Abstract
Irritable Bowel Syndrome (IBS) is a disorder of gut- brain interaction characterized by recurrent abdominal pain associated with altered bowel habits. The therapeutic options for IBS patients include the use of probiotics. The aim of this study was to assess the effect of a multi-strain probiotic made up by Lactobacillus rhamnosus LR 32, Bifidobacterium lactis BL 04, and Bifidobacterium longum BB 536 (Serobioma, Bromatech s.r.l., Milano, Italy) on an in vitro model of the intestinal epithelial barrier in the presence of mucosal mediators that are released by IBS patients. IBS (n = 28; IBS with predominant diarrhea, IBS-D = 10; IBS with predominant constipation, IBS-C = 9; and IBS with mixed bowel habits, IBS-M = 9) patients, diagnosed according to the Rome IV criteria, and asymptomatic controls (ACs, n = 7) were enrolled. Mucosal mediators that were spontaneously released by colonic biopsies were collected (supernatants). Two doses of Serobioma were tested with/without IBS/AC mediators. RNA was extracted from Caco-2 cells to evaluate the tight junction (TJ) expression. Serobioma (106 CFU/mL) significantly reinforced the Caco-2 monolayer compared to growth medium alone (p < 0.05). IBS supernatants significantly increased Caco-2 paracellular permeability compared to the AC supernatants. The co-incubation of Caco-2 cells with IBS supernatants and Serobioma (106 CFU/mL) avoided the paracellular permeability alterations that were induced by IBS supernatants alone (p < 0.001), and, in particular, IBS-D and IBS-M ones. The co-incubation of Serobioma (106 CFU/mL) and IBS-D supernatants significantly increased ZO-1 expression compared to Caco-2 cells incubated with supernatants alone (p < 0.05), as confirmed via qPCR analyses. Serobioma (106 CFU/mL) counteracts the paracellular permeability changes that are induced by IBS supernatants, in particular IBS-D and IBS-M supernatants, likely modulating ZO-1 expression.
1. Introduction
Irritable Bowel Syndrome (IBS) is a disorder of gut- brain interaction characterized by recurrent abdominal pain associated with altered bowel habits, including diarrhea (IBS-D), constipation (IBS-C), or a combination of both (IBS-M). A fourth subtype is the unclassified type (IBS-U). IBS affects approximately 10–15% of the global population and poses a significant healthcare burden due to the considerable impact on patients’ quality of life, the cumbersome diagnosis due to the absence of biomarkers, and the heterogeneity of the condition [1,2].
Although the precise pathophysiological mechanisms of IBS remain elusive, it is widely recognized as a multifactorial disorder involving a complex interplay of altered gut motility, visceral hypersensitivity, and psychosocial factors [3]. More recent research has highlighted the role of gut microbiota dysbiosis, intestinal permeability changes, and altered production of short-chain fatty acids (SCFAs) in IBS’s pathophysiology [4,5,6,7].
Increased intestinal permeability has garnered particular interest in the context of IBS, since it can allow for the translocation of microbial products into the lamina propria, which may trigger low-grade inflammation, and also into the bloodstream, contributing to IBS symptom development [7,8].
Given the multifaceted nature of IBS, a comprehensive approach to treatment is required, often combining dietary interventions, probiotics, pharmacotherapy, and psychological therapies to address the varied symptoms that are experienced by patients [9].
Probiotics are defined by the World Health Organization as “live microorganisms that, when administered in adequate amounts, confer a health benefit on the host” [10]. Among the proposed mechanisms of action of probiotics is gut barrier reinforcement [10], which can be achieved through several pathways: the competitive inhibition of pathogen adhesion, production of bioactive metabolites, stimulation of digestive enzymes, and synthesis of short-chain and branched-chain fatty acids [11,12].
Lactobacilli and Bifidobacteria are important components of the human gut microbiota and are commonly used as probiotics [13]. B. longum BB536 is a highly regarded probiotic bacterial strain with well-established benefits. Specifically, this strain plays a role in maintaining a balanced gut microbiota, can positively influence the immune response, and supports tight junction stability via exopolysaccharide and butyrate production [14,15,16]. A randomized, double-blind, placebo-controlled, and multicenter trial demonstrated that B. longum BB536, when added to standard treatment, improved symptoms in patients with mild to moderately active ulcerative colitis [17]. L. rhamnosus LR32 has shown immunomodulatory properties in vitro [18]. In an animal model, it helped restore the balance of the gut microbial community, enhanced the expression of tight junction proteins in both the ileum and hypothalamus, and supported the expression of genes involved in central 5-HT metabolism [19]. B. lactis BL04 is widely used in probiotic formulations with beneficial effects on gastrointestinal (GI) symptoms and on gut microbiota composition [20,21,22]. A randomized, double-blind, and placebo-controlled trial reported that B. lactis BL04 reduced the risk of upper respiratory tract infection in healthy subjects [23].
The aims of the present study were to characterize the effect of Serobioma, a multi-strain probiotic comprising L. rhamnosus LR32, B. lactis BL04, and B. longum BB 536, on an in vitro model of the intestinal epithelial barrier in the presence of mucosal mediators that are released by IBS patients compared to that of asymptomatic controls. In addition, molecular analyses were performed to evaluate the gene expression of zonula occludens-1 (ZO-1), occludin, and junctional adhesion molecule-A (JAM-A) to assess their possible involvement in permeability changes.
2. Results
2.1. Demographical Characteristics of Study Subjects
Table 1 shows the demographic characteristics of the study subjects. The IBS group was significantly younger than the AC group, and the same was the case for IBS-D and IBS-M patients. IBS-D patients were also significantly younger than IBS-C ones. A significantly higher percentage of women was present in the IBS-C group compared to the AC group (p < 0.05) and the other IBS subgroups (p = 0.05).

Table 1.
Demographic and clinical characteristics of study subjects.
The IBS subtypes were comparable for abdominal pain and distension, except for the abdominal distention severity score, which was significantly higher in IBS-C patients compared to IBS-D ones.
The quality-of-life score was significantly higher in the AC group compared to IBS-M and IBS-D subtypes. In addition, IBS-D patients achieved the lowest quality of life score among the three IBS subtypes.
2.2. Assessment of pH and Cell Viability of Caco-2
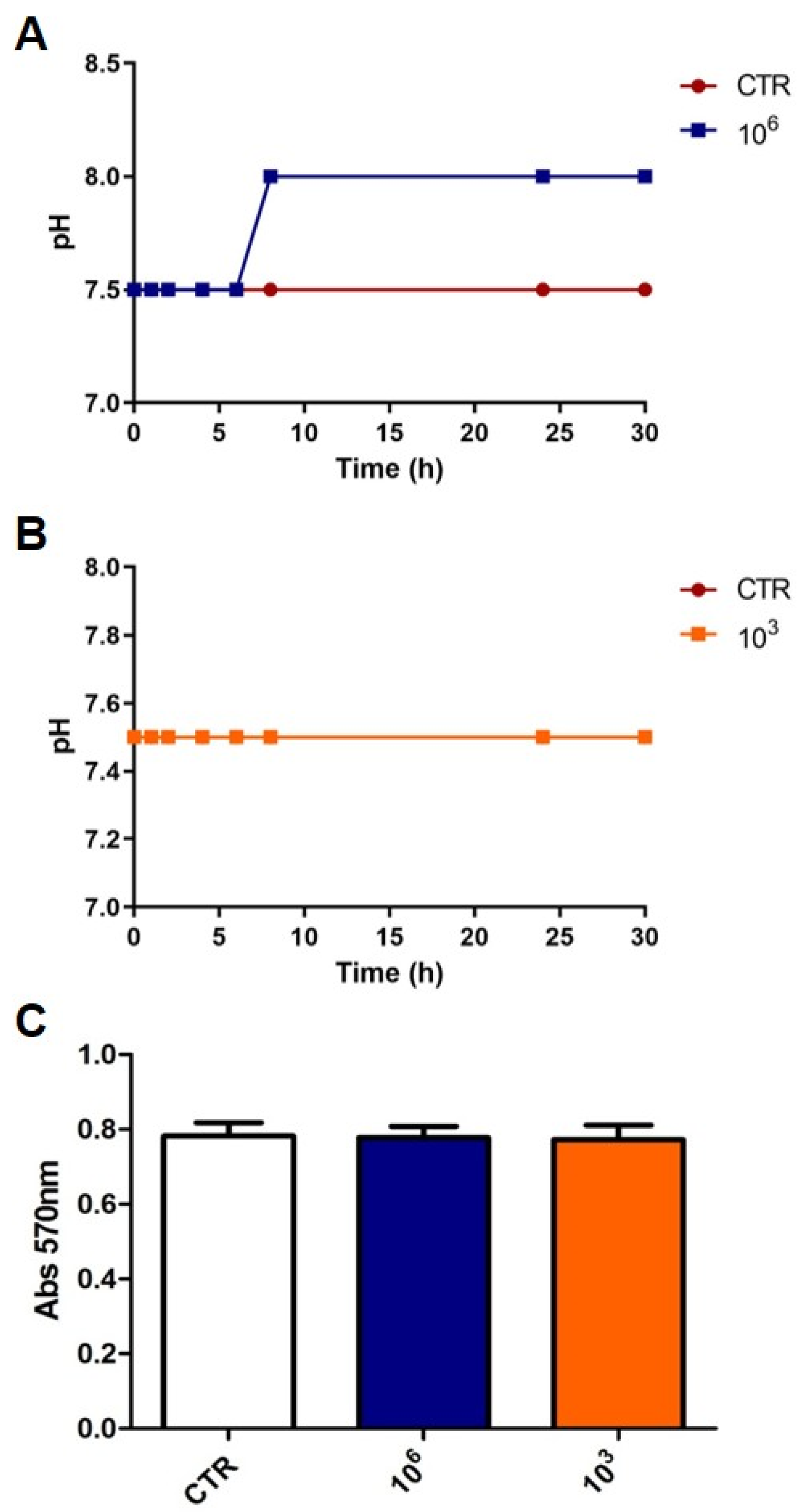
In order to define two doses of Serobioma for further testing on Caco-2 cells, preliminary experiments were carried out by evaluating the effect of different doses on pH levels and Caco-2 viability. Thus, a change in these parameters could affect the permeability results.
As we have previously shown that a subset of IBS supernatants, containing the mucosal mediators that are spontaneously released by IBS biopsies, caused increased paracellular permeability in Caco-2 cells compared to supernatants from healthy individuals after 6 h of incubation [6], to choose the two doses of Serobioma, we focused on those that did not alter the pH or Caco-2 viability after 6 h of incubation. The highest dose of Serobioma that did not change these two parameters was 106 CFU/mL, from now on referred to as S1 (Figure 1A–C). A second dose of 103 CFU/mL, from now on referred to as S2, was selected arbitrary, and as shown in Figure 1, it did not influence the medium’s pH (Figure 1B) or the viability of the Caco-2 cells (Figure 1C).
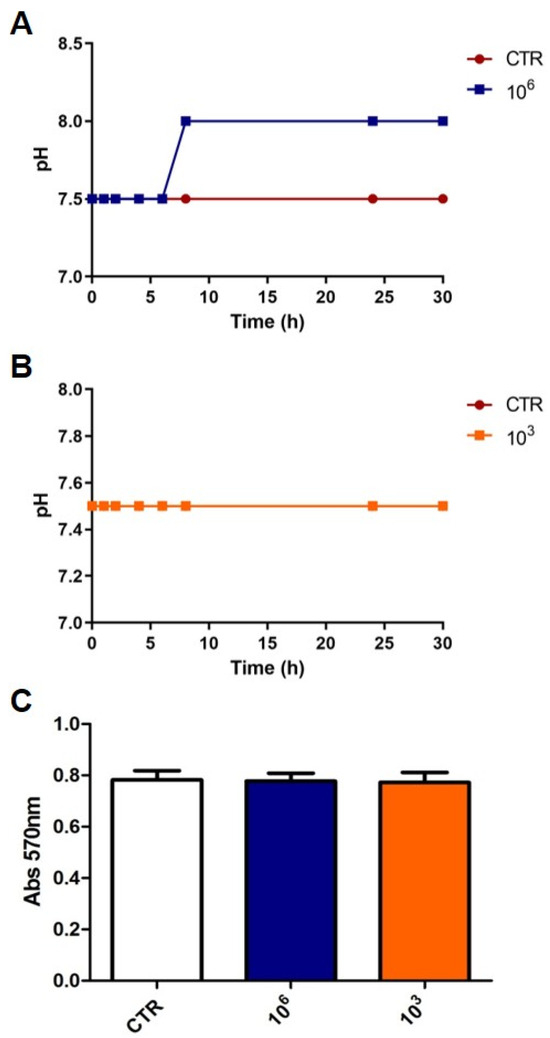
Figure 1.
Effect of Serobioma on pH of medium and Caco-2 viability. (A,B) pH evaluation after 2, 4, 6, 8, 24, and 30 h of cell incubation with or without Serobioma (106 CFU/mL and 103 CFU/mL, respectively). (C) Caco-2 viability assay after 6 h of incubation with or without Serobioma (106 and 103 CFU/mL). CTR: Caco-2 cells incubated with medium alone (n = 4); 106: Caco-2 cells incubated with 106 CFU/mL (n = 2); 103: Caco-2 cells incubated with 103 CFU/mL (n = 2). Each condition was tested in triplicate.
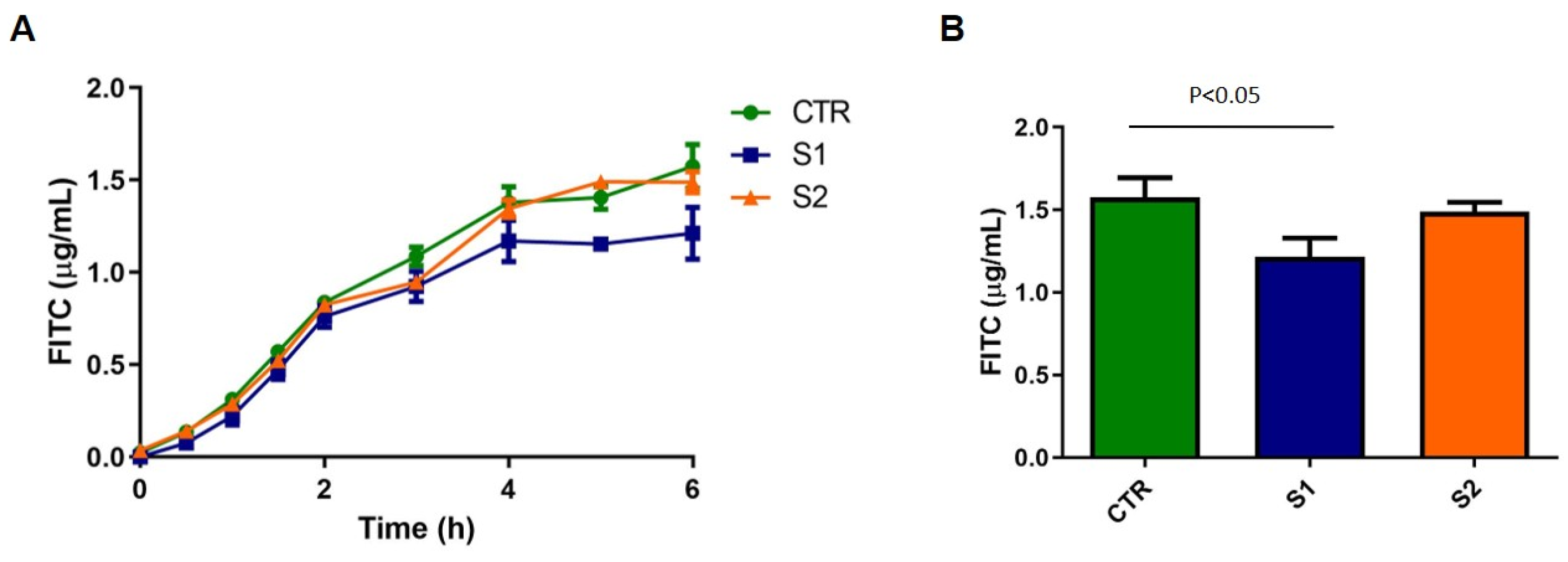
2.3. Effect of Serobioma on Caco-2 Paracellular Permeability
Caco-2 cells were incubated with the medium alone or with the two concentrations of Serobioma, S1 and S2. Compared to the Caco-2 cells that were incubated with the medium alone, S1 significantly reinforced Caco-2 monolayer (p < 0.05, Figure 2).
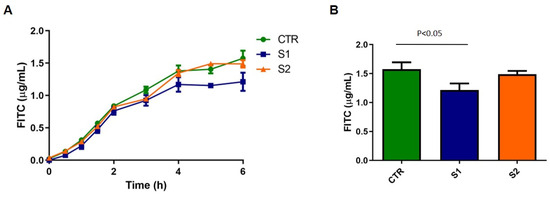
Figure 2.
Effect of Serobioma on Caco-2 paracellular permeability. (A) Paracellular permeability changes during 6 h of Caco-2 incubation with/without Serobioma. (B) Paracellular permeability changes at 6 h of Caco-2 incubation with/without Serobioma. CTR: Caco-2 cells incubated with medium alone (n = 7); S1: Caco-2 cells incubated with 106 CFU/mL (n = 6); S2: Caco-2 cells incubated with 103 CFU/mL (n = 4).
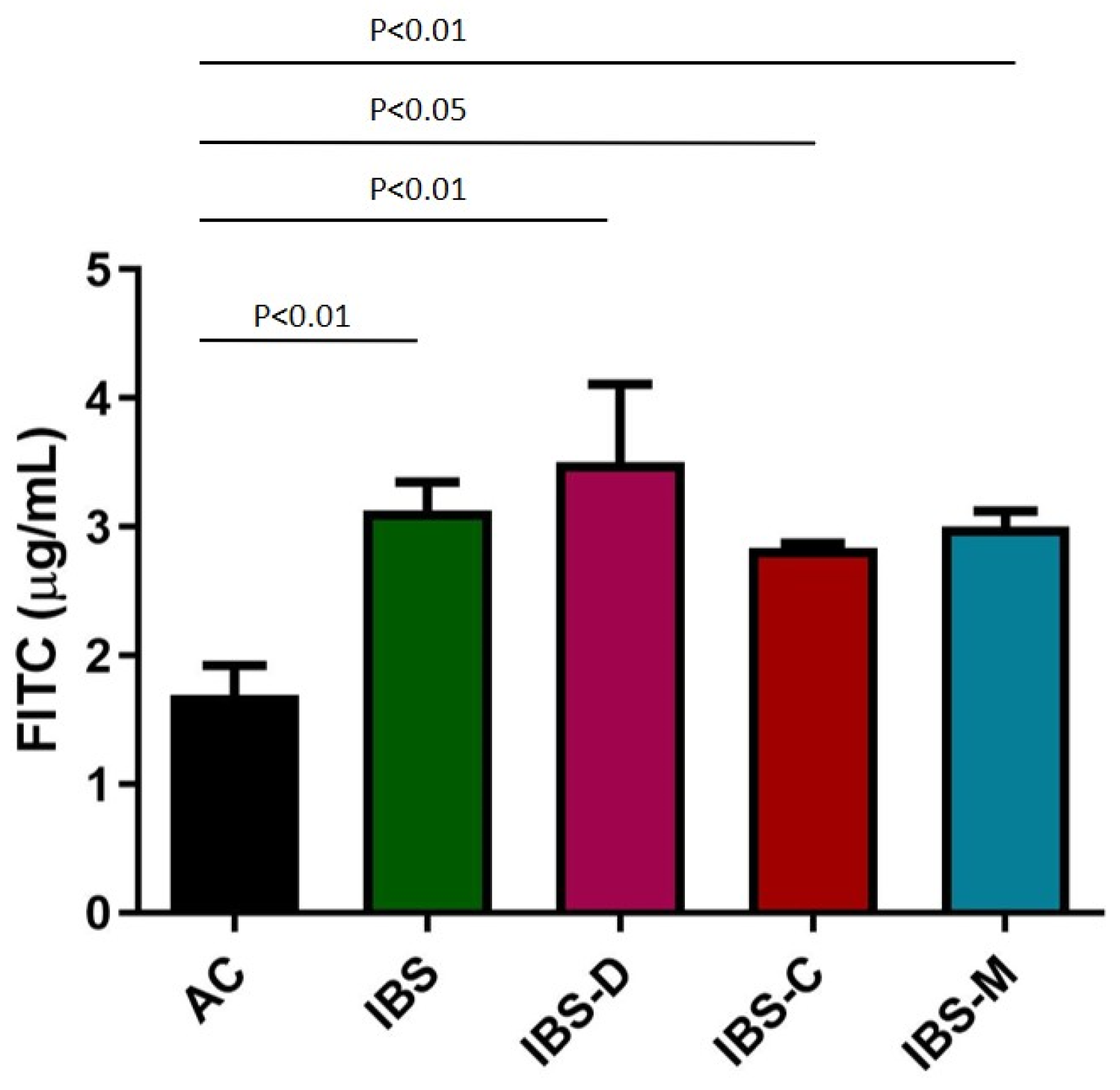
2.4. Effect of IBS Supernatants on Caco-2 Paracellular Permeability
IBS supernatants caused a significant increase in paracellular permeability compared to the AC group after 6 h of incubation (p < 0.01). When analyzing IBS subtypes based on bowel habits, all subgroups showed a significant increase in Caco-2 paracellular permeability compared to the AC group (Figure 3).
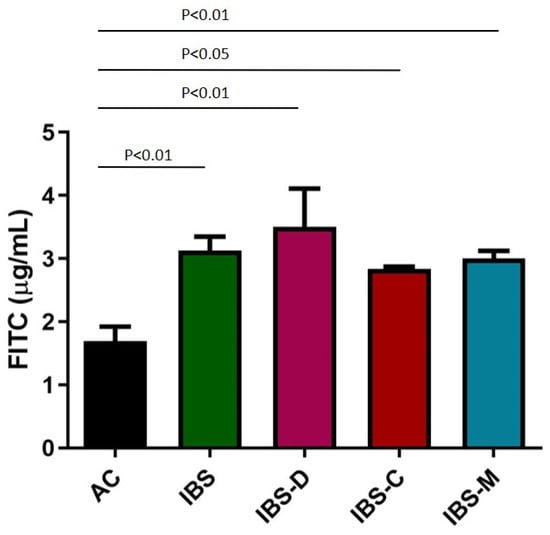
Figure 3.
Effect of AC/IBS supernatants on Caco-2 paracellular permeability after 6 h of incubation. AC: Caco-2 cells incubated with AC supernatants (n = 7); IBS: Caco-2 cells incubated with IBS-D supernatants (n = 10) plus Caco-2 cells incubated with IBS-C supernatants (n = 9) plus Caco-2 cells incubated with IBS-M supernatants (n = 9); IBS-D: Caco-2 cells incubated with IBS-D supernatants (n = 10); IBS-C: Caco-2 cells incubated with IBS-C supernatants (n = 9); and IBS-M: Caco-2 cells incubated with IBS-M supernatants (n = 9).
2.5. Effect of Serobioma and IBS Supernatants on Caco-2 Paracellular Permeability
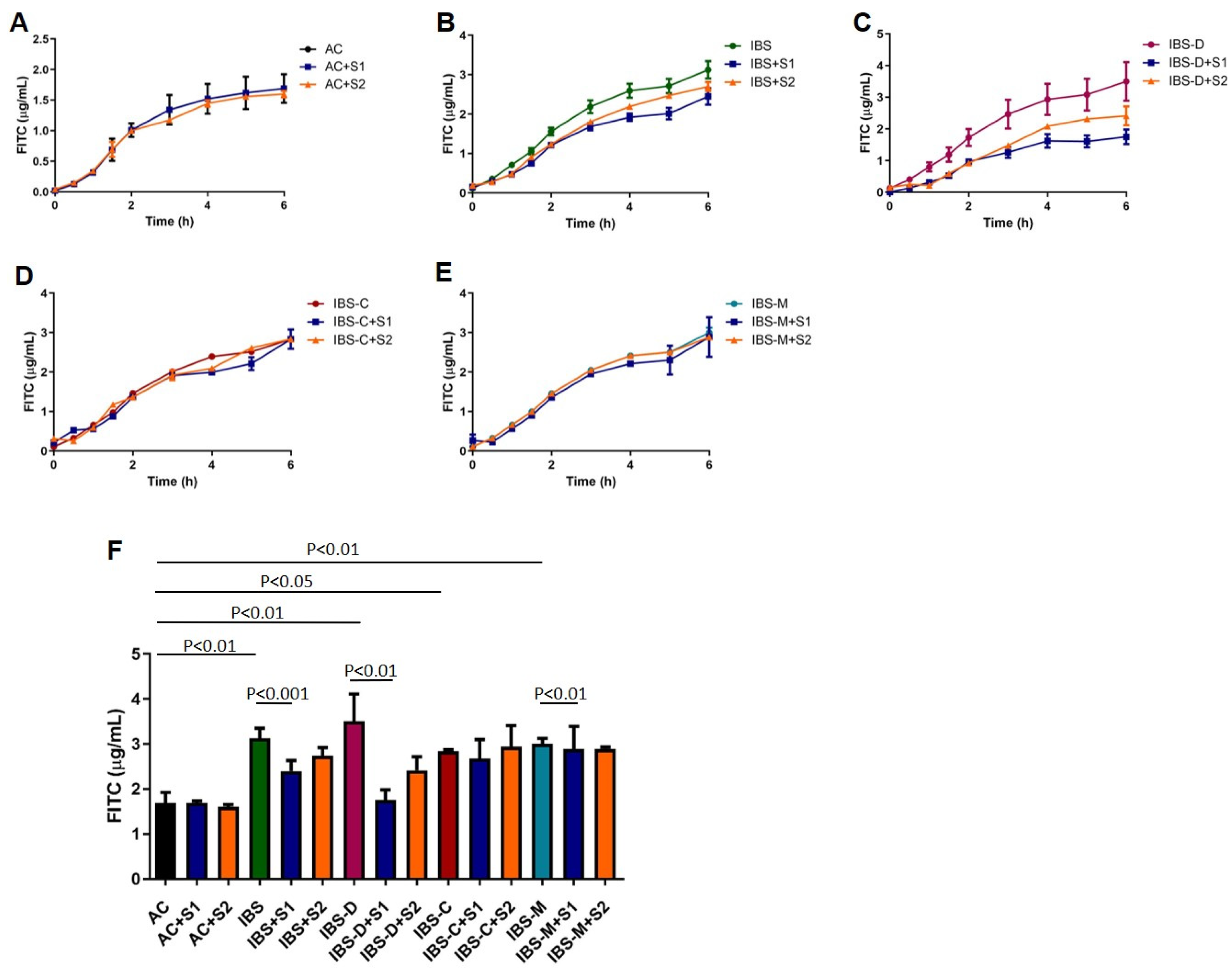
The effect of co-incubation of Serobioma and AC/IBS supernatants over time is shown in Figure 4. The highest dose of Serobioma (S1) significantly reduced the increase in paracellular permeability that was induced by the IBS supernatants (IBS vs. IBS+S1, p < 0.001). Regarding IBS subtypes, the highest dose of Serobioma significantly reduced the increase in paracellular permeability that was induced by the IBS-D (p < 0.01) and IBS-M (p < 0.01) supernatants, while no effect was observed with IBS-C ones.
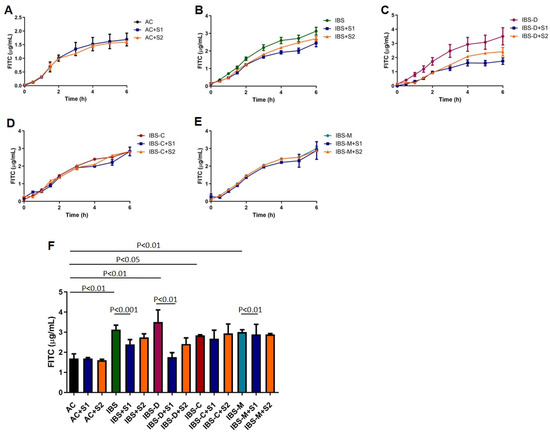
Figure 4.
Effect of Serobioma being co-incubated with AC/IBS supernatants. (A) Effect of co-incubation of AC and Serobioma over time; (B) effect of co-incubation of IBS (IBS-D plus IBS-C plus IBS-M) and Serobioma over time; (C) effect of co-incubation of IBS-D and Serobioma over time; (D) effect of co-incubation of IBS-C and Serobioma over time; (E) effect of co-incubation of IBS-M and Serobioma over time; (F) depiction of paracellular permeability changes after 6 h of incubation. AC: Caco-2 cells incubated with AC supernatants; AC+S1: Caco-2 cells incubated with AC supernatants and 106 CFU/mL of Serobioma; AC+S2: Caco-2 cells incubated with AC supernatants and 103 CFU/mL of Serobioma; IBS: Caco-2 cells incubated with IBS-D supernatants plus Caco-2 cells incubated with IBS-C supernatants plus Caco-2 cells incubated with IBS-M supernatants; IBS+S1: Caco-2 cells incubated with IBS supernatants and 106 cell/well Serobioma; IBS+S2: Caco-2 cells incubated with IBS supernatants and 103 CFU/mL of Serobioma; IBS-D: Caco-2 cells incubated with IBS-D supernatants; IBS-D+S1: Caco-2 cells incubated with IBS-D supernatants and 106 CFU/mL of Serobioma; IBS-D+S2: Caco-2 cells incubated with IBS-D supernatants and 103 CFU/mL of Serobioma; IBS-C: Caco-2 cells incubated with IBS-C supernatants; IBS-C+S1: Caco-2 cells incubated with IBS-C supernatants and 106 CFU/mL of Serobioma; IBS-C+S2: Caco-2 cells incubated with IBS-C supernatants and 103 CFU/mL of Serobioma; IBS-M: Caco-2 cells incubated with IBS-M supernatants; IBS-M+S1: Caco-2 cells incubated with IBS-M supernatants and 106 CFU/mL of Serobioma; and IBS-M+S2: Caco-2 cells incubated with IBS-M supernatants and 103 CFU/mL of Serobioma.
2.6. Effect of Serobioma with/Without AC/IBS Supernatants on ZO-1, Occludin, and JAM-A Expression
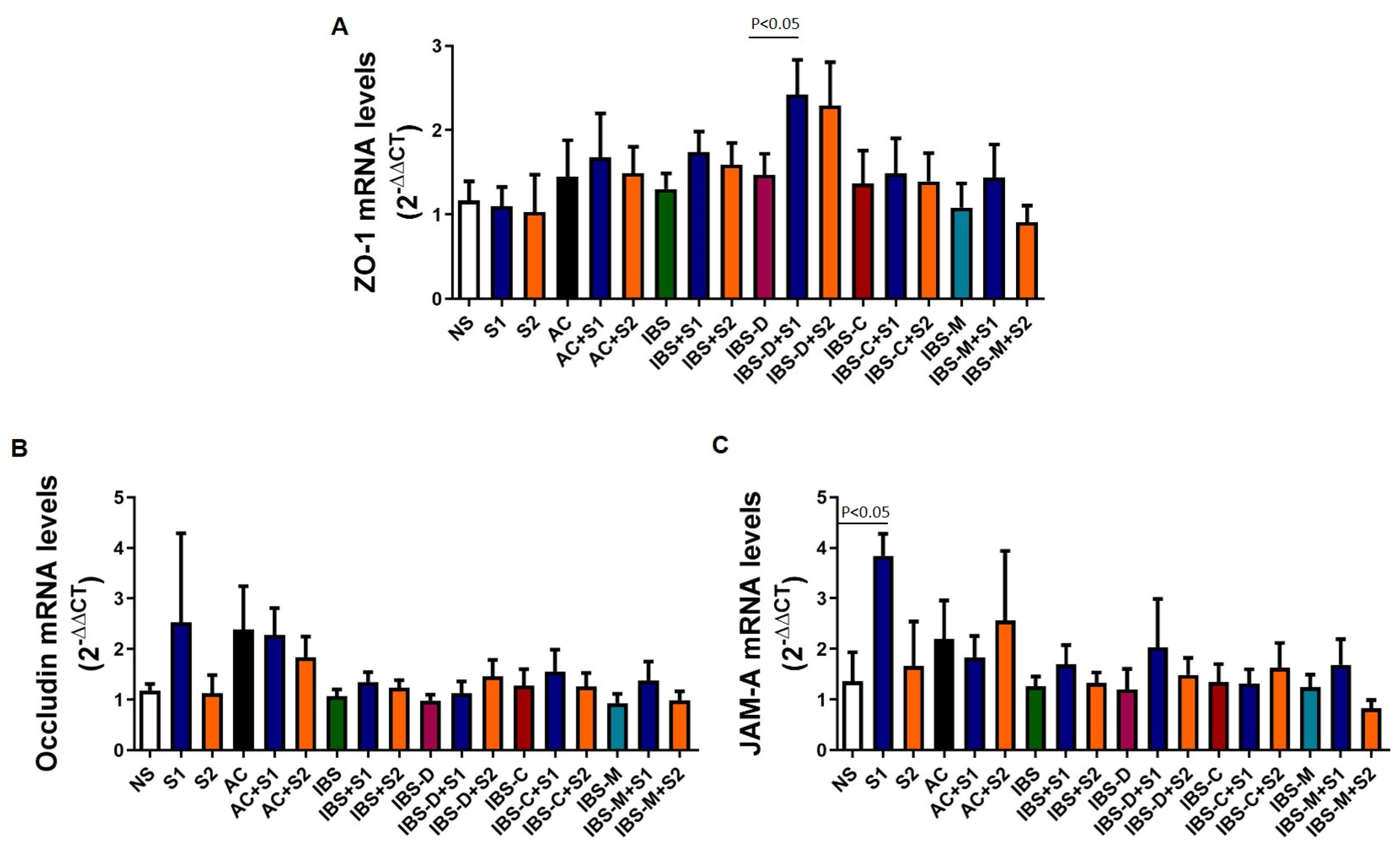
To investigate the potential molecular mechanisms of Serobioma in reversing the paracellular permeability changes induced by IBS supernatants, qPCR analyses were performed on RNA extracted from Caco-2 cells at the end of the permeability experiments (Figure 5).The co-incubation of Serobioma and AC/IBS supernatants induced an increase in the expression of ZO-1 compared to supernatants alone, although this difference only reached statistical significance for S1 that was co-incubated with IBS-D supernatants (Figure 5A). The highest dose of Serobioma also induced an increase in occludin expression with and without IBS supernatants, although statistical significance was not reached for any of the conditions (Figure 5B). The highest dose of Serobioma induced a significant increase in JAM-A expression compared to Caco-2 cells that were incubated with growth medium alone, while when co-incubated with IBS-D and IBS-M supernatants, it induced an increase in JAM-A expression which did not reach statistical significance (Figure 5C).
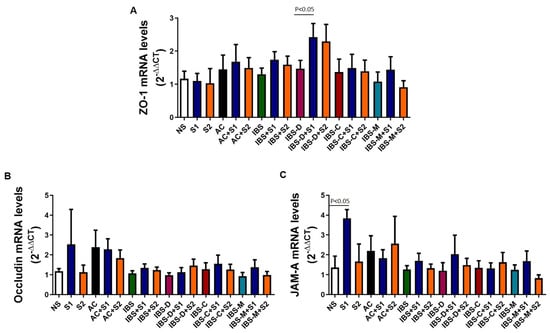
Figure 5.
Effect of Serobioma with/without AC/IBS supernatants on ZO-1 (A), occludin (B), and JAM-A (C) expression. NS: Caco-2 cells incubated with medium alone; S1: Caco-2 cells incubated with 106 CFU/mL of Serobioma; S2: Caco-2 cells incubated with 103 CFU/mL of Serobioma. AC: Caco-2 cells incubated with AC supernatants; AC+S1: Caco-2 cells incubated with AC supernatants and 106 CFU/mL of Serobioma; AC+S2: Caco-2 cells incubated with AC supernatants and 103 CFU/mL of Serobioma; IBS: Caco-2 cells incubated with IBS-D supernatants plus Caco-2 cells incubated with IBS-C supernatants plus Caco-2 cells incubated with IBS-M supernatants; IBS+S1: Caco-2 cells incubated with IBS supernatants and 106 cell/well Serobioma; IBS+S2: Caco-2 cells incubated with IBS supernatants and 103 CFU/mL of Serobioma; IBS-D: Caco-2 cells incubated with IBS-D supernatants; IBS-D+S1: Caco-2 cells incubated with IBS-D supernatants and 106 CFU/mL of Serobioma; IBS-D+S2: Caco-2 cells incubated with IBS-D supernatants and 103 CFU/mL of Serobioma; IBS-C: Caco-2 cells incubated with IBS-C supernatants; IBS-C+S1: Caco-2 cells incubated with IBS-C supernatants and 106 CFU/mL of Serobioma; IBS-C+S2: Caco-2 cells incubated with IBS-C supernatants and 103 CFU/mL of Serobioma; IBS-M: Caco-2 cells incubated with IBS-M supernatants; IBS-M+S1: Caco-2 cells incubated with IBS-M supernatants and 106 CFU/mL of Serobioma; and IBS-M+S2: Caco-2 cells incubated with IBS-M supernatants and 103 CFU/mL of Serobioma. Expression was calculated considering corresponding condition without Serobioma as calibrator (e.g., the expression of “IBS-D+S1” was calculated using “IBS-D” as calibrator).
3. Discussion
In the present study, we demonstrated that 106 CFU/mL of Serobioma prevents the paracellular permeability changes that are induced by IBS supernatants, particularly the IBS-D and IBS-M subtypes, on the Caco-2 monolayer after 6 h of incubation. In exploring the molecular mechanisms underlying this effect, we found that S1 induced an increase in the gene expression of ZO-1 in Caco-2 cells that were incubated with IBS-D supernatants compared to supernatants alone.
The intestinal barrier is crucial for protecting the body from harmful antigens and maintaining homeostasis. Growing evidence indicates that the intestinal barrier is compromised, leading to increased permeability, in several intestinal and extra-intestinal conditions, including IBS [24]. The exact role of changes in the intestinal permeability in IBS remains debated, although it can be hypothesized that barrier disruption allows luminal antigens to activate the immune system, causing low-grade inflammation and altered neuro-immune interactions, which likely contribute to symptom development. Interestingly, among the therapeutic options for IBS patients, probiotics are noteworthy [25]. Certain strains of probiotics have been shown to restore barrier function by modulating TJ proteins and reducing permeability [26].
Here, we demonstrated that the use of Serobioma can avoid the paracellular permeability increase that is induced by mucosal mediators that are released by IBS biopsies, particularly, IBS-D. We also found that Serobioma induced an increase in ZO-1 expression, suggesting that this could be one of the molecular mechanisms underlying the Serobioma effect. ZO-1 is a key protein involved in maintaining the integrity of TJs in the intestinal epithelium, playing a crucial role in regulating intestinal permeability. Using the same translational model based on Caco-2 cells and IBS mucosal mediators, previous evidence demonstrated that ZO-1 expression was reduced by IBS mediators [8,9]. Moreover, an altered expression or localization of ZO-1 has been reported in jejunal and colonic biopsies of IBS patients, suggesting an important role for this TJ protein in IBS [27,28].
Using the same probiotic formulation, previously published studies reported effects in the form of reinforcement of the Caco-2 monolayer by enhancing the expression of various TJ proteins, including ZO-1 [16]. In addition, the same research group demonstrated that in a co-culture model based on Caco-2 cells and HMC-1.2 (a mast cell line), Serobioma reduced cytokine production and barrier alterations, induced by LPS [29]. In our study, we used the mucosal mediators that are spontaneously released by IBS biopsies, which include several mast cell mediators (e.g., histamine, proteases, serotonin, cytokines, etc.), thus providing a stronger rationale for further evaluation of Serobioma in IBS [30].
Our study has some limitations: first, the use of an in vitro model is a highly simplified version of the intestinal environment; second, since this was a pilot study, only a limited number of samples were analyzed; third, there were differences in the age and percentage of females between the groups of subjects enrolled; fourth, we cannot exclude that diet may have a role in the composition of IBS supernatants and therefore in the results obtained, so we cannot generalize the obtained effect to geographical regions that are different from ours. However, this study has several important strengths: it utilized mediators that are spontaneously released from patient biopsies, which include molecules that are present in the gut; the preliminary pH tests ensured that the probiotic doses used during the chosen incubation period, did not alter the pH of the growth medium, thus avoiding a major error in the assessment of changes in permeability; finally, a control group of subjects was included to compare the results obtained in the IBS patient group.
Understanding the underlying mechanisms, particularly those related to the gut microbiota and intestinal paracellular permeability, remains an area of active research on the topic of IBS, with the aim of developing more targeted therapies. The results of this study provide an important starting point for future research aimed at clarifying the therapeutic effects of Serobioma in IBS.
4. Materials and Methods
4.1. Subjects
Consecutive patients with IBS (n = 28; IBS-D = 10; IBS-C = 9; and IBS-M = 9), diagnosed according to the Rome IV criteria, and asymptomatic controls (ACs, n = 7) were recruited at the Department of Medical and Surgical Sciences, University of Bologna (Italy). ACs were selected from subjects undergoing colonoscopy for colorectal cancer screening or following polypectomy and were individuals who met the exclusion criteria and had no gastrointestinal symptoms.
The exclusion criteria for all included subjects were as follows: any relevant organic, systemic, or metabolic disease; organic bowel diseases, including celiac disease or inflammatory bowel disease (Crohn’s disease, diverticular disease, ulcerative colitis, infectious colitis, ischemic colitis, microscopic colitis); previous major abdominal surgeries; patients consuming probiotics or receiving topical antibiotic therapy within the past month; and the use of corticosteroids, non-steroidal anti-inflammatory drugs, serotonergic agents, including 5-HT3 receptor antagonists (i.e., granisetron, ondansetron) and 5-HT4 receptor agonists (i.e., prucalopride), and tricyclic anti-depressants. In each subject, during the colonoscopy, four biopsies were taken at the level of the proximal descending colon to collect spontaneously released mediators.
All participants gave written informed consent. The protocol was approved by the Ethic Committee of Area Vasta Emilia Centro (CE-AVEC, approval identification number: 822/2021/Sper/AOUBo) and conducted in accordance with the Declaration of Helsinki.
4.2. Symptom Questionnaires
At the time of biopsy collection, patients completed a modified Italian version of the Bowel Disease Questionnaire (BDQ) to score the frequency and severity of their abdominal pain and bloating in the past 2 weeks prior to the interview [7].
Symptom severity was graded as 0–4 according to its impact on patients’ daily activities: 0—absent; 1—mild (not influencing activities); 2—relevant (diverting from, but not urging modification of, activities); 3—severe (influencing activities markedly enough to urge modifications); 4—extremely severe (precluding daily activities). The frequency was graded as 0–4 according to the following scale: 0—absent; 1—up to 1 day/week; 2—2 or 3 days/week; 3—4–6 days per week; 4—daily. The quality of life, as an expression of general well-being, was monitored using a 0–10 visual analog scale (0 = “I have never felt so bad”; 10 = “I have never felt so good”).
4.3. Mucosal Mediator Collection
Mucosal mediators spontaneously released from colonic biopsies, were collected according to a previously validated method [7]. Briefly, the biopsies were immediately immersed in plastic tubes containing 1 mL of Hepes–Krebs buffer solution (pH 7.4), weighed, and volume-adjusted to incubate 15 mg of biopsies in 1 mL of buffer. Incubation was carried out under continuous oxygenation at 37 °C for 25 min. Tubes were centrifuged at 200× g at 4 °C for 7 min, and supernatants containing mediators (called supernatants) were aliquoted and stored at −20 °C until the analysis. Before treatment, supernatants were filtered with 0.22 µm filters (Millex-GP, Millipore, Milan, Italy).
4.4. Caco-2 Cell Culture
A previously published protocol was followed to establish the in vitro model of the intestinal epithelial barrier based on the human intestinal epithelial cell line Caco-2 (EATCC, Port Down, UK) [7]. Briefly, cells were seeded onto porous filters (12-well Transwell Clear, 0.40 μm porosity, 1.1 cm of diameter; Corning, Milan, Italy) at a density of 200,000 cells/filter and cultured in Dulbecco’s modified Eagle’s medium (DMEM) (Gibco, Thermo Scientific, Milan, Italy), supplemented with 2 mmol/L L-glutamine (Gibco, Thermo Scientific, Milan, Italy), 50 IU/mL penicillin, 50 μg/mL streptomycin (Gibco, Thermo Scientific, Milan, Italy), and 10% heat-inactivated fetal bovine serum (FBS) (Gibco, Thermo Scientific, Milan, Italy) at 37 °C and using 5% of CO2. The culture medium was changed every 2 days. Using a volt-ohm-meter (Millicel® ERS-2, Millipore, Milan, Italy), we measured the trans-epithelial cell resistance (TEER) every two days in order to follow the formation and differentiation of the Caco-2 monolayer.
4.5. Preparation of the Serobioma
A capsule containing a total of 8 × 109 CFU living cells of Lactobacillus rhamnosus LR 32, Bifidobacterium lactis BL04, and Bifidobacterium longum BB 536, commercially available as Serobioma, was supplied by Bromatech S.r.l. (Milano, Italy). Serobioma was suspended in DMEM without supplements.
4.6. pH and Viability Assay
Caco-2 cells were seeded onto 24-well plates at a density of 70,000 CFU/mL and cultured until confluence. Before the assay, cells were washed with PBS and incubated with DMEM without supplements.
In the 30 h following incubation, using litmus/acid test papers, the change in pH was measured. In particular, the pH was assessed immediately after incubation and then every two hours for the first eight hours; subsequently, the pH was determined at the twenty-fourth and thirtieth hours.
Two concentrations of Serobioma, 106 (S1) and 103 CFU/mL (S2), that did not induce a pH change before 6 h of incubation, were selected to evaluate their effect on Caco-2 vitality.
A Sulforhodamine B colorimetric (SRB) assay was used to assess the cell viability. The method has been optimized to adherent cells in a 24-well plate. Cells were fixed with 50% trichloro acetic acid (TCA) at 4 °C for 1 h. Sequentially, the plate was washed 5 times with sterile water and left overnight to dry. The following day, cells were incubated with 300 μL of 0.4% SRB, dissolved in 1% acetic acid, for 30 min in the dark; then, the plate was washed 4 times with 200 μL of 1% acetic acid. After solubilization with TRIS 10 mM pH 10.5, the absorbance was measured at λ = 540 nm using a spectrophotometer (TECAN Spark, Milan, Italy). The absorbance was directly proportional to the protein content and therefore to the number of live cells that were present in each well. Caco-2 viability was assessed after 6 h of incubation with the two concentrations of Serobioma or only with DMEM served as a blank (control). The pH and cell viability were assessed for each of the above-mentioned conditions, at least in duplicate.
4.7. Permeability Assay
Paracellular permeability alterations were assessed by evaluating the flow of Fluorescein-5-(and-6)-Sulfonic Acid (FITC 0.1 mg/mL; absorption/emission peak: 485/535, Invitrogen) through the Caco-2 monolayer over time. A standard curve was used to convert the absorbance results into concentrations of FITC.
Basolateral aliquots of 150 μL were taken, and the amount of FITC was measured using a 96-well fluorescent plate reader (Spark Multimode Microplate Reader, TECAN, Milan, Italy). After the measurement, the aliquots were re-added to the basolateral side. Absorbance evaluations were performed at time 0 (immediately after the addition of treatments), every 30 min for the first 2 h, and then each hour for the subsequent 4 h. The FITC absorbance values obtained were directly proportional to the permeability changes in the cell monolayer.
4.8. CaCo-2 Treatments and Permeability Evaluation
Caco-2 cell monolayers were incubated for 6 h with supernatants of ACs and IBS patients with or without the simultaneous incubation of S1 and S2 of Serobioma. In case of co-incubation, Serobioma was added to Caco-2 cells at the same time as the supernatants. Each condition was tested in duplicate.
4.9. qPCR Analyses
After the paracellular permeability experiments, the Caco-2 cells were rinsed with PBS and preserved in RNAlater buffer until RNA extraction (RNeasy Minikit, Qiagen, Milan, Italy) and reverse transcription using the SuperScript™VILO™ cDNA Synthesis Kit in a final volume of 20 µL, according to the manufacturer’s instructions (Thermo Scientific, Milan, Italy). The gene expression was assessed via qPCR (PowerUp SYBR Green, Thermo Scientific, Milan, Italy) for ZO-1, occludin, and JAM-A on a QuantStudio Real-Time PCR Systems 5 (Thermo Scientific, Milan, Italy). The expression of each gene was normalized to the reference gene Glyceraldehyde-3-phosphate dehydrogenase (GAPDH).
The following primers were used: ZO-1: forward 5′-gaatgatggttggtatggtgcg-3′, reverse 5′-tcagaagtgtgtctactgtccg-3′; occluding forward 5′-tcctataaatccacgccggttc-3′, reverse 5′-ctcaaagttaccaccgctgctg-3′; JAM-A forward 5′-cagaggtgattcatggctctgtg-3′, reverse 5′-ttccaggctggcaataactgac-3′; GAPDH: forward 5′-cagcaagagcacaagaggaag-3′, reverse 5′-caactgtgaggaggggagatt-3′.
The amplification conditions were as follows:
- ZO-1 gene: 15 min at 95 °C, followed by 40 cycles of 15 s at 95 °C, 30 s at 53 °C, and 30 s at 72 °C;
- Occludin gene: 15 min at 95 °C, followed by 40 cycles of 15 s at 95 °C, 30 s at 53 °C, and 30 s at 72 °C;
- JAM-A gene: 15 min at 95 °C, followed by 40 cycles of 15 s at 95 °C, 30 s at 53 °C, and 30 s at 72 °C
- GAPDH gene: 15 min at 95 °C, followed by 40 cycles of 15 s at 95 °C, 30 s at 53 °C, and 30 s at 72 °C.
The melting curve data were analyzed at the end of each reaction. The relative gene expression was calculated using the corresponding condition without Serobioma as the calibrator. A negative control for the PCR reaction (1 µL of water instead of cDNA) and a no-reverse-transcription control were included on each PCR plate. Each reaction was performed in duplicate, and the mean threshold cycle (Ct) was determined from the two runs. The relative gene expression was calculated using the ΔΔCt method, and the gene expression was reported as the fold difference (2−ΔΔCt).
4.10. Statistical Analysis
Results are expressed as mean ± SE. Statistical analysis was carried out with the computer-assisted PrismGraphPad program (Prism version 8.1; GraphPad Software, SanDiego, CA, USA). Kruskal–Wallis test was used for multiple comparison; Mann–Whitney U-test was used for paired comparisons; Spearman rank test was used for correlation analysis; and Pearson χ2 was used for gender analysis. p values < 0.05 were considered significant.
Author Contributions
M.R.B. and G.B. planned the study. M.R.B. wrote the first draft, and all authors reviewed the manuscript for important intellectual content. C.C. and G.M. enrolled patients. M.R.B., C.C., F.B., V.S. and G.B. contributed to data interpretation. G.M. contributed to the statistical analysis. The following authors contributed to the experimental design: M.R.B. and F.B. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by an unrestricted grant from Bromatech S.r.l.to G.B. The funders had no role in the design of the study; in the collection, analysis, or interpretation of data; or in the writing of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethic Committee of Area Vasta Emilia Centro (CE-AVEC, approval identification number: 822/2021/Sper/AOUBo).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available in Zenodo at the following link: https://doi.org/10.5281/zenodo.14826087.
Acknowledgments
The authors would like to thank Ludovica Campolongo for support in the qPCR experiments.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| ACs | Asymptomatic controls |
| TJ | Tight junction |
| IBS | Irritable Bowel Syndrome |
| IBS-D | diarrhea-predominant Irritable Bowel Syndrome |
| IBS-C | constipation-prevalent Irritable Bowel Syndrome |
| IBS-M | Irritable Bowel Syndrome with mixed bowel habits |
| IBS-U | unclassified Irritable Bowel Syndrome |
| SCFAs | Short-chain fatty acids |
| S1 | Serobioma 106 CFU/mL |
| S2 | Serobioma 103 CFU/mL |
| BDQ | Bowel Disease Questionnaire |
| ZO-1 | Zonula Occludens-1 |
| JAM-A | Junctional adhesion molecule-A |
| GAPDH | Glyceraldehyde-3-phosphate dehydrogenase |
References
- Lacy, B.E.; Mearin, F.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel Disorders. Gastroenterology 2016, 150, 1393–1407.e5. [Google Scholar] [CrossRef] [PubMed]
- Lovell, R.M.; Ford, A.C. Global Prevalence of and Risk Factors for Irritable Bowel Syndrome: A Meta-Analysis. Clin. Gastroenterol. Hepatol. 2012, 10, 712–721.e4. [Google Scholar] [CrossRef] [PubMed]
- Chey, W.D.; Kurlander, J.; Eswaran, S. Irritable Bowel Syndrome: A Clinical Review. JAMA 2015, 313, 949–958. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, I.B.; O’Toole, P.W.; Öhman, L.; Claesson, M.J.; Deane, J.; Quigley, E.M.M.; Simrén, M. An Irritable Bowel Syndrome Subtype Defined by Species-Specific Alterations in Faecal Microbiota. Gut 2012, 61, 997–1006. [Google Scholar] [CrossRef]
- Rodiño-Janeiro, B.K.; Vicario, M.; Alonso-Cotoner, C.; Pascua-García, R.; Santos, J. A Review of Microbiota and Irritable Bowel Syndrome: Future in Therapies. Adv. Ther. 2018, 35, 289–310. [Google Scholar] [CrossRef]
- Barbaro, M.R.; Fuschi, D.; Cremon, C.; Carapelle, M.; Dino, P.; Marcellini, M.M.; Dothel, G.; De Ponti, F.; Stanghellini, V.; Barbara, G. Escherichia Coli Nissle 1917 Restores Epithelial Permeability Alterations Induced by Irritable Bowel Syndrome Mediators. Neurogastroenterol. Motil. 2018, 30, e13388. [Google Scholar] [CrossRef]
- Barbaro, M.R.; Cremon, C.; Marasco, G.; Savarino, E.; Guglielmetti, S.; Bonomini, F.; Palombo, M.; Fuschi, D.; Rotondo, L.; Mantegazza, G.; et al. Molecular Mechanisms Underlying Loss of Vascular and Epithelial Integrity in Irritable Bowel Syndrome. Gastroenterology 2024, 167, 1152–1166. [Google Scholar] [CrossRef]
- Vazquez-Roque, M.I.; Camilleri, M.; Smyrk, T.; Murray, J.A.; O’Neill, J.; Carlson, P.; Lamsam, J.; Eckert, D.; Janzow, D.; Burton, D.; et al. Association of HLA-DQ Gene with Bowel Transit, Barrier Function, and Inflammation in Irritable Bowel Syndrome with Diarrhea. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 303, G1262–G1269. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Moayyedi, P.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.R.; Quigley, E.M.M. Task Force on the Management of Functional Bowel Disorders American College of Gastroenterology Monograph on the Management of Irritable Bowel Syndrome and Chronic Idiopathic Constipation. Am. J. Gastroenterol. 2014, 109 (Suppl. S1), S2–S26; quiz S27. [Google Scholar] [CrossRef]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. The International Scientific Association for Probiotics and Prebiotics Consensus Statement on the Scope and Appropriate Use of the Term Probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef]
- Ohland, C.L.; MacNaughton, W.K. Probiotic Bacteria and Intestinal Epithelial Barrier Function. Am. J. Physiol.-Gastrointest. Liver Physiol. 2010, 298, G807–G819. [Google Scholar] [CrossRef] [PubMed]
- Reid, G.; Younes, J.A.; Van der Mei, H.C.; Gloor, G.B.; Knight, R.; Busscher, H.J. Microbiota Restoration: Natural and Supplemented Recovery of Human Microbial Communities. Nat. Rev. Microbiol. 2011, 9, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Sarita, B.; Samadhan, D.; Hassan, M.Z.; Kovaleva, E.G. A Comprehensive Review of Probiotics and Human Health-Current Prospective and Applications. Front. Microbiol. 2025, 15, 1487641. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.B.; Odamaki, T.; Xiao, J. Beneficial Effects of Bifidobacterium Longum Subsp. Longum BB536 on Human Health: Modulation of Gut Microbiome as the Principal Action. J. Funct. Foods 2019, 54, 506–519. [Google Scholar] [CrossRef]
- Akatsu, H.; Iwabuchi, N.; Xiao, J.; Matsuyama, Z.; Kurihara, R.; Okuda, K.; Yamamoto, T.; Maruyama, M. Clinical Effects of Probiotic Bifidobacterium Longum BB536 on Immune Function and Intestinal Microbiota in Elderly Patients Receiving Enteral Tube Feeding. J. Parenter. Enter. Nutr. 2013, 37, 631–640. [Google Scholar] [CrossRef]
- di Vito, R.; Conte, C.; Traina, G. A Multi-Strain Probiotic Formulation Improves Intestinal Barrier Function by the Modulation of Tight and Adherent Junction Proteins. Cells 2022, 11, 2617. [Google Scholar] [CrossRef]
- Tamaki, H.; Nakase, H.; Inoue, S.; Kawanami, C.; Itani, T.; Ohana, M.; Kusaka, T.; Uose, S.; Hisatsune, H.; Tojo, M.; et al. Efficacy of Probiotic Treatment with Bifidobacterium Longum 536 for Induction of Remission in Active Ulcerative Colitis: A Randomized, Double-blinded, Placebo-controlled Multicenter Trial. Dig. Endosc. 2016, 28, 67–74. [Google Scholar] [CrossRef]
- Vale, G.C.; Mota, B.I.S.; Ando-Suguimoto, E.S.; Mayer, M.P.A. Effect of Probiotics Lactobacillus Acidophilus and Lacticaseibacillus Rhamnosus on Antibacterial Response Gene Transcription of Human Peripheral Monocytes. Probiotics Antimicrob. Proteins 2023, 15, 264–274. [Google Scholar] [CrossRef]
- Huang, C.; Yue, Q.; Sun, L.; Di, K.; Yang, D.; Hao, E.; Wang, D.; Chen, Y.; Shi, L.; Zhou, R.; et al. Restorative Effects of Lactobacillus Rhamnosus LR-32 on the Gut Microbiota, Barrier Integrity, and 5-HT Metabolism in Reducing Feather-Pecking Behavior in Laying Hens with Antibiotic-Induced Dysbiosis. Front. Microbiol. 2023, 14, 1173804. [Google Scholar] [CrossRef]
- Ouwehand, A.C.; DongLian, C.; Weijian, X.; Stewart, M.; Ni, J.; Stewart, T.; Miller, L.E. Probiotics Reduce Symptoms of Antibiotic Use in a Hospital Setting: A Randomized Dose Response Study. Vaccine 2014, 32, 458–463. [Google Scholar] [CrossRef]
- Engelbrektson, A.; Korzenik, J.R.; Pittler, A.; Sanders, M.E.; Klaenhammer, T.R.; Leyer, G.; Kitts, C.L. Probiotics to Minimize the Disruption of Faecal Microbiota in Healthy Subjects Undergoing Antibiotic Therapy. J. Med. Microbiol. 2009, 58, 663–670. [Google Scholar] [CrossRef]
- Bartosch, S.; Woodmansey, E.J.; Paterson, J.C.M.; McMurdo, M.E.T.; Macfarlane, G.T. Microbiological Effects of Consuming a Synbiotic Containing Bifidobacterium Bifidum, Bifidobacterium Lactis, and Oligofructose in Elderly Persons, Determined by Real-Time Polymerase Chain Reaction and Counting of Viable Bacteria. Clin. Infect. Dis. 2005, 40, 28–37. [Google Scholar] [CrossRef] [PubMed]
- West, N.P.; Horn, P.L.; Pyne, D.B.; Gebski, V.J.; Lahtinen, S.J.; Fricker, P.A.; Cripps, A.W. Probiotic Supplementation for Respiratory and Gastrointestinal Illness Symptoms in Healthy Physically Active Individuals. Clin. Nutr. 2014, 33, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Grover, M.; Vanuytsel, T.; Chang, L. Intestinal Permeability in Disorders of Gut-Brain Interaction: From Bench to Bedside. Gastroenterology 2024, 168, 480–495. [Google Scholar] [CrossRef]
- Lacy, B.E.; Chey, W.D.; Lembo, A.J. New and Emerging Treatment Options for Irritable Bowel Syndrome. Gastroenterol. Hepatol. 2015, 11, 1–19. [Google Scholar]
- So, D.; Quigley, E.M.M.; Whelan, K. Probiotics in Irritable Bowel Syndrome and Inflammatory Bowel Disease: Review of Mechanisms and Effectiveness. Curr. Opin. Gastroenterol. 2023, 39, 103–109. [Google Scholar] [CrossRef]
- Martínez, C.; Lobo, B.; Pigrau, M.; Ramos, L.; González-Castro, A.M.; Alonso, C.; Guilarte, M.; Guilá, M.; de Torres, I.; Azpiroz, F.; et al. Diarrhoea-Predominant Irritable Bowel Syndrome: An Organic Disorder with Structural Abnormalities in the Jejunal Epithelial Barrier. Gut 2013, 62, 1160–1168. [Google Scholar] [CrossRef]
- Dunlop, S.P.; Hebden, J.; Campbell, E.; Naesdal, J.; Olbe, L.; Perkins, A.C.; Spiller, R.C. Abnormal Intestinal Permeability in Subgroups of Diarrhea-Predominant Irritable Bowel Syndromes. Am. J. Gastroenterol. 2006, 101, 1288–1294. [Google Scholar] [CrossRef]
- di Vito, R.; Di Mezza, A.; Conte, C.; Traina, G. The Crosstalk between Intestinal Epithelial Cells and Mast Cells Is Modulated by the Probiotic Supplementation in Co-Culture Models. Int. J. Mol. Sci. 2023, 24, 4157. [Google Scholar] [CrossRef]
- Barbaro, M.R.; Di Sabatino, A.; Cremon, C.; Giuffrida, P.; Fiorentino, M.; Altimari, A.; Bellacosa, L.; Stanghellini, V.; Barbara, G. Interferon-γ Is Increased in the Gut of Patients with Irritable Bowel Syndrome and Modulates Serotonin Metabolism. Am. J. Physiol. Gastrointest. Liver Physiol. 2016, 310, G439–G447. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).