


Anti-Cancer Properties of Two Intravenously Administrable Curcumin Formulations as Evaluated in the 3D Patient-Derived Cancer Spheroid Model

Abstract
1. Introduction
2. Results
2.1. Patient Collective
2.2. Anti-Cancer Effects of Curcumin Formulations in PDCS
2.3. Anti-Cancer Effects of Curcumin Formulations Depending on Patient Cohort Parameters
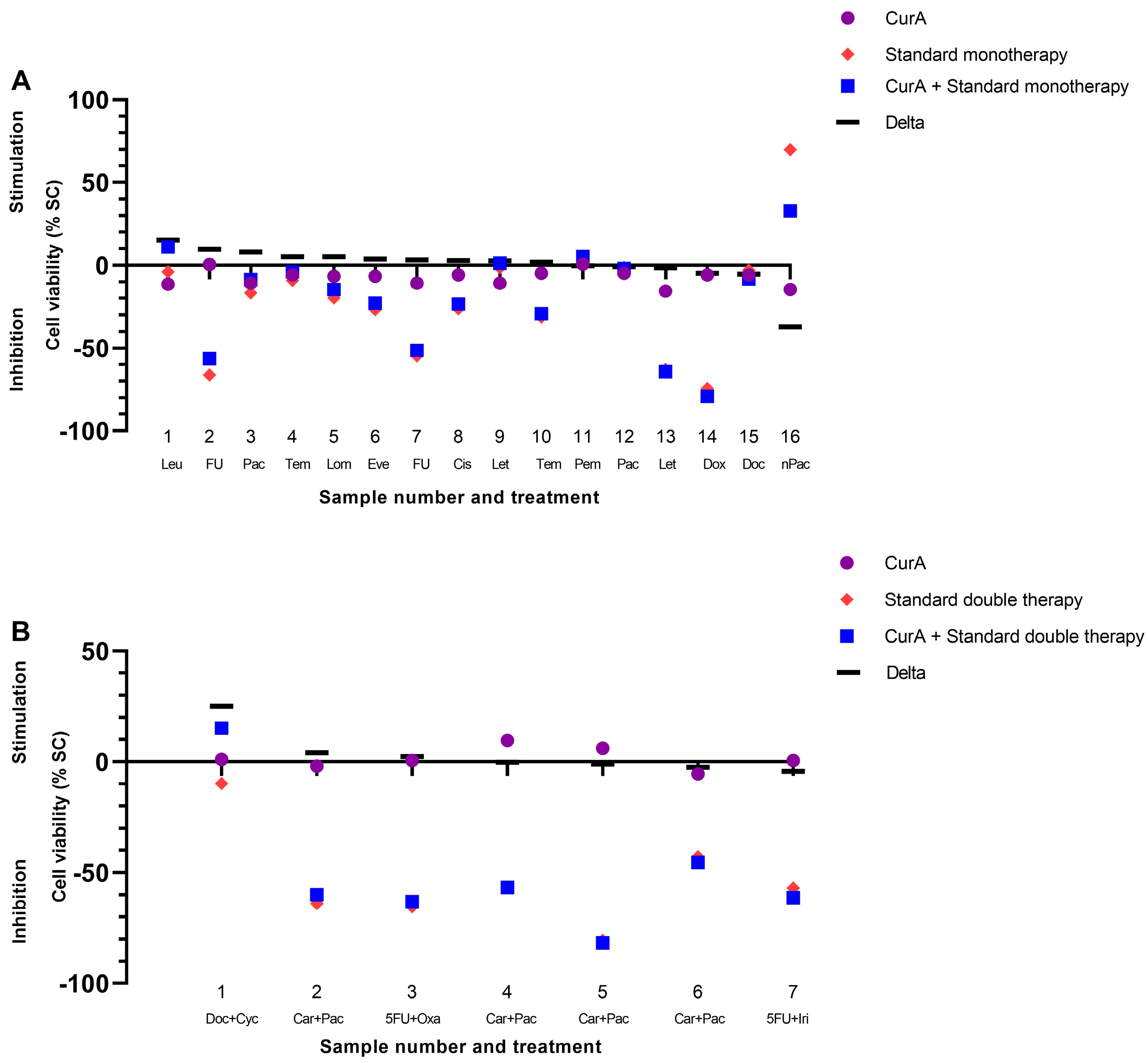
2.4. Modulation of Standard Therapy through Curcumin Formulations
2.5. Modulation of Curcumin Formulations by Other Complementary Compounds
3. Discussion
4. Materials and Methods
4.1. Patient Characteristics and Cancer Tissue
4.2. Spheroid Formation
4.3. Curcumin Formulations and Treatment
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Meaning |
| 5FU+Cis | 5-Fluorouracil+Cisplatin |
| 5FU+Iri | 5-Fluorouracil+Irinotecan |
| 5FU+Oxa | 5-Fluorouracil+Oxaliplatin |
| Art | Artesunate |
| Bic | Bicalutamide |
| Car | Carboplatin |
| Car+Pac | Carboplatin+Paclitaxel |
| Cis | Cisplatin |
| CTx | Chemotherapy |
| CTx Double | Chemo double therapy |
| CTx Mono | Chemo Monotherapy |
| Cur | Curcumin |
| CurA | Curcumin A |
| CurB | Curcumin B |
| Doc | Docetaxel |
| Doc+Cyc | Docetaxel+Cyclophosphamid |
| Doc+Pre | Docetaxel+Prednisolone |
| Double | Double Therapy |
| Dox | Doxorubicin |
| End | Endoxifen |
| Eve | Everolimus |
| FU | 5-Fluorouracil |
| Gem | Gemcitabine |
| GI | Gastrointestinal |
| Gyn. | Gynecological |
| Let | Letrozol |
| Leu | Leuprorelin |
| Lom | Lomustine |
| Mono | Monotherapy |
| N | Number of patients |
| n | Number of samples |
| nPac | Nab-Paclitaxel |
| OGJ Adenocarcinoma | Esophageal gastric junctional Adenocarcinoma |
| ORR | Objective response rate |
| OS | Overall survival |
| p | p-value |
| Pac | Paclitaxel |
| PDCS | Patient-derived cancer spheroid |
| PEG | Polyethylene Glycol |
| Pem | Pembrolizumab |
| Peme | Pemetrexed |
| PFS | Progression-free survival |
| PSA | Prostate-specific antigen |
| RCT | Randomized–controlled trial |
| Res | Resveratrol |
| SC | Solvent Control |
| SC CurA | Solvent Control Curcumin A; Cyclodextrin, Polethylene Glycol |
| SC CurB | Solvent Control Curcumin B; Kolliphor ELP, Citrate |
| Tdm | TDM-1 |
| Tem | Temozolomide |
| VitC | Vitamin C |
References
- Center for the Promotion of Imports—Netherlands Ministry of Foreign Affairs. Available online: https://www.cbi.eu/market-information/natural-ingredients-health-products/turmeric/market-potential#:~:text=The%20European%20market%20is%20promising,by%20the%20COVID%2D19%20crisis (accessed on 4 April 2024).
- Bhatia, M.; Bhalerao, M.; Cruz-Martins, N.; Kumar, D. Curcumin and cancer biology: Focusing regulatory effects in different signalling pathways. Phytother. Res. 2021, 35, 4913–4929. [Google Scholar] [CrossRef] [PubMed]
- Farghadani, R.; Naidu, R. Curcumin: Modulator of Key Molecular Signaling Pathways in Hormone-Independent Breast Cancer. Cancers 2021, 13, 3427. [Google Scholar] [CrossRef] [PubMed]
- Joshi, P.; Joshi, S.; Semwal, D.; Bisht, A.; Paliwal, S.; Dwivedi, J.; Sharma, S. Curcumin: An Insight into Molecular Pathways Involved in Anticancer Activity. Mini Rev. Med. Chem. 2021, 21, 2420–2457. [Google Scholar] [CrossRef] [PubMed]
- Zoi, V.; Kyritsis, A.P.; Galani, V.; Lazari, D.; Sioka, C.; Voulgaris, S.; Alexiou, G.A. The Role of Curcumin in Cancer: A Focus on the PI3K/Akt Pathway. Cancers 2024, 16, 1554. [Google Scholar] [CrossRef] [PubMed]
- Hidayat, Y.M.; Wagey, F.; Suardi, D.; Susanto, H.; Laihad, B.J.; Tobing, M.D.L. Analysis of curcumin as a radiosensitizer in cancer therapy with serum survivin examination: Randomised control trial. Asian Pac. J. Cancer Prev. APJCP 2021, 22, 139–143. [Google Scholar] [CrossRef] [PubMed]
- He, Z.Y.; Shi, C.B.; Wen, H.; Li, F.L.; Wang, B.L.; Wang, J. Upregulation of p53 expression in patients with colorectal cancer by administration of curcumin. Cancer Investig. 2011, 29, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.A.; Euden, S.A.; Platton, S.L.; Cooke, D.N.; Shafayat, A.; Hewitt, H.R.; Marczylo, T.H.; Morgan, B.; Hemingway, D.; Plummer, S.M.; et al. Phase I clinical trial of oral curcumin: Biomarkers of systemic activity and compliance. Clin. Cancer Res. 2004, 10, 6847–6854. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.A.; McLelland, H.R.; Hill, K.A.; Ireson, C.R.; Euden, S.A.; Manson, M.M.; Pirmohamed, M.; Marnett, L.J.; Gescher, A.J.; Steward, W.P. Pharmacodynamic and pharmacokinetic study of oral Curcuma extract in patients with colorectal cancer. Clin. Cancer Res. 2001, 7, 1894–1900. [Google Scholar] [PubMed]
- Howells, L.M.; Iwuji, C.O.; Irving, G.R.; Barber, S.; Walter, H.; Sidat, Z.; Griffin-Teall, N.; Singh, R.; Foreman, N.; Patel, S.R. Curcumin combined with FOLFOX chemotherapy is safe and tolerable in patients with metastatic colorectal cancer in a randomized phase IIa trial. J. Nutr. 2019, 149, 1133–1139. [Google Scholar] [CrossRef]
- Saghatelyan, T.; Tananyan, A.; Janoyan, N.; Tadevosyan, A.; Petrosyan, H.; Hovhannisyan, A.; Hayrapetyan, L.; Arustamyan, M.; Arnhold, J.; Rotmann, A.-R. Efficacy and safety of curcumin in combination with paclitaxel in patients with advanced, metastatic breast cancer: A comparative, randomized, double-blind, placebo-controlled clinical trial. Phytomed. Int. J. Phytother. Phytopharm. 2020, 70, 153218. [Google Scholar] [CrossRef]
- Rai, B.; Kaur, J.; Jacobs, R.; Singh, J. Possible action mechanism for curcumin in pre-cancerous lesions based on serum and salivary markers of oxidative stress. J. Oral Sci. 2010, 52, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Hsu, C.H.; Lin, J.K.; Hsu, M.M.; Ho, Y.F.; Shen, T.S.; Ko, J.Y.; Lin, J.T.; Lin, B.R.; Ming-Shiang, W.; et al. Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or pre-malignant lesions. Anticancer Res. 2001, 21, 2895–2900. [Google Scholar] [PubMed]
- Kuriakose, M.A.; Ramdas, K.; Dey, B.; Iyer, S.; Rajan, G.; Elango, K.K.; Suresh, A.; Ravindran, D.; Kumar, R.R.; Prathiba, R.; et al. A Randomized Double-Blind Placebo-Controlled Phase IIB Trial of Curcumin in Oral Leukoplakia. Cancer Prev. Res. 2016, 9, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.L.; Heckler, C.E.; Ling, M.; Katz, A.; Williams, J.P.; Pentland, A.P.; Morrow, G.R. Curcumin for radiation dermatitis: A randomized, double-blind, placebo-controlled clinical trial of thirty breast cancer patients. Radiat. Res. 2013, 180, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, V.; Ghadirian, S.; Shabani, M.; Boroumand, M.A.; Daneshvar, R.; Saghafi, F. Efficacy of curcumin for amelioration of radiotherapy-induced oral mucositis: A preliminary randomized controlled clinical trial. BMC Cancer 2023, 23, 354. [Google Scholar] [CrossRef] [PubMed]
- Delavarian, Z.; Pakfetrat, A.; Ghazi, A.; Jaafari, M.R.; Homaei Shandiz, F.; Dalirsani, Z.; Mohammadpour, A.H.; Rahimi, H.R. Oral administration of nanomicelle curcumin in the prevention of radiotherapy-induced mucositis in head and neck cancers. Spec. Care Dent. 2019, 39, 166–172. [Google Scholar] [CrossRef]
- Panahi, Y.; Saadat, A.; Beiraghdar, F.; Nouzari, S.M.H.; Jalalian, H.R.; Sahebkar, A. Antioxidant effects of bioavailability-enhanced curcuminoids in patients with solid tumors: A randomized double-blind placebo-controlled trial. J. Funct. Foods 2014, 6, 615–622. [Google Scholar] [CrossRef]
- Panahi, Y.; Saberi-Karimian, M.; Valizadeh, O.; Behnam, B.; Saadat, A.; Jamialahmadi, T.; Majeed, M.; Sahebkar, A. Effects of Curcuminoids on Systemic Inflammation and Quality of Life in Patients with Colorectal Cancer Undergoing Chemotherapy: A Randomized Controlled Trial. Adv. Exp. Med. Biol. 2021, 1328, 1–9. [Google Scholar] [CrossRef] [PubMed]
- De Waure, C.; Bertola, C.; Baccarini, G.; Chiavarini, M.; Mancuso, C. Exploring the Contribution of Curcumin to Cancer Therapy: A Systematic Review of Randomized Controlled Trials. Pharmaceutics 2023, 15, 1275. [Google Scholar] [CrossRef]
- Howells, L.; Malhotra Mukhtyar, R.; Theofanous, D.; Pepper, C.; Thomas, A.; Brown, K.; Khan, S. A Systematic Review Assessing Clinical Utility of Curcumin with a Focus on Cancer Prevention. Mol. Nutr. Food Res. 2021, 65, e2000977. [Google Scholar] [CrossRef]
- Sadeghian, M.; Rahmani, S.; Jamialahmadi, T.; Johnston, T.P.; Sahebkar, A. The effect of oral curcumin supplementation on health-related quality of life: A systematic review and meta-analysis of randomized controlled trials. J. Affect. Disord. 2021, 278, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Arslan, A.K.K.; Uzunhisarcıklı, E.; Yerer, M.B.; Bishayee, A. The golden spice curcumin in cancer: A perspective on finalized clinical trials during the last 10 years. J. Cancer Res. Ther. 2022, 18, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Hegde, M.; Girisa, S.; BharathwajChetty, B.; Vishwa, R.; Kunnumakkara, A.B. Curcumin Formulations for Better Bioavailability: What We Learned from Clinical Trials Thus Far? ACS Omega 2023, 8, 10713–10746. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, N.; Jaiswal, M. Bioavailability enhancement of curcumin via esterification processes: A review. Eur. J. Med. Chem. Rep. 2022, 6, 100081. [Google Scholar] [CrossRef]
- Idoudi, S.; Bedhiafi, T.; Hijji, Y.M.; Billa, N. Curcumin and derivatives in nanoformulations with therapeutic potential on colorectal cancer. AAPS PharmSciTech 2022, 23, 115. [Google Scholar] [CrossRef]
- Nittayananta, W.; Lerdsamran, H.; Chutiwitoonchai, N.; Promsong, A.; Srichana, T.; Netsomboon, K.; Prasertsopon, J.; Kerdto, J. A novel film spray containing curcumin inhibits SARS-CoV-2 and influenza virus infection and enhances mucosal immunity. Virol. J. 2024, 21, 26. [Google Scholar] [CrossRef]
- Ravindranathan, P.; Pasham, D.; Balaji, U.; Cardenas, J.; Gu, J.; Toden, S.; Goel, A. A combination of curcumin and oligomeric proanthocyanidins offer superior anti-tumorigenic properties in colorectal cancer. Sci. Rep. 2018, 8, 13869. [Google Scholar] [CrossRef]
- Elbadawy, M.; Hayashi, K.; Ayame, H.; Ishihara, Y.; Abugomaa, A.; Shibutani, M.; Hayashi, S.-M.; Hazama, S.; Takenouchi, H.; Nakajima, M. Anti-cancer activity of amorphous curcumin preparation in patient-derived colorectal cancer organoids. Biomed. Pharmacother. 2021, 142, 112043. [Google Scholar] [CrossRef]
- Chen, L.; Dai, Z.; Ge, C.; Huang, D.; Zhou, X.; Pan, K.; Xu, W.; Fu, J.; lin Du, J. Specific metabolic response of patient-derived organoids to curcumin of colorectal cancer. J. Chromatogr. B 2022, 1203, 123260. [Google Scholar] [CrossRef]
- Halfter, K.; Ditsch, N.; Kolberg, H.-C.; Fischer, H.; Hauzenberger, T.; von Koch, F.E.; Bauerfeind, I.; von Minckwitz, G.; Funke, I.; Crispin, A. Prospective cohort study using the breast cancer spheroid model as a predictor for response to neoadjuvant therapy—The SpheroNEO study. BMC Cancer 2015, 15, 519. [Google Scholar] [CrossRef]
- Mayer, B.; Karakhanova, S.; Bauer, N.; Liu, L.; Zhu, Y.; Philippov, P.P.; Werner, J.; Bazhin, A.V. A marginal anticancer effect of regorafenib on pancreatic carcinoma cells in vitro, ex vivo, and in vivo. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2017, 390, 1125–1134. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, O.I.; Regenauer, M.; Czogalla, B.; Brambs, C.; Burges, A.; Mayer, B. Interpatient Heterogeneity in Drug Response and Protein Biomarker Expression of Recurrent Ovarian Cancer. Cancers 2022, 14, 2279. [Google Scholar] [CrossRef]
- Hoffmann, O.I.; Ilmberger, C.; Magosch, S.; Joka, M.; Jauch, K.W.; Mayer, B. Impact of the spheroid model complexity on drug response. J. Biotechnol. 2015, 205, 14–23. [Google Scholar] [CrossRef]
- European Society for Medical Oncology. Available online: https://www.esmo.org/policy/rare-cancers-working-group/what-are-rare-cancers/definition-of-rare-cancers (accessed on 4 April 2024).
- Kiss, L.; Walter, F.R.; Bocsik, A.; Veszelka, S.; Ózsvári, B.; Puskás, L.G.; Szabó-Révész, P.; Deli, M.A. Kinetic analysis of the toxicity of pharmaceutical excipients Cremophor EL and RH40 on endothelial and epithelial cells. J. Pharm. Sci. 2013, 102, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Qiu, N.; Li, X.; Liu, J. Application of cyclodextrins in cancer treatment. J. Incl. Phenom. Macrocycl. Chem. 2017, 89, 229–246. [Google Scholar] [CrossRef]
- Liu, G.; Li, Y.; Yang, L.; Wei, Y.; Wang, X.; Wang, Z.; Tao, L. Cytotoxicity study of polyethylene glycol derivatives. RSC Adv. 2017, 7, 18252–18259. [Google Scholar] [CrossRef]
- Ilinskaya, A.N.; Clogston, J.D.; McNeil, S.E.; Dobrovolskaia, M.A. Induction of oxidative stress by Taxol® vehicle Cremophor-EL triggers production of interleukin-8 by peripheral blood mononuclear cells through the mechanism not requiring de novo synthesis of mRNA. Nanomed. Nanotechnol. Biol. Med. 2015, 11, 1925–1938. [Google Scholar] [CrossRef] [PubMed]
- Lucia Appleton, S.; Navarro-Orcajada, S.; Martínez-Navarro, F.J.; Caldera, F.; López-Nicolás, J.M.; Trotta, F.; Matencio, A. Cyclodextrins as anti-inflammatory agents: Basis, drugs and perspectives. Biomolecules 2021, 11, 1384. [Google Scholar] [CrossRef]
- Matassoli, F.L.; Leão, I.C.; Bezerra, B.B.; Pollard, R.B.; Lütjohann, D.; Hildreth, J.E.; Arruda, L.B.d. Hydroxypropyl-beta-cyclodextrin reduces inflammatory signaling from monocytes: Possible implications for suppression of HIV chronic immune activation. mSphere 2018, 3, 10–128. [Google Scholar] [CrossRef]
- Shimomura, T.; Fujiwara, H.; Ikawa, S.; Kigawa, J.; Terakawa, N. Effects of Taxol on blood cells. Lancet 1998, 352, 541–542. [Google Scholar] [CrossRef]
- Castagne, D.; Fillet, M.; Delattre, L.; Evrard, B.; Nusgens, B.; Piel, G. Study of the cholesterol extraction capacity of β-cyclodextrin and its derivatives, relationships with their effects on endothelial cell viability and on membrane models. J. Incl. Phenom. Macrocycl. Chem. 2009, 63, 225–231. [Google Scholar] [CrossRef]
- Shi, D.; Beasock, D.; Fessler, A.; Szebeni, J.; Ljubimova, J.Y.; Afonin, K.A.; Dobrovolskaia, M.A. To PEGylate or not to PEGylate: Immunological properties of nanomedicine’s most popular component, polyethylene glycol and its alternatives. Adv. Drug Deliv. Rev. 2022, 180, 114079. [Google Scholar] [CrossRef]
- Gelderblom, H.; Verweij, J.; Nooter, K.; Sparreboom, A. Cremophor EL: The drawbacks and advantages of vehicle selection for drug formulation. Eur. J. Cancer 2001, 37, 1590–1598. [Google Scholar] [CrossRef] [PubMed]
- Greil, R.; Greil-Ressler, S.; Weiss, L.; Schönlieb, C.; Magnes, T.; Radl, B.; Bolger, G.T.; Vcelar, B.; Sordillo, P.P. A phase 1 dose-escalation study on the safety, tolerability and activity of liposomal curcumin (Lipocurc™) in patients with locally advanced or metastatic cancer. Cancer Chemother. Pharmacol. 2018, 82, 695–706. [Google Scholar] [CrossRef]
- Storka, A.; Vcelar, B.; Klickovic, U.; Gouya, G.; Weisshaar, S.; Aschauer, S.; Bolger, G.; Helson, L.; Woltz, M. Safety, tolerability and pharmacokinetics of liposomal curcumin (Lipocurc™) in healthy humans. Int. J. Clin. Pharmacol. Ther. 2015, 53, 54–65. [Google Scholar] [CrossRef]
- Gilad, O.; Rosner, G.; Ivancovsky-Wajcman, D.; Zur, R.; Rosin-Arbesfeld, R.; Gluck, N.; Strul, H.; Lehavi, D.; Rolfe, V.; Kariv, R. Efficacy of Wholistic Turmeric Supplement on Adenomatous Polyps in Patients with Familial Adenomatous Polyposis—A Randomized, Double-Blinded, Placebo-Controlled Study. Genes 2022, 13, 2182. [Google Scholar] [CrossRef]
- Martínez, N.; Herrera, M.; Frías, L.; Provencio, M.; Pérez-Carrión, R.; Díaz, V.; Morse, M.; Crespo, M. A combination of hydroxytyrosol, omega-3 fatty acids and curcumin improves pain and inflammation among early stage breast cancer patients receiving adjuvant hormonal therapy: Results of a pilot study. Clin. Transl. Oncol. 2019, 21, 489–498. [Google Scholar] [CrossRef]
- Belcaro, G.; Hosoi, M.; Pellegrini, L.; Appendino, G.; Ippolito, E.; Ricci, A.; Ledda, A.; Dugall, M.; Cesarone, M.R.; Maione, C. A controlled study of a lecithinized delivery system of curcumin (Meriva®) to alleviate the adverse effects of cancer treatment. Phytother. Res. 2014, 28, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Niederreiter, M.; Klein, J.; Arndt, K.; Werner, J.; Mayer, B. Anti-Cancer Effects of Artesunate in Human 3D Tumor Models of Different Complexity. Int. J. Mol. Sci. 2023, 24, 7844. [Google Scholar] [CrossRef]
- Vernousfaderani, E.K.; Akhtari, N.; Rezaei, S.; Rezaee, Y.; Shiranirad, S.; Mashhadi, M.; Hashemi, A.; Khankandi, H.P.; Behzad, S. Resveratrol and colorectal cancer: A molecular approach to clinical researches. Curr. Top. Med. Chem. 2021, 21, 2634–2646. [Google Scholar] [CrossRef]
- Hoppe, C.; Freuding, M.; Büntzel, J.; Münstedt, K.; Hübner, J. Clinical efficacy and safety of oral and intravenous vitamin C use in patients with malignant diseases. J. Cancer Res. Clin. Oncol. 2021, 147, 3025–3042. [Google Scholar] [CrossRef]
- Gosselin, T. ONS Guidelines™ for cancer treatment-related radiodermatitis. Oncol. Nurs. Forum 2020, 47, 654–670. [Google Scholar] [CrossRef] [PubMed]
- Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften. S3-Leitlinie Komplementärmedizin in der Behandlung von onkologischen PatientInnen, Version 1.1. Available online: https://www.leitlinienprogramm-onkologie.de/fileadmin/user_upload/Downloads/Leitlinien/Komplement%C3%A4r/Version_1/LL_Komplement%C3%A4r_Langversion_1.1.pdf (accessed on 4 April 2024).
- Hwang, I.G.; Kwon, M.; Kim, J.W.; Kim, S.H.; Lee, Y.-G.; Kim, J.Y.; Koh, S.-J.; Ko, Y.H.; Shin, S.H.; Hong, S. Prevalence and predictive factors for upfront dose reduction of the first cycle of first-line chemotherapy in older adults with metastatic solid cancer: Korean cancer study group (KCSG) multicenter study. Cancers 2021, 13, 331. [Google Scholar] [CrossRef] [PubMed]
- Rosati, G.; Lonardi, S.; Galli, F.; Di Bartolomeo, M.; Ronzoni, M.; Zampino, M.G.; Banzi, M.; Zaniboni, A.; Pasini, F.; Bozzarelli, S.; et al. Oxaliplatin plus fluoropyrimidines as adjuvant therapy for colon cancer in older patients: A subgroup analysis from the TOSCA trial. Eur. J. Cancer 2021, 148, 190–201. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.H.; Han, D.H.; Kim, S.w.; Kim, M.J.; Sung, H.H.; Jeon, H.G.; Jeong, B.C.; Seo, S.I.; Jeon, S.S.; Lee, H.M. A randomized, double-blind, placebo-controlled trial to evaluate the role of curcumin in prostate cancer patients with intermittent androgen deprivation. Prostate 2019, 79, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Hejazi, J.; Rastmanesh, R.; Taleban, F.; Molana, S.; Ehtejab, G. A pilot clinical trial of radioprotective effects of curcumin supplementation in patients with prostate cancer. J. Cancer Sci. Ther. 2013, 5, 320–324. [Google Scholar]
- Passildas-Jahanmohan, J.; Eymard, J.C.; Pouget, M.; Kwiatkowski, F.; Van Praagh, I.; Savareux, L.; Atger, M.; Durando, X.; Abrial, C.; Richard, D. Multicenter randomized phase II study comparing docetaxel plus curcumin versus docetaxel plus placebo in first-line treatment of metastatic castration-resistant prostate cancer. Cancer Med. 2021, 10, 2332–2340. [Google Scholar] [CrossRef] [PubMed]
- Trimble, C.L.; Levinson, K.; Maldonado, L.; Donovan, M.J.; Clark, K.T.; Fu, J.; Shay, M.E.; Sauter, M.E.; Sanders, S.A.; Frantz, P.S.; et al. A first-in-human proof-of-concept trial of intravaginal artesunate to treat cervical intraepithelial neoplasia 2/3 (CIN2/3). Gynecol. Oncol. 2020, 157, 188–194. [Google Scholar] [CrossRef]
- Markowska, A.; Antoszczak, M.; Markowska, J.; Huczyński, A. Role of Vitamin C in Selected Malignant Neoplasms in Women. Nutrients 2022, 14, 882. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | N = 82 | |
|---|---|---|
| Biological Gender | Male | 31 |
| Female | 51 | |
| Age (years) | ||
| <40 | 6 | |
| 40–49 | 17 | |
| 50–59 | 27 | |
| 60–69 | 18 | |
| >70 | 14 | |
| Tumor entity | Gynecological Tumors | 39 |
| Breast Cancer | 33 | |
| Ovarian Cancer | 3 | |
| Cervical Cancer | 1 | |
| Vaginal Cancer | 1 | |
| Endometrial Cancer | 1 | |
| Gastrointestinal Tumors | 15 | |
| Colorectal Cancer | 8 | |
| OGJ adenocarcinoma | 2 | |
| Esophageal Cancer | 1 | |
| Gastric Cancer | 1 | |
| Appendix Neoplasia | 1 | |
| Papilla Vateri Cancer | 1 | |
| Pancreatic Cancer | 1 | |
| Rare Cancers # | 13 | |
| Sarcoma | 6 | |
| Glioblastoma | 2 | |
| Peritoneal Mesothelioma | 1 | |
| Hepatoblastoma | 1 | |
| Pleural Fibroma | 1 | |
| Pleural Mesothelioma | 1 | |
| Bladder Cancer | 1 | |
| Others | 15 | |
| Prostate Cancer | 10 | |
| Lung Cancer | 2 | |
| Melanoma | 1 | |
| Parotic Cancer | 1 | |
| Lingual Cancer | 1 | |
| Number of pre-treated standard regimens * | 0 | 32 |
| 1 | 18 | |
| >1 | 32 | |
| Tumor status | Primary tumors | 47 |
| Locally restricted | 17 | |
| Locally advanced | 7 | |
| Metastasized | 23 | |
| Recurrent tumors | 35 | |
| Locally restricted | 11 | |
| Locally advanced | 7 | |
| Metastasized | 17 |
| Subgroup Analyses | Fisher’s Exact Test p-Value | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cur Overall | CurA | CurB | Cur Overall | CurA | CurB | |||||||||
| Mean (%) | n | p-Value | Mean (%) | n | p-Value | Mean (%) | n | p-Value | ||||||
| Biological gender | Male | −8.16 | 41 | 0.58 | −9.60 | 23 | 0.36 | −6.33 | 18 | 0.63 | 0.692 | 0.29 | 0.36 | |
| Female | −8.67 | 65 | −10.26 | 39 | −6.27 | 26 | ||||||||
| Median | 58 | |||||||||||||
| Age (years) | ≤58 | −7.87 | 64 | 0.58 | −9.15 | 37 | 0.46 | −6.12 | 27 | 1.00 | 0.843 | 0.80 | 0.75 | |
| >58 | −9.38 | 42 | −11.29 | 25 | −6.58 | 17 | ||||||||
| <40 | −12.27 | 8 | −13.81 | 6 | −7.67 | 2 | ||||||||
| 40–49 | −7.23 | 23 | −8.96 | 11 | −5.64 | 12 | ||||||||
| 50–59 | −7.01 | 35 | −7.60 | 21 | −6.14 | 14 | ||||||||
| 60–69 | −8.18 | 26 | −8.63 | 16 | −7.47 | 10 | ||||||||
| >70 | −12.52 | 14 | −17.74 | 8 | −5.56 | 6 | ||||||||
| Tumor entity | Breast cancer | −9.35 | 41 | 0.51 | −11.68 | 24 | 0.32 | −6.06 | 17 | 0.58 | 0.544 | 0.12 | 0.75 | |
| Non-Breast cancer | −7.91 | 65 | −8.96 | 38 | −6.44 | 27 | ||||||||
| Breast cancer | −9.35 | 41 | −11.68 | 24 | −6.06 | 17 | ||||||||
| Other gynecological tumors * | 0.30 | 10 | −0.03 | 6 | 0.79 | 4 | ||||||||
| Gastrointestinal tumors | −8.03 | 21 | −7.07 | 12 | −9.31 | 9 | ||||||||
| Prostate cancer | −19.54 | 10 | −26.86 | 6 | −8.56 | 4 | ||||||||
| Lung cancer | −13.79 | 2 | −13.79 | 2 | x | x | ||||||||
| Melanoma | −1.30 | 2 | −1.40 | 1 | −1.20 | 1 | ||||||||
| Parotic cancer | 0.92 | 1 | 0.92 | 1 | x | x | ||||||||
| Lingual cancer | −17.47 | 1 | x | x | −17.47 | 1 | ||||||||
| Rare cancers | −5.93 | 18 | −6.62 | 10 | −5.06 | 8 | ||||||||
| Number of pre-treated standard regimens | 0 | −7.11 | 46 | 0.11 | −9.96 | 27 | 0.57 | −3.06 | 19 | 0.06 | 0.166 | 0.61 | 0.36 | |
| ≥1 | −9.51 | 60 | −10.06 | 35 | −8.76 | 25 | ||||||||
| 0 | −7.11 | 46 | −9.96 | 27 | −3.06 | 19 | ||||||||
| 1 | −10.72 | 21 | −12.41 | 16 | −5.33 | 5 | ||||||||
| > 1 | −8.86 | 39 | −8.08 | 19 | −9.61 | 20 | ||||||||
| Tumor status | Non-metasta-sized | −8.12 | 50 | 0.65 | −10.96 | 33 | 0.42 | −2.60 | 17 | 0.06 | 0.326 | 1.00 | 0.11 | |
| Metasta-sized | −8.79 | 56 | −8.93 | 29 | −8.62 | 27 | ||||||||
| Primary locally restricted | −7.70 | 20 | −12.29 | 11 | −2.08 | 9 | ||||||||
| Primary locally advanced | −12.57 | 9 | −11.96 | 8 | −17.47 | 1 | ||||||||
| Primary metastasized | −9.87 | 35 | −10.12 | 20 | −9.53 | 15 | ||||||||
| Recurrent locally restricted | −4.35 | 14 | −6.44 | 9 | −0.59 | 5 | ||||||||
| Recurrent locally advanced | −11.14 | 7 | −14.58 | 5 | −2.53 | 2 | ||||||||
| Recurrent metastasized | −6.97 | 21 | −6.29 | 9 | −7.49 | 12 | ||||||||
| Tumor Status | Tumor Infiltration into Neighbor Organs | Local Lymph Node Metastasis | Distant Metastasis |
|---|---|---|---|
| Locally restricted | -- | -- | -- |
| Locally advanced | X | -- | -- |
| -- | X | -- | |
| X | X | -- | |
| Metastasized | -- | -- | X |
| X | -- | X | |
| -- | X | X | |
| X | X | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niederreiter, M.; Klein, J.; Schmitz, S.B.M.; Werner, J.; Mayer, B. Anti-Cancer Properties of Two Intravenously Administrable Curcumin Formulations as Evaluated in the 3D Patient-Derived Cancer Spheroid Model. Int. J. Mol. Sci. 2024, 25, 8543. https://doi.org/10.3390/ijms25158543
Niederreiter M, Klein J, Schmitz SBM, Werner J, Mayer B. Anti-Cancer Properties of Two Intravenously Administrable Curcumin Formulations as Evaluated in the 3D Patient-Derived Cancer Spheroid Model. International Journal of Molecular Sciences. 2024; 25(15):8543. https://doi.org/10.3390/ijms25158543
Chicago/Turabian StyleNiederreiter, Marlene, Julia Klein, Sebastian B. M. Schmitz, Jens Werner, and Barbara Mayer. 2024. "Anti-Cancer Properties of Two Intravenously Administrable Curcumin Formulations as Evaluated in the 3D Patient-Derived Cancer Spheroid Model" International Journal of Molecular Sciences 25, no. 15: 8543. https://doi.org/10.3390/ijms25158543
APA StyleNiederreiter, M., Klein, J., Schmitz, S. B. M., Werner, J., & Mayer, B. (2024). Anti-Cancer Properties of Two Intravenously Administrable Curcumin Formulations as Evaluated in the 3D Patient-Derived Cancer Spheroid Model. International Journal of Molecular Sciences, 25(15), 8543. https://doi.org/10.3390/ijms25158543