


The Stress of Measuring Plantar Tissue Stress in People with Diabetes-Related Foot Ulcers: Biomechanical and Feasibility Findings from Two Prospective Cohort Studies

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
1.1. Global Burden of Diabetes and Foot Ulcers
1.2. Mechanical Stress Is Still Poorly Understood
1.3. Challenging Equipment of Sensors
1.4. Aims and Hypotheses
2. Materials and Methods
2.1. Design and Participants
2.2. Participant Characteristics
2.3. Outcomes of Interest
2.3.1. Plantar Pressure
2.3.2. Daily Weight-Bearing Activity
2.3.3. Adherence to Using an Offloading Device
2.3.4. Plantar Shear Stress
2.4. Cumulative Plantar Tissue Stress Model
2.5. Primary Outcomes
2.6. Feasibility Outcomes
2.7. Sample Size Calculations
2.8. Statistical Analysis
3. Results
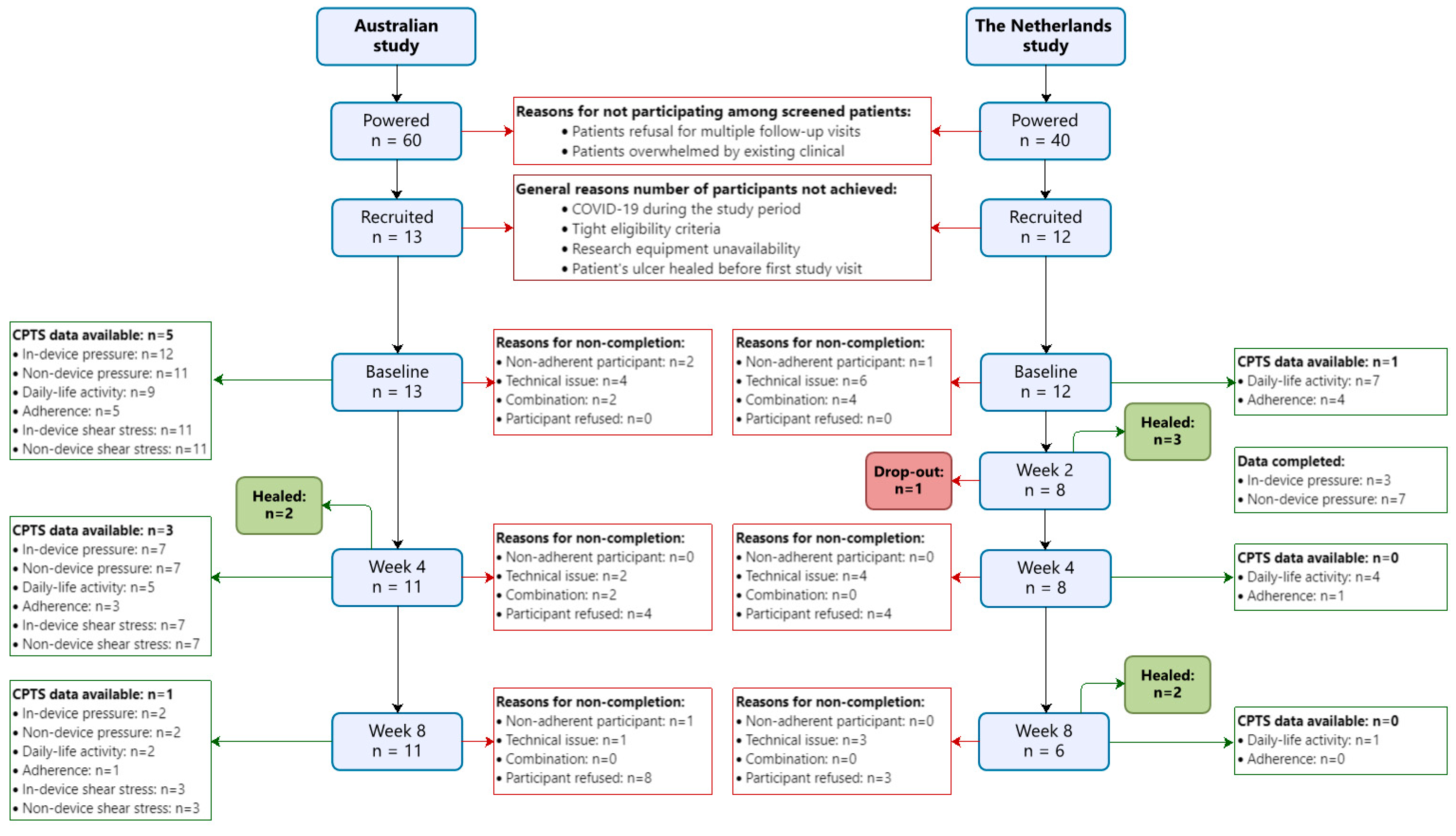
3.1. Participant Recruitment
3.2. Participant Characteristics and Primary Outcomes

3.3. Outcomes of Interest
3.4. Feasibility Outcomes

{kind=link}
| Participants | Australian Study (n = 13) | Healed Ulcer (n = 7) | Non-healed Ulcer (n = 6) | Effect Size | Netherlands Study (n = 12) | Healed Ulcer (n = 5) a | Non-healed Ulcer (n = 6) a | Effect Size |
|---|---|---|---|---|---|---|---|---|
| CPTS (MPa·s/day) | ||||||||
| -Model | 369.0 [95.8; 514.1] (n = 5) | 369.0 [112.2; 373.2] (n = 3) | 525.6 [118.8; 932.4] (n = 2) | 0.26 | 8.7 (n = 1) | NA | 8.7 (n = 1) | NA |
| -Model weighted for thermal stress response | 457.4 [24.3; 944.2] (n = 5) | 457.4 [117.0; 726.7] (n = 3) | 679.2 [311.8; 1327.2] (n = 2) | 0.26 | NA | NA | NA | NA |
| In-shoe plantar pressure | ||||||||
| -PTI in device (kPa·s) | 66.2 [60.0; 74.7] (n = 12) | 74.7 [66.2; 85.9] (n = 6) | 60.4 [59.6; 66.2] | 0.51 | 64.7 [48.5, 111.0] (n = 3) | NA | 64.7 [48.5; 111.0] (n = 3) | NA |
| -PPP in device (kPa) | 140.6 [110.9; 302.7] (n = 12) | 160.8 [105.4; 287.1] (n = 6) | 140.6 [124.1; 351.3] | 0.19 | 119.4 [81.8, 179.8] (n = 3) | NA | 119.4 [81.8; 180.0-] (n = 3) | NA |
| -PTI in footwear (kPa·s) | 72.2 [67.2; 86.3] (n = 11) | 87.4 [78.9; 91.6] (n = 5) | 70.4 [50.5; 72.2] | 0.61 | NA | NA | NA | NA |
| -PPP in footwear (kPa) | 178.7 [141.4; 236.4] (n = 11) | 172.4 [134.4; 233.6] (n = 5) | 189.4 [152.4; 243.8] | 0.22 | NA | NA | NA | NA |
| Barefoot plantar pressure | ||||||||
| -PTI barefoot (kPa·s) | NA | NA | NA | NA | 495.2 [235.7; 626.1] (n = 7) | 620.1 [327.4; 1062.6] (n = 4) | 325.4 [235.7; 452.8] (n = 3) | 0.40 |
| -PPP barefoot (kPa) | NA | NA | NA | NA | 646.3 [446.0; 923.8] (n = 7) | 836.3 [409.4; 1062.6] (n = 4) | 625.0 [446.0; 641.0] (n = 3) | 0.40 |
| Weight-bearing activity (per day) | ||||||||
| -Number of steps | 7444 [1015; 12,456] (n = 9) | 7444 [988; 10,636] (n = 5) | 7854 [2197; 25,215] (n = 4) | 0.16 | 2146 [1400; 4232] (n = 7) | 3075 [1600; 5880] (n = 4) | 2146 [566; 3732] (n = 3) | 0.13 |
| Adherence to using device (%) | ||||||||
| -Strides in device | 50.9 [26.6; 68.7] (n = 5) | 50.9 [37.5; 74.9] (n = 3) | 35.7 [7.5; 63.9] (n = 2) | 0.26 | 48.1 [16.8; 85.5] (n = 4) | 54.2 [15.9; 92.4] (n = 2) | 48.1 [17.7, 78.5] (n = 2) | 0.00 |
| Thermal stress response | ||||||||
| -In-device | 0.66 [0.30; 1.07] (n = 11) | 1.35 [−0.19; 3.37] (n = 6) | 0.42 [0.14; 0.71] (n = 5) | 0.17 | NA | NA | NA | NA |
| -Non-device | 1.45 [−0.15; 2.54] (n = 11) | 0.98 [0.66; 1.28] (n = 6) | 1.45 [−0.22; 1.84] (n = 5) | 0.44 | NA | NA | NA | NA |
4. Discussion
4.1. The Association between CPTS and Ulcer Healing
4.2. Feasability of Measuring CPTS
4.3. Strengths and Limitations
4.4. Future Directions and Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed. 2021. Available online: https://www.diabetesatlas.org (accessed on 1 December 2023).
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lazzarini, P.A.; McPhail, S.M.; van Netten, J.J.; Armstrong, D.G.; Pacella, R.E. Global disability burdens of diabetes-related lower-extremity complications in 1990 and 2016. Diabetes Care 2020, 43, 964–974. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, P.A.; Raspovic, K.M.; Meloni, M.; van Netten, J.J. A new declaration for feet’s sake: Halving the global diabetic foot disease burden from 2% to 1% with next generation care. Diabetes Metab. Res. Rev. 2023, 40, e3747. [Google Scholar] [CrossRef] [PubMed]
- Schaper, N.C.; Van Netten, J.J.; Apelqvist, J.; Bus, S.A.; Fitridge, R.; Game, F.; Monteiro-Soares, M.; Senneville, E.; on behalf of the, I.E. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab. Res. Rev. 2023, 40, e3657. [Google Scholar] [CrossRef] [PubMed]
- Vileikyte, L.; Crews, R.T.; Reeves, N.D. Psychological and Biomechanical Aspects of Patient Adaptation to Diabetic Neuropathy and Foot Ulceration. Curr. Diab. Rep. 2017, 17, 109. [Google Scholar] [CrossRef] [PubMed]
- Boulton, A.J.M.; Vileikyte, L.; Ragnarson-Tennvall, G.; Apelqvist, J. The global burden of diabetic foot disease. Lancet 2005, 366, 1719–1724. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, P.A.; Crews, R.T.; van Netten, J.J.; Bus, S.A.; Fernando, M.E.; Chadwick, P.J.; Najafi, B. Measuring Plantar Tissue Stress in People With Diabetic Peripheral Neuropathy: A Critical Concept in Diabetic Foot Management. J. Diabetes Sci. Technol. 2019, 13, 869–880. [Google Scholar] [CrossRef] [PubMed]
- McDermott, K.; Fang, M.; Boulton, A.J.M.; Selvin, E.; Hicks, C.W. Etiology, Epidemiology, and Disparities in the Burden of Diabetic Foot Ulcers. Diabetes Care 2023, 46, 209–211. [Google Scholar] [CrossRef] [PubMed]
- Monteiro-Soares, M.; Boyko, E.J.; Ribeiro, J.; Ribeiro, I.; Dinis-Ribeiro, M. Predictive factors for diabetic foot ulceration: A systematic review. Diabetes Metab. Res. Rev. 2012, 28, 574–600. [Google Scholar] [CrossRef] [PubMed]
- Crews, R.T.; King, A.L.; Yalla, S.V.; Rosenblatt, N.J. Recent advances and future opportunities to address challenges in offloading diabetic feet: A mini-review. Gerontology 2018, 64, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.C.; Crews, R.T.; Armstrong, D.G. The pivotal role of offloading in the management of neuropathic foot ulceration. Curr. Diab. Rep. 2005, 5, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, P.A.; Armstrong, D.G.; Crews, R.T.; Gooday, C.; Jarl, G.; Kirketerp-Moller, K.; Viswanathan, V.; Bus, S.A. Effectiveness of offloading interventions for people with diabetes-related foot ulcers: A systematic review and meta-analysis. Diabetes Metab. Res. Rev. 2023, 40, e3650. [Google Scholar] [CrossRef] [PubMed]
- Raspovic, A.; Landorf, K.B. A survey of offloading practices for diabetes-related plantar neuropathic foot ulcers. J. Foot Ankle Res. 2014, 7, 35. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.C.; Jensen, J.L.; Weber, A.K.; Robinson, D.E.; Armstrong, D.G. Use of pressure offloading devices in diabetic foot ulcers do we practice what we preach? Diabetes Care 2008, 31, 2118–2119. [Google Scholar] [CrossRef] [PubMed]
- Maluf, K.S.; Mueller, M.J. Comparison of physical activity and cumulative plantar tissue stress among subjects with and without diabetes mellitus and a history of recurrent plantar ulcers. Clin. Biomech. 2003, 18, 567–575. [Google Scholar] [CrossRef] [PubMed]
- van Netten, J.J.; van Baal, J.G.; Bril, A.; Wissink, M.; Bus, S.A. An exploratory study on differences in cumulative plantar tissue stress between healing and non-healing plantar neuropathic diabetic foot ulcers. Clin. Biomech. 2018, 53, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Bus, S.A.; Armstrong, D.G.; Crews, R.T.; Gooday, C.; Jarl, G.; Kirketerp-Moller, K.; Viswanathan, V.; Lazzarini, P.A. Guidelines on offloading foot ulcers in persons with diabetes (IWGDF 2023 update). Diabetes Metab. Res. Rev. 2023, 36, e3274. [Google Scholar] [CrossRef] [PubMed]
- van Netten, J.J.; Bus, S.A.; Apelqvist, J.; Chen, P.; Chuter, V.; Fitridge, R.; Game, F.; Hinchliffe, R.J.; Lazzarini, P.A.; Mills, J.; et al. Definitions and criteria for diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab. Res. Rev. 2023, 40, e3654. [Google Scholar] [CrossRef] [PubMed]
- Jeffcoate, W.J.; Bus, S.A.; Game, F.L.; Hinchliffe, R.J.; Price, P.E.; Schaper, N.C. Reporting standards of studies and papers on the prevention and management of foot ulcers in diabetes: Required details and markers of good quality. Lancet Diabetes Endocrinol. 2016, 4, 781–788. [Google Scholar] [CrossRef]
- Mills, J.L.; Conte, M.S.; Armstrong, D.G.; Pomposelli, F.B.; Schanzer, A.; Sidawy, A.N.; Andros, G. The society for vascular surgery lower extremity threatened limb classification system: Risk stratification based on Wound, Ischemia, and foot Infection (WIfI). J. Vasc. Surg. 2014, 59, 220–234. [Google Scholar] [CrossRef] [PubMed]
- Senneville, É.; Albalawi, Z.; van Asten, S.A.; Abbas, Z.G.; Allison, G.; Aragón-Sánchez, J.; Embil, J.M.; Lavery, L.A.; Alhasan, M.; Oz, O.; et al. IWGDF/IDSA guidelines on the diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023). Diabetes Metab. Res. Rev. 2023, 40, e3687. [Google Scholar] [CrossRef] [PubMed]
- Phelan, E.A.; Mahoney, J.E.; Voit, J.C.; Stevens, J.A. Assessment and Fall Risk in Primary Health care. Physiol. Behav. 2015, 99, 281–293. [Google Scholar] [CrossRef]
- Price, C.; Parker, D.; Nester, C. Validity and repeatability of three in-shoe pressure measurement systems. Gait Posture 2016, 46, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Arts, M.L.J.; Bus, S.A. Twelve steps per foot are recommended for valid and reliable in-shoe plantar pressure data in neuropathic diabetic patients wearing custom made footwear. Clin. Biomech. 2011, 26, 880–884. [Google Scholar] [CrossRef] [PubMed]
- Bus, S.A.; Lange, A. De A comparison of the 1-step, 2-step, and 3-step protocols for obtaining barefoot plantar pressure data in the diabetic neuropathic foot. Clin. Biomech. 2005, 20, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Rabinovich, R.A.; Louvaris, Z.; Raste, Y.; Langer, D.; Van Remoortel, H.; Giavedoni, S.; Burtin, C.; Regueiro, E.M.G.; Vogiatzis, I.; Hopkinson, N.S.; et al. Validity of physical activity monitors during daily life in patients with COPD. Eur. Respir. J. 2013, 42, 1205–1215. [Google Scholar] [CrossRef] [PubMed]
- de Groot, S.; Nieuwenhuizen, M.G. Validity and reliability of measuring activities, movement intensity and energy expenditure with the DynaPort MoveMonitor. Med. Eng. Phys. 2013, 35, 1499–1505. [Google Scholar] [CrossRef] [PubMed]
- Van Schooten, K.S.; Rispens, S.M.; Elders, P.J.M.; Lips, P.; Van Dieën, J.H.; Pijnappels, M. Assessing physical activity in older adults: Required days of trunk accelerometer measurements for reliable estimation. J. Aging Phys. Act. 2015, 23, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.E.; Ainsworth, B.E.; Thompson, R.W.; Bassett, D.R. Sources of variance in daily physical activity levels as measured by an accelerometer. Med. Sci. Sports Exerc. 2002, 34, 1376–1381. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, B.; Kamsma, Y.; Zijlstra, W. Detection of gait and posture using a miniaturised triaxial accelerometer-based system: Accuracy in community-dwelling older adults. Age Ageing 2010, 39, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Lutjeboer, T.; Van Netten, J.J.; Postema, K.; Hijmans, J.M. Validity and feasibility of a temperature sensor for measuring use and non-use of orthopaedic footwear. J. Rehabil. Med. 2018, 50, 920–926. [Google Scholar] [CrossRef]
- Menz, H.B.; Bonanno, D.R. Objective measurement of adherence to wearing foot orthoses using an embedded temperature sensor. Med. Eng. Phys. 2021, 88, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Groningen Algorithm, Version 2. 2021. Available online: https://github.com/CHulshof/Orthotimer_algorithm (accessed on 24 July 2023).
- Jarl, G.; Hulshof, C.M.; Busch-Westbroek, T.E.; Bus, S.A.; van Netten, J.J. Adherence and Wearing Time of Prescribed Footwear among People at Risk of Diabetes-Related Foot Ulcers: Which Measure to Use? Sensors 2023, 23, 1648. [Google Scholar] [CrossRef] [PubMed]
- Wrobel, J.S.; Ammanath, P.; Le, T.; Luring, C.; Wensman, J.; Grewal, G.S.; Najafi, B.; Pop-Busui, R. A novel shear reduction insole effect on the thermal response to walking stress, balance, and gait for diabetic neuropathy. J. Diabetes Sci. Technol. 2014, 8, 1151–1156. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Najafi, B.; Grewal, G.S.; Bharara, M.; Menzies, R.; Talal, T.K.; Armstrong, D.G. Can’t Stand the Pressure: The Association between Unprotected Standing, Walking, and Wound Healing in People with Diabetes. J. Diabetes Sci. Technol. 2017, 11, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Hulshof, C.M.; Van Netten, J.J.; Oosterhof, C.M.; Der, J.V.; Pijnappels, M.; Bus, S.A. New biomechanical models for cumulative plantar tissue stress assessment in people with diabetes at high risk of foot ulceration. J. Biomech. 2024, 163, 111940. [Google Scholar] [CrossRef] [PubMed]
- Perrin, B.M.; van Netten, J.J.; aan de Stegge, W.B.; Busch-Westbroek, T.E.; Bus, S.A. Health-related quality of life and associated factors in people with diabetes at high risk of foot ulceration. J. Foot Ankle Res. 2022, 15, 83. [Google Scholar] [CrossRef] [PubMed]
- Waaijman, R.; De Haart, M.; Arts, M.L.J.; Wever, D.; Verlouw, A.J.W.E.; Nollet, F.; Bus, S.A. Risk factors for plantar foot ulcer recurrence in neuropathic diabetic patients. Diabetes Care 2014, 37, 1697–1705. [Google Scholar] [CrossRef]
- Cortes-Penfield, N.W.; Armstrong, D.G.; Brennan, M.B.; Fayfman, M.; Ryder, J.H.; Tan, T.W.; Schechter, M.C. Evaluation and Management of Diabetes-related Foot Infections. Clin. Infect. Dis. 2023, 77, E1–E13. [Google Scholar] [CrossRef]
- Van Netten, J.J.; Fijen, V.M.; Bus, S.A. Weight-bearing physical activity in people with diabetes-related foot disease: A systematic review. Diabetes Metab. Syndr. Clin. Res. Rev. 2022, 38, e3552. [Google Scholar] [CrossRef] [PubMed]
- Kluding, P.M.; Bareiss, S.K.; Hastings, M.; Marcus, R.L.; Sinacore, D.R.; Mueller, M.J. Physical Training and Activity in People With Diabetic Peripheral Neuropathy: Paradigm Shift. Phys. Ther. 2017, 97, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, P.A.; Jarl, G. Knee-high devices are gold in closing the foot ulcer gap: A review of offloading treatments to heal diabetic foot ulcers. Medicina 2021, 57, 941. [Google Scholar] [CrossRef] [PubMed]
- Samuelson, K.L.; Kiefer, C.T.; Wu, S.C.; Crews, R.T. Changing Perspectives: Offloading a Patient With a Diabetic Foot Ulcer as Opposed to Offloading a Diabetic Foot Ulcer. Foot Ankle Spec. 2020, 14, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Srass, H.; Ead, J.K.; Armstrong, D.G. Adherence and the Diabetic Foot: High Tech Meets High Touch? Sensors 2023, 23, 6898. [Google Scholar] [CrossRef] [PubMed]
- Ruder, K. Diabetic Foot Infections and Amputations Are All Too Common—Here’s What Could Move the Needle. J. Am. Med. Assoc. 2024, 331, 998–1000. [Google Scholar] [CrossRef] [PubMed]
- Bus, S.A.; Reeves, N.D.; Armstrong, D.G.; Najafi, B. Offloading and adherence through technological advancements: Modern approaches for better foot care in diabetes. Diabetes Metab. Res. Rev. 2024, 40, e3769. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Mishra, R.; Vigano, D.; Macagno, M.; Rossotti, S.; D’Huyvetter, K.; Garcia, J.; Armstrong, D.G.; Najafi, B. Smart Offloading Boot System for Remote Patient Monitoring: Toward Adherence Reinforcement and Proper Physical Activity Prescription for Diabetic Foot Ulcer Patients. J. Diabetes Sci. Technol. 2022, 17, 42–51. [Google Scholar] [CrossRef]
| Measurements | 0 Weeks | 2 Weeks | 4 Weeks | 8 Weeks | 12 Weeks |
|---|---|---|---|---|---|
| Plantar pressure | AU | NL | AU | AU | |
| Plantar shear stress | AU | AU | AU | ||
| Daily weight-bearing activity | AU, NL | AU, NL | AU, NL | ||
| Wearing time of offloading device | AU, NL | -------------------------------------------------------------> | |||
| Adherence to offloading device | AU, NL | AU, NL | AU, NL | ||
| Participants | Australian Study (n = 13) | Healed Ulcer at 12 Weeks (n = 7) | Non-Healed Ulcer at 12 Weeks (n = 6) | Netherlands Study (n = 12) | Healed Ulcer at 12 Weeks (n = 5) a | Non-Healed Ulcer at 12 Weeks (n = 6) a |
|---|---|---|---|---|---|---|
| Age (years) | 60.0 [49.0; 72.5] | 64.0 [52.0; 75.0] | 54.0 [45.3; 66.5] | 66.0 [61.3.; 75.0] | 67.0 [61.5; 71.5] | 63.5 [60.5; 75.5] |
| Sex (% (n)) | * | * | ||||
| -Female | 31 (4) | 57 (4) | 0 (0) | 17 (2) | 0 (0) | 17 (1) |
| -Male | 69 (9) | 43 (3) | 100 (6) | 83 (10) | 100 (5) | 83 (5) |
| Body mass index (kg/m2) | 28.4 [26.2; 31.9] | 27.5 [26.0; 30.3] | 30.8 [27.8; 41.3] | 34.0 [26.5; 36.2] | 34.6 [34.0; 37.1] | 29.9 [26.0; 37.7] |
| Diabetes type (% (n)) | ||||||
| -Type 1 | 0 (0) | 0 (0) | 0 (0) | 17 (2) | 0 (0) | 33 (2) |
| -Type 2 | 100 (13) | 100 (7) | 100 (6) | 83 (10) | 100 (5) | 67 (4) |
| Diabetes duration (years) | 15.0 [7.0; 20.0] (n = 11) | 17.0 [10.0; 21.8] (n = 6) | 7.0 [7.0; 20.0] (n = 5) | 15.5 [8.0; 29.0] | 8.0 [5.3; 11.5] ** | 26.0 [19.0; 41.0] ** |
| HbA1c (mmol/mol) | 7.4 [6.3; 9.0] (n = 9) | 7.5 [6.5; 8.7] (n = 4) | 7.4 [6.1; 9.4] (n = 5) | 7.3 [6.7; 8.5] (n = 10) | 7.3 [6.6; 7.9] | 8.3 [7.2; 10.4] (n = 4) |
| Ulcer history (% (n)) | ||||||
| -Yes | 92 (12) | 86 (6) | 100 (6) | 83 (10) | 80 (4) | 100 (6) |
| -No | 8 (1) | 14 (1) | 0 (0) | 17 (2) | 20 (1) | 0 (0) |
| Amputation history (% (n)) | *** | *** | ||||
| -Yes | 46 (6) | 29 (2) | 67 (4) | 50 (6) | 0 (0) | 100 (6) |
| -No | 54 (7) | 71 (5) | 33 (2) | 50 (6) | 100 (5) | 0 (0) |
| Peripheral artery disease (% (n)) | (n = 11) | (n = 5) | ||||
| -Yes | 8 (1) | 14 (1) | 0 (0) | 18 (2) | 0 (0) | 40 (2) |
| -No | 92 (12) | 86 (6) | 100 (6) | 82 (9) | 100 (5) | 60 (3) |
| Nephropathy (% (n)) | (n = 11) | (n = 5) | ||||
| -Yes | 15 (2) | 14 (1) | 17 (1) | 18 (2) | 20 (1) | 20 (1) |
| -No | 85 (11) | 86 (6) | 83 (5) | 82 (9) | 80 (4) | 80 (4) |
| Retinopathy (% (n)) | ** | ** (n = 10) | (n = 4) | (n = 5) | ||
| -Yes | 15 (2) | 29 (2) | 0 (0) | 70 (7) | 100 (4) | 60 (3) |
| -No | 85 (11) | 71 (5) | 100 (6) | 30 (3) | 0 (0) | 40 (2) |
| Ulcer duration before study (weeks) | 6.0 [3.0; 24.0] (n = 12) | 6.5 [1.8; 72.0] (n = 6) | 6.0 [3.8; 29.0] | 2.5 [2.0; 5.8] | 2.0 [1.0; 12.5] | 2.5 [1.5; 4.3] |
| Ulcer site (% (n)) | ||||||
| -Hallux | 23 (3) | 14 (1) | 33 (2) | 33 (4) | 80 (4) | 17 (1) |
| -Forefoot | 62 (8) | 71 (5) | 50 (3) | 50 (6) | 20 (1) | 50 (3) |
| -Midfoot | 0 (0) | 0 (0) | 0 (0) | 17 (2) | 0 (0) | 33 (2) |
| -Rearfoot | 15 (2) | 14 (1) | 17 (1) | 0 (0) | 0 (0) | 0 (0) |
| Ulcer size (mm2) | 12.0 [5.5; 77.0] | 9.0 [4.0; 20.0] | 23.0 [7.0; 62.0] | 20.5 [4.9; 177.5] | 16.0 [4.1; 37.5] | 134.0 [5.9; 550.0] |
| Ulcer depth (mm) | 1.0 [1.0; 2.5] | 1.0 [1.0; 3.0] | 1.0 [1.0; 2.0] | 1.0 [1.0; 2.0] (n = 9) | 1.0 [1.0; 1.8] (n = 4) | 2.0 [1.3; 2.0] (n = 4) |
| Texas classification (% (n)) | (n = 11) | (n = 5) | ||||
| -Superficial (1) | 100 (13) | 100 (7) | 100 (6) | 82 (9) | 92 (11) | 80 (4) |
| -Penetrate to tendon or capsule (2) | 0 (0) | 0 (0) | 0 (0) | 18 (2) | 8 (1) | 20 (1) |
| -Penetrate to bone (3) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Mild infection (% (n)) | (n = 11) | (n = 5) | ||||
| -Yes | 0 (0) | 0 (0) | 0 (0) | 18 (2) | 20 (1) | 20 (1) |
| -No | 100 (13) | 100 (7) | 100 (6) | 82 (9) | 80 (4) | 80 (4) |
| Ischemia (% (n)) | (n = 11) | (n = 5) | ||||
| -Yes | 8 (1) | 14 (1) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| -No | 92 (12) | 86 (6) | 100 (6) | 100 (11) | 100 (5) | 100 (5) |
| Offloading device used (% (n)) | ||||||
| -Removable knee-high | 15 (2) | 29 (2) | 0 (0) | 8 (1) | 0 (0) | 17 (1) |
| -Removable ankle-high | 23 (3) | 14 (1) | 33 (2) | 17 (2) | 20 (1) | 17 (1) |
| -Custom-made insoles or footwear | 62 (8) | 57 (4) | 67 (4) | 75 (9) | 80 (4) | 67 (4) |
| Participants | CPTS Available (n = 5) | CPTS Not Available (n = 8) | p-Value |
|---|---|---|---|
| Age (years) | 56.0 [47.5; 75.5] | 61.5 [47.5; 68.5] | 1.000 |
| Sex (% (n)) | 0.569 | ||
| -Female | 40 (2) | 25 (2) | |
| -Male | 60 (3) | 75 (6) | |
| BMI (kg/m2) | 26.2 [23.3; 27.4] | 30.9 [28.6; 36.7] | 0.006 ** |
| Diabetes type (% (n)) | NA | ||
| -Type 1 | 0 (0) | 0 (0) | |
| -Type 2 | 100 (5) | 100 (8) | |
| Diabetes duration (years) | 17.5 [9.0; 25.3] (n = 4) | 13.0 [7.0; 19.0] (n = 7) | 0.315 |
| HbA1c (mmol/mol) | 6.6 [6.1; 8.4] (n = 4) | 7.9 [6.9; 9.4] (n = 5) | 0.190 |
| Ulcer history (% (n)) | 0.188 | ||
| -Yes | 80 (4) | 100 (8) | |
| -No | 20 (1) | 0 (0) | |
| Amputation history (% (n)) | 0.135 | ||
| -Yes | 20 (1) | 63 (5) | |
| -No | 80 (4) | 38 (3) | |
| Peripheral artery disease (% (n)) | 0.188 | ||
| -Yes | 20 (1) | 0 (0) | |
| -No | 80 (4) | 100 (8) | |
| Nephropathy (% (n)) | 0.052 | ||
| -Yes | 40 (2) | 0 (0) | |
| -No | 60 (3) | 100 (8) | |
| Retinopathy (% (n)) | 0.052 | ||
| -Yes | 40 (2) | 0 (0) | |
| -No | 60 (3) | 100 (8) | |
| Ulcer duration before study (weeks) | 24.0 [5.5; 185.0] (n = 4) | 3.5 [2.3; 15.5] | 0.073 |
| Ulcer site (% (n)) | 0.231 | ||
| -Hallux | 0 (0) | 38 (3) | |
| -Forefoot | 80 (4) | 50 (4) | |
| -Midfoot | 0 (0) | 0 (0) | |
| -Rearfoot | 20 (1) | 13 (1) | |
| Ulcer size (mm2) | 7.0 [3.0; 20.0] | 19.0 [8.3; 148.5] | 0.127 |
| Ulcer depth (mm) | 2.0 [1.0; 5.0] | 1.0 [1.0; 1.0] | 0.171 |
| Texas classification (% (n)) | NA | ||
| -Superficial (1) | 100 (5) | 100 (8) | |
| -Penetrate to tendon or capsule (2) | 0 (0) | 0 (0) | |
| -Penetrate to bone (3) | 0 (0) | 0 (0) | |
| Infection (% (n)) | NA | ||
| -Yes | 0 (0) | 0 (0) | |
| -No | 100 (5) | 100 (8) | |
| Ischemia (% (n)) | 0.188 | ||
| -Yes | 20 (1) | 0 (0) | |
| -No | 80 (4) | 100 (8) | |
| Offloading device used (% (n)) | 0.296 | ||
| -Removable knee-high | 20 (1) | 13 (1) | |
| -Removable ankle-high | 0 (0) | 38 (3) | |
| -Custom-made insoles or footwear | 80 (4) | 50 (4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hulshof, C.M.; Page, M.; van Baal, S.G.; Bus, S.A.; Fernando, M.E.; van Gemert-Pijnen, L.; Kappert, K.D.R.; Lucadou-Wells, S.; Najafi, B.; van Netten, J.J.; et al. The Stress of Measuring Plantar Tissue Stress in People with Diabetes-Related Foot Ulcers: Biomechanical and Feasibility Findings from Two Prospective Cohort Studies. Sensors 2024, 24, 2411. https://doi.org/10.3390/s24082411
Hulshof CM, Page M, van Baal SG, Bus SA, Fernando ME, van Gemert-Pijnen L, Kappert KDR, Lucadou-Wells S, Najafi B, van Netten JJ, et al. The Stress of Measuring Plantar Tissue Stress in People with Diabetes-Related Foot Ulcers: Biomechanical and Feasibility Findings from Two Prospective Cohort Studies. Sensors. 2024; 24(8):2411. https://doi.org/10.3390/s24082411
Chicago/Turabian StyleHulshof, Chantal M., Madelyn Page, Sjef G. van Baal, Sicco A. Bus, Malindu E. Fernando, Lisette van Gemert-Pijnen, Kilian D. R. Kappert, Scott Lucadou-Wells, Bijan Najafi, Jaap J. van Netten, and et al. 2024. "The Stress of Measuring Plantar Tissue Stress in People with Diabetes-Related Foot Ulcers: Biomechanical and Feasibility Findings from Two Prospective Cohort Studies" Sensors 24, no. 8: 2411. https://doi.org/10.3390/s24082411
APA StyleHulshof, C. M., Page, M., van Baal, S. G., Bus, S. A., Fernando, M. E., van Gemert-Pijnen, L., Kappert, K. D. R., Lucadou-Wells, S., Najafi, B., van Netten, J. J., & Lazzarini, P. A. (2024). The Stress of Measuring Plantar Tissue Stress in People with Diabetes-Related Foot Ulcers: Biomechanical and Feasibility Findings from Two Prospective Cohort Studies. Sensors, 24(8), 2411. https://doi.org/10.3390/s24082411