
Tumor and Peritoneum-Associated Macrophage Gene Signature as a Novel Molecular Biomarker in Gastric Cancer

 , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. Derivation of the Immune Cell Subset-Specific Gene Panels as Transcriptomic Signatures of GC Outcomes
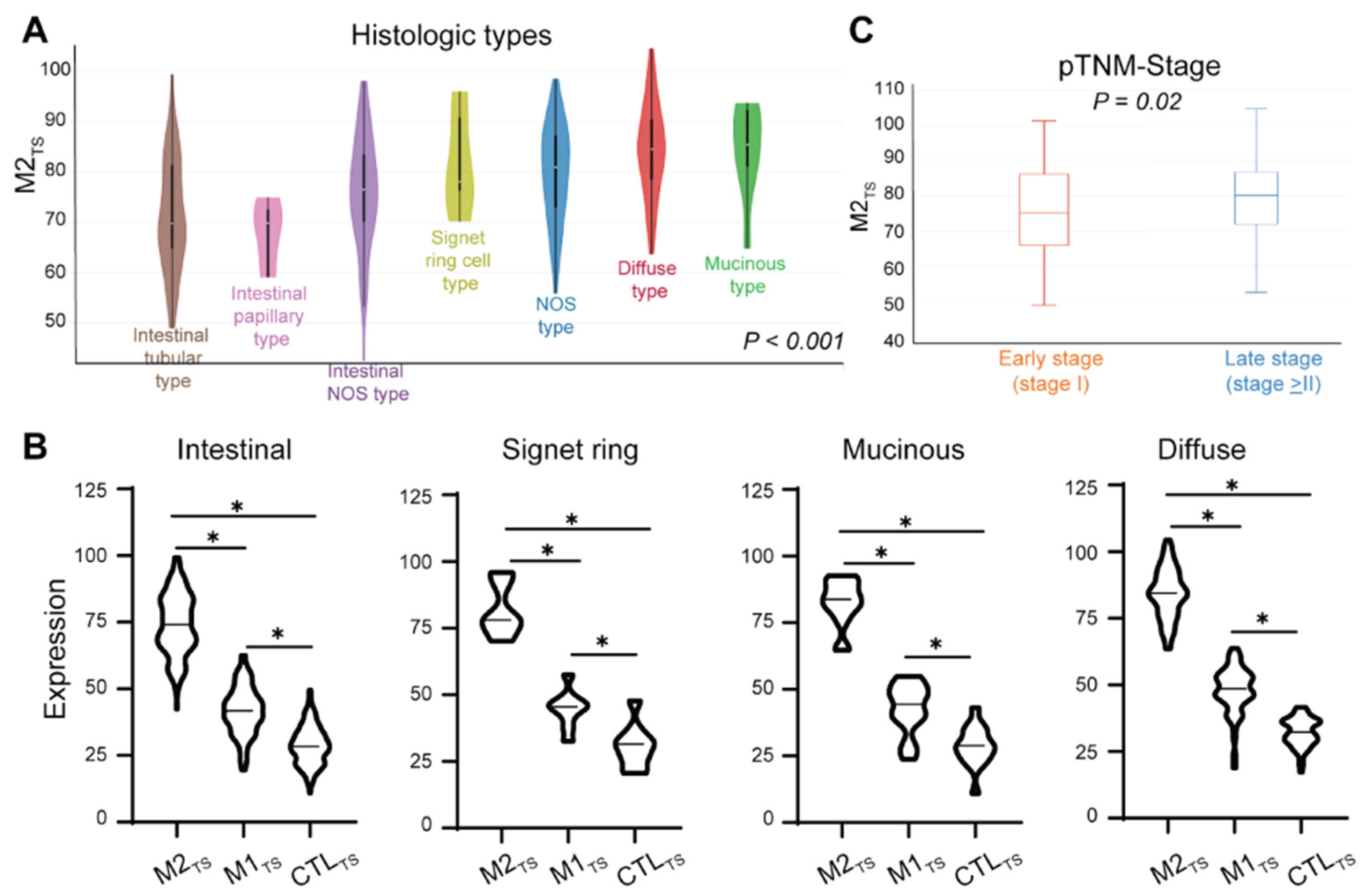
2.2. Highly Immunosuppressive M2TS Is Associated with Negative Prognostic Clinical Factors
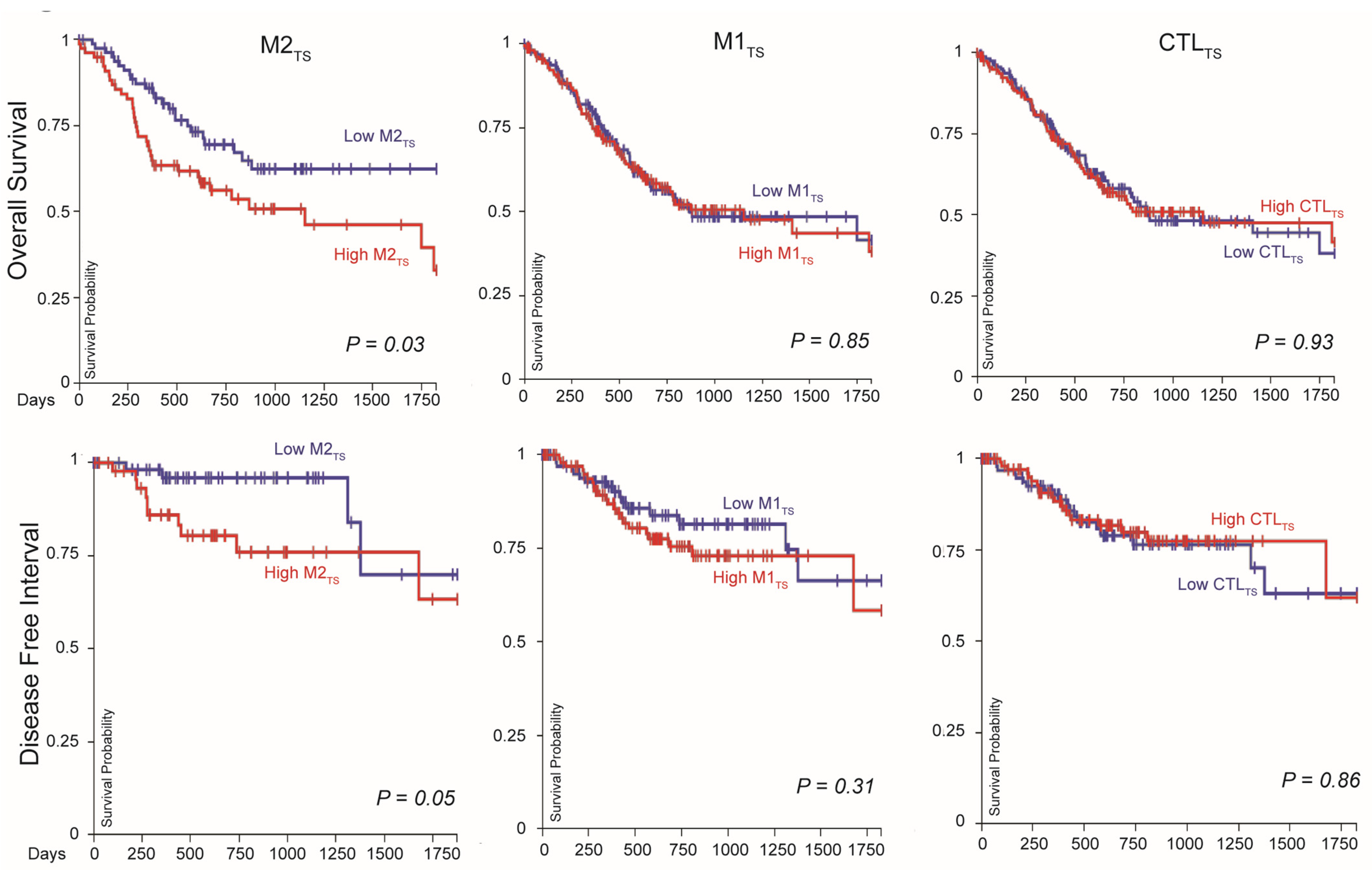
2.3. High M2TS Expression in Primary GC Is Associated with Poor Survival
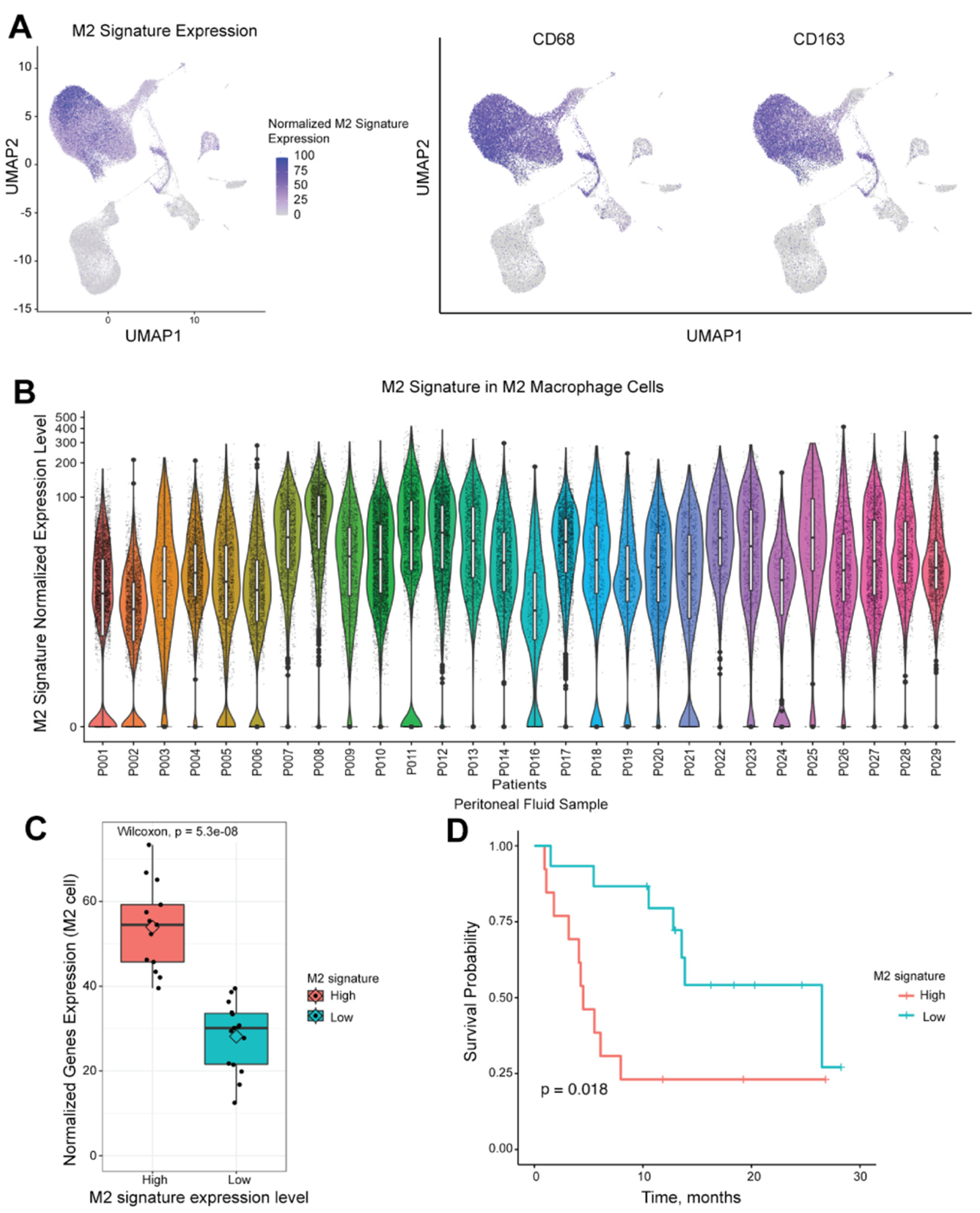
2.4. Single-Cell RNA Sequencing Demonstrates Different Populations of M2 Macrophage Polarization
2.5. M2TS in Peritoneal Macrophages Is Associated with OS in GC Patients
3. Discussion
4. Materials and Methods
4.1. The Cancer Genome Atlas (TCGA) Stomach Cancer Dataset Analysis
4.2. Prospective Cohort of Peritoneal Samples
4.3. Single-Cell RNA Sequencing
4.4. Single-Cell Type Identification
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Laversanne, M.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today (Version 1.1); International Agency for Research on Cancer: Lyon, France, 2024; Available online: https://gco.iarc.who.int/today (accessed on 14 March 2024).
- Thrift, A.P.; El-Serag, H.B. Burden of Gastric Cancer. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2020, 18, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Wada, I.; Odaira, K.; Hosoi, A.; Kobayashi, Y.; Nagaoka, K.; Karasaki, T.; Matsushita, H.; Yagi, K.; Yamashita, H.; et al. Integrative immunogenomic analysis of gastric cancer dictates novel immunological classification and the functional status of tumor-infiltrating cells. Clin. Transl. Immunol. 2020, 9, e1194. [Google Scholar] [CrossRef]
- Shitara, K.; Van Cutsem, E.; Bang, Y.J.; Fuchs, C.; Wyrwicz, L.; Lee, K.W.; Kudaba, I.; Garrido, M.; Chung, H.C.; Lee, J.; et al. Efficacy and Safety of Pembrolizumab or Pembrolizumab Plus Chemotherapy vs Chemotherapy Alone for Patients with First-line, Advanced Gastric Cancer: The KEYNOTE-062 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1571–1580. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Kawazoe, A.; Yañez, P.; Li, N.; Lonardi, S.; Kolesnik, O.; Barajas, O.; Bai, Y.; Shen, L.; Tang, Y.; et al. The KEYNOTE-811 trial of dual PD-1 and HER2 blockade in HER2-positive gastric cancer. Nature 2021, 600, 727–730. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, C.S.; Doi, T.; Jang, R.W.; Muro, K.; Satoh, T.; Machado, M.; Sun, W.; Jalal, S.I.; Shah, M.A.; Metges, J.P.; et al. Safety and Efficacy of Pembrolizumab Monotherapy in Patients with Previously Treated Advanced Gastric and Gastroesophageal Junction Cancer: Phase 2 Clinical KEYNOTE-059 Trial. JAMA Oncol. 2018, 4, e180013. [Google Scholar] [CrossRef]
- Jiang, H.; Shi, Z.; Wang, P.; Wang, C.; Yang, L.; Du, G.; Zhang, H.; Shi, B.; Jia, J.; Li, Q.; et al. Claudin18.2-Specific Chimeric Antigen Receptor Engineered T Cells for the Treatment of Gastric Cancer. J. Natl. Cancer Inst. 2019, 111, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, K.; Iwai, M.; Yajima, S.; Tanaka, M.; Yanagihara, K.; Seto, Y.; Todo, T. Efficacy of a Third-Generation Oncolytic Herpes Virus G47Δ in Advanced Stage Models of Human Gastric Cancer. Mol. Ther. Oncolytics 2020, 17, 205–215. [Google Scholar] [CrossRef]
- Zeng, D.; Zhou, R.; Yu, Y.; Luo, Y.; Zhang, J.; Sun, H.; Bin, J.; Liao, Y.; Rao, J.; Zhang, Y.; et al. Gene expression profiles for a prognostic immunoscore in gastric cancer. Br. J. Surg. 2018, 105, 1338–1348. [Google Scholar] [CrossRef]
- Kim, T.S.; da Silva, E.; Coit, D.G.; Tang, L.H. Intratumoral Immune Response to Gastric Cancer Varies by Molecular and Histologic Subtype. Am. J. Surg. Pathol. 2019, 43, 851–860. [Google Scholar] [CrossRef]
- Wu, M.; Wang, Y.; Liu, H.; Song, J.; Ding, J. Genomic analysis and clinical implications of immune cell infiltration in gastric cancer. Biosci. Rep. 2020, 40, BSR20193308. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, X.; Shen, Z.; Xu, J.; Qin, J.; Sun, Y. Infiltration of diametrically polarized macrophages predicts overall survival of patients with gastric cancer after surgical resection. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2015, 18, 740–750. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Fushida, S.; Yamamoto, Y.; Tsukada, T.; Kinoshita, J.; Oyama, K.; Miyashita, T.; Tajima, H.; Ninomiya, I.; Munesue, S.; et al. Tumor-associated macrophages of the M2 phenotype contribute to progression in gastric cancer with peritoneal dissemination. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2016, 19, 1052–1065. [Google Scholar] [CrossRef] [PubMed]
- Yin, S.; Huang, J.; Li, Z.; Zhang, J.; Luo, J.; Lu, C.; Xu, H.; Xu, H. The Prognostic and Clinicopathological Significance of Tumor-Associated Macrophages in Patients with Gastric Cancer: A Meta-Analysis. PLoS ONE 2017, 12, e0170042. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Pan, Y.; Ma, J.; Kang, Z.; Xu, X.; Zhu, Y.; Chen, J.; Zhang, W.; Chang, W.; Zhu, J. Prognostic significance of the infiltration of CD163(+) macrophages combined with CD66b(+) neutrophils in gastric cancer. Cancer Med. 2018, 7, 1731–1741. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, S.; Kagawa, S.; Kuwada, K.; Ito, A.; Kajioka, H.; Kakiuchi, Y.; Watanabe, M.; Kagawa, T.; Yoshida, R.; Kikuchi, S.; et al. Intraperitoneal cancer-immune microenvironment promotes peritoneal dissemination of gastric cancer. Oncoimmunology 2019, 8, e1671760. [Google Scholar] [CrossRef] [PubMed]
- Boutilier, A.J.; Elsawa, S.F. Macrophage Polarization States in the Tumor Microenvironment. Int. J. Mol. Sci. 2021, 22, 6995. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.J. Macrophage Polarization. Annu. Rev. Physiol. 2017, 79, 541–566. [Google Scholar] [CrossRef] [PubMed]
- Guerriero, J.L. Macrophages: The Road Less Traveled, Changing Anticancer Therapy. Trends Mol. Med. 2018, 24, 472–489. [Google Scholar] [CrossRef]
- Barros, M.H.; Hauck, F.; Dreyer, J.H.; Kempkes, B.; Niedobitek, G. Macrophage polarisation: An immunohistochemical approach for identifying M1 and M2 macrophages. PLoS ONE 2013, 8, e80908. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.J.; Allen, J.E.; Biswas, S.K.; Fisher, E.A.; Gilroy, D.W.; Goerdt, S.; Gordon, S.; Hamilton, J.A.; Ivashkiv, L.B.; Lawrence, T.; et al. Macrophage activation and polarization: Nomenclature and experimental guidelines. Immunity 2014, 41, 14–20. [Google Scholar] [CrossRef]
- Martinez, F.O.; Gordon, S.; Locati, M.; Mantovani, A. Transcriptional Profiling of the Human Monocyte-to-Macrophage Differentiation and Polarization: New Molecules and Patterns of Gene Expression. J. Immunol. 2006, 177, 7303–7311. [Google Scholar] [CrossRef] [PubMed]
- Orecchioni, M.; Ghosheh, Y.; Pramod, A.B.; Ley, K. Macrophage Polarization: Different Gene Signatures in M1(LPS+) vs. Classically and M2(LPS−) vs. Alternatively Activated Macrophages. Front. Immunol. 2019, 10, 1084. [Google Scholar] [CrossRef] [PubMed]
- Badylak, S.F.; Valentin, J.E.; Ravindra, A.K.; McCabe, G.P.; Stewart-Akers, A.M. Macrophage phenotype as a determinant of biologic scaffold remodeling. Tissue Eng. Part A 2008, 14, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Buscher, K.; Ehinger, E.; Gupta, P.; Pramod, A.B.; Wolf, D.; Tweet, G.; Pan, C.; Mills, C.D.; Lusis, A.J.; Ley, K. Natural variation of macrophage activation as disease-relevant phenotype predictive of inflammation and cancer survival. Nat. Commun. 2017, 8, 16041. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Zhou, S.; Chen, C.; Wang, Z.; Xu, W.; Zhang, J.; Wei, S.; Yang, J.; Chen, H. CCL19: A novel prognostic chemokine modulates the tumor immune microenvironment and outcomes of cancers. Aging 2023, 15, 12369–12387. [Google Scholar] [CrossRef] [PubMed]
- Correale, P.; Rotundo, M.S.; Botta, C.; Del Vecchio, M.T.; Ginanneschi, C.; Licchetta, A.; Conca, R.; Apollinari, S.; De Luca, F.; Tassone, P.; et al. Tumor infiltration by T lymphocytes expressing chemokine receptor 7 (CCR7) is predictive of favorable outcome in patients with advanced colorectal carcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2012, 18, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wang, Y.; Zhao, Y.; Liu, T.; Wang, Z.; Zhang, N.; Dai, Z.; Wu, W.; Cao, H.; Feng, S.; et al. PTX3 mediates the infiltration, migration, and inflammation-resolving-polarization of macrophages in glioblastoma. CNS Neurosci. Ther. 2022, 28, 1748–1766. [Google Scholar] [CrossRef] [PubMed]
- Rőszer, T. Understanding the Mysterious M2 Macrophage through Activation Markers and Effector Mechanisms. Mediat. Inflamm. 2015, 2015, 816460. [Google Scholar] [CrossRef] [PubMed]
- Väyrynen, J.P.; Haruki, K.; Lau, M.C.; Väyrynen, S.A.; Zhong, R.; Dias Costa, A.; Borowsky, J.; Zhao, M.; Fujiyoshi, K.; Arima, K.; et al. The Prognostic Role of Macrophage Polarization in the Colorectal Cancer Microenvironment. Cancer Immunol. Res. 2021, 9, 8–19. [Google Scholar] [CrossRef]
- Li, Y.; Shen, Z.; Chai, Z.; Zhan, Y.; Zhang, Y.; Liu, Z.; Liu, Y.; Li, Z.; Lin, M.; Zhang, Z.; et al. Targeting MS4A4A on tumour-associated macrophages restores CD8+ T-cell-mediated antitumour immunity. Gut 2023, 72, 2307–2320. [Google Scholar] [CrossRef]
- Sanyal, R.; Polyak, M.J.; Zuccolo, J.; Puri, M.; Deng, L.; Roberts, L.; Zuba, A.; Storek, J.; Luider, J.M.; Sundberg, E.M.; et al. MS4A4A: A novel cell surface marker for M2 macrophages and plasma cells. Immunol. Cell Biol. 2017, 95, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Qin, H.; Li, Y.; Xiao, A.; Zheng, E.; Zeng, H.; Su, C.; Luo, X.; Lu, Q.; Liao, M.; et al. CD36-mediated metabolic crosstalk between tumor cells and macrophages affects liver metastasis. Nat. Commun. 2022, 13, 5782. [Google Scholar] [CrossRef] [PubMed]
- Su, P.; Wang, Q.; Bi, E.; Ma, X.; Liu, L.; Yang, M.; Qian, J.; Yi, Q. Enhanced Lipid Accumulation and Metabolism Are Required for the Differentiation and Activation of Tumor-Associated Macrophages. Cancer Res. 2020, 80, 1438–1450. [Google Scholar] [CrossRef] [PubMed]
- Su, C.; Jia, S.; Ma, Z.; Zhang, H.; Wei, L.; Liu, H. HMGB1 Promotes Lymphangiogenesis through the Activation of RAGE on M2 Macrophages in Laryngeal Squamous Cell Carcinoma. Dis. Markers 2022, 2022, 4487435. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Yang, S.; Ma, J.; Chen, Z.; Song, G.; Rao, D.; Cheng, Y.; Huang, S.; Liu, Y.; Jiang, S.; et al. Spatiotemporal Immune Landscape of Colorectal Cancer Liver Metastasis at Single-Cell Level. Cancer Discov. 2022, 12, 134–153. [Google Scholar] [CrossRef] [PubMed]
- Korbecki, J.; Grochans, S.; Gutowska, I.; Barczak, K.; Baranowska-Bosiacka, I. CC Chemokines in a Tumor: A Review of Pro-Cancer and Anti-Cancer Properties of Receptors CCR5, CCR6, CCR7, CCR8, CCR9, and CCR10 Ligands. Int. J. Mol. Sci. 2020, 21, 7619. [Google Scholar] [CrossRef] [PubMed]
- Kamat, K.; Krishnan, V.; Dorigo, O. Macrophage-derived CCL23 upregulates expression of T-cell exhaustion markers in ovarian cancer. Br. J. Cancer 2022, 127, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, V.; Tallapragada, S.; Schaar, B.; Kamat, K.; Chanana, A.M.; Zhang, Y.; Patel, S.; Parkash, V.; Rinker-Schaeffer, C.; Folkins, A.K.; et al. Omental macrophages secrete chemokine ligands that promote ovarian cancer colonization of the omentum via CCR1. Commun. Biol. 2020, 3, 524. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Li, Y.; Zhang, A.Z.; Jiang, C.H.; Li, F.P.; Xie, Y.F.; Li, J.F.; Liang, W.H.; Zhang, H.J.; Liu, C.X.; et al. Tumor-associated macrophage polarization promotes the progression of esophageal carcinoma. Aging 2020, 13, 2049–2072. [Google Scholar] [CrossRef]
- Yan, J.; Kong, L.Y.; Hu, J.; Gabrusiewicz, K.; Dibra, D.; Xia, X.; Heimberger, A.B.; Li, S. FGL2 as a Multimodality Regulator of Tumor-Mediated Immune Suppression and Therapeutic Target in Gliomas. J. Natl. Cancer Inst. 2015, 107, djv137. [Google Scholar] [CrossRef]
- Ajani, J.A.; D’Amico, T.A.; Bentrem, D.J.; Chao, J.; Cooke, D.; Corvera, C.; Das, P.; Enzinger, P.C.; Enzler, T.; Fanta, P.; et al. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN 2022, 20, 167–192. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Liu, H.; Zhang, J.; Wang, Z.; Yang, S.; Liu, D.; Liu, J.; Li, Y.; Fu, X.; Zhang, X. Fibronectin-1: A Predictive Immunotherapy Response Biomarker for Muscle-Invasive Bladder Cancer. Arch. Esp. Urol. 2023, 76, 70–83. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Sohn, B.H.; Hwang, J.E.; Jang, H.J.; Lee, H.S.; Oh, S.C.; Shim, J.J.; Lee, K.W.; Kim, E.H.; Yim, S.Y.; Lee, S.H.; et al. Clinical Significance of Four Molecular Subtypes of Gastric Cancer Identified by the Cancer Genome Atlas Project. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2017, 23, 4441–4449. [Google Scholar] [CrossRef]
- Wu, M.H.; Lee, W.J.; Hua, K.T.; Kuo, M.L.; Lin, M.T. Macrophage Infiltration Induces Gastric Cancer Invasiveness by Activating the β-Catenin Pathway. PLoS ONE 2015, 10, e0134122. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Sung, J.Y.; Lee, J.; Park, Y.K.; Kim, Y.W.; Kim, G.Y.; Won, K.Y.; Lim, S.J. Polarized CD163+ tumor-associated macrophages are associated with increased angiogenesis and CXCL12 expression in gastric cancer. Clin. Res. Hepatol. Gastroenterol. 2016, 40, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.D.; Jiang, X.; Sullivan, K.M.; Jalikis, F.G.; Smythe, K.S.; Abbasi, A.; Vignali, M.; Park, J.O.; Daniel, S.K.; Pollack, S.M.; et al. Mobilization of CD8(+) T Cells via CXCR4 Blockade Facilitates PD-1 Checkpoint Therapy in Human Pancreatic Cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2019, 25, 3934–3945. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.-X.; Zhang, S.-X.; Wu, H.-J.; Rong, X.-L.; Guo, J. M2b macrophage polarization and its roles in diseases. J. Leukoc. Biol. 2019, 106, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Dang, M.; Harada, K.; Han, G.; Wang, F.; Pool Pizzi, M.; Zhao, M.; Tatlonghari, G.; Zhang, S.; Hao, D.; et al. Single-cell dissection of intratumoral heterogeneity and lineage diversity in metastatic gastric adenocarcinoma. Nat. Med. 2021, 27, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Song, S.; Harada, K.; Ghazanfari Amlashi, F.; Badgwell, B.; Pizzi, M.P.; Xu, Y.; Zhao, W.; Dong, X.; Jin, J.; et al. Multiplex profiling of peritoneal metastases from gastric adenocarcinoma identified novel targets and molecular subtypes that predict treatment response. Gut 2020, 69, 18–31. [Google Scholar] [CrossRef]
- Pyonteck, S.M.; Akkari, L.; Schuhmacher, A.J.; Bowman, R.L.; Sevenich, L.; Quail, D.F.; Olson, O.C.; Quick, M.L.; Huse, J.T.; Teijeiro, V.; et al. CSF-1R inhibition alters macrophage polarization and blocks glioma progression. Nat. Med. 2013, 19, 1264–1272. [Google Scholar] [CrossRef]
- Zhu, Y.; Yang, J.; Xu, D.; Gao, X.-M.; Zhang, Z.; Hsu, J.L.; Li, C.-W.; Lim, S.-O.; Sheng, Y.-Y.; Zhang, Y.; et al. Disruption of tumour-associated macrophage trafficking by the osteopontin-induced colony-stimulating factor-1 signalling sensitises hepatocellular carcinoma to anti-PD-L1 blockade. Gut 2019, 68, 1653–1666. [Google Scholar] [CrossRef]
- Fujiwara, T.; Yakoub, M.A.; Chandler, A.; Christ, A.B.; Yang, G.; Ouerfelli, O.; Rajasekhar, V.K.; Yoshida, A.; Kondo, H.; Hata, T.; et al. CSF1/CSF1R Signaling Inhibitor Pexidartinib (PLX3397) Reprograms Tumor-Associated Macrophages and Stimulates T-cell Infiltration in the Sarcoma Microenvironment. Mol. Cancer Ther. 2021, 20, 1388–1399. [Google Scholar] [CrossRef]
- Tap, W.D.; Gelderblom, H.; Palmerini, E.; Desai, J.; Bauer, S.; Blay, J.Y.; Alcindor, T.; Ganjoo, K.; Martín-Broto, J.; Ryan, C.W.; et al. Pexidartinib versus placebo for advanced tenosynovial giant cell tumour (ENLIVEN): A randomised phase 3 trial. Lancet 2019, 394, 478–487. [Google Scholar] [CrossRef]
- Weiss, S.A.; Djureinovic, D.; Jessel, S.; Krykbaeva, I.; Zhang, L.; Jilaveanu, L.; Ralabate, A.; Johnson, B.; Levit, N.S.; Anderson, G.; et al. A Phase I Study of APX005M and Cabiralizumab with or without Nivolumab in Patients with Melanoma, Kidney Cancer, or Non-Small Cell Lung Cancer Resistant to Anti-PD-1/PD-L1. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2021, 27, 4757–4767. [Google Scholar] [CrossRef]
- Pienta, K.J.; Machiels, J.-P.; Schrijvers, D.; Alekseev, B.; Shkolnik, M.; Crabb, S.J.; Li, S.; Seetharam, S.; Puchalski, T.A.; Takimoto, C.; et al. Phase 2 study of carlumab (CNTO 888), a human monoclonal antibody against CC-chemokine ligand 2 (CCL2), in metastatic castration-resistant prostate cancer. Investig. New Drugs 2013, 31, 760–768. [Google Scholar] [CrossRef]
- Advani, R.; Flinn, I.; Popplewell, L.; Forero, A.; Bartlett, N.L.; Ghosh, N.; Kline, J.; Roschewski, M.; LaCasce, A.; Collins, G.P.; et al. CD47 Blockade by Hu5F9-G4 and Rituximab in Non-Hodgkin’s Lymphoma. N. Engl. J. Med. 2018, 379, 1711–1721. [Google Scholar] [CrossRef]
- Sikic, B.I.; Lakhani, N.; Patnaik, A.; Shah, S.A.; Chandana, S.R.; Rasco, D.; Colevas, A.D.; O’Rourke, T.; Narayanan, S.; Papadopoulos, K.; et al. First-in-Human, First-in-Class Phase I Trial of the Anti-CD47 Antibody Hu5F9-G4 in Patients With Advanced Cancers. J. Clin. Oncol. 2019, 37, 946–953. [Google Scholar] [CrossRef]
- Oyarce, C.; Vizcaino-Castro, A.; Chen, S.; Boerma, A.; Daemen, T. Re-polarization of immunosuppressive macrophages to tumor-cytotoxic macrophages by repurposed metabolic drugs. Oncoimmunology 2021, 10, 1898753. [Google Scholar] [CrossRef]
- Nishida-Aoki, N.; Gujral, T.S. Polypharmacologic Reprogramming of Tumor-Associated Macrophages toward an Inflammatory Phenotype. Cancer Res. 2022, 82, 433–446. [Google Scholar] [CrossRef]
- Jaynes, J.M.; Sable, R.; Ronzetti, M.; Bautista, W.; Knotts, Z.; Abisoye-Ogunniyan, A.; Li, D.; Calvo, R.; Dashnyam, M.; Singh, A.; et al. Mannose receptor (CD206) activation in tumor-associated macrophages enhances adaptive and innate antitumor immune responses. Sci. Transl. Med. 2020, 12, eaax6337. [Google Scholar] [CrossRef]
- Goldman, M.J.; Craft, B.; Hastie, M.; Repečka, K.; McDade, F.; Kamath, A.; Banerjee, A.; Luo, Y.; Rogers, D.; Brooks, A.N.; et al. Visualizing and interpreting cancer genomics data via the Xena platform. Nat. Biotechnol. 2020, 38, 675–678. [Google Scholar] [CrossRef]
- Stuart, T.; Butler, A.; Hoffman, P.; Hafemeister, C.; Papalexi, E.; Mauck, W.M., 3rd; Hao, Y.; Stoeckius, M.; Smibert, P.; Satija, R. Comprehensive Integration of Single-Cell Data. Cell 2019, 177, 1888–1902.e1821. [Google Scholar] [CrossRef]
- Budczies, J.; Klauschen, F.; Sinn, B.V.; Győrffy, B.; Schmitt, W.D.; Darb-Esfahani, S.; Denkert, C. Cutoff Finder: A comprehensive and straightforward Web application enabling rapid biomarker cutoff optimization. PLoS ONE 2012, 7, e51862. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| M2TS Expression | p-Value | |||
|---|---|---|---|---|
| Low n = 15 (%) | High n = 13 (%) | |||
| Age (years) | ≤40 | 6 (40.0) | 1 (7.7) | 0.086 |
| >40 and ≤65 | 4 (26.7) | 8 (61.5) | ||
| >65 | 5 (33.3) | 4 (30.8) | ||
| Age (years) | Mean ± SD | 51.7 ± 20.2 | 60.7 ± 13.6 | 0.184 |
| Gender | Female | 9 (60.0) | 4 (33.3) | 0.322 |
| Male | 6 (40.0) | 8 (66.7) | ||
| Ethnicity | Asian | 5 (33.3) | 4 (30.8) | 0.288 |
| Black | 1 (6.7) | 0 (0.0) | ||
| Hispanic | 6 (40.0) | 3 (23.1) | ||
| Non-Hispanic White | 2 (13.3) | 6 (46.2) | ||
| Other | 1 (6.7) | 0 (0.0) | ||
| Cytology | Negative | 6 (40.0) | 4 (30.8) | 0.91 |
| Positive | 9 (60.0) | 9 (69.2) | ||
| Lauren Classification | Diffuse | 11 (73.3) | 10 (76.9) | 1.0 |
| Intestinal | 4 (26.7) | 3 (23.1) | ||
| Differentiation | Moderately | 0 (0.0) | 2 (15.4) | 0.144 |
| Poorly | 15 (100.0) | 10 (76.9) | ||
| Well to moderately | 0 (0.0) | 1 (7.7) | ||
| Signet Ring Cell | Absent | 5 (33.3) | 8 (61.5) | 0.266 |
| Present | 10 (66.7) | 5 (38.5) | ||
| Microsatellite Status | MSI high | 1 (6.7) | 0 (0.0) | 0.55 |
| MSS | 12 (80.0) | 12 (92.3) | ||
| Unknown | 2 (13.3) | 1 (7.7) | ||
| PD-L1 | Negative | 4 (26.7) | 5 (38.5) | 0.52 |
| Positive | 10 (66.7) | 6 (46.2) | ||
| Unknown | 1 (6.7) | 2 (15.4) | ||
| Stage | I–III | 2 (13.3) | 2 (15.4) | 1.0 |
| IV | 13 (86.7) | 11 (84.6) | ||
| Serum Albumin | <3 g/dL | 4 (26.7) | 5 (38.5) | 0.794 |
| ≥3 g/dL | 11 (73.3) | 8 (61.5) | ||
| Patients (%) | HR (95% CI, p-Value) | ||
|---|---|---|---|
| M2TS Expression | Low | 15 (53.6) | ref |
| High | 13 (46.4) | 3.14 (1.17–8.46, 0.02) | |
| Age (years) | ≤40 | 7 (25.0) | ref |
| >40 and ≤65 | 12 (42.9) | 3.67 (0.79–17.05, 0.097) | |
| >65 | 9 (32.1) | 2.51 (0.50–12.53, 0.26) | |
| Age (years) | Mean ± SD | 55.9 ± 17.7 | 1.01 (0.99–1.04, 0.33) |
| Gender | Female | 13 (48.1) | ref |
| Male | 14 (51.9) | 0.96 (0.36–2.57, 0.93) | |
| Ethnicity | Asian | 9 (32.1) | ref |
| Black | 1 (3.6) | 3.21 (0.35–29.23, 0.30) | |
| Hispanic | 9 (32.1) | 0.93 (0.25–3.49, 0.92) | |
| Non-Hispanic White | 8 (28.6) | 1.76 (0.53–5.79, 0.35) | |
| Other | 1 (3.6) | 0.00 (0.00–Inf, 1.0) | |
| Resection | No | 17 (60.7) | ref |
| Yes | 11 (39.3) | 2.31 (0.89–6.02, 0.09) | |
| Stage | I-III | 4 (14.3) | ref |
| IV | 24 (85.7) | 5.53 (0.69–44.07, 0.106) | |
| Lauren Classification | Diffuse | 21 (75.0) | ref |
| Intestinal | 7 (25.0) | 1.53 (0.56–4.18, 0.40) | |
| Differentiation | Moderately | 2 (7.1) | ref |
| Poorly | 25 (89.3) | 0.23 (0.05–1.09, 0.06) | |
| Well to moderately | 1 (3.6) | NA | |
| Microsatellite Status | MSS | 24 (85.7) | ref |
| MSI high | 1 (3.6) | 15.04 (1.34–169.06, 0.028) | |
| Unknown | 3 (10.7) | 2.36 (0.66–8.50, 0.19) |
| Patients (%) | HR (95% CI, p-Value) | ||
|---|---|---|---|
| M2TS Expression | Low | 15 (53.6) | ref |
| High | 13 (46.4) | 6.58 (1.68–25.79, 0.007) | |
| Resection | No | 17 (60.7) | ref |
| Yes | 11 (39.3) | 2.30 (0.67–7.98, 0.19) | |
| Stage | I-III | 4 (14.3) | ref |
| IV | 24 (85.7) | 14.71 (1.11–194.42, 0.041) | |
| Differentiation | Moderately | 2 (7.1) | ref |
| Poorly | 25 (89.3) | 0.98 (0.16–6.11, 0.98) | |
| Well to moderately | 1 (3.6) | 4 × 109 (0.00–Inf, 1.000) | |
| Microsatellite Status | MSS | 24 (85.7) | ref |
| MSI high | 1 (3.6) | 145.33 (6.55–3225.37, 0.002) | |
| Unknown | 3 (10.7) | 3.67 (0.74–18.18, i) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sullivan, K.M.; Li, H.; Yang, A.; Zhang, Z.; Munoz, R.R.; Mahuron, K.M.; Yuan, Y.-C.; Paz, I.B.; Von Hoff, D.; Han, H.; et al. Tumor and Peritoneum-Associated Macrophage Gene Signature as a Novel Molecular Biomarker in Gastric Cancer. Int. J. Mol. Sci. 2024, 25, 4117. https://doi.org/10.3390/ijms25074117
Sullivan KM, Li H, Yang A, Zhang Z, Munoz RR, Mahuron KM, Yuan Y-C, Paz IB, Von Hoff D, Han H, et al. Tumor and Peritoneum-Associated Macrophage Gene Signature as a Novel Molecular Biomarker in Gastric Cancer. International Journal of Molecular Sciences. 2024; 25(7):4117. https://doi.org/10.3390/ijms25074117
Chicago/Turabian StyleSullivan, Kevin M., Haiqing Li, Annie Yang, Zhifang Zhang, Ruben R. Munoz, Kelly M. Mahuron, Yate-Ching Yuan, Isaac Benjamin Paz, Daniel Von Hoff, Haiyong Han, and et al. 2024. "Tumor and Peritoneum-Associated Macrophage Gene Signature as a Novel Molecular Biomarker in Gastric Cancer" International Journal of Molecular Sciences 25, no. 7: 4117. https://doi.org/10.3390/ijms25074117
APA StyleSullivan, K. M., Li, H., Yang, A., Zhang, Z., Munoz, R. R., Mahuron, K. M., Yuan, Y.-C., Paz, I. B., Von Hoff, D., Han, H., Fong, Y., & Woo, Y. (2024). Tumor and Peritoneum-Associated Macrophage Gene Signature as a Novel Molecular Biomarker in Gastric Cancer. International Journal of Molecular Sciences, 25(7), 4117. https://doi.org/10.3390/ijms25074117