

Influence of Various Strontium Formulations (Ranelate, Citrate, and Chloride) on Bone Mineral Density, Morphology, and Microarchitecture: A Comparative Study in an Ovariectomized Female Mouse Model of Osteoporosis
 ,
,  ,
,  , , ,
, , ,  , , and
, , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
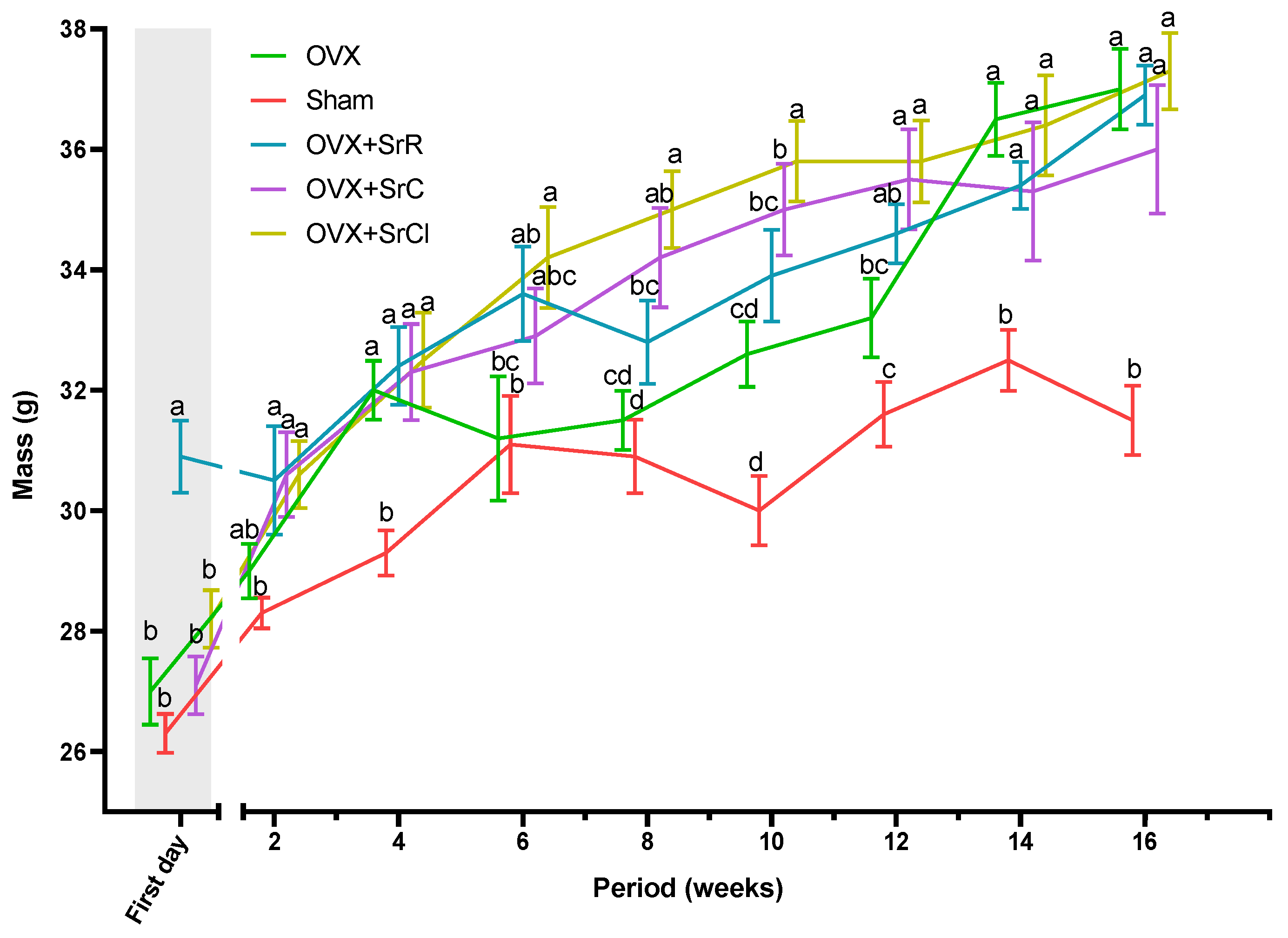
2.1. The Body Weight of the Animals
2.2. Osteometric Properties of the Femur
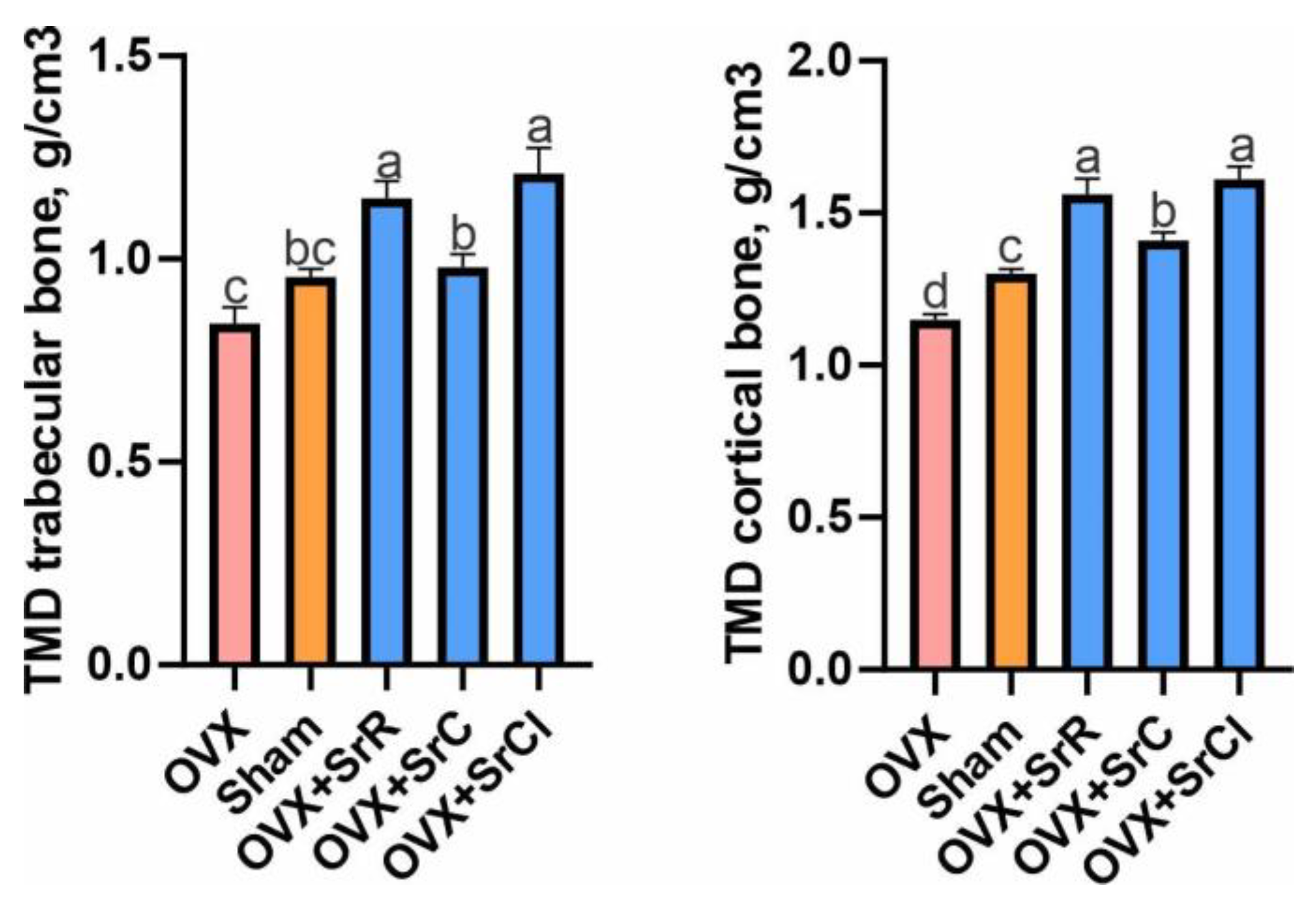
2.3. Bone Mineral Density of the Trabecular and Cortical Bones
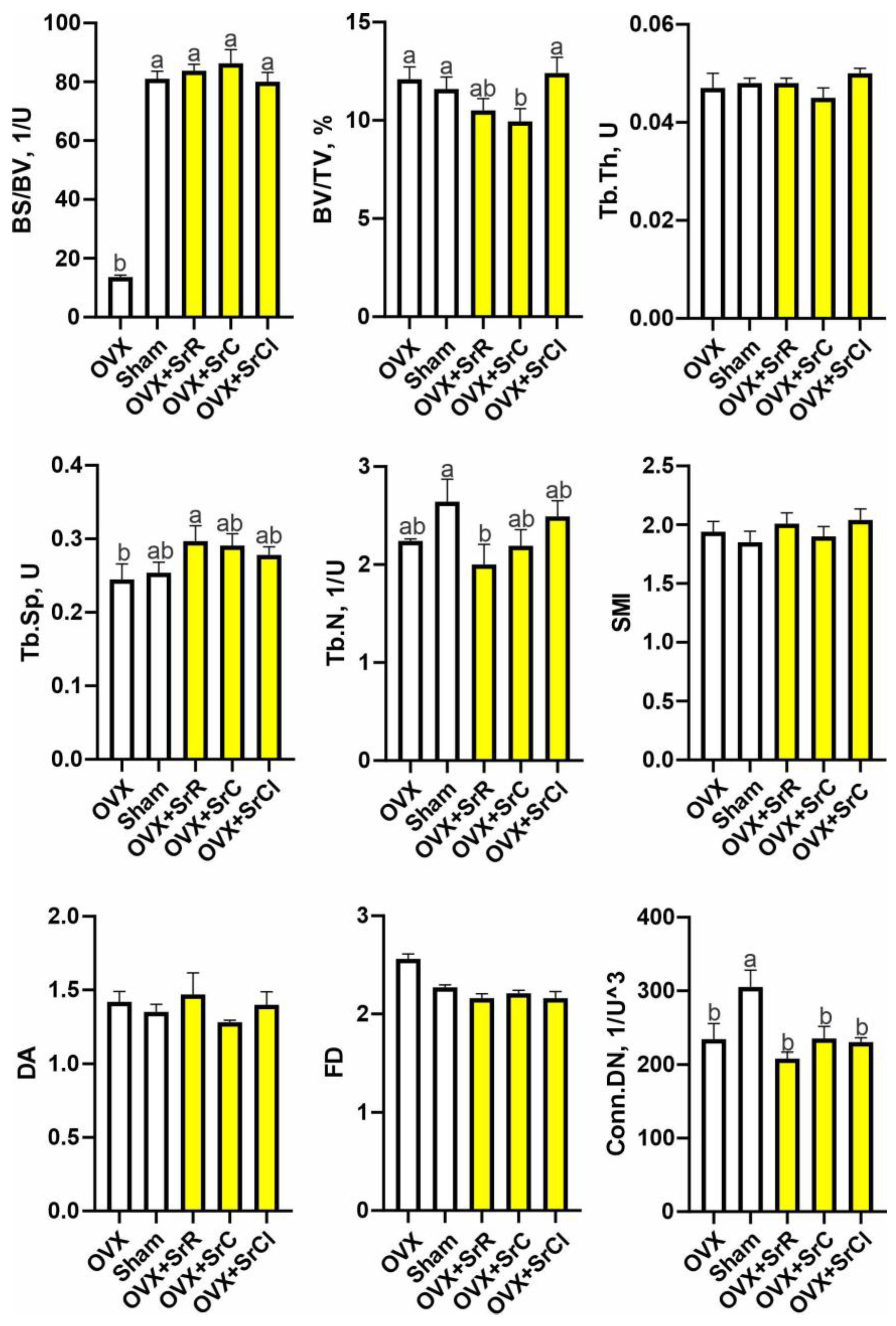
2.4. Cancellous Bone Microarchitecture
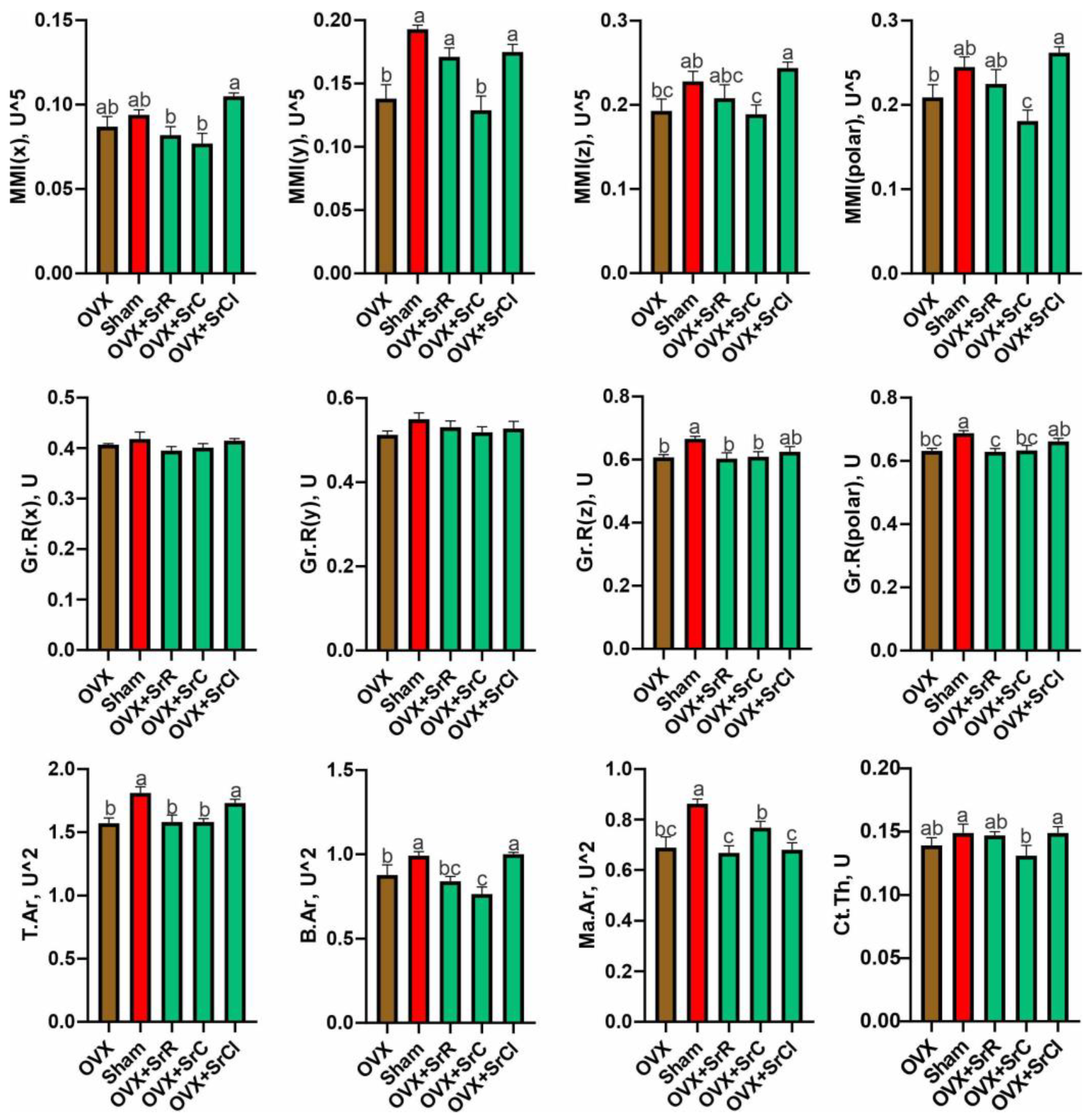
2.5. Cortical Bone Morphology
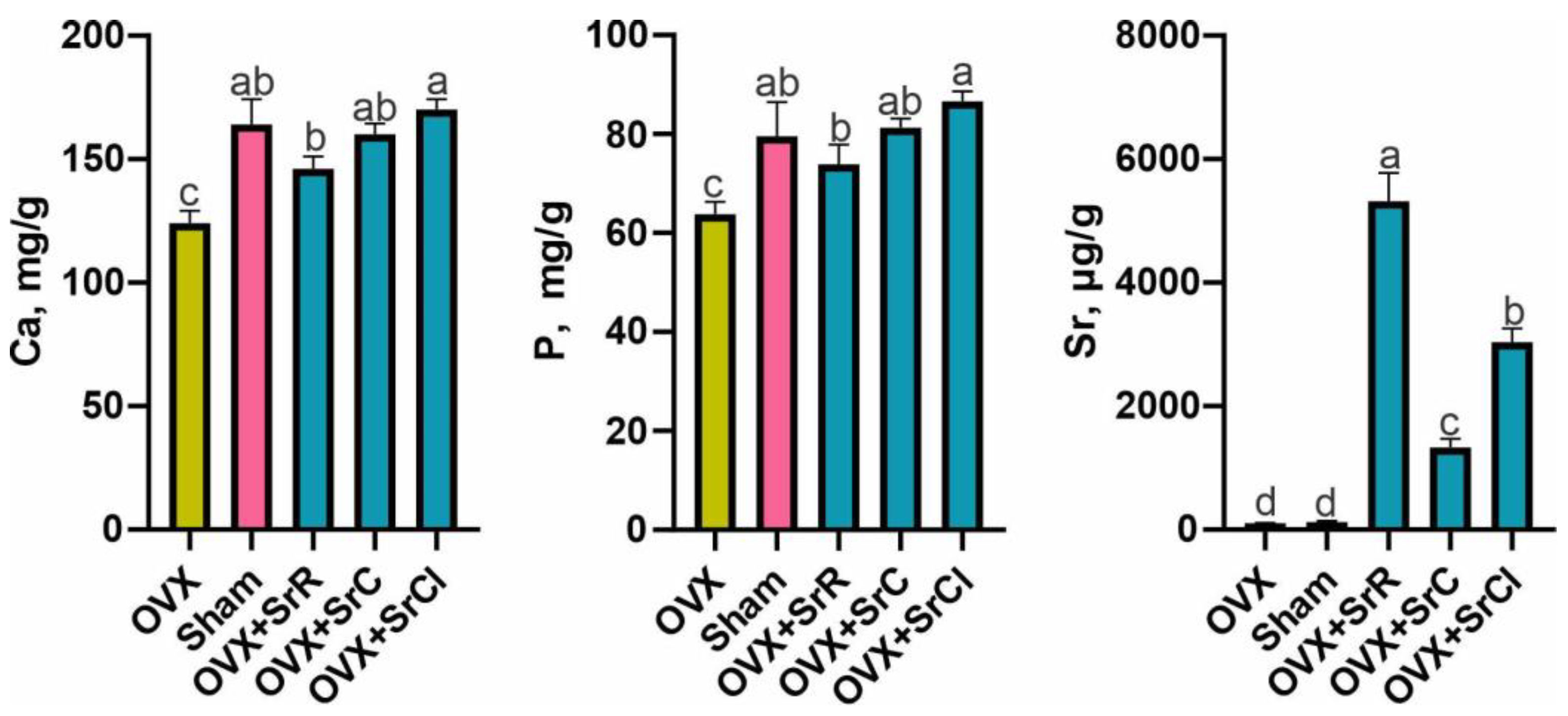
2.6. Content of Ca, P, and Sr in the Mineral Fraction of Bone Tissue
3. Discussion
4. Materials and Methods
4.1. Animals and Experimental Design
4.2. Administration of SrR, SrC, and SrCl
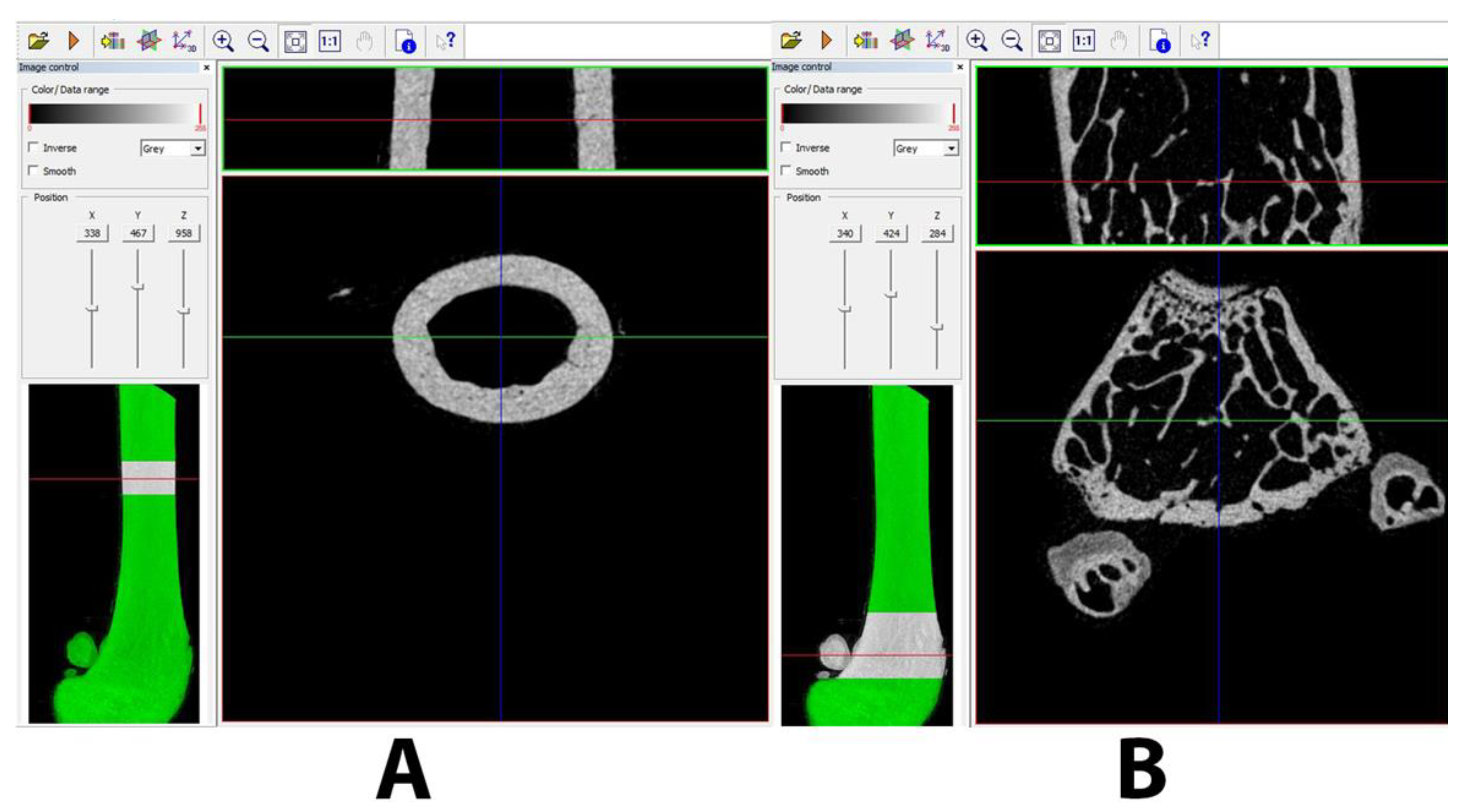
4.3. Miro-CT Analysis
4.4. Analysis of the Content of Calcium, Phosphorus, and Strontium in the Mineral Fraction of Bone Tissue
4.5. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Molino, G.; Montalbano, G.; Pontremoli, C.; Fiorilli, S.; Vitale-Brovarone, C. Imaging Techniques for the Assessment of the Bone Osteoporosis-Induced Variations with Particular Focus on Micro-CT Potential. Appl. Sci. 2020, 10, 8939. [Google Scholar] [CrossRef]
- Sozen, T.; Ozisik, L.; Calik Basaran, N. An Overview and Management of Osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Albrand, G.; Munoz, F.; Sornay-Rendu, E.; DuBoeuf, F.; Delmas, P.D. Independent Predictors of All Osteoporosis-Related Fractures in Healthy Postmenopausal Women: The OFELY Study. Bone 2003, 32, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Svedbom, A.; Hernlund, E.; Ivergård, M.; Compston, J.; Cooper, C.; Stenmark, J.; McCloskey, E.V.; Jönsson, B.; Kanis, J.A. Osteoporosis in the European Union: A Compendium of Country-Specific Reports. Arch. Osteoporos. 2013, 8, 137. [Google Scholar] [CrossRef] [PubMed]
- Raport o Osteoporozie NFZ 2019. 2019. Available online: https://Glosseniora.Pl/2019/12/10/Raport-o-Zdrowiu-Narodowego-Funduszu-Zdrowia-Poswiecony-Osteoporozie (accessed on 10 December 2019).
- Baron, R.; Tsouderos, Y. In Vitro Effects of S12911-2 on Osteoclast Function and Bone Marrow Macrophage Differentiation. Eur. J. Pharmacol. 2002, 450, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Wohl, G.R.; Chettle, D.R.; Pejović-Milić, A.; Druchok, C.; Webber, C.E.; Adachi, J.D.; Beattie, K.A. Accumulation of Bone Strontium Measured by In Vivo XRF in Rats Supplemented with Strontium Citrate and Strontium Ranelate. Bone 2013, 52, 63–69. [Google Scholar] [CrossRef]
- Moise, H.; Adachi, J.D.; Chettle, D.R.; Pejović-Milić, A. Monitoring Bone Strontium Levels of an Osteoporotic Subject due to Self-Administration of Strontium Citrate with a Novel Diagnostic Tool, In Vivo XRF: A Case Study. Bone 2012, 51, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Moise, H.; Chettle, D.R.; Pejović-Milić, A. Monitoring Bone Strontium Intake in Osteoporotic Females Self-Supplementing with Strontium Citrate with a Novel In-Vivo X-ray Fluorescence Based Diagnostic Tool. Bone 2014, 61, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Gaffney-Stomberg, E. The Impact of Trace Minerals on Bone Metabolism. Biol. Trace Elem. Res. 2019, 188, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Tohidnezhad, M.; Kubo, Y.; Lichte, P.; Heigl, T.; Roch, D.; Barahmand Pour, N.; Bergmann, C.; Sönmez, T.T.; Hock, J.V.P.; Fragoulis, A.; et al. Effects of Strontium-Doped β-Tricalcium Scaffold on Longitudinal Nuclear Factor-Kappa Beta and Vascular Endothelial Growth Factor Receptor-2 Promoter Activities during Healing in a Murine Critical-Size Bone Defect Model. Int. J. Mol. Sci. 2020, 21, 3208. [Google Scholar] [CrossRef] [PubMed]
- Strontium Ranelate Returns to UK as an Osteoporosis Drug Treatment. Available online: https://www.Osteodorset.Org.Uk/2019/02/Strontium-Ranelate-Returns-to-the-Uk-as-an-Osteoporosis-Drug-Treatment/ (accessed on 5 October 2023).
- Available online: https://www.Bruker.Com/Products/Microtomography/Academy/2016/Microct-Morphometric-Analysis.Html (accessed on 1 January 2016).
- Bouxsein, M.L.; Boyd, S.K.; Christiansen, B.A.; Guldberg, R.E.; Jepsen, K.J.; Müller, R. Guidelines for Assessment of Bone Microstructure in Rodents Using Micro–Computed Tomography. J. Bone Miner. Res. 2010, 25, 1468–1486. [Google Scholar] [CrossRef] [PubMed]
- Reginster, J.-Y.; Hiligsmann, M.; Bruyere, O. Strontium Ranelate: Long-Term Efficacy against Vertebral, Nonvertebral and Hip Fractures in Patients with Postmenopausal Osteoporosis. Ther. Adv. Musculoskelet. Dis. 2010, 2, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Delannoy, P.; Bazot, D.; Marie, P.J. Long-Term Treatment with Strontium Ranelate Increases Vertebral Bone Mass without Deleterious Effect in Mice. Metabolism 2002, 51, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Hott, M.; Deloffre, P.; Tsouderos, Y.; Marie, P.J. S12911-2 Reduces Bone Loss Induced by Short-Term Immobilization in Rats. Bone 2003, 33, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Bain, S.D.; Jerome, C.; Shen, V.; Dupin-Roger, I.; Ammann, P. Strontium Ranelate Improves Bone Strength in Ovariectomized Rat by Positively Influencing Bone Resistance Determinants. Osteoporos. Int. 2009, 20, 1417–1428. [Google Scholar] [CrossRef] [PubMed]
- Brooks, H.L.; Pollow, D.P.; Hoyer, P.B. The VCD Mouse Model of Menopause and Perimenopause for the Study of Sex Differences in Cardiovascular Disease and the Metabolic Syndrome. Physiology 2016, 31, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Kołodziejska, B.; Stępień, N.; Kolmas, J. The Influence of Strontium on Bone Tissue Metabolism and Its Application in Osteoporosis Treatment. Int. J. Mol. Sci. 2021, 22, 6564. [Google Scholar] [CrossRef] [PubMed]
- Borciani, G.; Ciapetti, G.; Vitale-Brovarone, C.; Baldini, N. Strontium Functionalization of Biomaterials for Bone Tissue Engineering Purposes: A Biological Point of View. Materials 2022, 15, 1724. [Google Scholar] [CrossRef] [PubMed]
- Grynpas, M.D.; Marie, P.J. Effects of Low Doses of Strontium on Bone Quality and Quantity in Rats. Bone 1990, 11, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Marie, P.J.; Hott, M.; Modrowski, D.; De Pollak, C.; Guillemain, J.; Deloffre, P.; Tsouderos, Y. An Uncoupling Agent Containing Strontium Prevents Bone Loss by Depressing Bone Resorption and Maintaining Bone Formation in Estrogen-Deficient Rats. J. Bone Miner. Res. 1993, 8, 607–615. [Google Scholar] [CrossRef]
- Taylor, B.A.; Bezuhly, M.; Brace, M.; Carter, M.; Hong, P. Effect of Strontium Citrate on Bone Consolidation during Mandibular Distraction Osteogenesis. Laryngoscope 2017, 127, E212–E218. [Google Scholar] [CrossRef] [PubMed]
- Mirza, F.S. Change in Bone Mineral Density with Strontium Citrate: An Illusion or Reality. J. Nutr. Health Food Sci. 2016, 4, 1–3. [Google Scholar] [CrossRef]
- Siccardi, A.J.; Padgett-Vasquez, S.; Garris, H.W.; Nagy, T.R.; D’Abramo, L.R.; Watts, S.A. Dietary Strontium Increases Bone Mineral Density in Intact Zebrafish (Danio Rerio): A Potential Model System for Bone Research. Zebrafish 2010, 7, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Ammann, P.; Shen, V.; Robin, B.; Mauras, Y.; Bonjour, J.-P.; Rizzoli, R. Strontium Ranelate Improves Bone Resistance by Increasing Bone Mass and Improving Architecture in Intact Female Rats. J. Bone Miner. Res. 2004, 19, 2012–2020. [Google Scholar] [CrossRef] [PubMed]
- Buehler, J.; Chappuis, P.; Saffar, J.L.; Tsouderos, Y.; Vignery, A. Strontium Ranelate Inhibits Bone Resorption while Maintaining Bone Formation in Alveolar Bone in Monkeys (Macaca Fascicularis). Bone 2001, 29, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.L.; Zeng, Q.Q.; Porras, L.L.; Harvey, A.; Moore, T.L.; Shelbourn, T.L.; Dalsky, G.P.; Wronski, T.J.; Aguirre, J.I.; Bryant, H.U.; et al. Teriparatide [rhPTH (1-34)], but not Strontium Ranelate, Demonstrated Bone Anabolic Efficacy in Mature, Osteopenic, Ovariectomized Rats. Endocrinology 2011, 152, 1767–1778. [Google Scholar] [CrossRef] [PubMed]
- Pei, Y.; Zheng, K.; Shang, G.; Wang, Y.; Wang, W.; Qiu, E.; Li, S.; Zhang, X. Therapeutic Effect of Strontium Ranelate on Bone in Chemotherapy-Induced Osteopenic Rats via Increased Bone Volume and Reduced Bone Loss. Biol. Trace Elem. Res. 2019, 187, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Shahnazari, M.; Sharkey, N.A.; Fosmire, G.J.; Leach, R.M. Effects of Strontium on Bone Strength, Density, Volume, and Microarchitecture in Laying Hens. J. Bone Miner. Res. 2006, 21, 1696–1703. [Google Scholar] [CrossRef] [PubMed]
- Morohashi, T.; Sano, T.; Yamada, S. Effects of Strontium on Calcium Metabolism in Rats. I. A Distinction between the Pharmacological and Toxic Doses. Jpn. J. Pharmacol. 1994, 64, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, R.K.; Allen, M.R.; Condon, K.W.; Reinwald, S.; Miller, L.M.; McClenathan, D.; Keck, B.; Phipps, R.J.; Burr, D.B. Strontium Ranelate does not Stimulate Bone Formation in Ovariectomized Rats. Osteoporos. Int. 2008, 19, 1331–1341. [Google Scholar] [CrossRef]
- Aveline, P.; Cesaro, A.; Mazor, M.; Best, T.M.; Lespessailles, E.; Toumi, H. Cumulative Effects of Strontium Ranelate and Impact Exercise on Bone Mass in Ovariectomized Rats. Int. J. Mol. Sci. 2021, 22, 3040. [Google Scholar] [CrossRef] [PubMed]
- Marie, P.J.; Hott, M. Short-Term Effects of Fluoride and Strontium on Bone Formation and Resorption in the Mouse. Metabolism 1986, 35, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Beaucage, K.L.; Pollmann, S.I.; Sims, S.M.; Dixon, S.J.; Holdsworth, D.W. Quantitative in Vivo Micro-Computed Tomography for Assessment of Age-Dependent Changes in Murine Whole-Body Composition. Bone Rep. 2016, 5, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Riggs, C.M.; Vaughan, L.C.; Evans, G.P.; Lanyon, L.E.; Boyde, A. Mechanical Implications of Collagen Fibre Orientation in Cortical Bone of the Equine Radius. Anat. Embryol. 1993, 187, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Doublier, A.; Farlay, D.; Khebbab, M.T.; Jaurand, X.; Meunier, P.J.; Boivin, G. Distribution of Strontium and Mineralization in Iliac Bone Biopsies from Osteoporotic Women Treated Long-Term with Strontium Ranelate. Eur. J. Endocrinol. 2011, 165, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Meunier, P.J.; Roux, C.; Seeman, E.; Ortolani, S.; Badurski, J.E.; Spector, T.D.; Cannata, J.; Balogh, A.; Lemmel, E.-M.; Pors-Nielsen, S.; et al. The Effects of Strontium Ranelate on the Risk of Vertebral Fracture in Women with Postmenopausal Osteoporosis. N. Engl. J. Med. 2004, 350, 459–468. [Google Scholar] [CrossRef]
- Meunier, P.J.; Slosman, D.O.; Delmas, P.D.; Sebert, J.L.; Brandi, M.L.; Albanese, C.; Lorenc, R.; Pors-Nielsen, S.; De Vernejoul, M.C.; Roces, A.; et al. Strontium Ranelate: Dose-Dependent Effects in Established Postmenopausal Vertebral Osteoporosis—A 2-Year Randomized Placebo Controlled Trial. J. Clin. Endocrinol. Metab. 2002, 87, 2060–2066. [Google Scholar] [CrossRef] [PubMed]
- Reginster, J.Y.; Neuprez, A.; Dardenne, N.; Beaudart, C.; Emonts, P.; Bruyere, O. Efficacy and Safety of Currently Marketed Anti-Osteoporosis Medications. Best Pract. Res. Clin. Endocrinol. Metab. 2014, 28, 809–834. [Google Scholar] [CrossRef] [PubMed]
- Cesareo, R.; Napolitano, C.; Iozzino, M. Strontium Ranelate in Postmenopausal Osteoporosis Treatment: A Critical Appraisal. Int. J. Womens Health 2010, 2, 1–6. [Google Scholar] [PubMed]
- Reginster, J.Y.; Seeman, E.; De Vernejoul, M.C.; Adami, S.; Compston, J.; Phenekos, C.; Devogelaer, J.P.; Curiel, M.D.; Sawicki, A.; Goemaere, S.; et al. Strontium Ranelate Reduces the Risk of Nonvertebral Fractures in Postmenopausal Women with Osteoporosis: Treatment of Peripheral Osteoporosis (TROPOS) Study. J. Clin. Endocrinol. Metab. 2005, 90, 2816–2822. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, K.J.; Silva, M.J.; Vashishth, D.; Guo, X.E.; Van Der Meulen, M.C. Establishing Biomechanical Mechanisms in Mouse Models: Practical Guidelines for Systematically Evaluating Phenotypic Changes in the Diaphyses of Long Bones. J. Bone Miner. Res. 2015, 30, 951–966. [Google Scholar] [CrossRef] [PubMed]
- Zacchetti, G.; Dayer, R.; Rizzoli, R.; Ammann, P. Systemic Treatment with Strontium Ranelate Accelerates the Filling of a Bone Defect and Improves the Material Level Properties of the Healing Bone. BioMed Res. Int. 2014, 2014, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Arlot, M.E.; Jiang, Y.; Genant, H.K.; Zhao, J.; Burt-Pichat, B.; Roux, J.-P.; Delmas, P.D.; Meunier, P.J. Histomorphometric and μCT Analysis of Bone Biopsies From Postmenopausal Osteoporotic Women Treated with Strontium Ranelate. J. Bone Miner. Res. 2008, 23, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Rizzoli, R.; Laroche, M.; Krieg, M.-A.; Frieling, I.; Thomas, T.; Delmas, P.; Felsenberg, D. Strontium Ranelate and Alendronate Have Differing Effects on Distal Tibia Bone Microstructure in Women with Osteoporosis. Rheumatol. Int. 2010, 30, 1341–1348. [Google Scholar] [CrossRef] [PubMed]
- Chavassieux, P.; Meunier, P.J.; Roux, J.P.; Portero-Muzy, N.; Pierre, M.; Chapurlat, R. Bone Histomorphometry of Transiliac Paired Bone Biopsies after 6 or 12 Months of Treatment with Oral Strontium Ranelate in 387 Osteoporotic Women: Randomized Comparison to Alendronate. J. Bone Miner. Res. 2014, 29, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Marx, D.; Rahimnejad Yazdi, A.; Papini, M.; Towler, M. A Review of the Latest Insights into the Mechanism of Action of Strontium in Bone. Bone Rep. 2020, 12, 100273. [Google Scholar] [CrossRef] [PubMed]
- Dahl, S.G.; Allain, P.; Marie, P.J.; Mauras, Y.; Boivin, G.; Ammann, P.; Tsouderos, Y.; Delmas, P.D.; Christiansen, C. Incorporation and Distribution of Strontium in Bone. Bone 2001, 28, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Pemmer, B.; Hofstaetter, J.G.; Meirer, F.; Smolek, S.; Wobrauschek, P.; Simon, R.; Fuchs, R.K.; Allen, M.R.; Condon, K.W.; Reinwald, S.; et al. Increased Strontium Uptake in Trabecular Bone of Ovariectomized Calcium-Deficient Rats Treated with Strontium Ranelate or Strontium Chloride. J. Synchrotron Radiat. 2011, 18, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Wronski, T.J.; Cintrón, M.; Dann, L.M. Temporal Relationship between Bone Loss and Increased Bone Turnover in Ovariectomized Rats. Calcif. Tissue Int. 1988, 43, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Bi, Y.N.; Zhang, P.Y.; Yuan, X.M.; Liu, Y.; Zhang, Y.; Huang, J.Y.; Zhou, K. Optimization of the Time Window of Interest in Ovariectomized Imprinting Control Region Mice for Antiosteoporosis Research. Biomed. Res. Int. 2017, 2017, 8417814. [Google Scholar] [CrossRef] [PubMed]
- Jabłoński, M.B.; Stefaniak, E.A.; Darchuk, L.; Turżańska, K.; Gorzelak, M.; Kuduk, R.; Dorriné, W.; Van Grieken, R. Microchemical investigation of bone derived from mice treated with strontium in different chemical forms using scanning electron microscopy and micro-Raman spectroscopy. Microchemical Journal. 2013, 108, 168–173. [Google Scholar] [CrossRef]
- Huang, J.; Li, Y.; Wang, L.; He, C. Combined Effects of Low-Frequency Pulsed Electromagnetic Field and Melatonin on Ovariectomy-Induced Bone Loss in Mice. Bioelectromagnetics. 2021, 42, 616–628. [Google Scholar] [CrossRef] [PubMed]
- Kruger, M.C.; Morel, P.C. Experimental Control for the Ovariectomized Rat Model: Use of Sham Versus Nonmanipulated Animal. J. Appl. Anim. Welf. Sci. 2016, 19, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Danielewicz, A.; Wójciak, M.; Sawicki, J.; Dresler, S.; Sowa, I.; Latalski, M. Comparison of Different Surgical Systems for Treatment of Early-Onset Scoliosis in the Context of Release of Titanium Ions. Spine 2021, 46, E594–E601. [Google Scholar] [CrossRef] [PubMed]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomczyk-Warunek, A.; Turżańska, K.; Posturzyńska, A.; Kowal, F.; Blicharski, T.; Pano, I.T.; Winiarska-Mieczan, A.; Nikodem, A.; Dresler, S.; Sowa, I.; et al. Influence of Various Strontium Formulations (Ranelate, Citrate, and Chloride) on Bone Mineral Density, Morphology, and Microarchitecture: A Comparative Study in an Ovariectomized Female Mouse Model of Osteoporosis. Int. J. Mol. Sci. 2024, 25, 4075. https://doi.org/10.3390/ijms25074075
Tomczyk-Warunek A, Turżańska K, Posturzyńska A, Kowal F, Blicharski T, Pano IT, Winiarska-Mieczan A, Nikodem A, Dresler S, Sowa I, et al. Influence of Various Strontium Formulations (Ranelate, Citrate, and Chloride) on Bone Mineral Density, Morphology, and Microarchitecture: A Comparative Study in an Ovariectomized Female Mouse Model of Osteoporosis. International Journal of Molecular Sciences. 2024; 25(7):4075. https://doi.org/10.3390/ijms25074075
Chicago/Turabian StyleTomczyk-Warunek, Agnieszka, Karolina Turżańska, Agnieszka Posturzyńska, Filip Kowal, Tomasz Blicharski, Inés Torné Pano, Anna Winiarska-Mieczan, Anna Nikodem, Sławomir Dresler, Ireneusz Sowa, and et al. 2024. "Influence of Various Strontium Formulations (Ranelate, Citrate, and Chloride) on Bone Mineral Density, Morphology, and Microarchitecture: A Comparative Study in an Ovariectomized Female Mouse Model of Osteoporosis" International Journal of Molecular Sciences 25, no. 7: 4075. https://doi.org/10.3390/ijms25074075
APA StyleTomczyk-Warunek, A., Turżańska, K., Posturzyńska, A., Kowal, F., Blicharski, T., Pano, I. T., Winiarska-Mieczan, A., Nikodem, A., Dresler, S., Sowa, I., Wójciak, M., & Dobrowolski, P. (2024). Influence of Various Strontium Formulations (Ranelate, Citrate, and Chloride) on Bone Mineral Density, Morphology, and Microarchitecture: A Comparative Study in an Ovariectomized Female Mouse Model of Osteoporosis. International Journal of Molecular Sciences, 25(7), 4075. https://doi.org/10.3390/ijms25074075