and differences with the serum metabolome. Fertil. Steril. 2022, 118, 970–979. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, J.; Zhang, L. The Impact of Follicular Fluid Oxidative Stress Levels on the Outcomes of Assisted Reproductive Therapy. Antioxidants 2023, 12, 2117. [Google Scholar] [CrossRef] [PubMed]
- Awonuga, A.O.; Camp, O.G.; Abu-Soud, H.M. A review of nitric oxide and oxidative stress in typical ovulatory women and in the pathogenesis of ovulatory dysfunction in PCOS. Reprod Biol Endocrinol. 2023, 21, 111. [Google Scholar] [CrossRef]
- Liu, J.; Zhu, K.; Xu, S.; Tu, W.; Lin, X.; Su, Y.; Huang, R.; Deng, Y.; Liu, Y. Double-edged sword: Effects of human sperm reactive oxygen species on embryo development in IVF cycles. Reprod Biol Endocrinol. 2023, 21, 1. [Google Scholar] [CrossRef]
- Várnagy, Á.; K˝oszegi, T.; Györgyi, E.; Szegedi, S.; Sulyok, E.; Prémusz, V.; Bódis, J. Levels of total antioxidant capacity and 8-hydroxy-20-deoxyguanosine of serum and follicular fluid in women undergoing in vitro fertilization: Focusing on endometriosis. Hum. Fertil. 2018, 23, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Gain, C.; Song, S.; Angtuaco, T.; Satta, S.; Kelesidis, T. The role of oxidative stress in the pathogenesis of infections with coronaviruses. Front. Microbiol. 2023, 13, 1111930. [Google Scholar] [CrossRef]
- Georgieva, E.; Ananiev, J.; Yovchev, Y.; Arabadzhiev, G.; Abrashev, H.; Abrasheva, D.; Atanasov, V.; Kostandieva, R.; Mitev, M.; Petkova-Parlapanska, K.; et al. COVID-19 Complications: Oxidative Stress, Inflammation, and Mitochondrial and Endothelial Dysfunction. Int. J. Mol. Sci. 2023, 24, 14876. [Google Scholar] [CrossRef]
- Castiglione Morelli, M.A.; Iuliano, A.; Matera, I.; Viggiani, L.; Schettini, S.C.A.; Colucci, P.; Ostuni, A. A Pilot Study Biochem. Profile Follicular Fluid Breast Cancer Patients. Metabolites 2023, 13, 441. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.K.; Lindon, J.C.; Holmes, E. ‘Metabonomics’: Understanding the metabolic responses of living systems to pathophysiological stimuli via multivariate statistical analysis of biological NMR spectroscopic data. Xenobiotica 1999, 29, 1181–1189. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients with Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An Inflammatory Cytokine Signature Predicts COVID-19 Severity and Survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef]
- Wang, C.; Sun, Y. Induction of Collagen I by CXCL10 in Ovarian Theca-Stroma Cells via the JNK Pathway. Front. Endocrinol. 2022, 13, 823740. [Google Scholar] [CrossRef] [PubMed]
- Díaz-García, E.; García-Tovar, S.; Alfaro, E.; Zamarrón, E.; Mangas, A.; Galera, R.; Ruíz-Hernández, J.J.; Solé-Violán, J.; Rodríguez-Gallego, C.; Van-Den-Rym, A.; et al. Role of CD39 in COVID-19 Severity: Dysregulation of Purinergic Signaling and Thromboinflammation. Front. Immunol. 2022, 13, 847894. [Google Scholar] [CrossRef]
- Shanmugham, M.; Bellanger, S.; Leo, C.H. Gut-Derived Metabolite, Trimethylamine-N-oxide (TMAO) in Cardio-Metabolic Diseases: Detection, Mechanism, and Potential Therapeutics. Pharmaceuticals 2023, 16, 504. [Google Scholar] [CrossRef]
- Shahini Shams Abadi, M.; Khodashahi, R.; Aliakbarian, M.; Beiraghdar, F.; Arjmand, M. The Association Between the Gut Microbiome and COVID-19 Severity: The Potential Role of TMAO Produced by the Gut Microbiome. Arch. Clin. Infect. Dis. 2023, 18, e140346. [Google Scholar] [CrossRef]
- Nappi, F.; Iervolino, A.; Avtaar Singh, S.S. Thromboembolic Complications of SARS-CoV-2 and Metabolic Derangements: Suggestions from Clinical Practice Evidence to Causative Agents. Metabolites 2021, 11, 341. [Google Scholar] [CrossRef] [PubMed]
- Chandel, N.S. Nucleotide Metabolism. Cold Spring Harb. Perspect. Biol. 2021, 13, a040592. [Google Scholar] [CrossRef] [PubMed]
- Castiglione Morelli, M.; Iuliano, A.; Schettini, S.C.A.; Petruzzi, D.; Ferri, A.; Colucci, P.; Viggiani, L.; Cuviello, F.; Ostuni, A. NMR metabolic profiling of follicular fluid for investigating the different causes of female infertility: A pilot study. Metabolomics 2019, 15, 19. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control § | SARS-CoV-2 Vaccinated | Recovered COVID-19 | |
|---|---|---|---|
| Number of patients | 19 | 11 | 25 |
| Age (years) | 36.9 (3.8) | 35.7 (4.4) | 37.1 (4.3) |
| FSH (UI/mL) | 7.1 (1.7) | 6.7 (2.6) | 6.5 (2.6) |
| AMH (ng/mL) | 5.3 (3.6) | 3.2 (2.9) | 2.4 (1.2) |
| AFC | 14.2 (3.2) | 15.1 (7.5) | 11.4 (8.3) |
| Estradiol (pg/mL) | 1675.0 (1065.5) | 1972.9 (1250.1) | 1763.0 (132.9) |
| Progesterone (ng/mL) | 1.3 (0.7) | 1.3 (0.9) | 1.3 (0.3) |
| BMI (kg/m2) | 22.5 (3.4) | 23.9 (4.1) | 23.8 (5.3) |
| Follicles monitored | 9.8 (4.9) | 11.3 (5.9) | 9.5 (6.9) |
| Total oocytes collected | 8.2 (5.0) | 7.5 (3.9) | 5.6 (4.3) |
| MII oocytes * | 6.9 (4.8) | 5.4 (3.9) | 3.6 (2.6) |
| Zygotes * | 1.4 (0.8) | 4.1 (2.5) | 2.7 (1.7) |
| Blastocysts | 1.3 (0.7) | 2.3 (2.4) | 1.4 (1.2) |
| Pregnancy rate % | 31.3 (5/16) | 45.5 (5/11) | 56 (9/17) |
| Pregnancy loss % | 20 (1/5) | 20 (1/5) | 11.1 (1/9) |
| Live Birth Rate per ET % | 25 (4/16) | 36.4 (4/11) | 47 (8/17) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castiglione Morelli, M.A.; Iuliano, A.; Viggiani, L.; Matera, I.; Pistone, A.; Schettini, S.C.A.; Colucci, P.; Ostuni, A. Redox Balance and Inflammatory Response in Follicular Fluids of Women Recovered by SARS-CoV-2 Infection or Anti-COVID-19 Vaccinated: A Combined Metabolomics and Biochemical Study. Int. J. Mol. Sci. 2024, 25, 8400. https://doi.org/10.3390/ijms25158400
Castiglione Morelli MA, Iuliano A, Viggiani L, Matera I, Pistone A, Schettini SCA, Colucci P, Ostuni A. Redox Balance and Inflammatory Response in Follicular Fluids of Women Recovered by SARS-CoV-2 Infection or Anti-COVID-19 Vaccinated: A Combined Metabolomics and Biochemical Study. International Journal of Molecular Sciences. 2024; 25(15):8400. https://doi.org/10.3390/ijms25158400
Chicago/Turabian StyleCastiglione Morelli, Maria A., Assunta Iuliano, Licia Viggiani, Ilenia Matera, Alessandro Pistone, Sergio C. A. Schettini, Paola Colucci, and Angela Ostuni. 2024. "Redox Balance and Inflammatory Response in Follicular Fluids of Women Recovered by SARS-CoV-2 Infection or Anti-COVID-19 Vaccinated: A Combined Metabolomics and Biochemical Study" International Journal of Molecular Sciences 25, no. 15: 8400. https://doi.org/10.3390/ijms25158400
APA StyleCastiglione Morelli, M. A., Iuliano, A., Viggiani, L., Matera, I., Pistone, A., Schettini, S. C. A., Colucci, P., & Ostuni, A. (2024). Redox Balance and Inflammatory Response in Follicular Fluids of Women Recovered by SARS-CoV-2 Infection or Anti-COVID-19 Vaccinated: A Combined Metabolomics and Biochemical Study. International Journal of Molecular Sciences, 25(15), 8400. https://doi.org/10.3390/ijms25158400