Abstract
The treatment landscape of metastatic colorectal cancer (mCRC) has undergone significant evolution, with the introduction of targeted therapies and immunotherapy dramatically altering the management of microsatellite instability-high (MSI-H) tumors. However, the majority of patients, particularly those with microsatellite-stable (MSS) disease, remain refractory to immunotherapy, necessitating the exploration of alternative therapeutic strategies. This review summarizes the current treatment options for heavily pretreated mCRC patients who are not eligible for targeted therapies or clinical trials. Approved therapies for refractory mCRC, including regorafenib, trifluridine/tipiracil (FTD/TPI), and fruquintinib, demonstrate modest survival benefits but are often associated with significant toxicities. Additionally, innovative approaches targeting specific mutations such as KRAS G12C, HER2 amplification, and BRAF V600E are discussed, highlighting emerging combination regimens with immune checkpoint inhibitors and other agents to overcome resistance mechanisms. The potential of rechallenge strategies using previously administered therapies, such as oxaliplatin and anti-EGFR agents, is examined, supported by retrospective and prospective studies. Furthermore, the role of older drugs like mitomycin C in combination with capecitabine is revisited, offering insights into their viability in advanced treatment settings. Ongoing clinical trials with novel agents and combinations are expected to provide further clarity on optimizing sequential treatment regimens and personalizing therapy for mCRC patients. This review emphasizes the need for comprehensive molecular profiling and shared decision-making to improve outcomes and quality of life in this challenging patient population.
Keywords:
colon cancer; chemotherapy; refractory; immunotherapy; target therapy; mitomycin C; rechallenge 1. Introduction
In recent years, the treatment of solid tumors has witnessed the emergence of numerous novel agents and targeted therapies across various disease settings and histotypes, reflecting the growing need for increasingly personalized treatment approaches. This evolution has rapidly transformed the management of many oncological conditions, affecting treatment protocols for both localized disease (through neoadjuvant and adjuvant strategies) and advanced stages. In metastatic disease, these advances have been integrated into treatment regimens and, in some cases, have gradually moved into first-line therapies, with the goal of achieving maximum benefit and early response—even within palliative care settings. In some instances, this has led to remarkable outcomes and durable complete responses, prompting a reevaluation of palliative treatment strategies for the future [1,2,3].
In metastatic colorectal cancer (mCRC), the treatment landscape is particularly complex, necessitating an intense effort to optimize available therapies in the metastatic setting—a process complicated by several factors. First, the subtype that has shown the most significant benefit in terms of practice-changing outcomes and complete responses is characterized by microsatellite instability (MSI), which permits the use of immune checkpoint inhibitors. Specifically, in these patients, pembrolizumab—administered both as first-line therapy and in subsequent lines—has dramatically altered the disease’s natural history. Notably, in the phase II KEYNOTE-164 trial, pretreated metastatic patients receiving pembrolizumab monotherapy achieved an objective response rate (ORR) of 33%. Moreover, the phase III randomized KEYNOTE-177 trial demonstrated that patients treated with pembrolizumab as first-line therapy experienced significantly longer progression-free survival (PFS) compared to those receiving chemotherapy (median, 16.5 months vs. 8.2 months; HR: 0.60; 95% CI: 0.45–0.80; p = 0.0002) [4,5]. However, only about 15% of CRC patients exhibit MSI-high status, limiting eligibility for these innovative treatments. Consequently, a significant portion of current research is dedicated to extending the benefits of immunotherapy to a larger group of mCRC patients, particularly those with microsatellite-stable tumors—a challenge that remains unresolved.
Another complicating factor in mCRC treatment is the presence of multiple concurrent mutations, which can substantially reduce the effectiveness of targeted therapies by inducing both primary and secondary resistance. Numerous studies are underway to explore combinations of new agents to overcome this resistance and identify targeted treatments that can provide durable responses. Despite these vigorous research efforts, this issue remains unsolved.
A third aspect, which is the primary focus of this review, concerns the management of heavily pretreated patients in the metastatic setting who do not have access to targeted therapies—either due to a lack of available options or the absence of clinical trials—but who nonetheless maintain a reasonable performance status. This review will examine recent studies on treatment strategies beyond the second line, including the use of antiangiogenic agents and various combination therapies, while also questioning the future role of standard chemotherapy and rechallenge strategies. The aim is to explore viable options for heavily pretreated patients who are currently excluded from ongoing innovative research yet represent a significant clinical challenge in daily oncology practice.
2. Refractory mCRC Disease
2.1. A Brief Summary of the Drugs Currently Indicated for Refractory Disease
In current clinical practice, the choice of the best treatment for patients with refractory colorectal cancer, i.e., pretreated in the first and second-line setting, is based on three fundamental assumptions: treatment lines already received, which depend on the disease’s characteristics, the clinical condition of the patient (especially their residual performance status), and lastly, but perhaps most importantly, the expected toxicity of the treatment (which thus impacts the patient’s quality of life). The choice of treatment cannot exclude these considerations, which should be discussed with the patient, as to date the best choice for third-line treatment is not known, nor is the optimal sequence of treatments for patients with refractory colon cancer. Certainly, patients with molecular characteristics susceptible to targeted therapy should be directed toward such treatments, but currently, it is rare that wild-type KRAS patients have not already undergone anti-EGFR therapy, and that patients with microsatellite instability (MSI) have not already received immunotherapy in earlier treatment settings. Rechallenge options are considered, and we will discuss this in the dedicated chapter. However, it must always be considered that pretreated patients may have poor bone marrow reserve, which makes them difficult candidates for chemotherapy rechallenge. Options for targeted therapies on other mutations (such as HER2, NTRK, RET) are extremely rare in current practice and are only available through clinical trials. Currently, the drugs indicated for patients with refractory mCRC are represented by two antiangiogenic drugs (regorafenib and fruquintinib) and an oral fluoropyrimidine (trifluridine/tipiracil), administered either as monotherapy or in combination with bevacizumab (see Table 1).
2.1.1. Correct Trial and Regorafenib
Regorafenib is a multikinase inhibitor of tyrosine kinases involved in tumor angiogenesis mechanisms (e.g., PDGFR, FGFRs 1–2, VEGFRs 1–3, TIE2), tumor proliferation (e.g., RET, RAF, KIT), tumor microenvironment, and metastasis processes (VEGFR2–3, PDGFR), approved by the FDA and EMA for the treatment of refractory mCRC. The multicenter, randomized, placebo-controlled phase 3 CORRECT study showed that patients with refractory mCRC treated with regorafenib had a significant improvement in overall survival (OS), progression-free survival (PFS), and objective response rate (ORR) [6]. Patients were randomized to receive 160 mg of regorafenib or placebo once daily, along with best supportive care (BSC), on days 1 to 21 of a 28-day cycle. The study found that OS was more than 1.4 months longer for patients in the regorafenib + BSC group compared to those in the placebo + BSC group (HR 0.77; 95% CI, 0.64–0.94; p = 0.0052), and PFS was more than 0.2 months longer for the regorafenib + BSC group (HR 0.49; 95% CI, 0.42–0.58; p < 0.0001). These data were confirmed in an Asian population in the CONCUR study [7]. Although regorafenib proved to be an interesting molecule, it exhibited significant toxicity, with 93% of patients in the regorafenib arm experiencing an adverse event of any grade. Common side effects included fatigue, hand-foot syndrome (HFS), and hypertension. This led to the search for dose optimization strategies, including the multicenter, open-label phase 2 ReDOS study, where patients were randomly assigned to receive 80 mg of regorafenib daily, with weekly dose escalation, or the standard dose of 160 mg daily for 21 consecutive days in a 28-day cycle. The incidence of grade 3 adverse events commonly associated with regorafenib, particularly fatigue, HFSR, and hypertension, was numerically lower in the dose-escalation group compared to the standard-dose group. Today, international guidelines recommend using the dose-escalation strategy, as suggested by the ReDOS study, as an alternative dosing approach [8].
2.1.2. RECOURSE, SUNLIGHT and Trifluridine/Tipiracil (FTD/TPI)
Trifluridine/tipiracil (FTD/TPI), an oral chemotherapeutic agent, specifically a third-generation fluoropyrimidine, is approved by the FDA and EMA for the treatment of refractory mCRC. The RECOURSE study is a multicenter, randomized, double-blind, placebo-controlled trial that compared the FTD/TPI + BSC arm with the placebo + BSC arm [9]. The FTD/TPI regimen involves oral administration twice a day on days 1 to 5 and 8 to 12 of a 28-day treatment cycle. The treatment with FTD/TPI demonstrated a benefit in both OS and PFS compared to placebo. Specifically, the median OS was 7.1 months for the FTD/TPI + BSC group compared to 5.3 months for the placebo + BSC group (HR, 0.68; 95% CI, 0.58–0.81; p < 0.001). Similar results were also published in a similar study conducted on an Asian population [10]. The rationale for combining the third-generation fluoropyrimidine with an anti-vascular agent led to the design of the SUNLIGHT study, which aimed to compare monochemotherapy with FTD/TPI to combination therapy with bevacizumab [11]. This study demonstrated the superiority of the combined therapy in terms of OS, 10.8 months vs. 7.5 months (HR, 0.61; 95% CI, 0.49–0.77; p < 0.001), and PFS, 5.6 vs. 2.4 months (HR, 0.44; 95% CI, 0.36–0.54; p < 0.001), even in the population that had already received bevacizumab in earlier treatment lines. Toxicity was significantly higher in the combination arm, but in both studies, RECOURSE and SUNLIGHT, the overall rate of adverse events was high, especially for hematological alterations (neutropenia, anemia), fatigue and diarrhea. It is important to note, however, when selecting patients for the use of FTD/TPI as monotherapy or in combination, that the population in the SUNLIGHT study is very different in terms of characteristics compared to the RECOURSE study, with the latter being heavily pretreated [12]. Moreover, current research suggests the use of the FTD/TPI combination in earlier treatment lines [13,14,15]. The optimization of the use of this molecule also includes understanding not only the best combination but also the subpopulation that could benefit from it. For example, a study presented at ESMO 2024, which combined FDT/TPI with Ramucirumab in a population with refractory mCRC, suggested that the potential benefit of such a combined therapy might apply to a specific category of patients. In the case of the aforementioned combination, this advantage was observed particularly in women and patients with left-sided colon cancer [16].
2.1.3. FRESCO2 and Fruquintinib
Fruquintinib is a selective oral VEGFR1, -2 and -3 inhibitor approved by the FDA and EMA for the treatment of patients with refractory mCRC. The FRESCO-2 study is an international, multicenter, randomized, double-blind, placebo-controlled trial that evaluated the efficacy of fruquintinib in terms of OS and PFS. Patients received fruquintinib orally once a day for the first 21 days of a 28-day cycle, compared to placebo + BSC, in a heavily pretreated patient population [17]. The median OS was 7.4 months for the Fruquintinib + BSC group compared to 4.8 months with placebo + BSC (HR, 0.66; 95% CI, 0.55–0.80; p < 0.001) and PFS of 3.7 months for the Fruquintinib group compared to 1.8 months for placebo (HR, 0.32; 95% CI, 0.27–0.39; p < 0.001). Again, the percentage of patients with adverse events was high, especially fatigue, hand-foot syndrome and hypertension, leading to treatment discontinuation in 20% of patients, dose interruptions in 47% and dose reductions in 24% of cases [17]. It is interesting to note that, in this study, a very high percentage of patients (73%) had received more than three treatment lines in the metastatic setting, with 100% of patients having previously received regorafenib or FTD/TPI, and some of them both. This is an extremely pretreated population, so despite the advantage in terms of OS and PFS compared to placebo, and considering the toxicity, it is important to note that no hematological toxicity was reported, despite the potential hematological and bone marrow reserve impairment in the population.
Interesting studies on the combination of fruquintinib with FTD/TPI or similar drugs have been conducted in heavily pretreated populations, from the third line onwards. This combination has shown greater activity than single-agent therapies in preclinical models [18] and has been proposed in both prospective and retrospective clinical studies [19,20].

Table 1.
Drugs currently indicated for refractory mCRC.
Table 1.
Drugs currently indicated for refractory mCRC.
| Study | Treatment | N pts | mOS | HR mOS | mPFS | HR mPFS | RR (%) | Main AEs | Prior Biologics |
|---|---|---|---|---|---|---|---|---|---|
| CORRECT Grothery et al. [6] | Regorafenib | 505 | 6.4 | HR 0.77 p = 0.0052 | 1.9 | HR 0.49 p < 0.0001 | 1.0 | HFSR Fatigue | 100% bevacizumab 100% anti-EGFR |
| RECOURSE Mayer et al. [9] | TAS-102 | 534 | 7.1 | HR 0.68 p < 0.0001 | 2.0 | HR 0.48 p < 0.0001 | 1.6 | Neutropenia Diarrhea | 100% bevacizumab 100% anti-EGFR |
| FRESCO Li et al. [19] | Fruquintinib | 278 | 9.3 | HR 0.65 p < 0.001 | 3.7 | HR 0.26 p < 0.001 | 4.7 | HFSR HTN | 30% bevacizumab 14% anti-EGFR |
| SUNLIGHT Prager et al. [11] | TAS-102 + Beva | 246 | 10.8 | HR 0.61 p < 0.001 | 5.6 | HR 0.44 p < 0.001 | 6.3% | Neutropenia HTN | 71% bevacizumab 94% anti-EGFR |
| FRESCO-2 Dasari et al. [17] | Fruquintinib | 516 | 7.1 | HR 0.66 p < 0.001 | 3.7 | HR 0.32 p < 0.001 | 2% | HFSR HTN | 97% anti-VEGF 39% anti-EGFR |
| RAMTAS Annals, 2024 [16] | TAS-102 + Ramucirumab | 213 | 7.46 | HR 0.871 p = 0.1941 | 2.37 | HR 0.774 p = 0.0110 | 1.9% | Neutropenia Leukopenia | 87% bevacizumab |
2.2. Ongoing Clinical Trials with RAS Inhibitors
The viral oncogenic proteins of rat sarcoma (RAS) belong to the GTPase protein family and consist of four members encoded by three genes (KRAS4a, KRAS4b, HRAS and NRAS), which share sequence homology and differ from each other by the presence of the hypervariable C-terminal region. Oncogenic mutations in these oncoproteins lead to GTP hydrolysis, resulting in persistent binding that triggers the subsequent activation of downstream signaling pathways, such as Raf/MEK/ERK, which continuously stimulate survival. The KRAS mutation has always generated considerable interest regarding the potential to exploit its positivity, as it is one of the most important oncogenic mutations in colorectal cancer (CRC). Much scientific research has been invested in potential targeted drugs aimed at inhibiting its activity, thus significantly impacting the natural progression of these malignancies, which typically have a poor prognosis. Indeed, the presence of the KRAS mutation indicates a more aggressive disease with worse prognosis [21]. Until recently, however, KRAS was considered non-targetable because in vitro studies did not yield promising results. In recent years, scientific research has started to present the first encouraging data on the clinical activity of KRASG12C inhibitors, particularly adagrasib and sotorasib, in terms of objective response rate (ORR) in heavily pretreated KRAS G12C-mutated mCRC populations [22,23].
Despite the encouraging data from the aforementioned phase Ib/II studies, it became clear early on that the KRASG12C inhibitor treatment was less effective and impactful compared to what has been observed in other diseases, such as KRASG12C-mutated lung cancer [24]. This was attributed to the specific molecular characteristics of colorectal cancer and the complex signaling pathways, as demonstrated by preclinical studies [25]. Specifically, it was described that, in colorectal cancer cell lines, the inhibition of KRASG12C induces a greater rebound of phospho-ERK compared to NSCLC cells, with reactivation of EGFR. EGFR-mediated signaling was identified as the dominant mechanism of resistance to KRASG12C inhibitors in colorectal cancer. Therefore, a combination therapy targeting both EGFR and KRASG12C was proposed to overcome resistance to KRASG12C blockade in colorectal cancer [26]. Both monoclonal anti-EGFR antibodies used in current clinical practice for metastatic colorectal cancer treatment, Cetuximab and Panitumumab, have been studied in combination with KRASG12C inhibitors. Specifically, Cetuximab was studied in combination with Adagrasib in the KRYSTAL-1 study, a phase I/II study that included 94 patients with pretreated metastatic CRC with KRAS G12C mutation. These patients were administered Adagrasib 600 mg twice daily in combination with Cetuximab at an initial loading dose of 400 mg per square meter of body surface area, followed by 250 mg per square meter weekly or 500 mg per square meter every two weeks [27]. The results were encouraging, with an ORR of 34%, a median PFS of 6.9 months and a median OS of 15.9 months. Consistent with these findings, the combination of Panitumumab with a KRAS G12C inhibitor, particularly Sotorasib, showed positive results in phase Ib/II studies, which were later confirmed in the phase III CodeBreaK 300 study. This study included 53 patients with advanced CRC with KRAS G12C mutation refractory to chemotherapy [28]. In this study, Panitumumab was studied in combination with Sotorasib at the standard dose of 960 mg and in combination with a reduced dose of 240 mg, compared to a control arm receiving standard treatment for refractory mCRC (trifluridine-tipiracil or regorafenib). The best results were seen with the Panitumumab + Sotorasib combination at the standard dose of 960 mg, showing an ORR of 26.4% and a median PFS of 5.6 months, with a significant advantage over the reduced Sotorasib dose combination and, most notably, over the standard treatment arm, which showed an ORR of 0% and a median PFS of 2.2 months.
Numerous trials are ongoing investigating combinations of monoclonal anti-EGFR antibodies with other KRAS G12C inhibitors [29,30]. To date, the best molecule is not known as there are no comparative studies, given the similar toxicity. Despite the promising data from combination studies with KRAS inhibitors and anti-EGFR monoclonal antibodies for patients with refractory mCRC, many questions remain unanswered. In particular, it will be interesting to understand whether the optimal regimen of such combinations in KRAS G12C-mutated disease should be proposed in earlier treatment lines, and if so, whether it should be combined with chemotherapy and with which safety profile. Some combination trials with chemotherapeutic agents are ongoing [31,32,33]. Considering the complexity of the downstream EGFR signaling, many studies have explored the potential use of inhibitors targeting other oncoproteins involved in signaling mechanisms of proliferation and cell survival in patients with KRAS G12C mutations, such as SHP2, SOS and MEK. The data from these studies are promising and interesting but still immature [34,35,36].
Since KRAS G12C mutation is not the most frequent in colorectal cancers, unlike lung cancer, considerable interest is focused on other potential KRAS inhibitors, particularly KRAS G12D, which represents the most common KRAS mutation in colorectal cancer. Currently, there is encouraging preclinical data on ASP3082, a KRAS G12D degrader, and a phase I/II study (NCT05382559) is ongoing. Another KRAS G12D inhibitor under investigation is MRTX1133, in a phase I/II clinical trial (NCT05737706). Other KRAS inhibitors being studied are pan-inhibitors, which should have a broad spectrum of action. It will be interesting to monitor their development and safety data, as well as understand in which treatment lines these molecules will be placed [37,38] (see Table 2).
2.3. Ongoing Clinical Studies with Combination Therapies Using Immune Checkpoint Inhibitors
Immunotherapy is a well-established standard treatment for patients with MSI-H mCRC, both in the first-line setting and in subsequent lines if not yet used [39,40]. This latter situation is now rare in clinical practice as patients eligible for treatment with immune checkpoint inhibitors are typically treated early. However, interesting data have emerged in the setting of heavily pretreated patients with microsatellite stable disease. It is known that this molecular footprint renders patients resistant to immunotherapy, but since they represent the majority of colorectal cancer cases, numerous efforts have been made to increase the percentage of patients susceptible to immunotherapy by combining with immunomodulatory drugs to overcome this resistance. In particular, it is believed that drugs acting on the tumor microenvironment may favor antigen expression and immune cell recruitment. Combination therapies with chemotherapy regimens have been studied, yielding interesting data, especially in terms of better patient selection for the combination, such as a tool used in the Atezotribe study, which utilized a signature of 27 immune-related genes that could predict greater sensitivity to immunotherapy [41]. However, no chemo-immunotherapy combinations for MSS mCRC patients have been approved in current clinical practice due to the lack of statistically significant efficacy data [42]. A recent very interesting study conducted in the refractory, heavily pretreated disease, which was not amenable to targeted therapy, is the phase I study evaluating the combination of Botensilimab, a multifunctional anti-CTLA-4 antibody with Fc-enhanced activity, in combination with Balstilimab, an anti-PD-1 antibody [43]. The rationale behind this combination is the potential activity of Botensilimab, designed to expand therapy to poorly immunogenic solid tumors such as MSS mCRC. Several interesting data have emerged from this study, particularly regarding patients with liver metastases. The population in this study was heavily pretreated, with a median of three prior therapeutic lines. About 17% of the population had active liver metastases, with the remaining 83% having no history of liver metastasis, and 14% having had liver disease treated locally (surgery or other locoregional treatment). The data from this study show more favorable outcomes for patients with non-hepatic metastatic disease, with ORR (22% vs. 0%), DCR (73% vs. 25%), PFR (4.1 vs. 1.4) and OS (20.9 vs. 7.4 months) [43]. These data reinforce findings from other studies, both clinical and preclinical, on resistance of liver disease to immune checkpoint inhibitor treatments [44,45], suggesting a possible additional factor to consider in patient selection (see Table 2).
2.4. Ongoing Clinical Studies with Drugs Targeting Other Specific Mutations
2.4.1. ERB2 Amplification
Good clinical practice encourages oncologists to enroll patients in clinical trials to provide access to targeted treatments. However, this is often challenging in heavily pretreated patients due to factors such as poor performance status (ECOG PS ≥ 2) and the focus of most trials on early treatment lines.
Several ongoing trials are exploring anti-HER2 therapies for mCRC patients with HER2 amplification, which occurs in about 5% of KRAS wild-type cases [46]. Studies in advanced treatment lines have shown promising response rates, supporting the role of targeted therapies. The HERACLES study demonstrated a 28% response rate with trastuzumab and lapatinib in HER2-overexpressing KRAS wild-type mCRC patients [47]. Similarly, the MyPathway study achieved a 32% response rate using trastuzumab and pertuzumab [48]. In contrast, the TAPUR study showed no benefit in patients with ERBB2/3 mutations but reported a 25% response rate in those with ERBB2 amplification [49].
Antibody-drug conjugates (ADCs), combining monoclonal antibodies with cytotoxic agents, have emerged as promising treatments, with agents like trastuzumab emtansine and trastuzumab deruxtecan showing potential [50,51]. These therapies are of particular interest due to the poor prognosis and reduced response to anti-EGFR drugs in RAS wild-type mCRC. Ongoing research aims to clarify the role and sequencing of anti-HER2 and anti-EGFR therapies in this subset of patients (see Table 2).
2.4.2. Braf V600E
Patients with mCRC (metastatic colorectal cancer) with BRAF mutation represent about 12% of metastatic colorectal tumors and generally have a more unfavorable prognosis, mostly affecting the right colon, often with microsatellite instability [52]. Compared to melanoma, treatment with BRAF inhibitors has a modest response rate, which should again be interpreted in light of the complexity of the signaling pathways and the key players in tumor oncogenesis in colorectal cancers. This has led to the need for combined treatments with other drugs, particularly chemotherapy and anti-EGFR antibodies. The BEACON trial demonstrated the efficacy of combining BRAF, MEK and EGFR inhibitors, with Encorafenib plus Cetuximab now considered the gold standard due to similar overall survival (OS) to the triplet regimen but with a better safety profile [53]. However, response duration remains unsatisfactory, prompting research into novel combinations, such as immune checkpoint inhibitors, which may enhance tumor immunogenicity [54]. Ongoing studies are exploring combinations targeting other pathways, such as PI3K inhibitors, to overcome resistance and improve outcomes [55,56,57,58]. Studies are underway to evaluate the efficacy and safety profile of these combinations (see Table 2).
2.4.3. NTRK
Kinase gene fusions, though rare (about 0.9% in colorectal cancers), are promising therapeutic targets, with NTRK being the most common, followed by RET, FGFR, ROS1 and ALK [59]. NTRK fusions are more frequent in MSI-high and RAS/BRAF wild-type tumors, showing clinical similarities to BRAF mutations, such as right-sided primary tumors and higher metastatic potential [60]. These fusions are associated with poor prognosis and resistance to EGFR inhibitors, increasing their scientific relevance.
The NTRK inhibitors larotrectinib and entrectinib have demonstrated efficacy in metastatic solid tumors, including colorectal cancer, with FDA approval based on data from phase I/II “basket” trials [61,62] (see Table 2).
However, resistance mechanisms have been identified: on-target (mutations reducing drug affinity) and off-target (activation of alternative pathways like BRAF and KRAS mutations). Second-generation inhibitors, such as selitrectinib and repotrectinib, have shown promise in overcoming on-target resistance, but off-target resistance remains a challenge, especially in colorectal cancer where MAPK signaling activation is common. Research is ongoing to develop targeted drug combinations to address these resistance mechanisms and improve treatment outcomes [63,64] (see Table 3).
Table 3.
Ongoing clinical studies for refractory mCRC.
Table 2.
Targeted therapies for refractory mCRC.
Table 2.
Targeted therapies for refractory mCRC.
| Study | Interventions | Patients (n) | ORR (%) | mPFS (m) | mOS (m) | Grade ≥ 3 AEs (% of Patients) |
|---|---|---|---|---|---|---|
| HERACLES-A (phase II) [47] | Trastuzumab + lapatinib | 35 | 30 | 4.7 | 10.0 | 22%, including fatigue (9%) and LVSD (6%) |
| MyPathway (phase II) [48] | Trastuzumab + pertuzumab | 57 | 32 | 2.9 | 11.5 | 37%, including hypokalemia (5%) and abdominal pain (3%) |
| HERACLES-B (phase II) [51] | Pertuzumab + T-DM1 | 31 | 9.7 | 4.1 | NR | Thrombocytopenia (6%) |
| TRIUMPH (phase II) [65] | Trastuzumab + pertuzumab | 30 | 33 (ctDNA evaluable) | 3.1 | 8.8 | NR |
| TAPUR (phase II) [49] | Trastuzumab + pertuzumab | 28 | 25; DCR 54 | 12 weeks | 60 weeks | 10.5%, including anemia, infusion reaction, diarrhea, LVSD, and lymphocyte count reduction |
| DESTINY-CRC01 (phase II) [50] | T-DXd 6.4 mg/kg | 53 | 45.3 | 6.9 | 15.5 | 85%, including neutrophil count reduction (22%), anemia (14%), and platelet count decreased (10%) |
| DESTINY-CRC02 (phase II) [66] | T-DXd 6.4 mg/kg | 40 | 27.5 | 5.8 | NE | 41%, including neutrophil count reduction (26%), anemia (27%), and platelet count decreased (10%) |
| T-DXd 5.4 mg/kg | 82 | 37.8 | 5.5 | 13.4 | 49%, including neutrophil count reduction (29%) and nausea (7%) | |
| DESTINY-PanTumor01 (phase II) [67] | T-DXd 5.4 mg/kg | 20 | 20 | NR | NR | NR |
| MOUNTAINEER (phase II) [68] | Trastuzumab + tucatinib | 84 | 38.1 | 8.1 | 23.9 | Hypertension (7%) and urinary tract infection (6%) |
| Tucatinib | 30 | - | NR | 21.1 | AST increase (6.7%) | |
| HER2-FUSCC (phase II) [69] | Trastuzumab + pyrotinib | 18 | 22.2 | 3.4 | NR | Diarrhea (65%) |
| CodeBreaK 100 (phase II) [22] | Sotorasib | 62 | 9.7 | 4.0 | 10.6 | 12%, including diarrhea, fatigue, increased alanine aminotransferase, and increased aspartate aminotransferase |
| CodeBreaK 300 (phase III) [28] | Sotorasib 960 mg + panitumumab | 53 | 30.2 | 5.6 vs. 2.0 | NE vs. 10.3 | 38.5%, including dermatitis acneiform (7.7%), hypomagnesemia (5.7%), and rash (7.7%) |
| Sotorasib 240 mg + panitumumab | 53 | 7.5 | 1.8 vs. 10.6 | NE vs. 10.3 | 7.5%, including dermatitis acneiform (1.9%) and hypomagnesemia (1.9%) | |
| KRYSTAL-1 (phase I–II) [27] | Adagrasib | 44 | 19 | 5.6 | 19.8 | 27%, including diarrhea (9%) and fatigue (7%) |
| Adagrasib + cetuximab | 32 | 46 | 6.9 | 13.4 | 16%, including diarrhea, dermatitis acneiform, stomatitis, and infusion-related reactions | |
| BEACON (phase III) [70] | Encorafenib + cetuximab + binimetinib | 224 | 26.8 | 4.5 vs. 1.5 | 9.3 vs. 5.9 | 65.8% |
| Encorafenib + cetuximab | 220 | 19.5 | 4.3 vs. 1.5 | 9.3 vs. 5.9 | 57.4% | |
| Chemotherapy | 221 | 1.8 | — | — | 64.2% | |
| Yaeger et al. [71] | Vemurafenib + panitumumab | 15 | 13.0 | 7.6 | 3.2 | 20% |
| Morris et al. [56] | Encorafenib + cetuximab + nivolumab | 23 | 48.0 | 15.1 | 7.4 | 19% |
| Tabernero et al. [58] | Encorafenib + cetuximab + alpelisib vs. Encorafenib + cetuximab | 52 vs. 50 | 27 vs. 22 | 15.2 vs. not reached | 5.4 vs. 4.2 | 79% and 58% |
| SWOG S1406 [72] | Vemurafenib + cetuximab + irinotecan vs. cetuximab + irinotecan | 50 vs. 56 | 17 vs. 4 | 9.6 vs. 5.9 | 4.2 vs. 2.0 | 30% vs 7% |
| Hong et al. [31] | Larotrectinib | 153 (8 colon) | 79 (50 colon) | 25.8 | 44.4 | 13% |
| Demetri et al. [73] | Entrectinib | 121 (10 colon) | 61 (20 colon) | 13.8 (2.8 colon) | 33.8 (16 colon) | Increased weight, anemia, nervous system disorder |
NR = not reported.
3. Patients with Heavily Pretreated mCRC Not Eligible to Target Therapy or Clinical Trials
These patients represent a significant portion of the most complex cases to manage in daily clinical practice, both in terms of therapeutic choice and management of toxicities. As we saw in the previous chapters, several molecules have been approved for the setting of advanced, refractory colon disease. However, the best order of use is still unknown, as these molecules have only been compared in retrospective studies [74]. What we do know is that the survival rates for colorectal cancer have significantly increased in recent years, and this has been linked not so much to improved first-line treatment but to the survival benefit gained from the sum of subsequent lines. This makes sequential therapies for colorectal cancer crucial, and it will be important in the near future to determine how to best propose therapies in treatment lines. The challenge will not only be to better select patients for targeted treatments based on a more thorough molecular understanding of the disease, thus enabling better treatment personalization, but also, with regard to innovative treatments, making thoughtful choices based on the therapies already received and the expected toxicities. Effective communication with the patient will become increasingly important in clinical practice, as patients need to be informed about potential options, and the choice should be shared. In this futuristic scenario, which points to increasingly complex molecules and treatment combinations, often with significant toxicities, it is crucial not to overlook what we have learned so far about this complex disease, including with respect to older chemotherapeutic treatments and rechallenging therapies already received. This includes the use of drugs such as mitomycin C, as well as rechallenging with Oxaliplatin and anti-EGFR drugs. Below is a brief summary of these potential scenarios.
3.1. Role of Treatments Rechallenge
The reintroduction of treatments previously received in earlier lines of therapy is not always feasible. It assumes, on one hand, that there was a response to the therapy, no progression during treatment and the absence of residual toxicities that would prevent reintroduction. This is the case, for example, with Oxaliplatin, a cornerstone drug in early chemotherapy lines, which is often suspended before progression, with treatment continuing with fluoropyrimidine, with or without a maintenance biologic drug, to reduce the likelihood of long-term neurological toxicity or significant hematological toxicities. Reintroduction in more advanced treatment lines is possible but constrained by residual peripheral sensory toxicity or limited bone marrow reserve, particularly thrombocytopenia.
Regarding Oxaliplatin, there is also the rechallenge strategy, which involves using the drug previously administered in earlier lines with an initial response to treatment, followed by progression that required a change in therapy. In the third or later line of chemotherapy, rechallenging allows for the reuse of Oxaliplatin, even after documented resistance, based on the assumption that, after one or more subsequent treatments, different from Oxaliplatin, the disease may have developed new mutations that make it responsive again to the drug. There are no prospective clinical studies in the literature, but retrospective real-life data seem to support this hypothesis [75,76,77]. Clinical trials are ongoing to evaluate the reintroduction/rechallenge of Oxaliplatin in patients with refractory mCRC, either in combination with biologic drugs, with fluoropyrimidine or as monotherapy (NCT03485027, NCT03940131, NCT03311750).
The possibility of rechallenging previously received treatments, despite documented progression, has always been of interest to oncologists, not only for necessity but also for the opportunity to use drugs already administered to the patient, with their toxicity already understood. In fact, we know that the molecules currently approved for refractory disease are often associated with high expected toxicity, and we do not always treat patients with a good ECOG PS. Often, marked asthenia or poor bone marrow reserve persist due to the accumulation of toxicities from prior treatments. We know that these molecules have been compared to placebo, but we lack objective data on the potential benefit compared to rechallenge treatments.
Some interesting data, although retrospective, seem to indicate that rechallenge therapy should not be considered inferior. One such retrospective study collected data from 394 patients across 21 centers, comparing PFS and OS in patients who, in the third line, received rechallenged fluoropyrimidine-based chemotherapy versus the third line with Regorafenib. It concluded that disease control rates and OS were higher with rechallenge therapy compared to Regorafenib, particularly in patients who had achieved disease control with fluoropyrimidine chemotherapy in one of the first two treatment lines [78].
One limitation in interpreting these data—aside from the retrospective nature of the study—is that the combination with biologic drugs (anti-EGFR or anti-VEGF) was allowed, with about 60% of patients receiving a biologic agent. This makes it difficult to discern whether the benefit of the rechallenge treatment was primarily due to the chemotherapy or the biologic treatments.
Several data now reinforce the idea that rechallenging biologic treatments has a rationale. Regarding anti-EGFR treatments, many retrospective studies had already suggested the potential efficacy of rechallenging therapy in subsequent lines for refractory mCRC [79,80,81], validated by prospective studies [82,83,84]. This potential benefit is based on molecular mechanisms that restore sensitivity to anti-EGFR treatment, particularly the restoration of Ras WT clones after a sufficient period from discontinuing anti-EGFR treatment. This is because the most frequent and well-studied mechanism of resistance to biologic treatment, particularly through tumor DNA (ctDNA) analysis via liquid biopsy, is the increase in KRAS-mutated disease. However, other resistant mutations may also occur, such as HER2 overexpression, ERBB2 amplification, BRAF V600E mutation and PI3K mutations. Therefore, it would be advisable to retest patients who were initially resistant to anti-EGFR treatment, following the mutation panel of refractory mCRC disease, to select patients who may benefit from such treatment [85] (see Table 4).
Table 4.
Rechallenge with EGFR inhibitors.
3.2. “Old Drugs”: The Case of Mitomycin C Combined with Capecitabine
Mitomycin C is an “old” oncological drug, a natural antibiotic administered intravenously that has shown antitumor activity and was used in a variety of solid tumors, including gastrointestinal cancers. It is usually a well-tolerated drug, although in some cases it can cause delayed bone marrow toxicity. The biological activity of mitomycin C in the treatment of colorectal cancer is well-known. In 2004, Rao and colleagues published a phase II study in a first-line metastatic colorectal cancer (mCRC) setting, demonstrating a benefit both in terms of overall response rate (ORR 38%) and progression-free survival (PFS 7.11 months), with a median overall survival (OS) of 14.3 months and no significant toxicity compared to capecitabine alone [93]. The authors argued that the benefit obtained with the combination of mitomycin C was supported by the data from the capecitabine monotherapy study, where the median OS was 12.9 months and the PFS was 4.6 months [94], concluding that this combination could be a valid therapeutic option in patients who prefer or cannot have a central venous catheter and are not candidates for other chemotherapy drugs. These data were replicated in an open-label phase II study that enrolled patients in third-line treatment (36 patients) who received the combination of mitomycin C and capecitabine. This study recorded a median overall survival of 9.3 months with a one-year survival rate of 30.6% and a median PFS of 5.4 months [95]. In clinical practice, several retrospective studies have been conducted, showing good tolerance to the treatment and disease control consistent with the data from advanced treatment lines [96,97]. Contrary to these data, another retrospective study by Ferrarotto in 2012, which analyzed data from 109 heavily pretreated patients who received mitomycin C and capecitabine, recorded a median survival of 4.5 months, similar to that of patients receiving best supportive care [98]. This may partly be explained by the idea that selecting patients who might benefit from the therapy is crucial, even—if not especially—in such advanced treatment settings, personalizing the treatment, when possible, especially in cases where patients can be enrolled in clinical trials with preserved performance status and targetable mutations.
4. Discussion
The treatment landscape for metastatic colorectal cancer (mCRC) continues to evolve, driven by the increasing complexity of disease biology, novel therapeutic options and the pressing need for personalized strategies. This review highlights key challenges in managing heavily pretreated mCRC patients, underscores the need for effective sequencing of existing therapies and explores emerging options, including rechallenge strategies and targeted combinations. Recent advancements in molecular profiling have reshaped the management of mCRC by enabling targeted therapies for specific genetic mutations, such as KRAS G12C, HER2 amplification and BRAF V600E. Despite promising data from clinical trials, the benefit of targeted therapies often remains limited in duration due to primary and acquired resistance mechanisms. For instance, KRAS G12C inhibitors like adagrasib and sotorasib have demonstrated efficacy in pretreated populations in combination with anti-EGFR agents [27,28]. Studies such as KRYSTAL-1 and CodeBreaK 300 highlight the potential of these combinations, yet further research is needed to optimize sequencing and define patient subgroups most likely to benefit. Rechallenge therapies represent an intriguing approach for managing refractory mCRC, always taking into account the residual toxicities from previous treatments and the expected toxicities. Retrospective studies and prospective trials suggest that rechallenging with anti-EGFR therapies can be effective in patients with restored RAS wild-type status, as determined by liquid biopsy [85]. Similarly, oxaliplatin rechallenge may offer benefit in select patients with preserved bone marrow reserve and manageable neurotoxicity, underscoring the importance of patient selection and molecular monitoring. However, the lack of large prospective studies comparing rechallenge with newer agents like regorafenib or trifluridine/tipiracil (FTD/TPI) limits definitive conclusions. Mitomycin C, combined with capecitabine, presents a potentially viable option in advanced treatment settings, particularly for patients ineligible for clinical trials or targeted therapies. Historical data demonstrate modest survival benefits and manageable toxicity profiles, yet conflicting results from retrospective studies highlight the need for careful patient selection. The observed variability in outcomes likely reflects differences in baseline patient characteristics and prior treatments, emphasizing the importance of shared decision-making and personalized approaches. Drugs like regorafenib, fruquintinib and FTD/TPI have shown survival benefits in refractory mCRC, as demonstrated in pivotal trials such as CORRECT, FRESCO-2 and RECOURSE [6,9,17]. All these molecules have demonstrated favorable quality-of-life outcomes compared to placebo in both clinical trials and retrospective real-life studies [99,100,101]. However, these agents are frequently associated with significant toxicities, including fatigue, hand-foot syndrome and hematological adverse events, which can limit their use in heavily pretreated patients. Strategies such as dose escalation for regorafenib (as validated by the ReDOS study) and combination therapies with bevacizumab (e.g., SUNLIGHT trial) are examples of how scientific research has focused in recent years on these two fundamental directions: increasing the effectiveness of treatments and reducing toxicities [8,11]. Further studies are warranted to refine these approaches and explore novel combinations, such as fruquintinib with FTD/TPI or immune checkpoint inhibitors [90]. Another aspect that has engaged research is aimed at increasing the number of patients eligible for immunotherapy treatments. In fact, while immune checkpoint inhibitors have revolutionized treatment for microsatellite instability-high (MSI-H) mCRC, MSS patients remain largely refractory to immunotherapy. Emerging combination strategies, such as Botensilimab and Balstilimab, aim to modulate the tumor microenvironment and enhance immunogenicity in MSS tumors [43]. Preliminary data from phase I studies indicate improved outcomes for patients without liver metastases, highlighting the need to better select patients in order to achieve an optimal response to immunotherapy treatment. The continued evolution of mCRC management hinges on the integration of novel therapeutic agents and combination regimens into clinical practice. Promising data from ongoing trials involving RAS inhibitors, HER2-targeted therapies and second-generation NTRK inhibitors underscore the potential for new targeted approaches [See Table 3]. Additionally, efforts to address off-target resistance mechanisms, optimize immunotherapy combinations and refine molecular profiling techniques will be crucial to improving outcomes [see Figure 1].
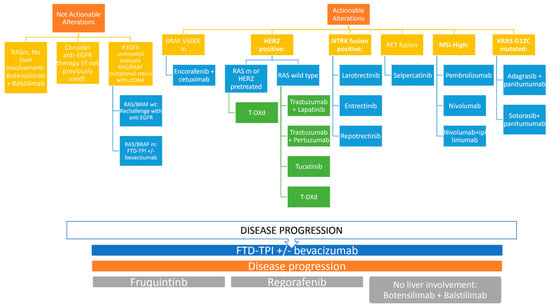
Figure 1.
Therapeutic algorithm.
5. Conclusions
The management of heavily pretreated mCRC remains a complex challenge, requiring a nuanced understanding of disease biology, therapeutic options and patient-specific factors. While significant progress has been made with targeted therapies, immunotherapy and rechallenge strategies, optimizing sequential treatment regimens and minimizing toxicity are paramount. Comprehensive molecular profiling and collaborative decision-making between clinicians and patients are essential to advancing personalized care. As ongoing research continues to provide new insights, the ultimate goal remains to extend survival and enhance quality of life for this challenging patient population.
Author Contributions
Study concept and design, A.Z. and S.C.; drafting of the manuscript, S.C. and M.L.; tables and figure, E.O.; critical revision of the manuscript for important intellectual content, S.N., A.Z. and F.M.; study supervision, A.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ree, A.H.; Høye, E.; Esbensen, Y.; Beitnes, A.R.; Negård, A.; Bernklev, L.; Tetlie, L.K.; Fretland, Å.A.; Hamre, H.M.; Kersten, C.; et al. Complete response of metastatic microsatellite-stable BRAF V600E colorectal cancer to first-line oxaliplatin-based chemotherapy and immune checkpoint blockade. Oncoimmunology 2024, 13, 2372886. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Robert, C.; Ribas, A.; Hamid, O.; Daud, A.; Wolchok, J.D.; Joshua, A.M.; Hwu, W.J.; Weber, J.S.; Gangadhar, T.C.; Joseph, R.W.; et al. Durable Complete Response After Discontinuation of Pembrolizumab in Patients with Metastatic Melanoma. J. Clin. Oncol. 2018, 36, 1668–1674. [Google Scholar] [CrossRef] [PubMed]
- Debien, V.; Agostinetto, E.; Bruzzone, M.; Ceppi, M.; Martins-Branco, D.; Molinelli, C.; Jacobs, F.; Nader-Marta, G.; Lambertini, M.; de Azambuja, E. The Impact of Initial Tumor Response on Survival Outcomes of Patients with HER2-Positive Advanced Breast Cancer Treated with Docetaxel, Trastuzumab, and Pertuzumab: An Exploratory Analysis of the CLEOPATRA Trial. Clin. Breast Cancer 2024, 24, 421–430.e3. [Google Scholar] [CrossRef] [PubMed]
- André, T.; Shiu, K.K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N. Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Kim, T.W.; Van Cutsem, E.; Geva, R.; Jäger, D.; Hara, H.; Burge, M.; O’Neil, B.; Kavan, P.; Yoshino, T.; et al. Phase II Open-Label Study of Pembrolizumab in Treatment-Refractory, Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: KEYNOTE-164. J. Clin. Oncol. 2020, 38, 11–19. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grothey, A.; Van Cutsem, E.; Sobrero, A.; Siena, S.; Falcone, A.; Ychou, M.; Humblet, Y.; Bouché, O.; Mineur, L.; Barone, C.; et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): An international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 2013, 381, 303–312. [Google Scholar] [CrossRef]
- Li, J.; Qin, S.; Xu, R.; Yau, T.C.C.; Ma, B.; Pan, H.; Xu, J.; Bai, Y.; Chi, Y.; Wang, L.; et al. Regorafenib plus best supportive care versus placebo plus best supportive care in Asian patients with previously treated metastatic colorectal cancer (CONCUR): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2015, 16, 619–629. [Google Scholar] [CrossRef]
- Bekaii-Saab, T.S.; Ou, F.S.; Ahn, D.H.; Boland, P.M.; Ciombor, K.K.; Heying, E.N.; Dockter, T.J.; Jacobs, N.L.; Pasche, B.C.; Cleary, J.M.; et al. Regorafenib dose-optimisation in patients with refractory metastatic colorectal cancer (ReDOS): A randomised, multicentre, open-label, phase 2 study. Lancet Oncol. 2019, 20, 1070–1082. [Google Scholar] [CrossRef]
- Mayer, R.J.; Van Cutsem, E.; Falcone, A.; Yoshino, T.; Garcia-Carbonero, R.; Mizunuma, N.; Yamazaki, K.; Shimada, Y.; Tabernero, J.; Komatsu, Y.; et al. RECOURSE Study Group. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N. Engl. J. Med. 2015, 372, 1909–1919. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Kim, T.W.; Shen, L.; Sriuranpong, V.; Pan, H.; Xu, R.; Guo, W.; Han, S.W.; Liu, T.; Park, Y.S.; et al. Results of a Randomized, Double-Blind, Placebo-Controlled, Phase III Trial of Trifluridine/Tipiracil (TAS-102) Monotherapy in Asian Patients with Previously Treated Metastatic Colorectal Cancer: The TERRA Study. J. Clin. Oncol. 2018, 36, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Prager, G.W.; Taieb, J.; Fakih, M.; Ciardiello, F.; Van Cutsem, E.; Elez, E.; Cruz, F.M.; Wyrwicz, L.; Stroyakovskiy, D.; Pápai, Z.; et al. Trifluridine-Tipiracil and Bevacizumab in Refractory Metastatic Colorectal Cancer. N. Engl. J. Med. 2023, 388, 1657–1667. [Google Scholar] [CrossRef] [PubMed]
- Zaniboni, A. Sunglasses for Sunlight: Considerations on New Treatment Opportunities for Refractory Colorectal Cancer. Cancers 2024, 16, 1348. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- André, T.; Falcone, A.; Shparyk, Y.; Moiseenko, F.; Polo-Marques, E.; Csöszi, T.; Campos-Bragagnoli, A.; Liposits, G.; Chmielowska, E.; Aubel, P.; et al. Trifluridine-tipiracil plus bevacizumab versus capecitabine plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer ineligible for intensive therapy (SOLSTICE): A randomised, open-label phase 3 study. Lancet Gastroenterol. Hepatol. 2023, 8, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Danielewicz, I.; Saunders, M.P.; Pfeiffer, P.; Argilés, G.; Borg, C.; Glynne-Jones, R.; Punt, C.J.A.; Van de Wouw, A.J.; Fedyanin, M.; et al. First-line trifluridine/tipiracil + bevacizumab in patients with unresectable metastatic colorectal cancer: Final survival analysis in the TASCO1 study. Br. J. Cancer 2022, 126, 1548–1554. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ciracì, P.; Conca, V.; Moretto, R.; Antoniotti, C.; Ambrosini, M.; Murgioni, S.; Gori, G.; Russo, A.; Bergamo, F.; Randon, G.; et al. Trifluridine/tipiracil plus capecitabine and bevacizumab as upfront treatment for metastatic colorectal cancer: Results of the phase 1 TriComB study. J. Clin. Oncol. 2024, 42, 3558. [Google Scholar] [CrossRef]
- Kasper-Virchow, S.; Hofheinz, R.D.; Stintzing, S.; Dechow, T.N.; Ettrich, T.J.; Sinn, M.; Roderburg, C.; von Weikersthal, L.F.; Graeven, U.; Mueller, C.; et al. LBA25 Randomized phase III trial of ramucirumab in combination with TAS102 (Trifluridin/Tipiracil) vs. TAS102 monotherapy in heavily pretreated metastatic colorectal cancer: The RAMTAS/IKF643 trial of the German AIO (AIO-KRK-0316). Ann. Oncol. 2024, 35 (Suppl. S2), 1–72. [Google Scholar] [CrossRef]
- Dasari, A.; Lonardi, S.; Garcia-Carbonero, R.; Elez, E.; Yoshino, T.; Sobrero, A.; Yao, J.; García-Alfonso, P.; Kocsis, J.; Cubillo Gracian, A.; et al. Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (FRESCO-2): An international, multicentre, randomised, double-blind, phase 3 study. Lancet 2023, 402, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Nukatsuka, M.; Fujioka, A.; Nagase, H.; Tanaka, G.; Hayashi, H. Evaluation of a Novel Combination Therapy, Based on Trifluridine/Tipiracil and Fruquintinib, against Colorectal Cancer. Chemotherapy 2023, 68, 102–110. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, L.; Wang, T.; Wu, Z.; Li, Y.; Ma, H.; Wang, L.; Lei, S.; Chen, W. Fruquintinib in combination with sintilimab or TAS-102 as third-line or above treatment in patients with metastatic colorectal cancer: A real-world study. Transl. Cancer Res. 2023, 12, 3034–3044. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zou, J.; Wang, Y.; Xu, J.; Li, J.; Wang, T.; Zhang, Y.; Bai, Y. A Retrospective Study of Trifluridine/Tipiracil with Fruquintinib in Patients with Chemorefractory Metastatic Colorectal Cancer. J. Clin. Med. 2023, 13, 57. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dinu, D.; Dobre, M.; Panaitescu, E.; Bîrlă, R.; Iosif, C.; Hoara, P.; Caragui, A.; Boeriu, M.; Constantinoiu, S.; Ardeleanu, C. Prognostic significance of KRAS gene mutations in colorectal cancer—Preliminary study. J. Med. Life 2015, 7, 581–587. [Google Scholar]
- Fakih, M.G.; Kopetz, S.; Kuboki, Y.; Kim, T.W.; Munster, P.N.; Krauss, J.C.; Falchook, G.S.; Han, S.-W.; Heinemann, V.; Muro, K.; et al. Sotorasib for previously treated colorectal cancers with KRASG12C mutation (CodeBreaK100): A prespecified analysis of a single-arm, phase 2 trial. Lancet Oncol. 2021, 23, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Weiss, L. ESMO 2021—Highlights in colorectal cancer. MEMO—Mag. Eur. Med. Oncol. 2022, 15, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Qunaj, L.; May, M.S.; Neugut, A.I.; Herzberg, B.O. Prognostic and therapeutic impact of the KRAS G12C mutation in colorectal cancer. Front. Oncol. 2023, 13, 1252516. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Miyashita, H.; Hong, D.S. Combining EGFR and KRAS G12C Inhibitors for KRAS G12C Mutated Advanced Colorectal Cancer. J. Cancer Immunol. 2024, 6, 62–69. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Amodio, V.; Yaeger, R.; Arcella, P.; Cancelliere, C.; Lamba, S.; Lorenzato, A.; Arena, S.; Montone, M.; Mussolin, B.; Bian, Y.; et al. EGFR Blockade Reverts Resistance to KRASG12C Inhibition in Colorectal Cancer. Cancer Discov. 2020, 10, 1129–1139. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yaeger, R.; Uboha, N.V.; Pelster, M.S.; Bekaii-Saab, T.S.; Barve, M.; Saltzman, J.; Sabari, J.K.; Peguero, J.A.; Paulson, A.S.; Janne, P.A.; et al. Efficacy and Safety of Adagrasib plus Cetuximab in Patients with KRASG12C-Mutated Metastatic Colorectal Cancer. Cancer Discov. 2024, 14, 982–993. [Google Scholar] [CrossRef]
- Fakih, M.G.; Salvatore, L.; Esaki, T.; Modest, D.P.; Lopez-Bravo, D.P.; Taieb, J.; Karamouzis, M.V.; Ruiz-Garcia, E.; Kim, T.-W.; Kuboki, Y.; et al. Sotorasib plus Panitumumab in Refractory Colorectal Cancer with Mutated, KRASG12C. N. Engl. J. Med. 2023, 389, 2125–2139. [Google Scholar] [CrossRef]
- Desai, J.; Alonso, G.; Kim, S.H.; Cervantes, A.; Karasic, T.; Medina, L.; Shacham-Shmueli, E.; Cosman, R.; Falcon, A.; Gort, E.; et al. Divarasib plus cetuximab in KRAS G12C-positive colorectal cancer: A phase 1b trial. Nat. Med. 2023, 30, 271–278. [Google Scholar] [CrossRef]
- Xu, R.-H.; Xu, Y.; Yan, D.; Munster, P.; Ruan, D.; Deng, Y.; Pan, H.; Underhill, C.; Richardson, G.; Nordman, I.; et al. 550O Safety and efficacy of D-1553 in combination with cetuximab in KRAS G12C mutated colorectal cancer (CRC): A phase II studytle. Ann. Oncol. 2023, 34, S410–S411. [Google Scholar] [CrossRef]
- Hong, D.S.; Kuboki, Y.; Strickler, J.H.; Fakih, M.; Houssiau, H.; Price, T.J.; Elez, E.; Siena, S.; Chan, E.; Nolte-Hippenmeyer, J.; et al. Sotorasib (Soto) plus panitumumab (Pmab) and FOLFIRI for previously treated KRAS G12C-mutated metastatic colorectal cancer (mCRC): CodeBreaK 101 phase 1b safety and efficacy. J. Clin. Oncol. 2023, 41 (Suppl. S16), 3513. [Google Scholar] [CrossRef]
- Clarke, J.M.; Felip, E.; Li, B.T.; Ruffinelli, J.C.; Garrido, P.; Zugazagoitia, J.; Goldberg, S.; Ramalingam, S.; Victoria, I.; Puri, S.; et al. MA0605 codeBreaK 101: Safety efficacy of sotorasib with carboplatin pemetrexed in KRAS G12C-mutated advanced NSCLC. J. Thorac. Oncol. 2023, 18, S118–S119. [Google Scholar] [CrossRef]
- Sakata, S.; Akamatsu, H.; Azuma, K.; Uemura, T.; Tsuchiya-Kawano, Y.; Yoshioka, H.; Osuga, M.; Koh, Y.; Morita, S.; Yamamoto, N. The primary endpoint analysis of SCARLET study: A single-arm, phase II study of sotorasib plus carboplatin-pemetrexed in patients with advanced non-squamous, non-small cell lung cancer with KRAS G12C mutation (WJOG14821L). J. Clin. Oncol. 2023, 41, 9006. [Google Scholar] [CrossRef]
- Ramalingam, S.; Fakih, M.; Strickler, J.; Govindan, R.; Li, B.T.; Goldberg, S.; Gandara, D.; Burns, T.; Barve, M.; Shu, C.; et al. Abstract P05-01: A phase 1b study evaluating the safety and efficacy of sotorasib, a KRASG12C inhibitor, in combination with trametinib, a MEK inhibitor, in KRAS p.G12C-Mutated Solid Tumors. Mol. Cancer Ther. 2021, 20, P05-01. [Google Scholar] [CrossRef]
- Awad, M.M.; Goldschmidt, J.; Spira, A.I.; Malhotra, R.; Yorio, J.T.; Bhambhani, V.; Cheng, Y.; Lee, P.S.; Govindan, R. Abstract C026: Initial safety, pharmacokinetics, and recommended Phase 2 dose from RAMP 203: A Phase 1/2 study of Avutometinib + Sotorasib in KRAS G12C Mutant Non-Small Cell Lung Cancer. Mol. Cancer Ther. 2023, 22, C026. [Google Scholar] [CrossRef]
- Hofmann, M.H.; Gmachl, M.; Ramharter, J.; Savarese, F.; Gerlach, D.; Marszalek, J.R.; Sanderson, M.P.; Kessler, D.; Trapani, F.; Arnhof, H.; et al. BI-3406, a potent and selective SOS1-KRAS interaction inhibitor, is effective in KRAS-driven cancers through combined MEK inhibition. Cancer Discov. 2021, 11, 142–157. [Google Scholar] [CrossRef]
- Jiang, J.; Jiang, L.; Maldonato, B.J.; Wang, Y.; Holderfield, M.; Aronchik, I.; Winters, I.P.; Salman, Z.; Blaj, C.; Menard, M.; et al. Translational and Therapeutic Evaluation of RAS-GTP Inhibition by RMC-6236 in RAS-Driven Cancers. Cancer Discov. 2024, 14, 994–1017. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Holderfield, M.; Lee, B.J.; Jiang, J.; Tomlinson, A.; Seamon, K.J.; Mira, A.; Patrucco, E.; Goodhart, G.; Dilly, J.; Gindin, Y.; et al. Concurrent inhibition of oncogenic and wild-type RAS-GTP for cancer therapy. Nature 2024, 629, 919–926. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grothey, A. Pembrolizumab in MSI-H-dMMR Advanced Colorectal Cancer—A New Standard of Care. N. Engl. J. Med. 2020, 383, 2283–2285. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Diaz, L.A., Jr.; Kim, T.W.; Van Cutsem, E.; Geva, R.; Jäger, D.; Hara, H.; Burge, M.; O’Neil, B.H.; Kavan, P.; et al. Pembrolizumab for previously treated, microsatellite instability-high/mismatch repair-deficient advanced colorectal cancer: Final analysis of KEYNOTE-164. Eur. J. Cancer 2023, 186, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Antoniotti, C.; Boccaccino, A.; Seitz, R.; Giordano, M.; Catteau, A.; Rossini, D.; Pietrantonio, F.; Salvatore, L.; McGregor, K.; Bergamo, F.; et al. An Immune-Related Gene Expression Signature Predicts Benefit from Adding Atezolizumab to FOLFOXIRI plus Bevacizumab in Metastatic Colorectal Cancer. Clin. Cancer Res. 2023, 29, 2291–2298. [Google Scholar] [CrossRef] [PubMed]
- Gandini, A.; Puglisi, S.; Pirrone, C.; Martelli, V.; Catalano, F.; Nardin, S.; Seeber, A.; Puccini, A.; Sciallero, S. The role of immunotherapy in microsatellites stable metastatic colorectal cancer: State of the art and future perspectives. Front. Oncol. 2023, 13, 1161048. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bullock, A.J.; Schlechter, B.L.; Fakih, M.G.; Tsimberidou, A.M.; Grossman, J.E.; Gordon, M.S.; Wilky, B.A.; Pimentel, A.; Mahadevan, D.; Balmanoukian, A.S.; et al. Botensilimab plus balstilimab in relapsed/refractory microsatellite stable metastatic colorectal cancer: A phase 1 trial. Nat. Med. 2024, 30, 2558–2567. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aruquipa, M.P.S.; Donadio, M.S.; Peixoto, R.D. Liver metastasis and resistance to immunotherapy in microsatellite stable colorectal cancer. A literature review. Ecancermedicalscience 2024, 18, 1771. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, E.X.; Loree, J.M.; Titmuss, E.; Jonker, D.J.; Kennecke, H.F.; Berry, S.; Couture, F.; Ahmad, C.E.; Goffin, J.R.; Kavan, P.; et al. Liver Metastases and Immune Checkpoint Inhibitor Efficacy in Patients with Refractory Metastatic Colorectal Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open. 2023, 6, e2346094. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Robinson, H.R.; Messersmith, W.A.; Lentz, R.W. HER2-Positive Metastatic Colorectal Cancer. Curr. Treat. Options Oncol. 2024, 25, 585–604. [Google Scholar] [CrossRef] [PubMed]
- Tosi, F.; Sartore-Bianchi, A.; Lonardi, S.; Amatu, A.; Leone, F.; Ghezzi, S.; Martino, C.; Bencardino, K.; Bonazzina, E.; Bergamo, F.; et al. Long-term Clinical Outcome of Trastuzumab and Lapatinib for HER2-positive Metastatic Colorectal Cancer. Clin. Color. Cancer 2020, 19, 256–262.e2. [Google Scholar] [CrossRef] [PubMed]
- Meric-Bernstam, F.; Hurwitz, H.; Raghav, K.P.S.; McWilliams, R.R.; Fakih, M.; VanderWalde, A.; Swanton, C.; Kurzrock, R.; Burris, H.; Sweeney, C.; et al. Pertuzumab plus trastuzumab for HER2-amplified metastatic colorectal cancer (MyPathway): An updated report from a multicentre, open-label, phase 2a, multiple basket study. Lancet Oncol. 2019, 20, 518–530. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gupta, R.; Meric-Bernstam, F.; Rothe, M.; Garrett-Mayer, E.; Mangat, P.K.; D’Andre, S.; Ahn, E.R.; O’Lone, R.; Halabi, S.; Grantham, G.N.; et al. Pertuzumab Plus Trastuzumab in Patients with Colorectal Cancer with ERBB2 Amplification or ERBB2/3 Mutations: Results From the TAPUR Study. JCO Precis. Oncol. 2022, 6, e2200306. [Google Scholar] [CrossRef] [PubMed]
- Siena, S.; Di Bartolomeo, M.; Raghav, K.; Masuishi, T.; Loupakis, F.; Kawakami, H.; Yamaguchi, K.; Nishina, T.; Fakih, M.; Elez, E.; et al. Trastuzumab deruxtecan (DS-8201) in patients with HER2-expressing metastatic colorectal cancer (DESTINY-CRC01): A multicentre, open-label, phase 2 trial. Lancet Oncol. 2021, 22, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Sartore-Bianchi, A.; Lonardi, S.; Martino, C.; Fenocchio, E.; Tosi, F.; Ghezzi, S.; Leone, F.; Bergamo, F.; Zagonel, V.; Ciardiello, F.; et al. Pertuzumab and trastuzumab emtansine in patients with HER2-amplified metastatic colorectal cancer: The phase II HERACLES-B trial. ESMO Open 2020, 5, e000911. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ros, J.; Rodríguez-Castells, M.; Saoudi, N.; Baraibar, I.; Salva, F.; Tabernero, J.; Élez, E. Treatment of BRAF-V600E mutant metastatic colorectal cancer: New insights and biomarkers. Expert Rev. Anticancer Ther. 2023, 23, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, J.; Grothey, A.; Van Cutsem, E.; Yaeger, R.; Wasan, H.; Yoshino, T.; Desai, J.; Ciardiello, F.; Loupakis, F.; Hong, Y.S.; et al. Encorafenib Plus Cetuximab as a New Standard of Care for Previously Treated BRAF V600E-Mutant Metastatic Colorectal Cancer: Updated Survival Results and Subgroup Analyses from the BEACON Study. J. Clin. Oncol. 2021, 39, 273–284. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Reddy, S.M.; Reuben, A.; Wargo, J.A. Influences of BRAF Inhibitors on the Immune Microenvironment and the Rationale for Combined Molecular and Immune Targeted Therapy. Curr. Oncol. Rep. 2016, 18, 42. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tian, J.; Chen, J.H.; Chao, S.X.; Pelka, K.; Giannakis, M.; Hess, J.; Burke, K.; Jorgji, V.; Sindurakar, P.; Braverman, J.; et al. Combined PD-1, BRAF and MEK inhibition in BRAFV600E colorectal cancer: A phase 2 trial. Nat. Med. 2023, 29, 458–466. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Morris, V.K.; Parseghian, C.M.; Escano, M.; Johnson, B.; Raghav, K.P.S.; Dasari, A.; Huey, R.; Overman, M.J.; Willis, J.; Lee, M.S.; et al. Phase I/II trial of encorafenib, cetuximab, and nivolumab in patients with microsatellite stable (MSS), BRAFV600E metastatic colorectal cancer. J. Clin. Oncol. 2022, 40, 3598. [Google Scholar] [CrossRef]
- Corcoran, R.; Giannakis, M.; Allen, J.; Chen, J.; Pelka, K.; Chao, S.; Meyerhardt, J.; Enzinger, A.; Enzinger, P.; McCleary, N.; et al. SO-26 clinical efficacy of combined BRAF, MEK, and PD-1 inhibition in BRAFV600E colorectal cancer patients. Ann. Oncol. 2020, 31, S226–S227. [Google Scholar] [CrossRef]
- Tabernero, J.; Geel, R.V.; Guren, T.K.; Yaeger, R.D.; Spreafico, A.; Faris, J.E.; Yoshino, T.; Yamada, Y.; Kim, T.W.; Bendell, J.C.; et al. Phase 2 results: Encorafenib (ENCO) and cetuximab (CETUX) with or without alpelisib (ALP) in patients with advanced BRAF-mutant colorectal cancer (BRAFm CRC). J. Clin. Oncol. 2016, 34, 3544. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Di Nicolantonio, F.; Schrock, A.B.; Lee, J.; Tejpar, S.; Sartore-Bianchi, A.; Hechtman, J.F.; Christiansen, J.; Novara, L.; Tebbutt, N.; et al. ALK, ROS1, and NTRK Rearrangements in Metastatic Colorectal Cancer. J. Natl. Cancer Inst. 2017, 109, djx089. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, Z.W.; Ou, Q.; Wu, X.; Nagasaka, M.; Shao, Y.; Ou, S.I.; Yang, Y. NTRK fusion positive colorectal cancer is a unique subset of CRC with high TMB and microsatellite instability. Cancer Med. 2022, 11, 2541–2549. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hong, D.S.; DuBois, S.G.; Kummar, S.; Farago, A.F.; Albert, C.M.; Rohrberg, K.S.; van Tilburg, C.M.; Nagasubramanian, R.; Berlin, J.D.; Federman, N.; et al. Larotrectinib in patients with TRK fusion-positive solid tumours: A pooled analysis of three phase 1/2 clinical trials. Lancet Oncol. 2020, 21, 531–540. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Doebele, R.C.; Drilon, A.; Paz-Ares, L.; Siena, S.; Shaw, A.T.; Farago, A.F.; Blakely, C.M.; Seto, T.; Cho, B.C.; Tosi, D.; et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: Integrated analysis of three phase 1–2 trials. Lancet Oncol. 2020, 21, 271–282, Erratum in Lancet Oncol. 2020, 21, e70. https://doi.org/10.1016/S1470-2045(20)30029-2. Erratum in Lancet Oncol. 2020, 21, e341. https://doi.org/10.1016/S1470-2045(20)30345-4. Erratum in Lancet Oncol. 2020, 21, e372. https://doi.org/10.1016/S1470-2045(20)30382-X. Erratum in Lancet Oncol. 2021, 22, e428. https://doi.org/10.1016/S1470-2045(21)00538-6. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cho, B.C.; Doebele, R.C.; Lin, J.; Nagasaka, M.; Baik, C.; Van Der Wekken, A.; Velcheti, V.; Lee, K.H.; Liu, S.; Solomon, B.; et al. MA11.07 phase 1/2 TRIDENT-1 study of repotrectinib in patients with ROS1+ or NTRK+ advanced solid tumors. J. Thorac. Oncol. 2021, 16, S174–S175. [Google Scholar] [CrossRef]
- Papadopoulos, K.P.; Borazanci, E.; Shaw, A.T.; Katayama, R.; Shimizu, Y.; Zhu, V.W.; Sun, T.Y.; Wakelee, H.A.; Madison, R.; Schrock, A.B.; et al. Phase I First-in-human Study of Taletrectinib (DS-6051b/AB-106), a ROS1/TRK Inhibitor, in Patients with Advanced Solid Tumors. Clin. Cancer Res. 2020, 26, 4785–4794. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Okamoto, W.; Kato, T.; Hasegawa, H.; Kato, K.; Iwasa, S.; Esaki, T.; Komatsu, Y.; Masuishi, T.; Nishina, T.; et al. TRIUMPH: Primary eficacy of a phase II trial of trastuzumab (T) and pertuzumab (P) in patients (pts) with metastatic colorectal cancer (mCRC) with HER2 (ERBB2) amplification (amp) in tumour tissue or circulating tumour DNA (ctDNA): A GOZILA sub-study. Ann. Oncol. 2019, 30, v199–v200. [Google Scholar] [CrossRef]
- Raghav, K.; Siena, S.; Takashima, A.; Kato, T.; Van den Eynde, M.; Pietrantonio, F.; Komatsu, Y.; Kawakami, H.; Peeters, M.; Andre, T.; et al. Trastuzumab deruxtecan in patients with HER2-positive advanced colorectal cancer (tapur-CRC02): Primary results from a multicentre, randomised, phase 2 trial. Lancet Oncol. 2024, 25, 1147–1162. [Google Scholar] [CrossRef] [PubMed]
- Meric-Bernstam, F.; Makker, V.; Oaknin, A.; Oh, D.-Y.; Banerjee, S.; Gonzalez-Martin, A.; Jung, K.H.; Ługowska, I.; Manso, L.; Manzano, A.; et al. Efficacy and safety of trastuzumab deruxtecan in patients with HER2-expressing solid tumors: Primary results from the DESTINY-pantumor02 phase II trial. J. Clin. Oncol. 2024, 42, 47–58. [Google Scholar] [CrossRef]
- Bekaii-Saab, T.S.; Van Cutsem, E.; Tabernero, J.; Siena, S.; Yoshino, T.; Nakamura, Y.; Raghav, K.P.S.; Cercek, A.; Heinemann, V.; Adelberg, D.E.; et al. MOUNTAINEER-03: Phase 3 study of tucatinib, trastuzumab, and mFOLFOX6 as first-line treatment in HER2+ metastatic colorectal cancer—Trial in progress. J. Clin. Oncol. 2023, 41, TPS261. [Google Scholar] [CrossRef]
- Chang, J.; Xu, M.; Wang, C.; Huang, D.; Zhang, Z.; Chen, Z.; Zhu, X.; Li, W. Dual HER2 targeted therapy with pyrotinib and trastuzumab in refractory HER2 positive metastatic colorectal cancer: A result from HER2-FUSCC-G study. Clin. Color. Cancer 2022, 21, 347–353. [Google Scholar] [CrossRef]
- Kopetz, S.; Murphy, D.A.; Pu, J.; Ciardiello, F.; Desai, J.; Grothey, A.; Van Cutsem, E.; Wasan, H.S.; Yaeger, R.; Yoshino, T.; et al. Molecular correlates of clinical benefit in previously treated patients (pts) with BRAF V600E-mutant metastatic colorectal cancer (mCRC) from the BEACON study. J. Clin. Oncol. 2021, 39, 3513. [Google Scholar] [CrossRef]
- Yaeger, R.; Cercek, A.; O’Reilly, E.M.; Reidy, D.L.; Kemeny, N.; Wolinsky, T.; Capanu, M.; Gollub, M.J.; Rosen, N.; Berger, M.F.; et al. Pilot trial of combined BRAF and EGFR inhibition in BRAF-mutant metastatic colorectal cancer patients. Clin. Cancer Res. 2015, 21, 1313–1320. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kopetz, S.; Guthrie, K.A.; Morris, V.K.; Lenz, H.J.; Magliocco, A.M.; Maru, D.; Yan, Y.; Lanman, R.; Manyam, G.; Hong, D.S.; et al. Randomized Trial of Irinotecan and Cetuximab with or Without Vemurafenib in BRAF-Mutant Metastatic Colorectal Cancer (SWOG S1406). J. Clin. Oncol. 2021, 39, 285–294. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Demetri, G.D.; De Braud, F.; Drilon, A.; Siena, S.; Patel, M.R.; Cho, B.C.; Liu, S.V.; Ahn, M.J.; Chiu, C.H.; Lin, J.J.; et al. Updated Integrated Analysis of the Efficacy and Safety of Entrectinib in Patients with NTRK Fusion-Positive Solid Tumors. Clin. Cancer Res. 2022, 28, 1302–1312, Erratum in Clin. Cancer Res. 2022, 28, 2196. https://doi.org/10.1158/1078-0432.CCR-22-1108. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, Q.; Wang, Q.; Wang, X.; Li, J.; Shen, L.; Peng, Z. Regorafenib, TAS-102, or fruquintinib for metastatic colorectal cancer: Any difference in randomized trials? Int. J. Color. Dis. 2020, 35, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Mauri, G.; Gori, V.; Bonazzina, E.; Amatu, A.; Tosi, F.; Bencardino, K.; Ruggieri, L.; Patelli, G.; Arena, S.; Bardelli, A.; et al. Oxaliplatin retreatment in metastatic colorectal cancer: Systematic review and future research opportunities. Cancer Treat Rev. 2020, 91, 102112. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, A.A.; Kalofonou, F.; Litsardopoulos, P.; Anastopoulou, G.G.; Kalofonos, H.P. Oxaliplatin rechallenge in metastatic colorectal cancer patients with clinically significant oxaliplatin-induced peripheral neurotoxicity. J. Peripher. Nerv. Syst. 2021, 26, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Townsend, A.R.; Bishnoi, S.; Broadbridge, V.; Beeke, C.; Karapetis, C.S.; Jain, K.; Luke, C.; Padbury, R.; Price, T.J. Rechallenge with oxaliplatin and fluoropyrimidine for metastatic colorectal carcinoma after prior therapy. Am. J. Clin. Oncol. 2013, 36, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Reddy, T.P.; Khan, U.; Burns, E.A.; Abdelrahim, M. Chemotherapy rechallenge in metastatic colon cancer: A case report and literature review. World J. Clin. Oncol. 2020, 11, 959–967. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, X.; George, G.C.; Tsimberidou, A.M.; Naing, A.; Wheler, J.J.; Kopetz, S.; Fu, S.; Piha-Paul, S.A.; Eng, C.; Falchook, G.S.; et al. Retreatment with anti-EGFR based therapies in metastatic colorectal cancer: Impact of intervening time interval and prior anti-EGFR response. BMC Cancer 2015, 15, 713. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schulz, M.S.; Wolf, S.; Struck, V.; Thomas, N.; Husman, G.; Zeuzem, S.; Koch, C.; Trojan, J.; Schnitzbauer, A.A.; Bechstein, W.O.; et al. Anti-EGFR Reintroduction and Rechallenge in Metastatic Colorectal Cancer (mCRC): A Real-World Analysis. Cancers 2022, 14, 1641. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chong, L.C.; Hardingham, J.E.; Townsend, A.R.; Piantadosi, C.; Rico, G.T.; Karapetis, C.; Padbury, R.; Maddern, G.; Roy, A.; Price, T.J. Rechallenge with Anti-EGFR Therapy in Metastatic Colorectal Cancer (mCRC): Results from South Australia mCRC Registry. Target Oncol. 2020, 15, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Rossini, D.; Dell’Aquila, E.; Lonardi, S.; Conca, E.; Del Re, M.; Busico, A.; Pietrantonio, F.; Danesi, R.; Aprile, G.; et al. Rechallenge for Patients with RAS and BRAF Wild-Type Metastatic Colorectal Cancer with Acquired Resistance to First-line Cetuximab and Irinotecan: A Phase 2 Single-Arm Clinical Trial. JAMA Oncol. 2019, 5, 343–350. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Masuishi, T.; Tsuji, A.; Kotaka, M.; Nakamura, M.; Kochi, M.; Takagane, A.; Shimada, K.; Denda, T.; Segawa, Y.; Tanioka, H.; et al. Phase 2 study of irinotecan plus cetuximab rechallenge as third-line treatment in KRAS wild-type metastatic colorectal cancer: JACCRO CC-08. Br. J. Cancer 2020, 123, 1490–1495. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tsuji, A.; Nakamura, M.; Watanabe, T.; Manaka, D.; Matsuoka, H.; Kataoka, M.; Takeuchi, M.; Ichikawa, W.; Fujii, M. Phase II Study of Third-Line Panitumumab Rechallenge in Patients with Metastatic Wild-Type KRAS Colorectal Cancer Who Obtained Clinical Benefit from First-Line Panitumumab-Based Chemotherapy: JACCRO CC-09. Target Oncol. 2021, 16, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Ciardiello, D.; Mauri, G.; Sartore-Bianchi, A.; Siena, S.; Zampino, M.G.; Fazio, N.; Cervantes, A. The role of anti-EGFR rechallenge in metastatic colorectal cancer, from available data to future developments: A systematic review. Cancer Treat Rev. 2024, 124, 102683. [Google Scholar] [CrossRef] [PubMed]
- Santini, D.; Vincenzi, B.; Addeo, R.; Garufi, C.; Masi, G.; Scartozzi, M.; Mancuso, A.; Frezza, A.M.; Venditti, O.; Imperatori, M.; et al. Cetuximab rechallenge in metastatic colorectal cancer patients: How to come away from acquired resistance? Ann. Oncol. 2012, 23, 2313–2318. [Google Scholar] [CrossRef]
- Ohhara, Y.; Shinozaki, E.; Osawa, H.; Nakamura, M.; Shindo, Y.; Shiozawa, M.; Uetake, H.; Matsumoto, H.; Ureshino, N.; Satake, H.; et al. Liquid biopsy for optimizing the rechallenge of cetuximab in metastatic colorectal cancer: Additional study of E-rechallenge trial. J. Clin. Oncol. 2019, 37, 585. [Google Scholar] [CrossRef]
- Sartore-Bianchi, A.; Pietrantonio, F.; Lonardi, S.; Mussolin, B.; Rua, F.; Crisafulli, G.; Bartolini, A.; Fenocchio, E.; Amatu, A.; Manca, P.; et al. Circulating tumor DNA to guide rechallenge with panitumumab in metastatic colorectal cancer: The phase 2 CHRONOS trial. Nat. Med. 2022, 28, 1612–1618. [Google Scholar] [CrossRef]
- Kagawa, Y.; Kotani, D.; Bando, H.; Takahashi, N.; Hamaguchi, T.; Kanazawa, A.; Kato, T.; Satake, K.A.H.; Shinozaki, E.; Sunakawa, Y.; et al. Plasma RAS dynamics and anti-EGFR rechallenge eficacy in patients with RAS/BRAF wild-type metastatic colorectal cancer: REMARRY and PURSUIT trials. J. Clin. Oncol. 2022, 40, 3518. [Google Scholar] [CrossRef]
- Martinelli, E.; Martini, G.; Famiglietti, V.; Troiani, T.; Napolitano, S.; Pietrantonio, F.; Ciardiello, D.; Terminiello, M.; Borrelli, C.; Vitiello, P.P.; et al. Cetuximab rechallenge plus avelumab in pretreated patients with RAS wild-type metastatic colorectal cancer: The phase 2 single-arm clinical CAVE trial. JAMA Oncol. 2021, 7, 1529–1535. [Google Scholar] [CrossRef]
- Napolitano, S.; De Falco, V.; Martini, G.; Ciardiello, D.; Martinelli, E.; Della Corte, C.M.; Esposito, L.; Famiglietti, V.; Di Liello, A.; Avallone, A.; et al. Panitumumab plus trifluridine-tipiracil as anti-epidermal growth factor receptor rechallenge therapy for refractory RAS wild-type metastatic colorectal cancer. JAMA Oncol. 2023, 9, 966–970. [Google Scholar] [CrossRef] [PubMed]
- Vivas, C.S.; Barrull, J.V.; Rodriguez, C.F.; Ballabrera, F.S.; Alonso-Orduna, V.; Garcia-Carbonero, R.; Losa, F.; Llavero, N.T.; Aguileria, M.S.; Herrero, F.R.; et al. 511MO—Third line rechallenge with cetuximab (Cet) and irinotecan in circulating tumor DNA (ctDNA) selected metastatic colorectal cancer (mCRC) patients: The randomized phase II CITRIC trial. Ann. Oncol. 2024, 35, S433–S434. [Google Scholar] [CrossRef]
- Rao, S.; Cunningham, D.; Price, T.; Hill, M.E.; Ross, P.J.; Tebbutt, N.; Norman, A.R.; Oates, J.; Shellito, P. Phase II study of capecitabine and mitomycin C as first-line treatment in patients with advanced colorectal cancer. Br. J. Cancer 2004, 91, 839–843. [Google Scholar] [CrossRef] [PubMed] [PubMed Central][Green Version]
- Twelves, C.; Xeloda Colorectal Cancer Group. Capecitabine as first-line treatment in colorectal cancer. Pooled data from two large, phase III trials. Eur. J. Cancer 2002, 38 (Suppl. S2), 15–20. [Google Scholar] [CrossRef] [PubMed]
- Chong, G.; Dickson, J.L.; Cunningham, D.; Norman, A.R.; Rao, S.; Hill, M.E.; Price, T.J.; Oates, J.; Tebbutt, N. Capecitabine and mitomycin C as third-line therapy for patients with metastatic colorectal cancer resistant to fluorouracil and irinotecan. Br. J. Cancer 2005, 93, 510–514. [Google Scholar] [CrossRef] [PubMed] [PubMed Central][Green Version]
- Dimou, A.; Syrigos, K.N.; Saif, M.W. Is there a role for mitomycin C in metastatic colorectal cancer? Expert Opin. Investig. Drugs. 2010, 19, 723–735. [Google Scholar] [CrossRef] [PubMed]
- Saif, M.W.; Kaley, K.; Brennan, M.; Garcon, M.C.; Rodriguez, G. Mitomycin-C and capecitabine (MIXE) as salvage treatment in patients with refractory metastatic colorectal cancer: A retrospective study. Anticancer. Res. 2013, 33, 2743–2746. [Google Scholar] [PubMed]
- Ferrarotto, R.; Machado, K.; Mak, M.P.; Shah, N.; Takahashi, T.K.; Costa, F.P.; Overman, M.J.; Kopetz, S.; Hoff, P.M. A multicenter, multinational analysis of mitomycin C in refractory metastatic colorectal cancer. Eur. J. Cancer 2012, 48, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Sobrero, A.; Dasari, A.; Aquino, J.; Lonardi, S.; Garcia-Carbonero, R.; Elez, E.; Yoshino, T.; Yao, J.; Garcia-Alfonso, P.; Kocsis, J.; et al. Health-related quality of life associated with fruquintinib in patients with metastatic colorectal cancer: Results from the FRESCO-2 study. Eur. J. Cancer 2025, 218, 115268. [Google Scholar] [CrossRef] [PubMed]
- Hofheinz, R.D.; Bruix, J.; Demetri, G.D.; Grothey, A.; Marian, M.; Bartsch, J.; Odom, D. Effect of Regorafenib in Delaying Definitive Deterioration in Health-Related Quality of Life in Patients with Advanced Cancer of Three Different Tumor Types. Cancer Manag. Res. 2021, 13, 5523–5533. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Van Cutsem, E.; Falcone, A.; Garcia-Carbonero, R.; Komatsu, Y.; Pastorino, A.; Peeters, M.; Shimada, Y.; Yamazaki, K.; Yoshino, T.; Zaniboni, A.; et al. Proxies of quality of life in metastatic colorectal cancer: Analyses in the RECOURSE trial. ESMO Open 2017, 2, e000261. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).