
Dynamics of CD4+ and CD8+ Lymphocytic Inflammatory Infiltrates in Lupus Nephritis
 , , and
, , and
Abstract
1. Introduction
2. Results
2.1. Clinico-Pathological Characteristics of the Study Group
2.2. Comparative Analysis of the Clinico-Biological Profiles among the LN Classes
2.3. Specific Morphological Lesion Assessment Using Original Semi-Quantitative Scores in Lupus Nephritis Classes
2.4. Relationship among Semi-Quantitative Scores, rSLEDAI Score, and Lupus Nephritis Classes
2.5. Correlation between rSLEDAI Score and Semi-Quantitative Scores in Lupus Nephritis Classes
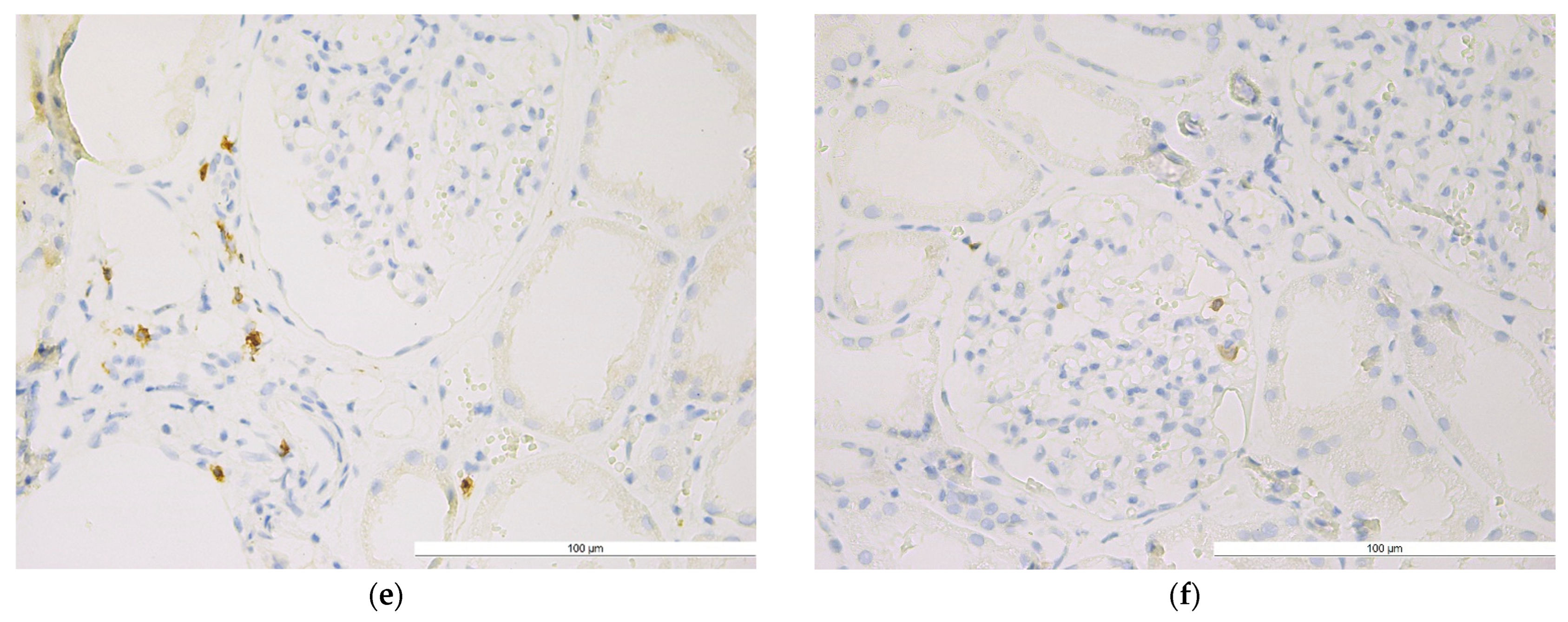
2.6. CD4+ T Lymphocytes in Lupus Nephrites Classes
2.6.1. Qualitative Evaluation
2.6.2. Quantitative Evaluation
2.6.3. Relationship between CD4+ T Lymphocytes and Semi-Quantitative Scores in Different Renal Biopsy Areas and Different Lupus Nephritis Classes
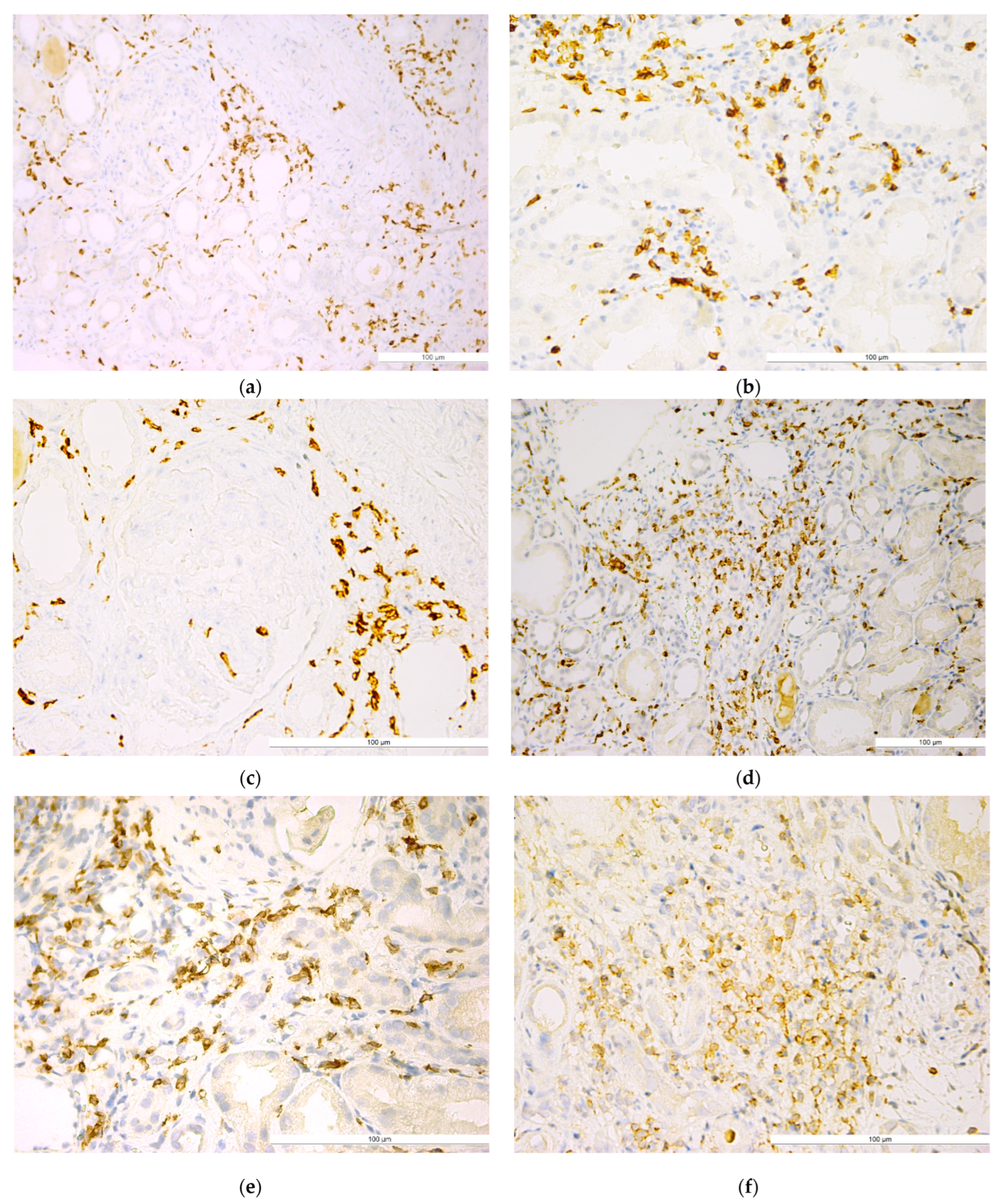
2.7. CD8+ T Lymphocytes in Lupus Nephrites Classes
2.7.1. Qualitative Evaluation
2.7.2. Quantitative Evaluation
2.7.3. Relationship between CD8+ T Lymphocytes and Semi-Quantitative Scores in Different Renal Biopsy Areas and Different Lupus Nephritis Classes
2.8. CD4+ T Versus CD8+ T Lymphocytes in Lupus Nephrites Classes
3. Discussion
4. Materials and Methods
4.1. Patients Data Collection
4.2. Histopathological Exam and Lesion Assessment Using Original Semi-Quantitative Algorithms
4.3. Immunohistochemical Exam for T Lymphocyte Assessment
4.4. T Lymphocyte Quantitative Assessment
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cervera, R.; Khamashta, M.A.; Font, J.; Sebastiani, G.D.; Gil, A.; Lavilla, P.; Mejía, J.C.; Aydintug, A.O.; Chwalinska-Sadowska, H.; de Ramón, E.; et al. European Working Party on Systemic Lupus Erythematosus. Morbidity and mortality in systemic lupus erythematosus during a 10-year period: A comparison of early and late manifestations in a cohort of 1000 patients. Medicine 2003, 82, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Portalatin, G.M.; Gebreselassie, S.K.; Bobart, S.A. Lupus nephritis—An update on disparities affecting african americans. J. Natl. Med. Assoc. 2022, 114, S34–S42. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Farinha, F.; Isenberg, D.A.; Rahman, A. Survival analysis of mortality and development of lupus nephritis in patients with systemic lupus erythematosus up to 40 years of follow-up. Rheumatology 2022, 62, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Cameron, J.S. Lupus nephritis. J. Am. Soc. Nephrol. 1999, 10, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Fulgeri, C.; Carpio, J.D.; Ardiles, L. Kidney injury in systemic lupus erythematosus: Lack of correlation between clinical and histological data. Nefrologia 2018, 38, 386–393. [Google Scholar] [CrossRef]
- Saxena, R.; Mahajan, T.; Mohan, C. Lupus nephritis: Current update. Arthritis Res. Ther. 2011, 13, 240. [Google Scholar] [CrossRef]
- Navarro, D.; Ferreira, A.C.; Viana, H.; Carvalho, F.; Nolasco, F. Morphological Indexes: Can They Predict Lupus Nephritis Outcomes? A Retrospective Study. Acta Med. Port. 2019, 32, 635–640. [Google Scholar] [CrossRef]
- Chen, P.M.; Tsokos, G.C. T Cell Abnormalities in the Pathogenesis of Systemic Lupus Erythematosus: An Update. Curr. Rheumatol. Rep. 2021, 23, 12. [Google Scholar] [CrossRef]
- Li, H.; Boulougoura, A.; Endo, Y.; Tsokos, G.C. Abnormalities of T cells in systemic lupus erythematosus: New insights in pathogenesis and therapeutic strategies. J. Autoimmun. 2022, 132, 102870. [Google Scholar] [CrossRef]
- Wągrowska-Danilewicz, M.; Danilewicz, M. Clinicopathological characteristics of segmental (IV-S) and global (IV-G) active subclasses of class IV lupus nephritis: A comparative study. Pol. J. Pathol. 2014, 65, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Podolska, M.J.; Biermann, M.H.; Maueröder, C.; Hahn, J.; Herrmann, M. Inflammatory etiopathogenesis of systemic lupus erythematosus: An update. J. Inflamm. Res. 2015, 8, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Corneth, O.B.J.; Neys, S.F.H.; Hendriks, R.W. Aberrant B Cell Signaling in Autoimmune Diseases. Cells 2022, 11, 3391. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Su, Y.; Jiao, A.; Wang, X.; Zhang, B. T cells in health and disease. Signal Transduct Target Ther. 2023, 8, 235. [Google Scholar] [CrossRef]
- Pan, L.; Lu, M.P.; Wang, J.H.; Xu, M.; Yang, S.R. Immunological pathogenesis and treatment of systemic lupus erythematosus. World J. Pediatr. 2020, 16, 19–30. [Google Scholar] [CrossRef]
- Mahajan, A.; Amelio, J.; Gairy, K.; Kaur, G.; Levy, R.A.; Roth, D.; Bass, D. Systemic lupus erythematosus, lupus nephritis and end-stage renal disease: A pragmatic review mapping disease severity and progression. Lupus 2020, 29, 1011–1020. [Google Scholar] [CrossRef]
- Wu, T.; Qin, X.; Kurepa, Z.; Kumar, K.R.; Liu, K.; Kanta, H.; Zhou, X.J.; Satterthwaite, A.B.; Davis, L.S.; Mohan, C. Shared signaling networks active in B cells isolated from genetically distinct mouse models of lupus. J. Clin. Investig. 2007, 117, 2186–2196. [Google Scholar] [CrossRef]
- Perl, A.; Fernandez, D.R.; Telarico, T.; Doherty, E.; Francis, L.; Phillips, P.E. T-cell and B-cell signaling biomarkers and treatment targets in lupus. Curr. Opin. Rheumatol. 2009, 21, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Brodie, E.J.; Infantino, S.; Low, M.S.Y.; Tarlinton, D.M. Lyn, Lupus, and (B) Lymphocytes, a Lesson on the Critical Balance of Kinase Signaling in Immunity. Front. Immunol. 2018, 9, 401. [Google Scholar] [CrossRef]
- Wen, L.; Zhang, B.; Wu, X.; Liu, R.; Fan, H.; Han, L.; Zhang, Z.; Ma, X.; Chu, C.Q.; Shi, X. Toll-like receptors 7 and 9 regulate the proliferation and differentiation of B cells in systemic lupus erythematosus. Front. Immunol. 2023, 14, 1093208. [Google Scholar] [CrossRef]
- Tilstra, J.S.; Avery, L.; Menk, A.V.; Gordon, R.A.; Smita, S.; Kane, L.P.; Chikina, M.; Delgoffe, G.M.; Shlomchik, M.J. Kidney-infiltrating T cells in murine lupus nephritis are metabolically and functionally exhausted. J. Clin. Investig. 2018, 128, 4884–4897. [Google Scholar] [CrossRef]
- Lioulios, G.; Mitsoglou, Z.; Fylaktou, A.; Xochelli, A.; Christodoulou, M.; Stai, S.; Moysidou, E.; Konstantouli, A.; Nikolaidou, V.; Papagianni, A.; et al. Exhausted but Not Senescent T Lymphocytes Predominate in Lupus Nephritis Patients. Int. J. Mol. Sci. 2022, 23, 13928. [Google Scholar] [CrossRef] [PubMed]
- Akahoshi, M.; Nakashima, H.; Tanaka, Y.; Kohsaka, T.; Nagano, S.; Ohgami, E.; Arinobu, Y.; Yamaoka, K.; Niiro, H.; Shinozaki, M.; et al. Th1/Th2 balance of peripheral T helper cells in systemic lupus erythematosus. Arthritis Rheum. 1999, 42, 1644–1648. [Google Scholar] [CrossRef]
- Koga, T.; Hedrich, C.M.; Mizui, M.; Yoshida, N.; Otomo, K.; Lieberman, L.A.; Rauen, T.; Crispín, J.C.; Tsokos, G.C. CaMK4-dependent activation of AKT/mTOR and CREM-α underlies autoimmunity-associated Th17 imbalance. J. Clin. Investig. 2014, 124, 2234–2245. [Google Scholar] [CrossRef] [PubMed]
- Katsuyama, T.; Tsokos, G.C.; Moulton, V.R. Aberrant T Cell Signaling and Subsets in Systemic Lupus Erythematosus. Front. Immunol. 2018, 9, 1088. [Google Scholar] [CrossRef] [PubMed]
- Paredes, J.L.; Fernandez-Ruiz, R.; Niewold, T.B. T Cells in Systemic Lupus Erythematosus. Rheum. Dis. Clin. N. Am. 2021, 47, 379–393. [Google Scholar] [CrossRef] [PubMed]
- Poddighe, D.; Dossybayeva, K.; Kozhakhmetov, S.; Rozenson, R.; Assylbekova, M. Double-Negative T (DNT) Cells in Patients with Systemic Lupus Erythematosus. Biomedicines 2024, 12, 166. [Google Scholar] [CrossRef]
- Castiglione, A.; Bucci, A.; Fellin, G.; d’Amico, G.; Atkins, R.C. The relationship of infiltrating renal leucocytes to disease activity in lupus and cryoglobulinaemic glomerulonephritis. Nephron 1988, 50, 14–23. [Google Scholar] [CrossRef]
- D’Agati, V.D.; Appel, G.B.; Estes, D.; Knowles, D.M., 2nd; Pirani, C.L. Monoclonal antibody identification of infiltrating mononuclear leukocytes in lupus nephritis. Kidney Int. 1986, 30, 573–581. [Google Scholar] [CrossRef]
- Alexopoulos, E.; Seron, D.; Hartley, R.B.; Cameron, J.S. Lupus nephritis: Correlation of interstitial cells with glomerular function. Kidney Int. 1990, 37, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Couzi, L.; Merville, P.; Deminière, C.; Moreau, J.F.; Combe, C.; Pellegrin, J.L.; Viallard, J.F.; Blanco, P. Predominance of CD8+ T lymphocytes among periglomerular infiltrating cells and link to the prognosis of class III and class IV lupus nephritis. Arthritis Rheum. 2007, 56, 2362–2370. [Google Scholar] [CrossRef]
- Steinmetz, O.M.; Velden, J.; Kneissler, U.; Marx, M.; Klein, A.; Helmchen, U.; Stahl, R.A.; Panzer, U. Analysis and classification of B-cell infiltrates in lupus and ANCA-associated nephritis. Kidney Int. 2008, 74, 448–457. [Google Scholar] [CrossRef]
- Chang, A.; Henderson, S.G.; Brandt, D.; Liu, N.; Guttikonda, R.; Hsieh, C.; Kaverina, N.; Utset, T.O.; Meehan, S.M.; Quigg, R.J.; et al. In situ B cell-mediated immune responses and tubulointerstitial inflammation in human lupus nephritis. J. Immunol. 2011, 186, 1849–1860. [Google Scholar] [CrossRef] [PubMed]
- Winchester, R.; Wiesendanger, M.; Zhang, H.Z.; Steshenko, V.; Peterson, K.; Geraldino-Pardilla, L.; Ruiz-Vazquez, E.; D’Agati, V. Immunologic characteristics of intrarenal T cells: Trafficking of expanded CD8+ T cell β-chain clonotypes in progressive lupus nephritis. Arthritis Rheum. 2012, 64, 1589–1600. [Google Scholar] [CrossRef]
- Saber, N.Z.; Maroof, S.H.; Soliman, D.A.; Fathi, M.S. Expression of T helper 17 cells and interleukin 17 in lupus nephritis patients. Egypt. Rheumatol. 2017, 39, 151–157. [Google Scholar] [CrossRef]
- Zampeli, E.; Klinman, D.M.; Gershwin, M.E.; Moutsopoulos, H.M. A comprehensive evaluation for the treatment of lupus nephritis. J. Autoimmun. 2017, 78, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bajema, I.M.; Wilhelmus, S.; Alpers, C.E.; Bruijn, J.A.; Colvin, R.B.; Cook, H.T.; D’Agati, V.D.; Ferrario, F.; Haas, M.; Jennette, J.C.; et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: Clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018, 93, 789–796. [Google Scholar] [CrossRef]
- Choi, S.E.; Fogo, A.B.; Lim, B.J. Histologic evaluation of activity and chronicity of lupus nephritis and its clinical significance. Kidney Res. Clin. Pract. 2023, 42, 166–173. [Google Scholar] [CrossRef]
- Muniz, M.P.R.; Brito, L.P.A.F.; Vale, P.H.C.; Guedes, F.L.; Oliveira, T.K.M.; de Araújo Brito, D.J.; Filho, N.S.; Dantas, M.; Silva, G.E.B. Renal involvement in systemic lupus erythematosus: Additional histopathological lesions. Arch. Med. Sci. 2020, 19, 1398–1409. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Zeng, Y.; Li, J.; Wang, C.; Li, W.; He, Z.; Ye, J.; Li, F.; Chen, Y.; Lin, X.; et al. Phenotypical changes and clinical significance of CD4+/CD8+ T cells in SLE. Lupus Sci. Med. 2022, 9, e000660. [Google Scholar] [CrossRef]
- Caruntu, I.D.; Azoicăi, T.; Avădănei, E.R.; Onofriescu, M.; Covic, C.A.; Giusca, S.E. Predictive value of activity and chronicity indices in lupus nephritis. Virchows Archiv. 2023, 483 (Suppl. 1), S-119. [Google Scholar]
- Grootscholten, C.; Bajema, I.M.; Florquin, S.; Steenbergen, E.J.; Peutz-Kootstra, C.J.; Goldschmeding, R.; Bijl, M.; Hagen, E.C.; van Houwelingen, H.C.; Derksen, R.H.; et al. Interobserver agreement of scoring of histopathological characteristics and classification of lupus nephritis. Nephrol. Dial. Transplant. 2008, 23, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, G.S.; D’Agati, V.D. Classification of lupus nephritis. Curr. Opin. Nephrol. Hypertens. 2009, 18, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Giannico, G.; Fogo, A.B. Lupus nephritis: Is the kidney biopsy currently necessary in the management of lupus nephritis? Clin. J. Am. Soc. Nephrol. 2013, 8, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Neumann, K.; Wallace, D.J.; Azen, C.; Nessim, S.; Fichman, M.; Metzger, A.L.; Klinenberg, J.R. Lupus in the 1980s: III. Influence of clinical variables, biopsy, and treatment on the outcome in 150 patients with lupus nephritis seen at a single center. Semin. Arthritis Rheum. 1995, 25, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Austin, H.A., 3rd; Muenz, L.R.; Joyce, K.M.; Antonovych, T.A.; Kullick, M.E.; Klippel, J.H.; Decker, J.L.; Balow, J.E. Prognostic factors in lupus nephritis. Contribution of renal histologic data. Am. J. Med. 1983, 75, 382–391. [Google Scholar] [CrossRef]
- Parichatikanond, P.; Francis, N.D.; Malasit, P.; Laohapand, T.; Nimmannit, S.; Singchoovong, L.; Nilwarangkur, S.; Chrirawong, P.; Vanichakarn, S. Lupus nephritis: Clinicopathological study of 162 cases in Thailand. J. Clin. Pathol. 1986, 39, 160–166. [Google Scholar] [CrossRef]
- Williams, W.; Sargeant, L.A.; Smikle, M.; Smith, R.; Edwards, H.; Shah, D. The outcome of lupus nephritis in Jamaican patients. Am. J. Med. Sci. 2007, 334, 426–430. [Google Scholar] [CrossRef]
- Rodriguez-Ramirez, S.; Wiegley, N.; Mejia-Vilet, J.M. Kidney Biopsy in Management of Lupus Nephritis: A Case-Based Narrative Review. Kidney Med. 2023, 6, 100772. [Google Scholar] [CrossRef]
- Blanco, P.; Pitard, V.; Viallard, J.F.; Taupin, J.L.; Pellegrin, J.L.; Moreau, J.F. Increase in activated CD8+ T lymphocytes expressing perforin and granzyme B correlates with disease activity in patients with systemic lupus erythematosus. Arthritis Rheum. 2005, 52, 201–211. [Google Scholar] [CrossRef]
- Arnold, F.; Kupferschmid, L.; Weissenborn, P.; Heldmann, L.; Hummel, J.F.; Zareba, P.; Sagar; Rogg, M.; Schell, C.; Tanriver, Y. Tissue-resident memory T cells break tolerance to renal autoantigens and orchestrate immune-mediated nephritis. Cell. Mol. Immunol. 2024, 21, 1066–1081. [Google Scholar] [CrossRef]
- Kärjä, V.; Aaltomaa, S.; Lipponen, P.; Isotalo, T.; Talja, M.; Mokka, R. Tumour-infiltrating lymphocytes: A prognostic factor of PSA-free survival in patients with local prostate carcinoma treated by radical prostatectomy. Anticancer Res. 2005, 25, 4435–4438. [Google Scholar] [PubMed]
- Bostwick, D.G.; de la Roza, G.; Dundore, P.; Corica, F.A.; Iczkowski, K.A. Intraepithelial and stromal lymphocytes in the normal human prostate. Prostate 2003, 15, 187–193. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Clinico-Pathological Characteristics | Total (n = 53) |
|---|---|
| Demographic Data | |
| Female | 44 |
| Male | 9 |
| Age (years) (mean ± SD) | 35 ± 13 |
| Paraclinical Data (mean ± SD) | |
| Urea (mg%) | 89.89 ± 69.66 |
| Creatinine (mg%) | 1.69 ± 1.79 |
| eGFR (CKD-EPI) (mL/min) | 68.18 ± 40.84 |
| Proteinuria 24 h (g/24 h) | 15.53 ± 46.97 |
| Urine Protein/Creatinine Ratio | 4.9 ± 4.75 |
| Hemoglobin (g%) | 10.15 ± 2.22 |
| Leucocyte (/mm3 × 103) | 7.24 ± 4.71 |
| Thrombocytes (/mm3 × 103) | 239.10 ± 114.67 |
| ESR (mm/2 h) | 68.27 ± 41.06 |
| Cholesterol (mg%) | 230.67 ± 79.61 |
| Triglyceride (mg%) | 199.44 ± 76.13 |
| Anti-dsDNA (IU/mL) | 209.49 ± 157.01 |
| Anti-phospholipid (IU/mL) | 16.17 ± 10.36 |
| Complement 3 (mg/dL) | 62.23 ± 26.78 |
| Renal SLEDAI Score | 11.57 ± 2.71 |
| Lupus Nephritis Classes | |
| Class II | 2 |
| Class III | 4 |
| Class IV | 19 |
| Class V | 22 |
| Class VI | 6 |
| Clinico-Biological Profile | Lupus Nephritis Classes | p Value † | |||
|---|---|---|---|---|---|
| II + III m ± SD | IV m ± SD | V m ± SD | VI m ± SD | ||
| Urea (mg%) | 41.75 ± 14.59 | 88.5 ± 78.79 | 95.33 ± 72.3 | 110 ± 44.99 | 0.495 |
| Creatinine (mg%) | 1.03 ± 0.77 | 1.2 ± 0.78 | 1.54 ± 1.36 | 4.45 ± 3.56 | 0.001 ** |
| II + III vs. VI: p = 0.044 *; IV vs. VI: p < 0.001 **; V vs. VI: p = 0.004 ** | |||||
| eGFR (CKD-EPI) mL/min | 75.01 ± 41.45 | 72.98 ± 36.24 | 74.1 ± 43.87 | 24.44 ± 14.75 | 0.046 * |
| II + III vs. VI: p = 0.018 *; IV vs. VI: p = 0.004 **; V vs. VI: p = 0.012 * | |||||
| Proteinuria (g/24 h) | 1.7 ± 1.94 | 5.43 ± 5.9 | 30.08 ± 72.33 | 12.45 ± 19.6 | 0.458 |
| UPCR | 2.86 ± 1.27 | 5.55 ± 4.57 | 5.48 ± 5.38 | 1.45 ± 1.3 | 0.372 |
| Hemoglobin g% | 12.03 ± 1.47 | 10.25 ± 2.23 | 9.84 ± 2.09 | 9.6 ± 3 | 0.317 |
| Leucocyte (/mm3 × 103) | 5.02 ± 2.39 | 8.651 ± 5.63 | 6.43 ± 3.74 | 7.62 ± 6.15 | 0.392 |
| Thrombocytes (/mm3 × 103) | 247.50 ± 108.44 | 246.64 ± 1418.11 | 217.08 ± 936.67 | 299.20 ± 103.60 | 0.537 |
| ESH (mm/2 h) | 51.8 ± 29.84 | 58.81 ± 39.29 | 82.3 ± 38.71 | 56.5 ± 62.47 | 0.232 |
| Cholesterol (mg%) | 204.2 ± 48.68 | 239.08 ± 59.06 | 243.05 ± 97.55 | 174.5 ± 50.24 | 0.376 |
| Triglyceride (mg%) | 141 ± 20.45 | 195.54 ± 58.28 | 231.84 ± 85.68 | 131.25 ± 21.7 | 0.016 * |
| II + III vs. IV: p = 0.037 *; II + III vs. V: p = 0.017 *; IV vs. VI: p = 0.016 *; V vs. VI: p = 0.009 ** | |||||
| Anti-dsDNA (IU/mL) | 118.88 ± 134.38 | 223.77 ± 129.52 | 249.98 ± 177.47 | 117.2 ± 123.8 | 0.197 |
| Anti-phospholipid (IU/mL) | 12.88 ± 10.84 | 22.3 ± 12.75 | 14.28 ± 8.26 | 0 ± 0 | 0.398 |
| Complement 3 (mg/dL) | 80.25 ± 35.56 | 54.27 ± 19.73 | 55.95 ± 21.02 | 91.25 ± 36.85 | 0.031 * |
| II + III vs. IV: p = 0.031 *; II + III vs. V: p = 0.041 *; IV vs. VI: p = 0.004 **; V vs. VI: p = 0.005 ** | |||||
| Scores | Lupus Nephritis Classes | p Value † | |||
|---|---|---|---|---|---|
| II + III m ± SD/ min ÷ max | IV m ± SD/ min ÷ max | V m ± SD/ min ÷ max | VI m ± SD/ min ÷ max | ||
| Semi-Quantitative Scores | |||||
| RC_S | 6.5 ± 2.51 3 ÷ 9 | 14.2 ± 3.28 8 ÷ 19 | 14.18 ± 6.69 5 ÷ 25 | 21 ± 0.63 20 ÷ 22 | <0.001 ** |
| II + III vs. IV: p < 0.001 **; II + III vs. V: p < 0.001 **; II + III vs. VI: p < 0.001 **; IV vs. VI: p < 0.001 **; V vs. VI: p < 0.001 ** | |||||
| TI_S | 2.66 ± 2.42 0 ÷ 7 | 5.21 ± 2.42 2 ÷ 11 | 5.68 ± 3.96 0 ÷ 13 | 11.33 ± 1.75 9 ÷ 14 | <0.001 ** |
| II + III vs. IV: p = 0.035 *; II + III vs. V: p = 0.045 *; II + III vs. VI: p < 0.001**; IV vs. VI: p < 0.001 **; V vs. VI: p < 0.001 ** | |||||
| Renal SLEDAI Score | 8.00 ± 3.162 4 ÷ 12 | 9.47 ± 2.342 5 ÷ 13 | 12.32 ± 2.147 8 ÷ 15 | 12.00 ± 2.757 8 ÷ 14 | <0.001 ** |
| II + III vs. V: p < 0.001 *; II + III vs. VI: p = 0.021 *; IV vs. V: p < 0.001 **; IV vs. VI: p = 0.037 *; | |||||
| Scores | Lupus Nephritis Classes | Total r/p | |||
|---|---|---|---|---|---|
| II + III r/p | IV r/p | V r/p | VI r/p | ||
| Renal SLEDAI score vs. RC_S | 0.781/ 0.067 | 0.356/ 0.135 | 0.172/ 0.445 | 0.688/ 0.364 | 0.361/ 0.008 ** |
| Renal SLEDAI score vs. TI_S | 0.392/ 0.443 | 0.187/ 0.442 | −0.088/ 0.696 | 0.456/ 0.364 | 0.239/ 0.085 |
| T CD4+ Lymphocytes | Lupus Nephritis Classes | p Value ‡ | |||
|---|---|---|---|---|---|
| II + III m ± SD/ min ÷ max | IV m ± SD/ min ÷ max | V m ± SD/ min ÷ max | VI m ± SD/ min ÷ max | ||
| Total | 93.33 ± 28.891 41.00 ÷ 121.00 | 110.05 ± 42.371 40.00 ÷ 192.00 | 90.32 ± 40.396 30.00 ÷ 167.00 | 207.5 ± 190.636 37.00 ÷ 496.00 | 0.432 |
| Intraglomerular | 1.5 ± 1.049 0.00 ÷ 3.00 | 3.16 ± 3.610 0.00 ÷ 12.00 | 3.77 ± 3.585 0.00 ÷ 12.00 | 1.67 ± 1.506 0.00 ÷ 4.00 | 0.439 |
| Periglomerular | 32.67 ± 10.520 17.00 ÷ 43.00 | 33.32 ± 13.115 9.00 ÷ 54.00 | 30.77 ± 14.700 12.00 ÷ 63.00 | 82.00 ± 109.148 10.00 ÷ 284.00 | 0.872 |
| Interstitial | 59.17 ± 23.626 24.00 ÷ 95.00 | 73.58 ± 35.260 12.00 ÷ 147.00 | 55.77 ± 25.547 17.00 ÷ 98.00 | 123.83 ± 92.791 27.00 ÷ 256.00 | 0.204 |
| CD4+ T Lymphocytes and Semi-Quantitative Scores | Lupus Nephritis Classes | Total rho/p | |||
|---|---|---|---|---|---|
| II + III rho/p | IV rho/p | V rho/p | VI rho/p | ||
| T CD4+ total vs. RC_S | −0.265/ 0.612 | 0.310/ 0.196 | 0.228/ 0.308 | 0.338/ 0.512 | 0.203/ 0.146 |
| T CD4+ IG vs. RC_S | 0.136/ 0.797 | 0.432/ 0.065 | 0.251/ 0.259 | 0.365/ 0.477 | 0.221/ 0.112 |
| T CD4+ PG vs. RC_S | 0.313/ 0.545 | 0.168/ 0.492 | 0.359/ 0.101 | 0.338/ 0.512 | 0.166/ 0.235 |
| T CD4+ IT vs. RC_S | −0.177/ 0.738 | 0.274/ 0.256 | 0.215/ 0.336 | 0.169/ 0.749 | 0.223/ 0.109 |
| T CD4+ total vs. TI_S | 0.406/ 0.425 | 0.140/ 0.568 | 0.169/ 0.452 | −0.290/ 0.577 | 0.127/ 0.364 |
| T CD4+ IG vs. TI_S | 0.493/ 0.321 | 0.208/ 0.393 | 0.344/ 0.117 | 0.204/ 0.699 | 0.192/ 0.168 |
| T CD4+ PG vs. TI_S | 0.397/ 0.436 | 0.239/ 0.325 | 0.134/ 0.553 | −0.058/ 0.913 | 0.064/ 0.649 |
| T CD4+ IT vs. TI_S | 0.493/ 0.321 | 0.064/ 0.796 | 0.210/ 0.347 | −0.377/ 0.461 | 0.163/ 0.244 |
| T CD8+ Lymphocytes | Lupus Nephritis Classes | p Value | |||
|---|---|---|---|---|---|
| II + III m ± SD/ min ÷ max | IV m ± SD/ min ÷ max | V m ± SD/ min ÷ max | VI m ± SD/ min ÷ max | ||
| Total | 146.33 ± 24.089 118.00 ÷ 175.00 | 481.11 ± 213.114 179.00 ÷ 870.00 | 794.86 ± 380.581 272.00 ÷ 1875.00 | 685.50 ± 358.330 81.00 ÷ 1098.00 | <0.001 **† |
| II + III vs. IV: p < 0.001 **; II + III vs. V: p < 0.001 **; IV vs. V: p = 0.013 * | |||||
| Intraglomerular | 4.67 ± 7.633 0.00 ÷ 20.00 | 15.47 ± 23.090 0.00 ÷ 102.00 | 9.27 ± 12.695 0.00 ÷ 54.00 | 10.50 ± 6.565 1.00 ÷ 18.00 | 0.157 ‡ |
| Periglomerular | 51.83 ± 21.922 18.00 ÷ 76.00 | 142.53 ± 73.972 67.00 ÷ 276.00 | 262.18 ± 131.932 115.00 ÷ 632.00 | 260.83 ± 148.829 23.00 ÷ 428.00 | <0.001 **† |
| II + III vs. IV: p < 0.001 **; II + III vs. V: p < 0.001 **; IV vs. V: p = 0.005 ** | |||||
| Interstitial | 89.83 ± 7.935 79.00 ÷ 99.00 | 323.11 ± 151.261 78.00 ÷ 586.00 | 523.41 ± 322.119 129.00 ÷ 1704.00 | 414.17 ± 207.607 57.00 ÷ 652.00 | 0.002 **† |
| II + III vs. IV: p < 0.001 **; II + III vs. V: p < 0.001 ** | |||||
| CD8+ T Lymphocytes and Semi-Quantitative Scores | Lupus Nephritis Classes | Total r/p | |||
|---|---|---|---|---|---|
| II + III r/p | IV r/p | V r/p | VI r/p | ||
| T CD8+ total vs. RC_S † | −0.618/0.191 | 0.224/0.356 | 0.625/0.002 ** | 0.169/0.749 | 0.514/<0.001 ** |
| T CD8+ IG vs. RC_S ‡ | 0.851/0.032 * | 0.150/0.540 | 0.372/0.088 | 0.257/0.623 | 0.341/0.013 * |
| T CD8+ PG vs. RC_S † | −0.883/0.020 * | 0.153/0.532 | 0.420/0.051 | 0.000/1.000 | 0.436/0.001 ** |
| T CD8+ IT vs. RC_S † | −0.530/0.280 | 0.290/0.229 | 0.717/<0.001 ** | 0.169/0.749 | 0.557/<0.001 ** |
| T CD8+ total vs. TI_S † | −0.464/0.354 | 0.416/0.077 | 0.512/0.015 * | −0.377/0.461 | 0.422/0.002 ** |
| T CD8+ IG vs. TI_S ‡ | 0.882/0.020 * | 0.131/0.594 | 0.479/0.024 * | −0.397/0.436 | 0.418/0.002 ** |
| T CD8+ PG vs. TI_S † | −0.754/0.084 | 0.208/0.392 | 0.273/0.219 | −0.485/0.329 | 0.332/0.015 * |
| T CD8+ IT vs. TI_S † | −0.522/0.288 | 0.401/0.089 | 0.502/0.017 * | −0.377/0.461 | 0.408/0.002 ** |
| Quantified Parameter | Score | ||||
|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | |
| Damage Extent | |||||
| Focal Lesions | Diffuse Lesions | ||||
| Mesangial Changes | |||||
| Hypercellularity | Absent | Low min 3 cells into one mesangial area | Moderate min 3 cells in 2 mesangial areas | Marked min 3 cells in >2 mesangial areas | |
| Matrix Proliferation | Absent | Low deposits in one mesangial area | Moderate deposits in 2 mesangial areas | Marked deposits in >2 mesangial areas | |
| Fibrinoid Necrosis | Absent | Absent | Absent | Present | |
| Sclerosis | Absent | Absent | Absent | Absent | Present |
| Glomerular Capillary Changes | |||||
| Absent | 2–3 inflammatory cells in 2 capillaries | Endocapillary hypercellularity | Capillary necrosis, hyaline trombi | Glomerular collapse | |
| Basement Membrane Changes. | |||||
| Absent | “Double contour” | “Wire loops” | Transformation into sclerosis | ||
| Segmental Sclerosis | |||||
| Absent | Present in <50% of RCs | Present in >50% of RCs | Present in >75% of RCs | ||
| Crescent | |||||
| Absent | Cellular | Fibro-cellular | Fibrillar | ||
| Global Sclerosis | |||||
| Absent | Present in <50% of RCs | Present in >50% of RCs | Present in >75% of RCs | Present in 90–100% of RCs | |
| Quantified Parameter | Score | ||||
|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | |
| Tubular Atrophy | |||||
| Absent | Mild <25% of biopsy | Moderate >25%, <50% of biopsy | Marked >50%, <75% of biopsy | Very marked >75% of biopsy | |
| Dilated Tubules | |||||
| Absent | present | ||||
| Chronic Interstitial Inflammatory Infiltrate | |||||
| Absent | Mild <25% of biopsy | Moderate >25%, <50% of biopsy | Marked >50%, <75% of biopsy | Very marked >75% of biopsy | |
| Acute Interstitial Inflammatory Infiltrate | |||||
| Absent | Present | ||||
| Interstitial Fibrosis | |||||
| Absent | Mild <25% of biopsy | Moderate >25%, <50% of biopsy | Marked >50%, <75% of biopsy | Very marked >75% of biopsy | |
| Vascular Lesions | |||||
| Absent | Fibrinoid necrosis | Intimal fibrosis | Hyalinosis | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azoicăi, T.; Avădănei, E.-R.; Giusca, S.-E.; Onofriescu, M.; Covic, A.C.; Dascalu, C.G.; Căruntu, I.-D. Dynamics of CD4+ and CD8+ Lymphocytic Inflammatory Infiltrates in Lupus Nephritis. Int. J. Mol. Sci. 2024, 25, 10775. https://doi.org/10.3390/ijms251910775
Azoicăi T, Avădănei E-R, Giusca S-E, Onofriescu M, Covic AC, Dascalu CG, Căruntu I-D. Dynamics of CD4+ and CD8+ Lymphocytic Inflammatory Infiltrates in Lupus Nephritis. International Journal of Molecular Sciences. 2024; 25(19):10775. https://doi.org/10.3390/ijms251910775
Chicago/Turabian StyleAzoicăi, Tudor, Elena-Roxana Avădănei, Simona-Eliza Giusca, Mihai Onofriescu, Adrian C. Covic, Cristina Gena Dascalu, and Irina-Draga Căruntu. 2024. "Dynamics of CD4+ and CD8+ Lymphocytic Inflammatory Infiltrates in Lupus Nephritis" International Journal of Molecular Sciences 25, no. 19: 10775. https://doi.org/10.3390/ijms251910775
APA StyleAzoicăi, T., Avădănei, E.-R., Giusca, S.-E., Onofriescu, M., Covic, A. C., Dascalu, C. G., & Căruntu, I.-D. (2024). Dynamics of CD4+ and CD8+ Lymphocytic Inflammatory Infiltrates in Lupus Nephritis. International Journal of Molecular Sciences, 25(19), 10775. https://doi.org/10.3390/ijms251910775