Abstract
Hair loss disorders pose a substantial global health burden, affecting millions of individuals and significantly impacting quality of life. Despite the widespread use of approved therapeutics like minoxidil and finasteride, their clinical efficacy remains limited. These challenges underscore the pressing need for more targeted and effective therapeutic solutions. This review examines the latest innovations in hair loss drug discovery, with a focus on small-molecule inhibitors, biologics, and stem cell-based therapies. By integrating insights from molecular mechanisms and leveraging advancements in research methods, the development of next-generation therapeutics holds the potential to transform the clinical management of hair loss disorders. Future drug development for hair loss disorders should prioritize antibody therapy and cell-based treatments, as these approaches offer unprecedented opportunities to address the limitations of existing options. Antibody therapies enable precise targeting of key molecular pathways involved in hair follicle regulation, providing highly specific and effective interventions. Similarly, cell-based therapies, including stem cell transplantation and dermal papilla cell regeneration, directly address the regenerative capacity of hair follicles, offering transformative potential for hair restoration.
1. Introduction
Hair loss disorders, including androgenetic alopecia (AGA) and alopecia areata (AA), are among the most prevalent dermatological conditions affecting millions of individuals worldwide. These disorders can result from genetic predisposition, autoimmune reactions, hormonal imbalances, environmental stressors, and aging [1,2,3,4]. While hair loss is often considered a cosmetic issue, it can significantly impact self-esteem, mental health, and overall quality of life. Despite the growing demand for effective treatments, current therapeutic options remain limited in efficacy and scope.
Existing pharmacological treatments, such as minoxidil (a potassium channel opener) and finasteride (a 5α-reductase inhibitor), have demonstrated partial success in slowing hair loss and promoting regrowth. However, their effects are often temporary, and many patients experience inadequate responses or undesirable side effects. In recent years, advancements in molecular biology, regenerative medicine, and targeted drug development have paved the way for novel therapeutic strategies. Understanding the key molecular pathways that regulate hair follicle cycling, stem cell activity, and immune responses is crucial for developing more effective and personalized treatments for hair loss disorders.
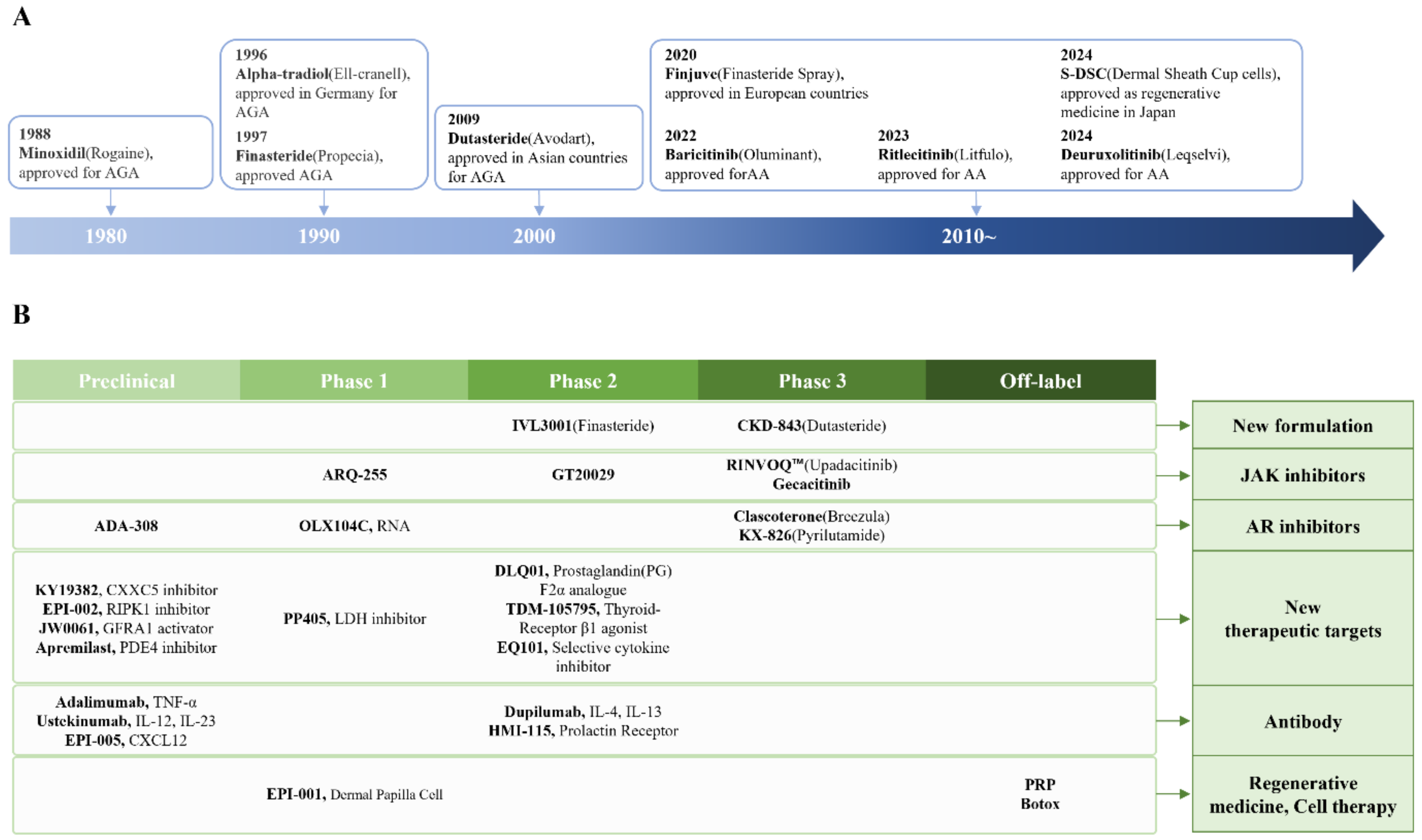
This paper explores the latest approaches in hair loss drug development, focusing on emerging small-molecule inhibitors, biologics, and stem cell-based therapies (Figure 1). It also examines the role of androgen receptor (AR) and critical signaling pathways such as Wnt/β-catenin, JAK/STAT, and CXCL12/CXCR4 in hair follicle regulation. By integrating insights from molecular dermatology and advanced drug discovery techniques, we aim to provide a comprehensive overview of the current landscape and future prospects in hair loss treatment.
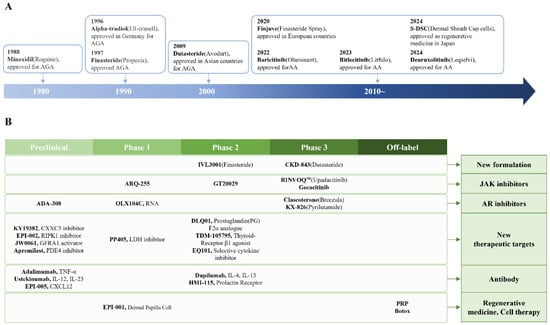
Figure 1.
Approved drugs (A) and new drug candidates (B) for hair loss disorders.
2. Current Approved Hair Loss Treatments
Several pharmacological treatments are currently available for hair loss disorders, with minoxidil, finasteride/dutasteride, and JAK inhibitors being among the most widely used (Table 1). While these medications have shown varying degrees of efficacy, they also have limitations that hinder their widespread success.

Table 1.
Approved drugs for hair loss treatment.
2.1. Minoxidil
Minoxidil is a potassium channel opener that promotes vasodilation, improving blood flow to hair follicles [5,6]. It extends the anagen phase of the hair cycle and stimulates dermal papilla cell (DPC) activity [7]. Approved by the FDA in 1988 for both male and female AGA, minoxidil is available as a topical solution or foam. However, its exact molecular mechanism remains only partially understood. Hair regrowth usually becomes visible after 3–6 months of continuous use, with peak efficacy at around 12 months. Dawber and Rundegren reported that the affected area became smaller in 561 of the 904 eligible subjects (62.0%), remained unchanged in 317 subjects (35.1%), and became larger in 26 subjects (2.9%) [8]. Hair density increases by approximately 10–30%, while hair thickness improves by 10–25% with Minoxidil treatment [9,10]. A 5% minoxidil solution is more effective than the 2% formulation, but women are generally advised to use the 2% solution due to potential side effects. Additionally, discontinuation leads to resumed hair loss. Common side effects include scalp irritation, itching, and unwanted facial or body hair growth (hypertrichosis). Low-dose oral minoxidil (0.25–5 mg/day) is emerging as an alternative to topical application, and studies suggest that it offers better patient adherence than the topical form [11,12]. However, side effects such as low blood pressure, swelling, and excessive hair growth in unwanted areas have been reported.
2.2. 5a-Reductase Inhibitors
Hair follicles in the scalp (especially the front and crown areas) exhibit high levels of AR expression. Testosterone and DHT bind to these receptors, triggering molecular signals that shorten the hair growth cycle. DHT shortens the anagen phase, meaning that hair stops growing sooner and falls out more quickly. Over time, hair follicles produce only vellus hairs, leading to baldness. Additionally, DHT increases inflammation and promotes fibrosis (scar tissue formation) in hair follicles, which makes it harder for follicles to recover, accelerating permanent hair loss.
Finasteride and dutasteride inhibit 5α-reductase enzymes, blocking the conversion of testosterone to dihydrotestosterone (DHT)—a crucial mediator in hair follicle miniaturization. By reducing scalp DHT levels, these drugs can slow hair loss progression and, in some cases, promote regrowth. Recent findings indicate that 5α-reductase type 1 and 3 (SRD5A1 and SRD5A3) are predominantly expressed in hair keratinocytes, and that DHT activation of the AR in DPCs triggers hair miniaturization [13].
Finasteride was FDA-approved for male AGA in 1997 (although not approved for women due to potential side effects) and is administered orally. Male AGA patients experience significant hair regrowth, but finasteride is ineffective for autoimmune-related hair loss. Finasteride increased hair density by 10–20% in cases of AGA after one year, and thicker hair shafts were observed in most patients. Over 80% of men maintained their existing hair over a five-year period. Finasteride is more effective than minoxidil for preventing hair loss. Some studies suggest that combining finasteride and minoxidil provides better results than using either treatment alone [14]. A 1 mg dose of finasteride is optimal for treating male pattern baldness, as 5 mg does not significantly increase hair growth but raises the risk of side effects.
Side effects such as erectile dysfunction, reduced libido, and gynecomastia occur in some men and may persist even after stopping therapy [15,16]. A systematic review suggested that dutasteride (0.5 mg) was more effective than finasteride (1 mg) in increasing hair counts (up to 1.5-fold), but approved in Asian countries. Finasteride inhibits only Type II 5α-reductase, while dutasteride inhibits both Type I and Type II 5α-reductase, making it more potent in reducing DHT levels [17]. Due to its longer half-life, dutasteride provides sustained benefits but also carries a higher risk of side effects [18].
2.3. JAK Inhibitors
Alopecia areata is an autoimmune disorder in which the immune system mistakenly attacks hair follicles, leading to sudden hair loss. This condition typically causes round or oval bald patches on the scalp, but in severe cases, it can result in total scalp hair loss (alopecia totalis) or complete body hair loss (alopecia universalis).
JAK inhibitors work by blocking the activity of Janus kinase enzymes, thereby interrupting the inflammatory signaling pathways that contribute to hair follicle miniaturization and loss. By modulating these pathways, JAK inhibitors can promote hair regrowth and extend the anagen phase of the hair cycle [19,20].
Early studies demonstrated that these JAK inhibitors could effectively reverse hair loss in patients with moderate to severe AA. This oral JAK inhibitor has been approved by the FDA for treating severe AA in adults and adolescents. Ruxolitinib and tofacitinib significantly increased hair shaft length, indicating their potential in promoting hair growth [20,21]. Clinical trials have also shown that baricitinib can lead to substantial hair regrowth, with some patients achieving at least 50% improvement compared to placebo [22]. Deuruxolitinib, a selective JAK1/JAK2 inhibitor, was recently FDA-approved for treating severe AA in adults [23,24]. Significant scalp hair regrowth was observed in approximately 65–70% of patients treated with deuruxolitinib, with improvements in hair thickness, coverage, and density. Unlike JAK1, which is broadly expressed in many tissues, JAK3 expression is largely restricted to hematopoietic cells. Of interest, selective inhibiting JAK3 signaling by ritlecitinib is sufficient to prevent and reverse AA [25]. 65–70% of patients in clinical trials achieved 50% or more scalp hair regrowth, and improvements in eyebrows and eyelashes were also noted [26,27]. In addition, many companies are developing JAK inhibitors as treatments for AA, as outlined in Table 2.
Table 2.
Emerging therapeutic target and its development.
Although JAK inhibitors have proven beneficial in AA, they are not FDA-approved for AGA and can be costly. Known risks include heightened susceptibility to infections, thrombosis, and cardiovascular events, especially with prolonged use. For example, JAK inhibitors have been associated with an increased risk of deep vein thrombosis and pulmonary embolism, particularly in high-risk patients [31]. Long-term use may slightly elevate the risk of heart attacks and strokes, especially in older patients with pre-existing cardiovascular conditions [32]. Moreover, once patients discontinue therapy, previously regrown hair may be lost again.
3. Emerging Therapeutic Targets for Alopecia Treatment
Recent progress in understanding inflammatory processes, hormonal imbalances, stem cell dysfunction, and immune dysregulation has driven the discovery of novel molecular targets for treating various types of alopecia [33,34,35,36,37,38,39]. Table 3 outlines emerging targets such as AR and Wnt/β-catenin pathways, which play pivotal roles in hair follicle cycling, immune regulation, and stem cell function.
Table 3.
Emerging therapeutic target and its development.
3.1. AR Inhibitors
AR inhibitors (ARIs) are pivotal in treating androgen-dependent conditions, notably prostate cancer and AGA [56,57]. Both systemic and topical ARIs are in development to enhance efficacy and mitigate resistance. Spironolactone, a potassium-sparing diuretic with anti-androgenic properties, is commonly used off-label for AGA and hirsutism [58,59]. It primarily functions by inhibiting AR, thus reducing androgenic signaling in HFs.
Clascoterone (Breezula®) is a topical AR inhibitor developed by Cassiopea, (San Diego, CA, USA) originally approved as Winlevi® for acne and currently in trials for AGA [42,60]. Kintor Pharmaceuticals’ pyrilutamide, a nonsteroidal topical ARI, has shown promising preliminary results, including significant increases in hair count [43,61]. OliX Pharmaceuticals is investigating OLX72021, an RNA interference-based therapy targeting AR for AGA [46,62]. This approach aims to reduce AR expression, potentially mitigating hair loss. These developments underscore the growing potential of ARIs in hair loss treatment.
3.2. Wnt Activators
The Wnt/β-catenin pathway is integral to hair follicle development and regeneration, making it a prime target for AGA therapies [48]. Pharmaceutical companies are actively pursuing Wnt activators to promote hair growth.
Biosplice Therapeutics (formerly Samumed) has developed SM04554, a small-molecule Wnt modulator [63]. JW Pharmaceutical has developed JW0061 (GFRA1 agonist), a first-in-class drug candidate that promotes hair follicle proliferation and hair regeneration by activating the Wnt signaling pathway in skin and hair follicle stem cells [64,65]. KY19382, a novel CXXC5–Dvl interaction inhibitor, fosters Wnt/β-catenin signaling, thereby enhancing hair regrowth and wound-induced hair neogenesis [49].
3.3. Thyroid Receptor
Thyroid hormones play a crucial role in regulating metabolism, development, and tissue homeostasis, including hair follicle function [66]. Mice lacking TRα1 and TRβ (the main thyroid hormone binding isoforms) display impaired hair cycling associated to a decrease in follicular hair cell proliferation. In addition, TRα1/TRβ-deficient mice developed alopecia after serial depilation [67]. Thyroid hormone signaling is an important determinant of the mobilization of stem cells out of their niche in the hair bulge [68]. Therefore, research is exploring TRβ-selective agonists to fine-tune thyroid hormone effects while minimizing hair loss [69].
TDM-105795 is a topical small molecule drug candidate developed by Technoderma Medicines for the treatment of AGA. As a potent thyromimetic, it offers potential advantages in efficacy and safety over existing treatments [50,70]. A Phase 2a clinical trial involving mild to moderate AGA proved efficacy of TDM-105795.
3.4. Prostaglandin Derivatives
Prostaglandin (PG) derivatives have been found to influence hair growth in different ways. Specifically, prostaglandin F2α (PGF2α) derivatives promote hair growth, whereas prostaglandin D2 (PGD2) has been shown to inhibit it [71]. For example, PGD2 levels were approximately three times higher in balding scalp areas compared to non-balding regions in men with AGA [51]. Blocking PGD2 activity or its receptor may help prevent hair follicle miniaturization and promote hair regrowth.
Latanoprost and Bimatoprost, originally developed to reduce intraocular pressure in glaucoma treatment, were observed to induce hair growth as a side effect [72,73]. These compounds stimulate follicular cell proliferation and extend the anagen phase of the hair cycle, leading to increased hair density and length. DLQ01 is a topical prostaglandin F2α analog developed by Dermaliq Therapeutics for the treatment of AGA, and Dermaliq announced positive results from a Phase 1b/2a clinical trial. DLQ01 treatment resulted in a 12.3% increase in hair counts from baseline, and 83% of subjects treated with DLQ01 experienced positive hair growth.
3.5. Lactate Dehydrogenase (LDH)
Recent research has highlighted the role of lactate dehydrogenase (LDH) in hair follicle stem cell (HFSC) activation, offering promising avenues for developing novel hair loss treatments [74,75,76]. HFSCs utilize glycolytic metabolism, producing significant amounts of lactate. This lactate production is crucial for HFSC activation, as deleting the enzyme LDH in these cells prevented their activation. Conversely, increasing lactate production accelerated HFSC activation and the hair cycle [77].
Pelage Pharmaceuticals is developing a topical small molecule drug that targets this metabolic pathway. Their approach aims to activate dormant HFSCs by modulating lactate production, thereby stimulating hair growth. Pelage’s treatment is designed to be non-invasive and suitable for all genders, and hair types. They have initiated a Phase 2a clinical trial to evaluate the safety and efficacy of their lead compound, PP405, in individuals with AGA [52].
3.6. PDE4 Inhibitors
Phosphodiesterase 4 (PDE4) inhibitors are being explored as potential treatments for AA [78]. PDE4 is an enzyme that modulates inflammatory pathways, and its inhibition can reduce inflammation. Elevated PDE4 expression has been observed in AA, suggesting that PDE4 inhibition could reduce inflammation-associated hair loss [79].
Apremilast is a well-known PDE4 inhibitor (CC-10004), and recent studies have investigated its efficacy in promoting hair regrowth in patients with AA [53]. For instance, a Japanese patient with AA showed significant hair regrowth after 14 weeks of treatment with apremilast. Apremilast leads to the downregulation of inflammatory cytokines such as TNF-α, IL-17, and IFN-γ, which play a significant role in autoimmune diseases.
3.7. RIPK1 Inhibitor
Necroptosis, a programmed form of inflammatory cell death, has been increasingly recognized as a contributing factor to hair follicle dysfunction and hair loss [80]. By inhibiting RIPK1, RIPK3, or MLKL, necroptosis-related damage may be reduced. Necrostatin-1s (Nec1-s) has shown protective effects on human outer root sheath cells and improved hair regrowth in mouse models by limiting follicular inflammation [54].
4. New Therapeutic Modalities for Alopecia Treatment
Beyond small-molecule inhibitors, novel therapeutic modalities such as biologics and stem cell-based therapies aim to address hair loss more precisely, potentially improving upon traditional interventions. Beyond efficacy, future efforts must emphasize long-term safety and personalized approaches. The integration of antibody and cell-based therapies into mainstream clinical practice will be essential for meeting the unmet needs of patients.
4.1. Antibody Therapy
Antibody-based treatments have emerged as a targeted approach for AA, a condition in which existing immunosuppressants often yield variable results [81,82]. Antibodies are rarely developed for AGA therapy due to the requirement to be responsive to androgens and their receptors surrounding the hair follicle [83]. However, direct injection into the areas of hair loss is also feasible, potentially enhancing treatment efficacy while minimizing systemic side effects. Table 4 summarizes key antibody therapies under investigation.
Table 4.
Antibody therapy for hair loss.
Dupilumab, initially approved for atopic dermatitis, is under Phase 2 evaluation for AA [81]. Dupilumab is a humanized monoclonal antibody against IL-4Rα that downregulates TH2 response [91]. Clinical data suggested that subcutaneous injection of dupilumab every week slows AA progression, particularly in patients with atopic backgrounds [84]. Ustekinumab, which targets IL-12 and IL-23, has shown promise in case reports but remains off-label for AA [85]. Adalimumab, targeting TNF-α, yields inconsistent results and is not recommended as a standard AA treatment [86].
Prolactin (PRL) and its receptor (PRLR) play significant roles in hair follicle regulation and hair cycle stages. In humans and some mammals, PRL prolongs the telogen phase, potentially leading to reduced hair growth and increased shedding [92]. High PRL levels have been associated with delayed anagen initiation, contributing to hair thinning [93,94]. In addition, PRL can upregulate AR, potentially exacerbating hair follicle miniaturization in AGA [95]. Hope Medicine’s monoclonal antibody HMI-115 blocks PRLR and is in Phase 2 trials, with early reports suggesting promising efficacy [87].
CXCL12, also known as stromal cell-derived factor 1 (SDF-1), is a chemokine that plays a crucial role in tissue regeneration, immune cell recruitment, and stem cell homing [96,97,98]. Recent studies suggest that CXCL12 signaling may contribute to hair loss by influencing hair follicle cycling and the dermal microenvironment. For example, elevated CXCL12 levels in the dermis interfere with the transition from telogen to anagen, leading to prolonged hair loss [88]. In addition, secreted CXCL12 from dermal fibroblasts upregulated AR expression in DPCs to induce hair miniaturization in AGA [89]. Its interaction with immune cells, particularly through the CXCR4 receptor, may trigger chronic inflammation, which is associated with hair loss in AA [90]. Given the large molecular weight and long half-life of monoclonal antibodies, monthly or bimonthly subcutaneous injections of CXCL12 could be feasible for hair loss treatments.
4.2. Growth Factors and Platelet-Rich Plasma (PRP)
Therapeutic proteins have emerged as a promising approach to promoting hair growth by targeting various biological pathways involved in hair follicle regeneration. One notable therapeutic protein in hair growth research is basic fibroblast growth factor (bFGF), which extends the anagen phase of the hair cycle [99,100]. Additionally, vascular endothelial growth factor (VEGF) plays a crucial role in increasing blood supply to hair follicles, thereby promoting their activity and enhancing hair density [101,102]. Another important protein is insulin-like growth factor 1 (IGF-1), which has been shown to protect hair follicle cells from apoptosis [103,104]. Moreover, platelet-derived growth factor (PDGF) and keratinocyte growth factor (KGF, also known as FGF-7) contribute to hair follicle regeneration by supporting epithelial cell proliferation and follicle differentiation [105,106].
Platelet-rich plasma (PRP) has gained significant attention as a promising treatment for hair loss due to its regenerative properties (Table 5). PRP is derived from a patient’s own blood and contains a high concentration of growth factors (i.e., PDGF, VEGF, FGF, and IGF-1) that stimulate hair regeneration [107,108]. Typically, three initial treatments are administered monthly, followed by maintenance sessions every 3–6 months. Clinical trials suggested that PRP therapy effectively enhances hair density and thickness in women with hair loss, with a favorable safety profile [108]. However, the effects of PRP on hair density and thickness vary with dosage, injection duration, and ethnicity, indicating the need for tailored treatment protocols.
Table 5.
Regenerative medicine for hair loss treatment.
4.3. Botulinum Toxin
Botulinum toxin (Botox) has been studied for AGA, aiming to relax scalp muscles and potentially enhance blood flow to the follicles [109,117]. While preliminary studies show encouraging hair count increases in some participants, findings are not yet conclusive [118,119,120]. Botulinum toxin may be a promising therapeutic option for patients with various scalp conditions, but larger, randomized controlled trials are needed to better understand its efficacy and safety.
4.4. Cell Therapy
The development of cell therapy for hair loss treatment is gaining significant attention as an innovative approach utilizing DPCs, DSCs, and stem cells to stimulate hair growth [121]. Compared to conventional treatments, cell therapy may offer long-term efficacy with a single administration and fewer adverse effects [121]. Several companies are developing advanced therapies (Table 5).
The regulation of cell therapies for hair loss varies across countries, with key differences in how stem cell treatments are classified and approved. The U.S. and Europe have established frameworks for approving advanced therapies, with varying levels of clinical trial requirements and regulatory flexibility. Japan, China, and South Korea have more lenient regulatory practices, particularly for autologous stem cell treatments, as these therapies tend to be better tolerated and have fewer side effects. In these countries, regenerative medicine is regulated under the Regenerative Medicine Safety Act and the Cell Therapy Act, which allow for accelerated approval of cell therapies for hair loss.
Tissue grafting is a surgical procedure in which tissue is transferred from one area of the body to another. Plastic surgeons and dermatologists have reliably used scalp tissue grafting to improve and enhance hair regeneration. A simple procedure was developed to isolate epidermal stem cells (EpSCs) from scalp tissue and inject them into areas of hair loss to promote hair growth. Automated devices for producing stromal vascular fraction from lipoaspirated fat or EpSCs from scalp tissue are commercially available in clinics and have shown effectiveness in hair regeneration [122,123].
Shiseido has been actively involved in the development of hair regenerative medicine, focusing on the use of DSCs. Since initiating this research in 2016, Shiseido has collaborated with institutions such as Tokyo Medical University Hospital and Toho University Ohashi Medical Center to conduct clinical studies verifying the safety and efficacy of their proprietary cell processing product, S-DSC®. These studies have demonstrated positive results in treating male and female pattern baldness [110,111,124]. Shiseido’s S-DSC® therapy represents a significant advancement in hair regenerative medicine. Shiseido began offering this treatment to patients in Japan on 1 July 2024. The procedure involves culturing autologous DSCs and injecting them into the scalp to promote hair growth.
DPCs, located at the base of hair follicles, play a pivotal role in regulating hair growth and cycling. Research has demonstrated that when DPCs are implanted between the epidermis and dermis, they can induce the formation of new hair follicles in hairless skin [125,126,127]. This finding underscores their potential in regenerative hair therapies. Currently, the treatment is in Phase 1/2a clinical trials for both male and female AGA. DPCs can be expanded in vitro while still maintaining their hair-inductive properties, while DSCs tend to lose their regenerative capacity more rapidly during in vitro expansion, limiting their potential for large-scale therapeutic applications [128]. As a result, DPC-based therapies hold greater promise for long-term and widespread use in regenerative medicine for hair loss treatment [112,121,127].
Adipose-derived stem cells (ADSCs) have emerged as a promising avenue for developing treatments for hair loss, particularly AGA [129,130]. These multipotent cells, harvested from adipose tissue, possess regenerative properties that can stimulate hair growth through various mechanisms [131,132,133,134]. Studies also have explored the use of ADSC-conditioned media (ADSC-CM) in hair regeneration therapies [135,136]. This approach involves applying the growth factors secreted by ADSCs to the scalp, promoting hair growth without the need for cell transplantation. Clinical trials have reported positive outcomes, indicating that cosmetics using ADSC-CM can effectively stimulate hair regeneration [137,138,139].
Stromal vascular fraction (SVF) is a component derived from adipose tissue and is gaining significant attention in regenerative medicine, including hair loss treatments [116,140,141]. SVF consists of a heterogeneous population of cells, including adipose-derived stem cells, endothelial cells, pericytes, fibroblasts, and immune cells, all of which contribute to tissue regeneration and repair [142]. Clinical studies have shown positive results, with patients experiencing increased hair density, thickness, and regrowth after SVF administration [114,115,116]. SVF helps improve the scalp’s microenvironment by increasing blood flow, reducing inflammation, and enhancing tissue repair [143].
4.5. Exosome for Hair Loss Treatments
Exosomes are tiny vesicles secreted by cells that contain various bioactive molecules, including proteins, lipids, and nucleic acids [144,145]. They play an important role in cell signaling and tissue regeneration and have recently garnered attention for their potential in treating hair loss. Current research indicates that exosomes are safe for use in hair loss treatment; however, data on their efficacy remain limited. A recent review highlighted that while preclinical studies have demonstrated positive effects of exosomes on hair growth, clinical data on their effectiveness and safety in humans are still insufficient [145]. Since exosome therapy is a relatively new field, further research is needed to establish its long-term effects and safety.
4.6. Innovations in Drug Delivery Systems for Hair Loss Treatments
Innovations in drug delivery systems for hair loss treatments are progressing rapidly. The development of novel finasteride and dutasteride formulations has generated considerable interest due to their potential for improved long-term safety and efficacy. For example, topical formulations aim to minimize systemic side effects by delivering the drug directly to the scalp, thereby reducing the risk of sexual dysfunction [146]. In addition, nanoparticle-based delivery systems enhance drug stability and therapeutic efficacy, while controlled-release mechanisms may improve patient compliance by reducing the frequency of application [147,148].
Lipid-based nanoparticles stabilize drugs by effectively encapsulating both hydrophilic and lipophilic substances. Nanostructured lipid carriers enhance drug stability, solubility, and sustained release, thereby improving drug penetration into the scalp. This delivery method may enhance the effectiveness and reduce the side effects of existing drugs such as minoxidil and finasteride [149].
Microneedles are used to deliver drugs directly into the scalp, enhancing absorption and maximizing treatment efficacy. Recently, they have been actively studied in the field of hair loss treatment as an alternative approach to overcome the limitations of oral medications and topical applications. For example, microneedles can effectively penetrate the stratum corneum of the scalp, delivering active ingredients such as minoxidil or finasteride [150,151,152]. Microneedle systems loaded with exosomes derived from stem cells and growth factors (e.g., bFGF, VEGF) have been developed to promote follicle regeneration [153,154,155].
3D-printed scaffolds also represent an innovative approach that is gaining attention in the field of hair restoration. This technique involves the use of 3D printing technology to create customized scaffolds that can be implanted into the scalp to promote hair growth. The scaffolds are designed to match the individual’s scalp condition and can be loaded with drugs for gradual release, thereby maximizing therapeutic effects.
5. Conclusions
Advances in molecular biology, regenerative medicine, and precision therapeutics are redefining the landscape of hair loss drug development. While current mainstays such as minoxidil and finasteride have provided some benefit, their limitations underscore the critical need for more targeted and effective therapies. Emerging modalities, including JAK inhibitors, Wnt activators, and gene-editing approaches, offer the potential for transformative advancements in hair restoration.
Antibody therapy and cell therapy, in particular, represent highly promising avenues for the development of next-generation hair loss treatments. Antibody-based therapies can provide precise targeting of key molecular pathways implicated in hair follicle cycling, offering enhanced specificity and minimized off-target effects. Meanwhile, cell-based approaches, including follicular stem cell transplantation and ex vivo expanded DPCs, have the potential to directly regenerate hair follicles and restore hair growth. As these therapies advance, their integration into the therapeutic pipeline will be critical to overcoming the limitations of current treatments.
One of the major challenges in this field is patient heterogeneity. Genetic variations, immune profiles, and hormonal influences can significantly affect treatment outcomes, making a one-size-fits-all approach inadequate. Personalized medicine, supported by AI-driven drug discovery and biomarker identification, holds promise for tailoring interventions to individual patients, thereby optimizing therapeutic efficacy. Additionally, innovations in drug delivery technologies—such as microneedles, nanoparticles, and 3D-printed scaffolds—could further enhance treatment outcomes by ensuring precise and sustained release of active compounds.
Combination therapies that leverage multiple mechanisms, including immunomodulation, follicle stem cell activation, and angiogenesis, are likely to surpass the efficacy of single-agent strategies. As gene- and cell-based therapies advance toward clinical application, ethical and regulatory considerations will play a pivotal role in ensuring their safe and equitable use.
Ultimately, the future of hair loss therapeutics will depend on interdisciplinary collaboration among dermatologists, bioengineers, pharmaceutical scientists, and AI experts. By integrating diverse expertise and prioritizing the development of antibody- and cell-based therapies, the field can accelerate the creation of innovative solutions to address the unmet needs of patients with hair loss disorders.
Author Contributions
J.K., S.-Y.S., and J.-H.S. contributed to the conceptualization, drafting, writing, reviewing, and editing of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Korean Fund for Regenerative Medicine funded by the Ministry of Science and ICT and the Ministry of Health and Welfare, Republic of Korea (grant numbers: 23C0125L1 and 24D0102L1).
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
Jong-Hyuk Sung is the CEO of Epi Biotech. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
References
- Guo, H.W.; Ye, Z.M.; Chen, S.Q.; McElwee, K.J. Innovative strategies for the discovery of new drugs against alopecia areata: Taking aim at the immune system. Expert. Opin. Drug Discov. 2024, 19, 1321–1338. [Google Scholar] [CrossRef] [PubMed]
- Vasserot, A.P.; Geyfman, M.; Poloso, N.J. Androgenetic alopecia: Combing the hair follicle signaling pathways for new therapeutic targets and more effective treatment options. Expert. Opin. Ther. Targets 2019, 23, 755–771. [Google Scholar] [CrossRef] [PubMed]
- Santos, Z.; Avci, P.; Hamblin, M.R. Drug discovery for alopecia: Gone today, hair tomorrow. Expert. Opin. Drug Discov. 2015, 10, 269–292. [Google Scholar] [CrossRef]
- Semalty, A.; Semalty, M.; Joshi, G.P.; Rawat, M.S. Techniques for the discovery and evaluation of drugs against alopecia. Expert. Opin. Drug Discov. 2011, 6, 309–321. [Google Scholar] [CrossRef]
- Shorter, K.; Farjo, N.P.; Picksley, S.M.; Randall, V.A. Human hair follicles contain two forms of ATP-sensitive potassium channels, only one of which is sensitive to minoxidil. FASEB J. 2008, 22, 1725–1736. [Google Scholar] [CrossRef]
- Lachgar, S.; Charveron, M.; Gall, Y.; Bonafe, J.L. Minoxidil upregulates the expression of vascular endothelial growth factor in human hair dermal papilla cells. Br. J. Dermatol. 1998, 138, 407–411. [Google Scholar] [CrossRef]
- Kwack, M.H.; Kang, B.M.; Kim, M.K.; Kim, J.C.; Sung, Y.K. Minoxidil activates beta-catenin pathway in human dermal papilla cells: A possible explanation for its anagen prolongation effect. J. Dermatol. Sci. 2011, 62, 154–159. [Google Scholar] [CrossRef]
- Dawber, R.P.; Rundegren, J. Hypertrichosis in females applying minoxidil topical solution and in normal controls. J. Eur. Acad. Dermatol. Venereol. 2003, 17, 271–275. [Google Scholar] [CrossRef]
- Adil, A.; Godwin, M. The effectiveness of treatments for androgenetic alopecia: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2017, 77, 136–141.e5. [Google Scholar] [CrossRef]
- van Zuuren, E.J.; Fedorowicz, Z.; Carter, B. Evidence-based treatments for female pattern hair loss: A summary of a Cochrane systematic review. Br. J. Dermatol. 2012, 167, 995–1010. [Google Scholar] [CrossRef]
- Vahabi-Amlashi, S.; Layegh, P.; Kiafar, B.; Hoseininezhad, M.; Abbaspour, M.; Khaniki, S.H.; Forouzanfar, M.; Sabeti, V. A randomized clinical trial on therapeutic effects of 0.25 mg oral minoxidil tablets on treatment of female pattern hair loss. Dermatol. Ther. 2021, 34, e15131. [Google Scholar] [CrossRef] [PubMed]
- Penha, M.A.; Miot, H.A.; Kasprzak, M.; Muller Ramos, P. Oral Minoxidil vs Topical Minoxidil for Male Androgenetic Alopecia: A Randomized Clinical Trial. JAMA Dermatol. 2024, 160, 600–605. [Google Scholar] [CrossRef] [PubMed]
- An, S.; Zheng, M.; Park, I.G.; Noh, M.; Sung, J.H. Differential expression of androgen receptor and 5-alpha reductase isoforms in skin cells. Arch. Dermatol. Res. 2024, 317, 138. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, J.; Wang, L.; Wang, H.; Chen, B. The Efficacy and Safety of Finasteride Combined with Topical Minoxidil for Androgenetic Alopecia: A Systematic Review and Meta-analysis. Aesthetic Plast. Surg. 2020, 44, 962–970. [Google Scholar] [CrossRef]
- Diviccaro, S.; Melcangi, R.C.; Giatti, S. Post-finasteride syndrome: An emerging clinical problem. Neurobiol. Stress. 2020, 12, 100209. [Google Scholar] [CrossRef]
- Safety update: Psychiatric and sexual adverse effects with finasteride. Drug Ther. Bull. 2024, 62, 101. [CrossRef]
- Almudimeegh, A.; AlMutairi, H.; AlTassan, F.; AlQuraishi, Y.; Nagshabandi, K.N. Comparison between dutasteride and finasteride in hair regrowth and reversal of miniaturization in male and female androgenetic alopecia: A systematic review. Dermatol. Rep. 2024, 16, 9909. [Google Scholar] [CrossRef]
- Herz-Ruelas, M.E.; Alvarez-Villalobos, N.A.; Millan-Alanis, J.M.; de Leon-Gutierrez, H.; Ocampo-Garza, S.S.; Gomez-Flores, M.; Grimalt, R. Efficacy of Intralesional and Oral Dutasteride in the Treatment of Androgenetic Alopecia: A Systematic Review. Skin. Appendage Disord. 2020, 6, 338–345. [Google Scholar] [CrossRef]
- Yale, K.; Pourang, A.; Plikus, M.V.; Mesinkovska, N.A. At the crossroads of 2 alopecias: Androgenetic alopecia pattern of hair regrowth in patients with alopecia areata treated with oral Janus kinase inhibitors. JAAD Case Rep. 2020, 6, 444–446. [Google Scholar] [CrossRef]
- Harel, S.; Higgins, C.A.; Cerise, J.E.; Dai, Z.; Chen, J.C.; Clynes, R.; Christiano, A.M. Pharmacologic inhibition of JAK-STAT signaling promotes hair growth. Sci. Adv. 2015, 1, e1500973. [Google Scholar] [CrossRef]
- Xing, L.; Dai, Z.; Jabbari, A.; Cerise, J.E.; Higgins, C.A.; Gong, W.; de Jong, A.; Harel, S.; DeStefano, G.M.; Rothman, L.; et al. Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition. Nat. Med. 2014, 20, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Kwon, O.; Senna, M.M.; Sinclair, R.; Ito, T.; Dutronc, Y.; Lin, C.Y.; Yu, G.; Chiasserini, C.; McCollam, J.; Wu, W.S.; et al. Efficacy and Safety of Baricitinib in Patients with Severe Alopecia Areata over 52 Weeks of Continuous Therapy in Two Phase III Trials (BRAVE-AA1 and BRAVE-AA2). Am. J. Clin. Dermatol. 2023, 24, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Sun Pharmaceutical Industries. U.S. FDA Approves LEQSELVI™ (deuruxolitinib), an Oral JAK Inhibitor for the Treatment of Severe Alopecia Areata. SUN PHARMA. 2024. Available online: https://www.prnewswire.com/news-releases/us-fda--approves-leqselvi-deuruxolitinib-an-oral-jak-inhibitor-for-the-treatment-of-severe-alopecia-areata-302207222.html (accessed on 12 February 2025).
- King, B.; Senna, M.M.; Mesinkovska, N.A.; Lynde, C.; Zirwas, M.; Maari, C.; Prajapati, V.H.; Sapra, S.; Brzewski, P.; Osman, L.; et al. Efficacy and safety of deuruxolitinib, an oral selective Janus kinase inhibitor, in adults with alopecia areata: Results from the Phase 3 randomized, controlled trial (THRIVE-AA1). J. Am. Acad. Dermatol. 2024, 91, 880–888. [Google Scholar] [CrossRef]
- Dai, Z.; Chen, J.; Chang, Y.; Christiano, A.M. Selective inhibition of JAK3 signaling is sufficient to reverse alopecia areata. JCI Insight 2021, 6, e142205. [Google Scholar] [CrossRef]
- Piliang, M.; Soung, J.; King, B.; Shapiro, J.; Rudnicka, L.; Farrant, P.; Magnolo, N.; Piraccini, B.M.; Luo, X.; Wolk, R.; et al. Efficacy and safety of the oral Janus kinase 3/tyrosine kinase expressed in hepatocellular carcinoma family kinase inhibitor ritlecitinib over 24 months: Integrated analysis of the ALLEGRO phase IIb/III and long-term phase III clinical studies in alopecia areata. Br. J. Dermatol. 2025, 192, 215–227. [Google Scholar] [CrossRef]
- Wang, Y.; Huh, Y.; Lejeune, A. Population exposure-response analysis of the effect of ritlecitinib on eyebrow assessment and eyelash assessment in patients with alopecia areata. CPT Pharmacomet. Syst. Pharmacol. 2025, 14, 389–402. [Google Scholar] [CrossRef]
- AbbVie, Inc. A Study to Evaluate the Safety and Effectiveness of Upadacitinib Tablets in Adult and Adolescent Participants with Severe Alopecia Areata (Up-AA). 2025. Available online: https://www.abbvieclinicaltrials.com/study/?id=M23-716 (accessed on 10 February 2025).
- Zelgen, S. Extension Study to Evaluate Safety and Efficacy of Jaktinib in Adults with Alopecia Areata. 2024. Available online: https://ctv.veeva.com/study/extension-study-to-evaluate-safety-and-efficacy-of-jaktinib-in-adults-with-alopecia-areata (accessed on 10 February 2025).
- Arcutis Biotherapeutics, Inc. Arcutis Completes Enrollment of Phase 1b Alopecia Areata Study Evaluating ARQ-255. Available online: https://www.arcutis.com/arcutis-completes-enrollment-of-phase-1b-alopecia-areata-study-evaluating-arq-255/ (accessed on 10 February 2025).
- Maeshima, T.; Aisu, S.; Ohkura, N.; Watanabe, M.; Itagaki, F. The Association Between Deep Vein Thrombosis, Pulmonary Embolism, and Janus Kinase Inhibitors: Reporting Status and Signal Detection in the Japanese Adverse Drug Event Report Database. Drugs Real. World Outcomes 2024, 11, 369–375. [Google Scholar] [CrossRef]
- Zhu, H.; Jian, Z.; Zhong, Y.; Ye, Y.; Zhang, Y.; Hu, X.; Pu, B.; Gu, L.; Xiong, X. Janus Kinase Inhibition Ameliorates Ischemic Stroke Injury and Neuroinflammation Through Reducing NLRP3 Inflammasome Activation via JAK2/STAT3 Pathway Inhibition. Front. Immunol. 2021, 12, 714943. [Google Scholar] [CrossRef]
- Gentile, P.; Garcovich, S. Advances in Regenerative Stem Cell Therapy in Androgenic Alopecia and Hair Loss: Wnt pathway, Growth-Factor, and Mesenchymal Stem Cell Signaling Impact Analysis on Cell Growth and Hair Follicle Development. Cells 2019, 8, 466. [Google Scholar] [CrossRef]
- Al-Refu, K. Stem cells and alopecia: A review of pathogenesis. Br. J. Dermatol. 2012, 167, 479–484. [Google Scholar] [CrossRef]
- Harries, M.J.; Paus, R. The pathogenesis of primary cicatricial alopecias. Am. J. Pathol. 2010, 177, 2152–2162. [Google Scholar] [CrossRef] [PubMed]
- Miao, Y.J.; Jing, J.; Du, X.F.; Mao, M.Q.; Yang, X.S.; Lv, Z.F. Frontal fibrosing alopecia: A review of disease pathogenesis. Front. Med. 2022, 9, 911944. [Google Scholar] [CrossRef]
- Charoensuksira, S.; Tantiwong, S.; Pongklaokam, J.; Hanvivattanakul, S.; Surinlert, P.; Krajarng, A.; Thanasarnaksorn, W.; Hongeng, S.; Ponnikorn, S. Disturbance of Immune Microenvironment in Androgenetic Alopecia through Spatial Transcriptomics. Int. J. Mol. Sci. 2024, 25, 9031. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Jacobo, L.; Villarreal-Villarreal, C.D.; Ortiz-Lopez, R.; Ocampo-Candiani, J.; Rojas-Martinez, A. Genetic and molecular aspects of androgenetic alopecia. Indian. J. Dermatol. Venereol. Leprol. 2018, 84, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.C.E.; Christiano, A.M. The Changing Landscape of Alopecia Areata: The Translational Landscape. Adv. Ther. 2017, 34, 1586–1593. [Google Scholar] [CrossRef]
- Cosmo Pharmaceuticals, Inc. Cosmo Announces the Beginning of the Phase III Trials in Males for the Treatment of Androgenetic Alopecia. 2023. Available online: https://www.cosmopharma.com/news/cosmo-announces-the-beginning-of-the-phase-iii-trials-in-males-for-the-treatment-of-androgenetic-alopecia (accessed on 10 February 2025).
- Cosmo Pharmaceuticals, Inc. Winlevi® (Clascoterone). Available online: https://www.cosmopharma.com/products/winlevi (accessed on 10 February 2025).
- Dhillon, S. Clascoterone: First Approval. Drugs 2020, 80, 1745–1750. [Google Scholar] [CrossRef]
- Lama, S.C. Kintor Announces Update on KX-826 (Pyrilutamide) for Hair Loss. 2023. Available online: https://hairscience.org/news/kintor-usa-clinical-trial-pyrilutamide-results/ (accessed on 12 February 2025).
- Kintor Pharmaceuticals, Inc. First Subject Enrollment in Phase 3 Stage of KX-826 1.0% For AGA. Available online: https://en.kintor.com.cn/news_details/6.html (accessed on 10 February 2025).
- Kintor Pharmaceuticals, Inc. Completion of First Subject Enrollment in Phase II Clinical Trial of GT20029 Gel for Treatment of Acne in China. Available online: https://en.kintor.com.cn/news_details/1803365118859653120.html (accessed on 10 February 2025).
- OliX Pharmaceuticals, Inc. OliX Pharmaceuticals Receives Regulatory Approval to Commence Phase 1 Clinical Trial of Treatment of Androgenic Alopecia. Olix Pharmaceuticals. 2023. Available online: https://www.businesswire.com/news/home/20230323005383/en/OliX-Pharmaceuticals-Receives-Regulatory-Approval-to-Commence-Phase-1-Clinical-Trial-of-Treatment-of-Androgenic-Alopecia (accessed on 10 February 2025).
- Anranda Pharma, Inc. ADA-308 for Androgenetic Alopecia. Available online: https://arandapharma.com/ada-308-for-androgenetic-alopecia.html#/ (accessed on 12 February 2025).
- Choi, B.Y. Targeting Wnt/beta-Catenin Pathway for Developing Therapies for Hair Loss. Int. J. Mol. Sci. 2020, 21, 4915. [Google Scholar] [CrossRef]
- Ryu, Y.C.; Lee, D.H.; Shim, J.; Park, J.; Kim, Y.R.; Choi, S.; Bak, S.S.; Sung, Y.K.; Lee, S.H.; Choi, K.Y. KY19382, a novel activator of Wnt/beta-catenin signalling, promotes hair regrowth and hair follicle neogenesis. Br. J. Pharmacol. 2021, 178, 2533–2546. [Google Scholar] [CrossRef]
- Technoderma Medicines, Inc. A Randomized, Double-Blind, Vehicle-Controlled, Parallel Group, Multi-Dose Study to Evaluate the Efficacy and Safety of TDM-105795 in Male Subjects with Androgenetic Alopecia. 2024. Available online: https://adisinsight.springer.com/trials/700361593 (accessed on 10 February 2025).
- Garza, L.A.; Liu, Y.; Yang, Z.; Alagesan, B.; Lawson, J.A.; Norberg, S.M.; Loy, D.E.; Zhao, T.; Blatt, H.B.; Stanton, D.C.; et al. Prostaglandin D2 inhibits hair growth and is elevated in bald scalp of men with androgenetic alopecia. Sci. Transl. Med. 2012, 4, 126ra134. [Google Scholar] [CrossRef]
- Pelage Pharmaceuticals, Inc. Pelage Pharmaceuticals Advances Clinical Program with First Patients Dosed in Phase 2 Study for Hair Loss and GV-Led $14M Series A-1 NEWS PROVIDED BY Pelage Pharmaceuticals. Available online: https://www.prnewswire.com/news-releases/pelage-pharmaceuticals-advances-clinical-program-with-first-patients-dosed-in-phase-2-study-for-hair-loss-and-gv-led-14m-series-a-1-302220301.html (accessed on 10 February 2025).
- Keren, A.; Shemer, A.; Ullmann, Y.; Paus, R.; Gilhar, A. The PDE4 inhibitor, apremilast, suppresses experimentally induced alopecia areata in human skin in vivo. J. Dermatol. Sci. 2015, 77, 74–76. [Google Scholar] [CrossRef]
- Zheng, M.; Choi, N.; Jang, Y.; Kwak, D.E.; Kim, Y.; Kim, W.S.; Oh, S.H.; Sung, J.H. Hair growth promotion by necrostatin-1s. Sci. Rep. 2020, 10, 17622. [Google Scholar] [CrossRef] [PubMed]
- Equillium, Inc. EQ101 phase 2 study. Available online: https://www.equilliumbio.com/EQ101-Phase-2-Study/ (accessed on 23 February 2025).
- Jacob, A.; Raj, R.; Allison, D.B.; Myint, Z.W. Androgen Receptor Signaling in Prostate Cancer and Therapeutic Strategies. Cancers 2021, 13, 5417. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Zhang, J.Y.; Zhao, L.J.; Guo, Y.Y. Synthesis and application of clinically approved small-molecule drugs targeting androgen receptor. Bioorg Chem. 2024, 143, 106998. [Google Scholar] [CrossRef]
- Wang, C.; Du, Y.; Bi, L.; Lin, X.; Zhao, M.; Fan, W. The Efficacy and Safety of Oral and Topical Spironolactone in Androgenetic Alopecia Treatment: A Systematic Review. Clin. Cosmet. Investig. Dermatol. 2023, 16, 603–612. [Google Scholar] [CrossRef]
- Rathnayake, D.; Sinclair, R. Use of spironolactone in dermatology. Skinmed 2010, 8, 328–332, quiz 333. [Google Scholar]
- Sun, H.Y.; Sebaratnam, D.F. Clascoterone as a novel treatment for androgenetic alopecia. Clin. Exp. Dermatol. 2020, 45, 913–914. [Google Scholar] [CrossRef]
- Saceda-Corralo, D.; Dominguez-Santas, M.; Vano-Galvan, S.; Grimalt, R. What’s New in Therapy for Male Androgenetic Alopecia? Am. J. Clin. Dermatol. 2023, 24, 15–24. [Google Scholar] [CrossRef]
- Moon, I.J.; Yoon, H.K.; Kim, D.; Choi, M.E.; Han, S.H.; Park, J.H.; Hong, S.W.; Cho, H.; Lee, D.K.; Won, C.H. Efficacy of Asymmetric siRNA Targeting Androgen Receptors for the Treatment of Androgenetic Alopecia. Mol. Pharm. 2023, 20, 128–135. [Google Scholar] [CrossRef]
- Biosplice Therapeutics, I. A Study of SM04554 Applied Topically to the Scalp of Male Subjects with Androgenetic Alopecia Analyzed by Biopsy of the Scalp Prior To and Post Dosing; Biosplice Therapeutics, Inc.: San Diego, CA, USA, 2020. [Google Scholar]
- JW Pharmaceutical, Inc. Hair Loss Treatment by JW0061-Mediated Wnt Modulation for “Growth in Hair Length & Follicular Number”. 2022. Available online: https://www.jw-pharma.co.kr/pharma/en/prcenter/all_view.jsp?contentsCd=230103120310932ATI8D (accessed on 10 February 2025).
- Adly, M.A.; Assaf, H.A.; Pertile, P.; Hussein, M.R.; Paus, R. Expression patterns of the glial cell line-derived neurotrophic factor, neurturin, their cognate receptors GFRalpha-1, GFRalpha-2, and a common signal transduction element c-Ret in the human skin hair follicles. J. Am. Acad. Dermatol. 2008, 58, 238–250. [Google Scholar] [CrossRef]
- Antonini, D.; Sibilio, A.; Dentice, M.; Missero, C. An Intimate Relationship between Thyroid Hormone and Skin: Regulation of Gene Expression. Front. Endocrinol. 2013, 4, 104. [Google Scholar] [CrossRef]
- Contreras-Jurado, C.; Garcia-Serrano, L.; Martinez-Fernandez, M.; Ruiz-Llorente, L.; Paramio, J.M.; Aranda, A. Impaired hair growth and wound healing in mice lacking thyroid hormone receptors. PLoS ONE 2014, 9, e108137. [Google Scholar] [CrossRef]
- Contreras-Jurado, C.; Lorz, C.; Garcia-Serrano, L.; Paramio, J.M.; Aranda, A. Thyroid hormone signaling controls hair follicle stem cell function. Mol. Biol. Cell 2015, 26, 1263–1272. [Google Scholar] [CrossRef]
- Zhi, J.; Li, F.; Jiang, X.; Bai, R. Thyroid receptor beta: A promising target for developing novel anti-androgenetic alopecia drugs. Drug Discov. Today 2024, 29, 104013. [Google Scholar] [CrossRef] [PubMed]
- Zhu, P.; Deng, W.; Yu, J.; Yang, S. Thyroid Hormone Receptor Agonist Promotes Hair Growth in Mice. Clin. Cosmet. Investig. Dermatol. 2022, 15, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Hossein Mostafa, D.; Samadi, A.; Niknam, S.; Nasrollahi, S.A.; Guishard, A.; Firooz, A. Efficacy of Cetirizine 1% Versus Minoxidil 5% Topical Solution in the Treatment of Male Alopecia: A Randomized, Single-blind Controlled Study. J. Pharm. Pharm. Sci. 2021, 24, 191–199. [Google Scholar] [CrossRef]
- Tosti, A.; Pazzaglia, M.; Voudouris, S.; Tosti, G. Hypertrichosis of the eyelashes caused by bimatoprost. J. Am. Acad. Dermatol. 2004, 51, S149–S150. [Google Scholar] [CrossRef]
- Choi, Y.M.; Diehl, J.; Levins, P.C. Promising alternative clinical uses of prostaglandin F2alpha analogs: Beyond the eyelashes. J. Am. Acad. Dermatol. 2015, 72, 712–716. [Google Scholar] [CrossRef]
- Ceyhan, Ç.; Düzkar, S.; Kandemir, O.; Özdal, M.Ö.; Erbaş, O. Effect of lactate dehydrogenase activity on hair follicle stem cell. Demiroglu Sci. Univ. Florence Nightngale J. Med. 2017, 3, 139–145. [Google Scholar] [CrossRef]
- Li, S.; Yu, J.; Zhang, J.; Li, X.; Yu, J. LSD1 interacting with HSP90 promotes skin wound healing by inducing metabolic reprogramming of hair follicle stem cells through the c-MYC/LDHA axis. FASEB J. 2023, 37, e23031. [Google Scholar] [CrossRef]
- Jelinek, D.; Flores, A.; Uebelhoer, M.; Pasque, V.; Plath, K.; Iruela-Arispe, M.L.; Christofk, H.R.; Lowry, W.E.; Coller, H.A. Mapping Metabolism: Monitoring Lactate Dehydrogenase Activity Directly in Tissue. J. Vis. Exp. 2018, 136, 57760. [Google Scholar] [CrossRef]
- Flores, A.; Schell, J.; Krall, A.S.; Jelinek, D.; Miranda, M.; Grigorian, M.; Braas, D.; White, A.C.; Zhou, J.L.; Graham, N.A.; et al. Lactate dehydrogenase activity drives hair follicle stem cell activation. Nat. Cell Biol. 2017, 19, 1017–1026. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Lu, J.; Yi, X.; Ding, Y.; Gao, Y.; Chen, W. Development of alopecia areata during phosphodiesterase 4 inhibitor treatment for psoriasis: A case report. Dermatol. Ther. 2020, 33, e14440. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Farinas, M.; Ungar, B.; Noda, S.; Shroff, A.; Mansouri, Y.; Fuentes-Duculan, J.; Czernik, A.; Zheng, X.; Estrada, Y.D.; Xu, H.; et al. Alopecia areata profiling shows TH1, TH2, and IL-23 cytokine activation without parallel TH17/TH22 skewing. J. Allergy Clin. Immunol. 2015, 136, 1277–1287. [Google Scholar] [CrossRef]
- Jang, Y.H.; Jin, M.; Moon, S.Y.; Eun, D.H.; Lee, W.J.; Lee, S.J.; Kim, M.K.; Kim, S.H.; do Kim, W. Investigation on the role of necroptosis in alopecia areata: A preliminary study. J. Am. Acad. Dermatol. 2016, 75, 436–439. [Google Scholar] [CrossRef]
- Starace, M.; Cedirian, S.; Quadrelli, F.; Pampaloni, F.; Brunetti, T.; Chessa, M.A.; Gurioli, C.; Piraccini, B.M.; Neri, I. Dupilumab and Alopecia Areata: A Possible Combined or Disturbance Therapy? A Review of The Literature. Dermatol. Pract. Concept. 2024, 14, e2024270. [Google Scholar] [CrossRef]
- Hong, J.J.; Hadeler, E.K.; Mosca, M.L.; Brownstone, N.D.; Bhutani, T.; Liao, W.J. Off-label uses of TNF-a inhibitors and IL-12/23 inhibitors in dermatology. Dermatol. Online J. 2021, 27, D3271156085. [Google Scholar] [CrossRef]
- Jin, S.E.; Kim, J.; Sung, J.H. Recent approaches of antibody therapeutics in androgenetic alopecia. Front. Pharmacol. 2024, 15, 1434961. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Renert-Yuval, Y.; Bares, J.; Chima, M.; Hawkes, J.E.; Gilleaudeau, P.; Sullivan-Whalen, M.; Singer, G.K.; Garcet, S.; Pavel, A.B.; et al. Phase 2a randomized clinical trial of dupilumab (anti-IL-4Ralpha) for alopecia areata patients. Allergy 2022, 77, 897–906. [Google Scholar] [CrossRef]
- Tauber, M.; Beneton, N.; Reygagne, P.; Bachelez, H.; Viguier, M. Alopecia areata developing during ustekinumab therapy: Report of two cases. Eur. J. Dermatol. 2013, 23, 912–913. [Google Scholar] [CrossRef]
- Kirshen, C.; Kanigsberg, N. Alopecia areata following adalimumab. J. Cutan. Med. Surg. 2009, 13, 48–50. [Google Scholar] [CrossRef]
- Hope Medicine, Inc. Hope Medicine Announces US FDA Clearance for Phase II Clinical Trial of A First-in-class Monoclonal Antibody, HMI-115, in AGA Alopecia. 2022. Available online: https://www.hopemedinc.com/company-release-5 (accessed on 3 February 2024).
- Zheng, M.; Oh, S.H.; Choi, N.; Choi, Y.J.; Kim, J.; Sung, J.H. CXCL12 inhibits hair growth through CXCR4. Biomed. Pharmacother. 2022, 150, 112996. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; An, S.; Park, I.G.; Kim, J.; Kim, W.S.; Noh, M.; Sung, J.H. Differential Expression of CXCL12 in Human and Mouse Hair: Androgens Induce CXCL12 in Human Dermal Papilla and Dermal Sheath Cup. Int. J. Mol. Sci. 2024, 26, 95. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Kim, M.H.; Park, S.G.; Kim, W.S.; Oh, S.H.; Sung, J.H. CXCL12 Neutralizing Antibody Promotes Hair Growth in Androgenic Alopecia and Alopecia Areata. Int. J. Mol. Sci. 2024, 25, 1705. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Jian, J.; Li, T.; Li, M.; Luo, K.; Deng, S.; Tang, Y.; Liu, F.; Zhao, Z.; Shi, W.; et al. Dupliumab therapy for alopecia areata: A case series and review of the literature. J. Dermatolog Treat. 2024, 35, 2312245. [Google Scholar] [CrossRef]
- Foitzik, K.; Krause, K.; Conrad, F.; Nakamura, M.; Funk, W.; Paus, R. Human scalp hair follicles are both a target and a source of prolactin, which serves as an autocrine and/or paracrine promoter of apoptosis-driven hair follicle regression. Am. J. Pathol. 2006, 168, 748–756. [Google Scholar] [CrossRef]
- Craven, A.J.; Nixon, A.J.; Ashby, M.G.; Ormandy, C.J.; Blazek, K.; Wilkins, R.J.; Pearson, A.J. Prolactin delays hair regrowth in mice. J. Endocrinol. 2006, 191, 415–425. [Google Scholar] [CrossRef]
- Langan, E.A.; Griffiths, C.E.; Paus, R. Utilizing the hair follicle to dissect the regulation and autocrine/paracrine activities of prolactin in humans. Am. J. Physiol. Endocrinol. Metab. 2012, 302, E1311–E1312. [Google Scholar] [CrossRef]
- Reiter, E.; Bonnet, P.; Sente, B.; Dombrowicz, D.; de Leval, J.; Closset, J.; Hennen, G. Growth hormone and prolactin stimulate androgen receptor, insulin-like growth factor-I (IGF-I) and IGF-I receptor levels in the prostate of immature rats. Mol. Cell Endocrinol. 1992, 88, 77–87. [Google Scholar] [CrossRef]
- Ratajczak, M.Z.; Zuba-Surma, E.; Kucia, M.; Reca, R.; Wojakowski, W.; Ratajczak, J. The pleiotropic effects of the SDF-1-CXCR4 axis in organogenesis, regeneration and tumorigenesis. Leukemia 2006, 20, 1915–1924. [Google Scholar] [CrossRef]
- Ma, Z.; Zhou, F.; Jin, H.; Wu, X. Crosstalk between CXCL12/CXCR4/ACKR3 and the STAT3 Pathway. Cells 2024, 13, 1027. [Google Scholar] [CrossRef]
- Cuesta-Margolles, G.; Schlecht-Louf, G.; Bachelerie, F. ACKR3 in Skin Homeostasis, an Overlooked Player in the CXCR4/CXCL12 Axis. J. Investig. Dermatol. 2024, articles in press. [Google Scholar] [CrossRef]
- Lin, W.H.; Xiang, L.J.; Shi, H.X.; Zhang, J.; Jiang, L.P.; Cai, P.T.; Lin, Z.L.; Lin, B.B.; Huang, Y.; Zhang, H.L.; et al. Fibroblast growth factors stimulate hair growth through beta-catenin and Shh expression in C57BL/6 mice. Biomed. Res. Int. 2015, 2015, 730139. [Google Scholar] [CrossRef]
- Liu, C.; Zhao, H.; Zhang, Y.; Wu, W. Clinical observation of basic fibroblast growth factor (bFGF) combined with minoxidil in the treatment of male androgenetic alopecia. J. Cosmet. Dermatol. 2022, 21, 4053–4059. [Google Scholar] [CrossRef] [PubMed]
- Yano, K.; Brown, L.F.; Detmar, M. Control of hair growth and follicle size by VEGF-mediated angiogenesis. J. Clin. Investig. 2001, 107, 409–417. [Google Scholar] [CrossRef]
- Ding, Y.W.; Li, Y.; Zhang, Z.W.; Dao, J.W.; Wei, D.X. Hydrogel forming microneedles loaded with VEGF and Ritlecitinib/polyhydroxyalkanoates nanoparticles for mini-invasive androgenetic alopecia treatment. Bioact. Mater. 2024, 38, 95–108. [Google Scholar] [CrossRef]
- Ahn, S.Y.; Pi, L.Q.; Hwang, S.T.; Lee, W.S. Effect of IGF-I on Hair Growth Is Related to the Anti-Apoptotic Effect of IGF-I and Up-Regulation of PDGF-A and PDGF-B. Ann. Dermatol. 2012, 24, 26–31. [Google Scholar] [CrossRef]
- Neely, E.K.; Morhenn, V.B.; Hintz, R.L.; Wilson, D.M.; Rosenfeld, R.G. Insulin-like growth factors are mitogenic for human keratinocytes and a squamous cell carcinoma. J. Invest. Dermatol. 1991, 96, 104–110. [Google Scholar] [CrossRef]
- Gonzalez, R.; Moffatt, G.; Hagner, A.; Sinha, S.; Shin, W.; Rahmani, W.; Chojnacki, A.; Biernaskie, J. Platelet-derived growth factor signaling modulates adult hair follicle dermal stem cell maintenance and self-renewal. NPJ Regen. Med. 2017, 2, 11. [Google Scholar] [CrossRef]
- Danilenko, D.M.; Ring, B.D.; Yanagihara, D.; Benson, W.; Wiemann, B.; Starnes, C.O.; Pierce, G.F. Keratinocyte growth factor is an important endogenous mediator of hair follicle growth, development, and differentiation. Normalization of the nu/nu follicular differentiation defect and amelioration of chemotherapy-induced alopecia. Am. J. Pathol. 1995, 147, 145–154. [Google Scholar]
- Paichitrojjana, A.; Paichitrojjana, A. Platelet Rich Plasma and Its Use in Hair Regrowth: A Review. Drug Des. Devel Ther. 2022, 16, 635–645. [Google Scholar] [CrossRef]
- Yuan, J.; He, Y.; Wan, H.; Gao, Y. Effectiveness of platelet-rich plasma in treating female hair loss: A systematic review and meta-analysis of randomized controlled trials. Skin. Res. Technol. 2024, 30, e70004. [Google Scholar] [CrossRef]
- Shon, U.; Kim, M.H.; Lee, D.Y.; Kim, S.H.; Park, B.C. The effect of intradermal botulinum toxin on androgenetic alopecia and its possible mechanism. J. Am. Acad. Dermatol. 2020, 83, 1838–1839. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, R.; Niiyama, S.; Irisawa, R.; Harada, K.; Nakazawa, Y.; Kishimoto, J. Autologous cell-based therapy for male and female pattern hair loss using dermal sheath cup cells: A randomized placebo-controlled double-blinded dose-finding clinical study. J. Am. Acad. Dermatol. 2020, 83, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Harada, K.; Ohyama, M.; Niiyama, S.; Irisawa, R.; Mae, K.; Mori, M.; Wakimoto, H.; Kinoshita-Ise, M.; Fukuyama, M.; Hayakawa, R.; et al. Efficacy of autologous dermal sheath cup cell transplantation in male and female pattern hair loss: A Single-Arm, Multi-Center, phase III equivalent clinical study. J. Dermatol. 2023, 50, 1539–1549. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Zheng, M.; Le, T.N.H.; Kim, H.; Sung, J.H. Hair growth promoting effects of human dermal papilla cells in pig. Exp. Dermatol. 2023, 32, 1156–1158. [Google Scholar] [CrossRef]
- Epi Biotech, Inc. Epibiotech, approved by the MFDS for phase 1/2a clinical trials for dermal papilla hair loss treatment. Available online: https://epibiotech.com (accessed on 25 December 2023).
- El-Khalawany, M.; Rageh, M.A.; Elnokrashy, I.; Ibrahim, S.M.A. Efficacy of autologous stromal vascular fraction injection in the treatment of androgenic alopecia. Arch. Dermatol. Res. 2023, 315, 1269–1276. [Google Scholar] [CrossRef]
- Anderi, R.; Makdissy, N.; Azar, A.; Rizk, F.; Hamade, A. Cellular therapy with human autologous adipose-derived adult cells of stromal vascular fraction for alopecia areata. Stem Cell Res. Ther. 2018, 9, 141. [Google Scholar] [CrossRef]
- Kim, S.J.; Kim, M.J.; Lee, Y.J.; Lee, J.C.; Kim, J.H.; Kim, D.H.; Do, Y.H.; Choi, J.W.; Chung, S.I.; Do, B.R. Innovative method of alopecia treatment by autologous adipose-derived SVF. Stem Cell Res. Ther. 2021, 12, 486. [Google Scholar] [CrossRef]
- Nassar, A.; Abdel-Aleem, H.; Samir, M.; Khattab, F.M. Efficacy of botulinum toxin A injection in the treatment of androgenic alopecia: A Comparative Controlled Study. J. Cosmet. Dermatol. 2022, 21, 4261–4268. [Google Scholar] [CrossRef]
- Singh, S.; Neema, S.; Vasudevan, B. A Pilot Study to Evaluate Effectiveness of Botulinum Toxin in Treatment of Androgenetic Alopecia in Males. J. Cutan. Aesthet. Surg. 2017, 10, 163–167. [Google Scholar] [CrossRef]
- Nguyen, B.; Perez, S.M.; Tosti, A. Botulinum Toxin for Scalp Conditions: A Systematic Review. Dermatol. Surg. 2023, 49, 1023–1026. [Google Scholar] [CrossRef]
- English, R.S., Jr.; Ruiz, S. Use of Botulinum Toxin for Androgenic Alopecia: A Systematic Review. Skin. Appendage Disord. 2022, 8, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.H. Effective and economical cell therapy for hair regeneration. Biomed. Pharmacother. 2023, 157, 113988. [Google Scholar] [CrossRef] [PubMed]
- Gentile, P.; Scioli, M.G.; Bielli, A.; Orlandi, A.; Cervelli, V. Stem cells from human hair follicles: First mechanical isolation for immediate autologous clinical use in androgenetic alopecia and hair loss. Stem Cell Investig. 2017, 4, 58. [Google Scholar] [CrossRef] [PubMed]
- Gentile, P.; Scioli, M.G.; Cervelli, V.; Orlandi, A.; Garcovich, S. Autologous Micrografts from Scalp Tissue: Trichoscopic and Long-Term Clinical Evaluation in Male and Female Androgenetic Alopecia. Biomed. Res. Int. 2020, 2020, 7397162. [Google Scholar] [CrossRef]
- Ishimatsu-Tsuji, Y.; Niiyama, S.; Irisawa, R.; Harada, K.; Kishimoto, J.; Tsuboi, R. High migratory activity of dermal sheath cup cells associated with the clinical efficacy of autologous cell-based therapy for pattern hair loss. J. Dermatol. Sci. 2024, 113, 26–33. [Google Scholar] [CrossRef]
- Reynolds, A.J.; Jahoda, C.A. Cultured dermal papilla cells induce follicle formation and hair growth by transdifferentiation of an adult epidermis. Development 1992, 115, 587–593. [Google Scholar] [CrossRef]
- Kim, H.; Choi, N.; Kim, D.Y.; Kim, S.Y.; Song, S.Y.; Sung, J.H. TGF-beta2 and collagen play pivotal roles in the spheroid formation and anti-aging of human dermal papilla cells. Aging 2021, 13, 19978–19995. [Google Scholar] [CrossRef]
- Zheng, M.; Jang, Y.; Choi, N.; Kim, D.Y.; Han, T.W.; Yeo, J.H.; Lee, J.; Sung, J.H. Hypoxia improves hair inductivity of dermal papilla cells via nuclear NADPH oxidase 4-mediated reactive oxygen species generation’. Br. J. Dermatol. 2019, 181, 523–534. [Google Scholar] [CrossRef]
- Yamao, M.; Inamatsu, M.; Ogawa, Y.; Toki, H.; Okada, T.; Toyoshima, K.E.; Yoshizato, K. Contact between dermal papilla cells and dermal sheath cells enhances the ability of DPCs to induce hair growth. J. Investig. Dermatol. 2010, 130, 2707–2718. [Google Scholar] [CrossRef]
- Hye Kim, J.; Gyu Park, S.; Kim, W.K.; Song, S.U.; Sung, J.H. Functional regulation of adipose-derived stem cells by PDGF-D. Stem Cells 2015, 33, 542–556. [Google Scholar] [CrossRef]
- Yi, T.; Kim, W.K.; Choi, J.S.; Song, S.Y.; Han, J.; Kim, J.H.; Kim, W.S.; Park, S.G.; Lee, H.J.; Cho, Y.K.; et al. Isolation of adipose-derived stem cells by using a subfractionation culturing method. Expert. Opin. Biol. Ther. 2014, 14, 1551–1560. [Google Scholar] [CrossRef] [PubMed]
- Choi, N.; Kim, W.S.; Oh, S.H.; Sung, J.H. HB-EGF Improves the Hair Regenerative Potential of Adipose-Derived Stem Cells via ROS Generation and Hck Phosphorylation. Int. J. Mol. Sci. 2019, 21, 122. [Google Scholar] [CrossRef] [PubMed]
- Choi, N.; Hwang, J.; Kim, D.Y.; Kim, J.; Song, S.Y.; Sung, J.H. Involvement of DKK1 secreted from adipose-derived stem cells in alopecia areata. Cell Prolif. 2024, 57, e13562. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, W.K.; Sung, Y.K.; Kwack, M.H.; Song, S.Y.; Choi, J.S.; Park, S.G.; Yi, T.; Lee, H.J.; Kim, D.D.; et al. The molecular mechanism underlying the proliferating and preconditioning effect of vitamin C on adipose-derived stem cells. Stem Cells Dev. 2014, 23, 1364–1376. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, S.G.; Song, S.Y.; Kim, J.K.; Sung, J.H. Reactive oxygen species-responsive miR-210 regulates proliferation and migration of adipose-derived stem cells via PTPN2. Cell Death Dis. 2013, 4, e588. [Google Scholar] [CrossRef]
- Song, S.Y.; Chung, H.M.; Sung, J.H. The pivotal role of VEGF in adipose-derived-stem-cell-mediated regeneration. Expert. Opin. Biol. Ther. 2010, 10, 1529–1537. [Google Scholar] [CrossRef]
- Yang, J.A.; Chung, H.M.; Won, C.H.; Sung, J.H. Potential application of adipose-derived stem cells and their secretory factors to skin: Discussion from both clinical and industrial viewpoints. Expert. Opin. Biol. Ther. 2010, 10, 495–503. [Google Scholar] [CrossRef]
- Tak, Y.J.; Lee, S.Y.; Cho, A.R.; Kim, Y.S. A randomized, double-blind, vehicle-controlled clinical study of hair regeneration using adipose-derived stem cell constituent extract in androgenetic alopecia. Stem Cells Transl. Med. 2020, 9, 839–849. [Google Scholar] [CrossRef]
- Legiawati, L.; Suseno, L.S.; Sitohang, I.B.S.; Yusharyahya, S.N.; Pawitan, J.A.; Liem, I.K.; Kurniawati, T.; Ardelia, A.; Paramastri, K. Combination of adipose-derived stem cell conditioned media and minoxidil for hair regrowth in male androgenetic alopecia: A randomized, double-blind clinical trial. Stem Cell Res. Ther. 2023, 14, 210. [Google Scholar] [CrossRef]
- Lee, Y.I.; Kim, J.; Kim, J.; Park, S.; Lee, J.H. The Effect of Conditioned Media From Human Adipocyte-Derived Mesenchymal Stem Cells on Androgenetic Alopecia After Nonablative Fractional Laser Treatment. Dermatol. Surg. 2020, 46, 1698–1704. [Google Scholar] [CrossRef]
- Mantovani, G.P.; Marra, C.; De Maria, F.; Pinto, V.; De Santis, G. Adipose-derived stromal vascular fraction (SVF) for the treatment of androgenic alopecia (AGA): A systematic review. Acta Biomed. 2023, 94, e2023236. [Google Scholar] [CrossRef]
- Kang, B.Y.; Li, A.W.; Lee, M.H.; Wong, C.C.; Naseer, N.; Ibrahim, S.A.; Miller, C.H.; Keimig, E.L.; Poon, E.; Alam, M. The safety and efficacy of autologous adipose-derived stromal vascular fraction for nonscarring alopecia: A systematic review. Arch. Dermatol. Res. 2022, 314, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Goncharov, E.N.; Koval, O.A.; Igorevich, E.I.; Encarnacion Ramirez, M.J.; Nurmukhametov, R.; Valentinovich, K.K.; Montemurro, N. Analyzing the Clinical Potential of Stromal Vascular Fraction: A Comprehensive Literature Review. Medicina 2024, 60, 221. [Google Scholar] [CrossRef] [PubMed]
- Butt, G.; Hussain, I.; Ahmad, F.J.; Choudhery, M.S. Stromal vascular fraction-enriched platelet-rich plasma therapy reverses the effects of androgenetic alopecia. J. Cosmet. Dermatol. 2020, 19, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.; Ma, C.; Chen, H.D.; Wu, Y.; Xu, X.G. The Roles of Exosomes in Regulating Hair Follicle Growth. Clin. Cosmet. Investig. Dermatol. 2024, 17, 1603–1612. [Google Scholar] [CrossRef]
- Queen, D.; Avram, M.R. Exosomes for Treating Hair Loss: A Review of Clinical Studies. Dermatol. Surg. 2024, 51, 409–415. [Google Scholar] [CrossRef]
- Piraccini, B.M.; Blume-Peytavi, U.; Scarci, F.; Jansat, J.M.; Falques, M.; Otero, R.; Tamarit, M.L.; Galvan, J.; Tebbs, V.; Massana, E.; et al. Efficacy and safety of topical finasteride spray solution for male androgenetic alopecia: A phase III, randomized, controlled clinical trial. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 286–294. [Google Scholar] [CrossRef]
- Kim, H.; Ryu, C.; Lee, M.; Lee, K.R.; Kim, J. A Phase I, Open-Label, Sequential, Single-Dose Clinical Trial to Evaluate the Pharmacokinetic, Pharmacodynamic, and Safety of IVL3001, a Finasteride-Based Novel Long-Acting Injection for Androgenetic Alopecia. Adv. Ther. 2024, 41, 2936–2952. [Google Scholar] [CrossRef]
- Hwang, K.M.; Choi, M.S.; Seok, S.H.; Park, E.S. Development of self-microemulsifying tablets containing dutasteride for enhanced dissolution and pharmacokinetic profile. Int. J. Pharm. 2022, 618, 121660. [Google Scholar] [CrossRef]
- Kushwaha, P.; Usmani, S.; Sufiyan, M.; Singh, P. Innovating alopecia treatment: Nanostructured lipid carriers as advanced delivery platforms. Naunyn Schmiedebergs Arch. Pharmacol. 2025. [Google Scholar] [CrossRef]
- Paredes, A.J.; Volpe-Zanutto, F.; Permana, A.D.; Murphy, A.J.; Picco, C.J.; Vora, L.K.; Coulter, J.A.; Donnelly, R.F. Novel tip-loaded dissolving and implantable microneedle array patches for sustained release of finasteride. Int. J. Pharm. 2021, 606, 120885. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Eum, J.; Yang, H.; Jung, H. Transdermal finasteride delivery via powder-carrying microneedles with a diffusion enhancer to treat androgenetic alopecia. J. Control Release 2019, 316, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Afika, N.; Saniy, A.F.; Fawwaz Dharma, A.A.; Ko, C.K.; Kamran, R.; Permana, A.D. Trilayer dissolving microneedle for transdermal delivery of minoxidil: A proof-of-concept study. J. Biomater. Sci. Polym. Ed. 2024, 35, 1750–1770. [Google Scholar] [CrossRef]
- Sun, Y.; Yang, L.; Du, L.; Zhou, Y.; Xu, K.; Chen, J.; He, Y.; Qu, Q.; Miao, Y.; Xing, M.; et al. Duo-role Platelet-rich Plasma: Temperature-induced fibrin gel and growth factors’ reservoir for microneedles to promote hair regrowth. J. Adv. Res. 2024, 55, 89–102. [Google Scholar] [CrossRef]
- Wang, X.; Cheng, W.; Su, J. Research Progress of Extracellular Vesicles-Loaded Microneedle Technology. Pharmaceutics 2024, 16, 326. [Google Scholar] [CrossRef]
- Yang, G.; Chen, Q.; Wen, D.; Chen, Z.; Wang, J.; Chen, G.; Wang, Z.; Zhang, X.; Zhang, Y.; Hu, Q.; et al. A Therapeutic Microneedle Patch Made from Hair-Derived Keratin for Promoting Hair Regrowth. ACS Nano 2019, 13, 4354–4360. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).