

An Era of Digital Healthcare—A Comprehensive Review of Sensor Technologies and Telehealth Advancements in Chronic Heart Failure Management


Abstract
1. Introduction
- Telephone support systems
- Implants (invasive): Cardiovascular electronic devices (ICDs, CRT-Ds), hemodynamic sensors (filling pressures such as right ventricular pressure, pulmonary artery pressure, left atrial pressure, central venous pressure, interstitial fluid pressure) for remote intra cardiac monitoring.
- Digital platforms (non-invasive): Commercial devices to measure vital signs (blood pressure, daily weight, heart rate, oxygen saturation, ECG) and assessment of HF symptoms (app-based surveys, medication adherence).
- Wearable technologies (non-invasive): smart watches, patches, or textiles to monitor body temperature, blood glucose levels, ECG, and body posture.
2. Sensor-Based HF Monitoring
2.1. Haemodynamic Sensors in Clinical Practice
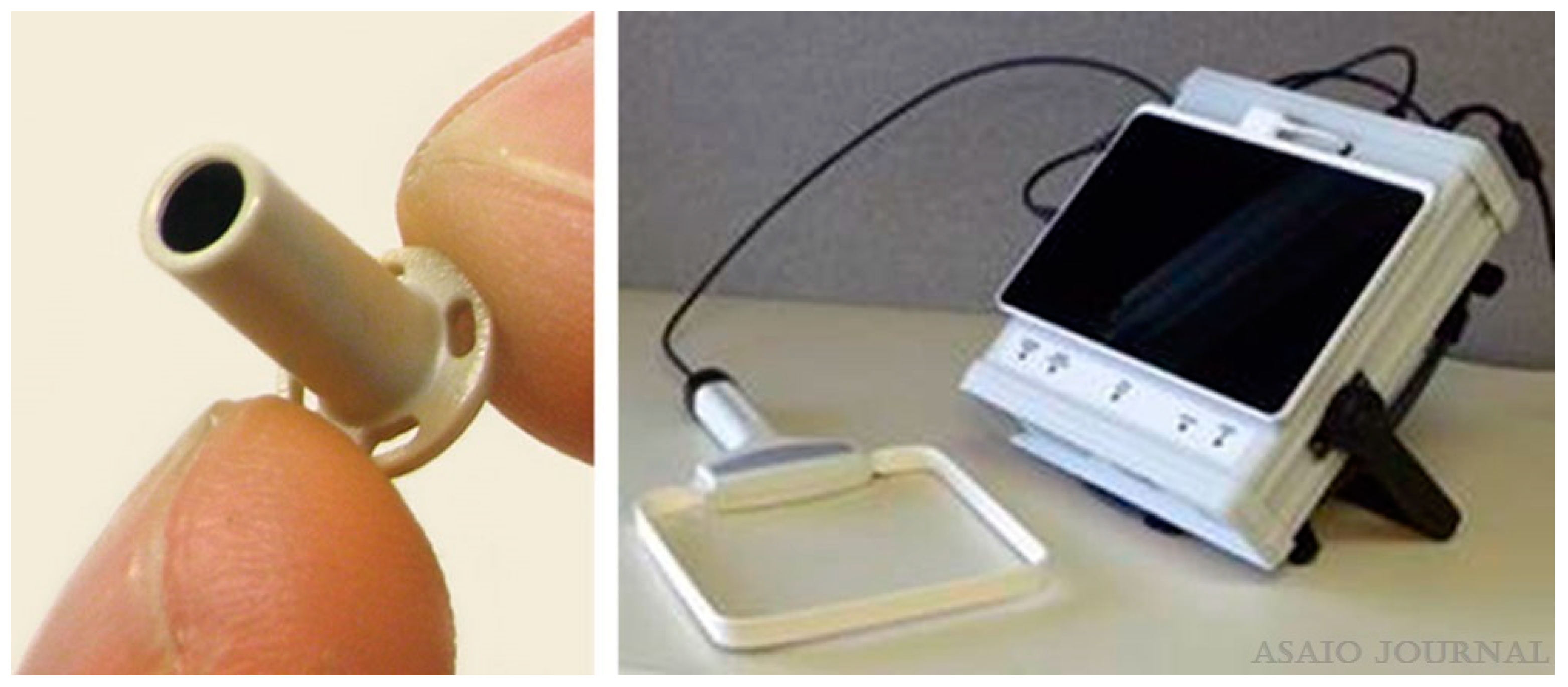
2.1.1. Left-Atrial Pressure (LAP) Monitoring
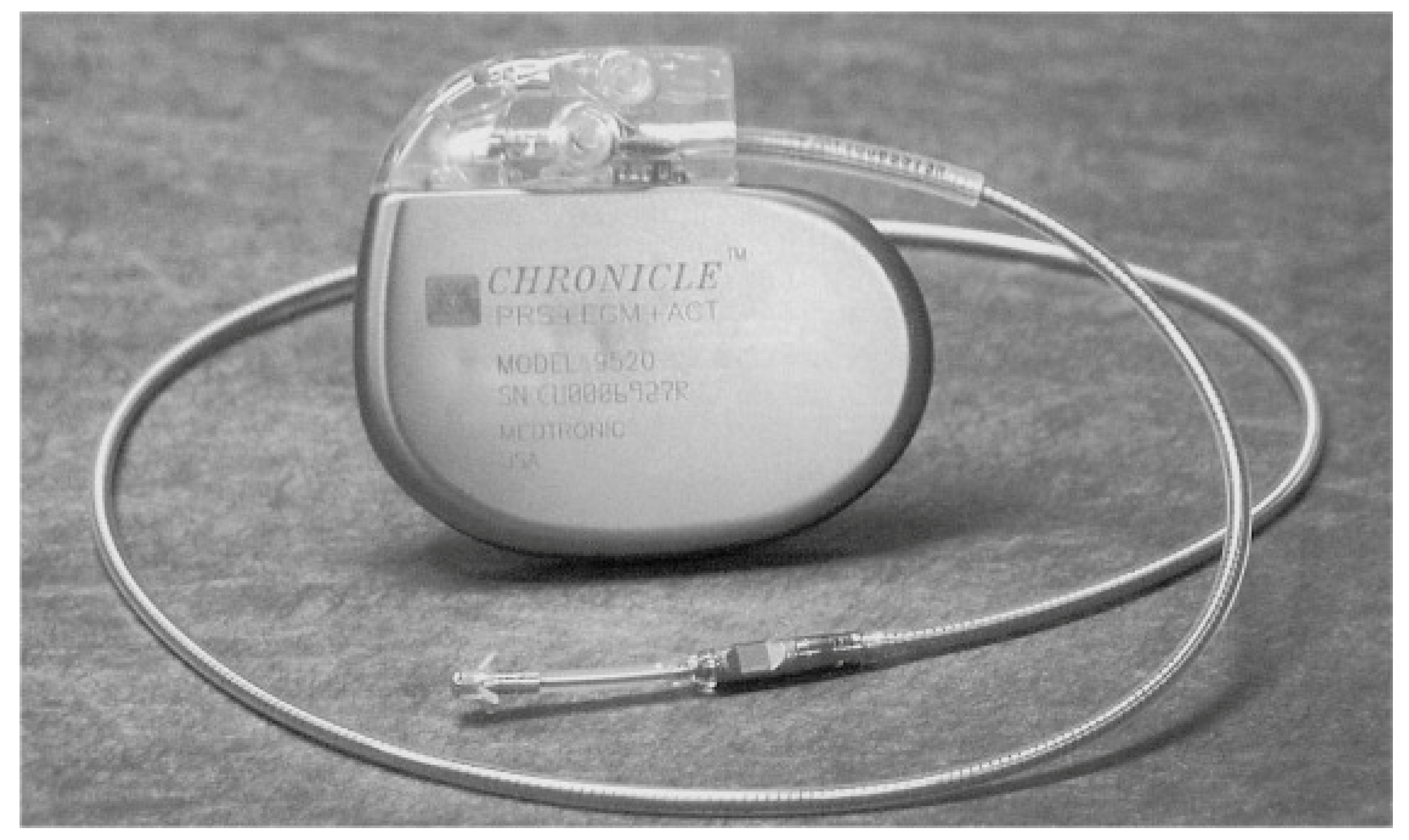
2.1.2. Right-Ventricular Pressure (RVP) Monitoring
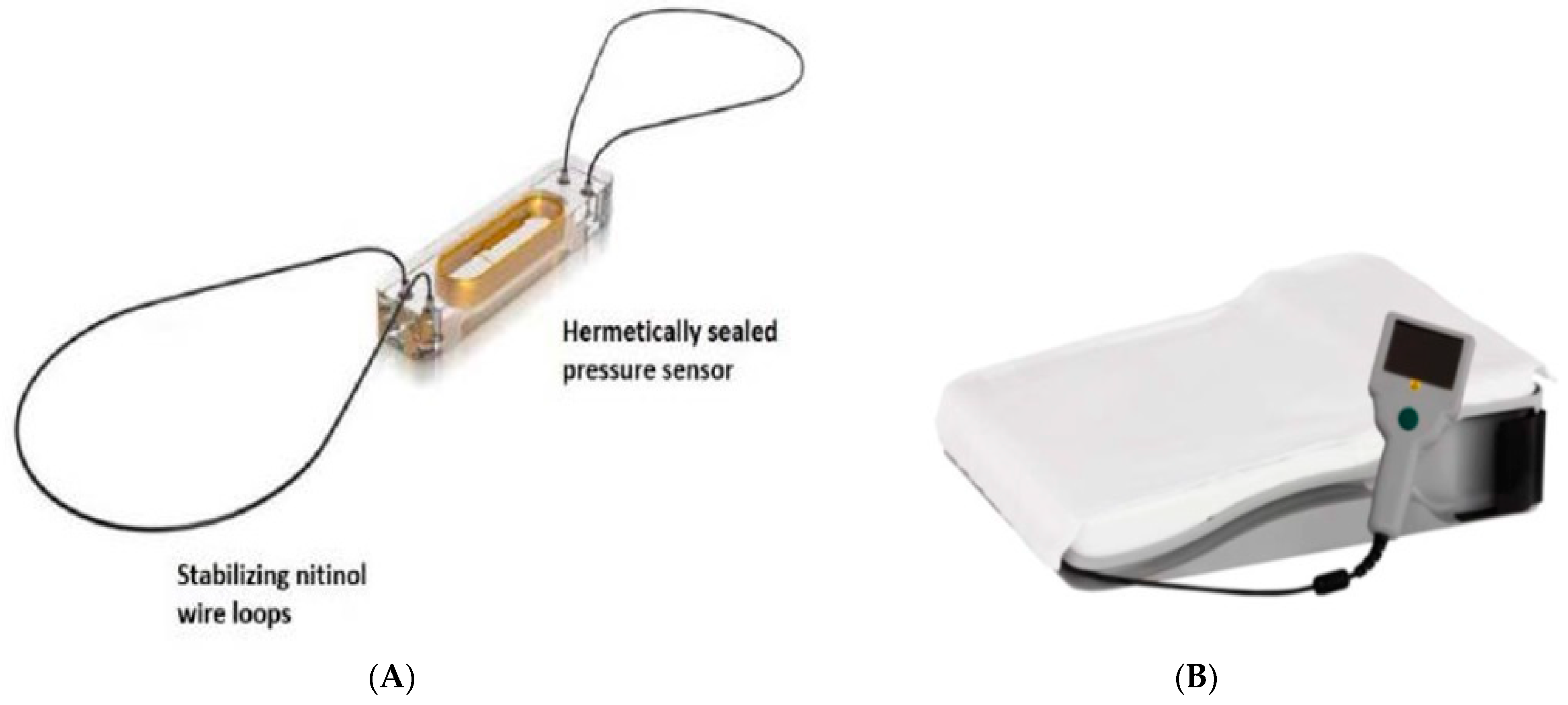
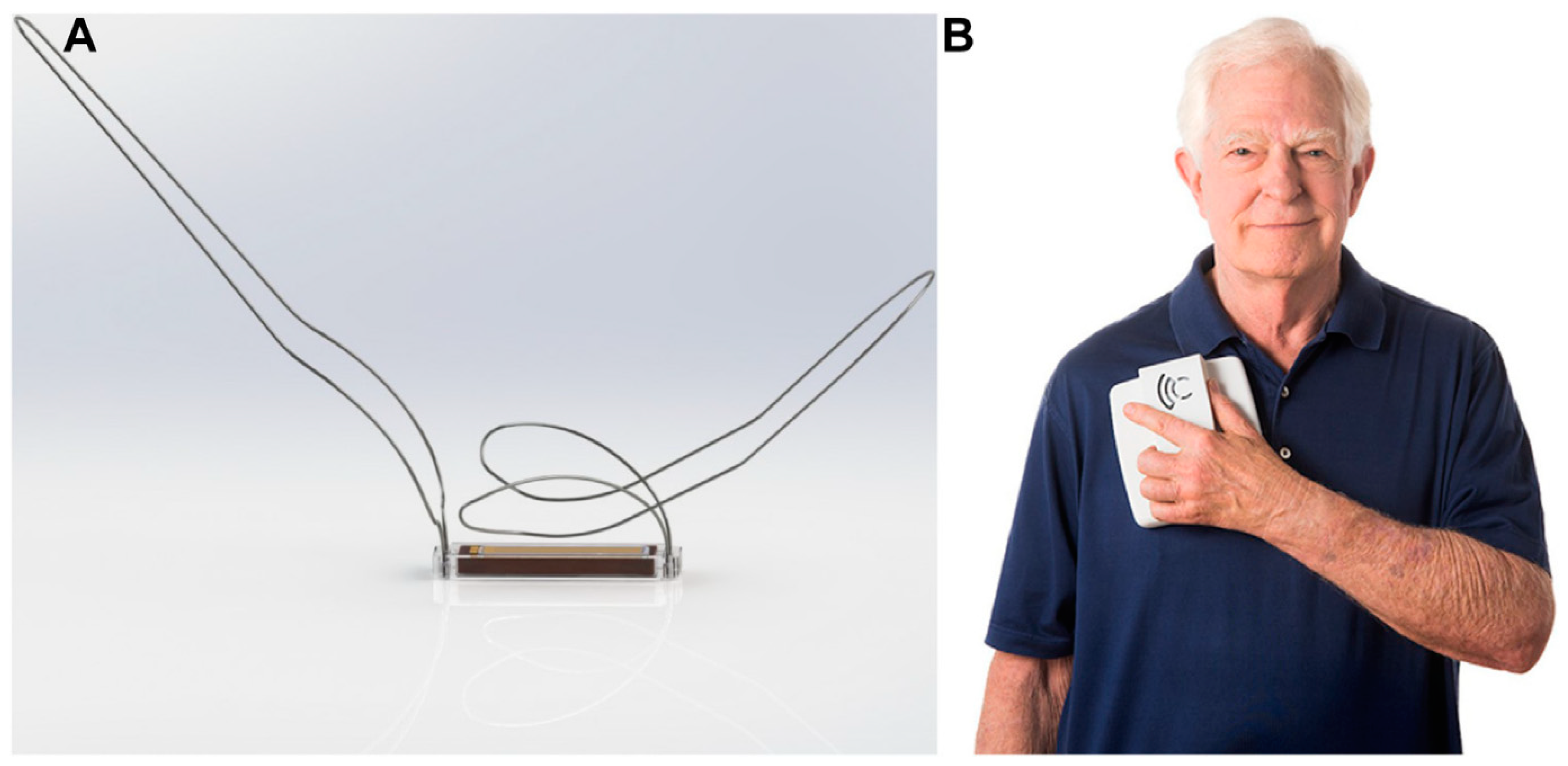
2.1.3. Pulmonary Artery Pressure (PAP) Monitoring
CardioMEMS HF System
Clinical Evidence
Safety & Clinical Efficacy
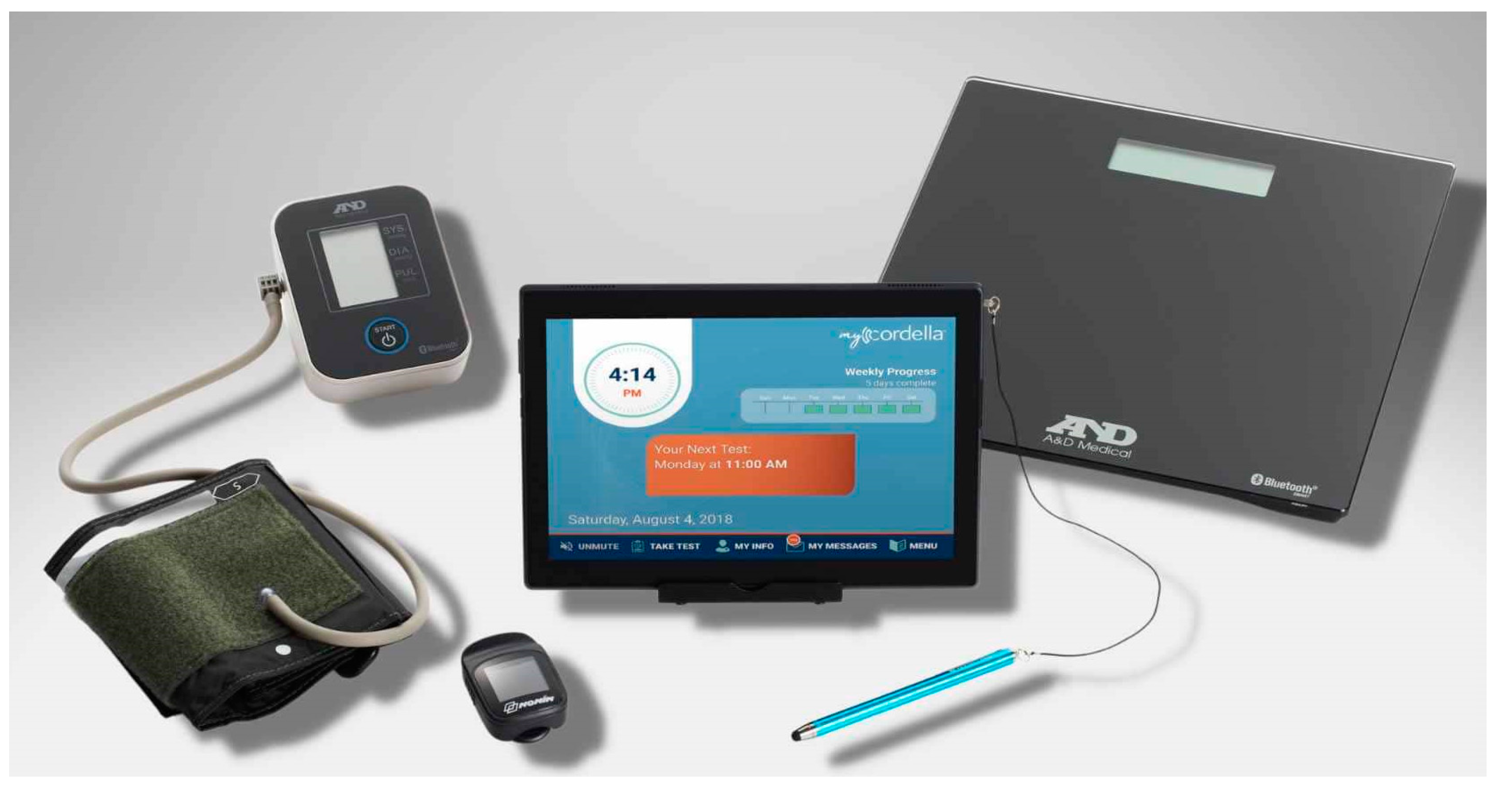
Cordella HF System
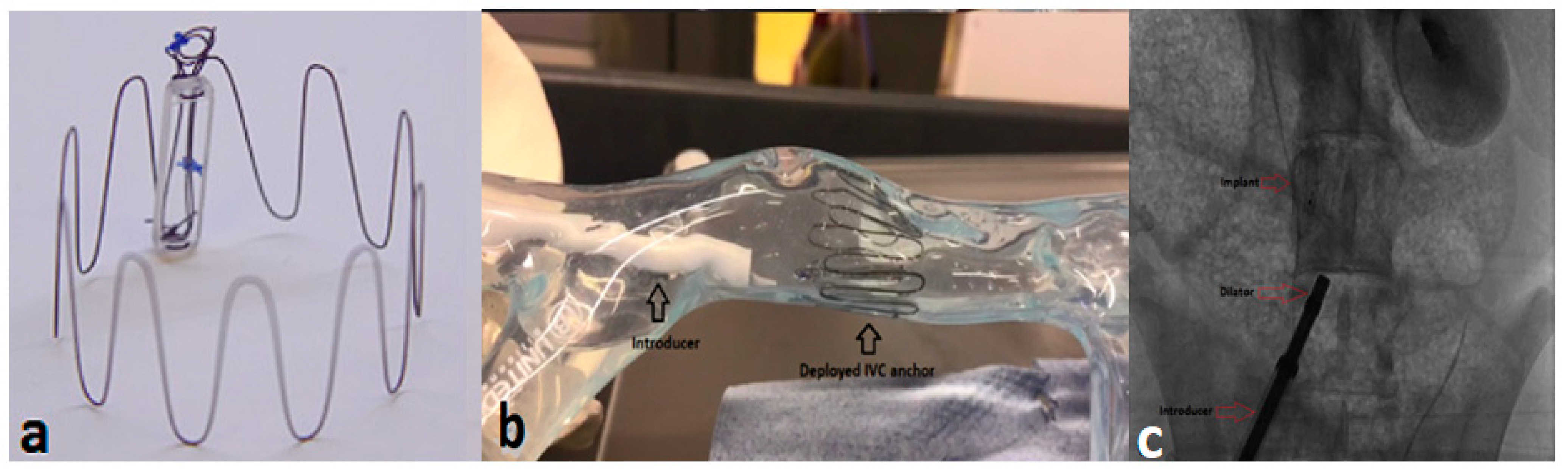
2.1.4. Inferior Vena Cava (IVC) Area Monitoring
Foundry Innovation and Research 1 Ltd. (Fire1) System
2.2. Haemodynamic Sensors in Preclinical Practice
2.2.1. Central Venous Pressure (CVP) Monitoring
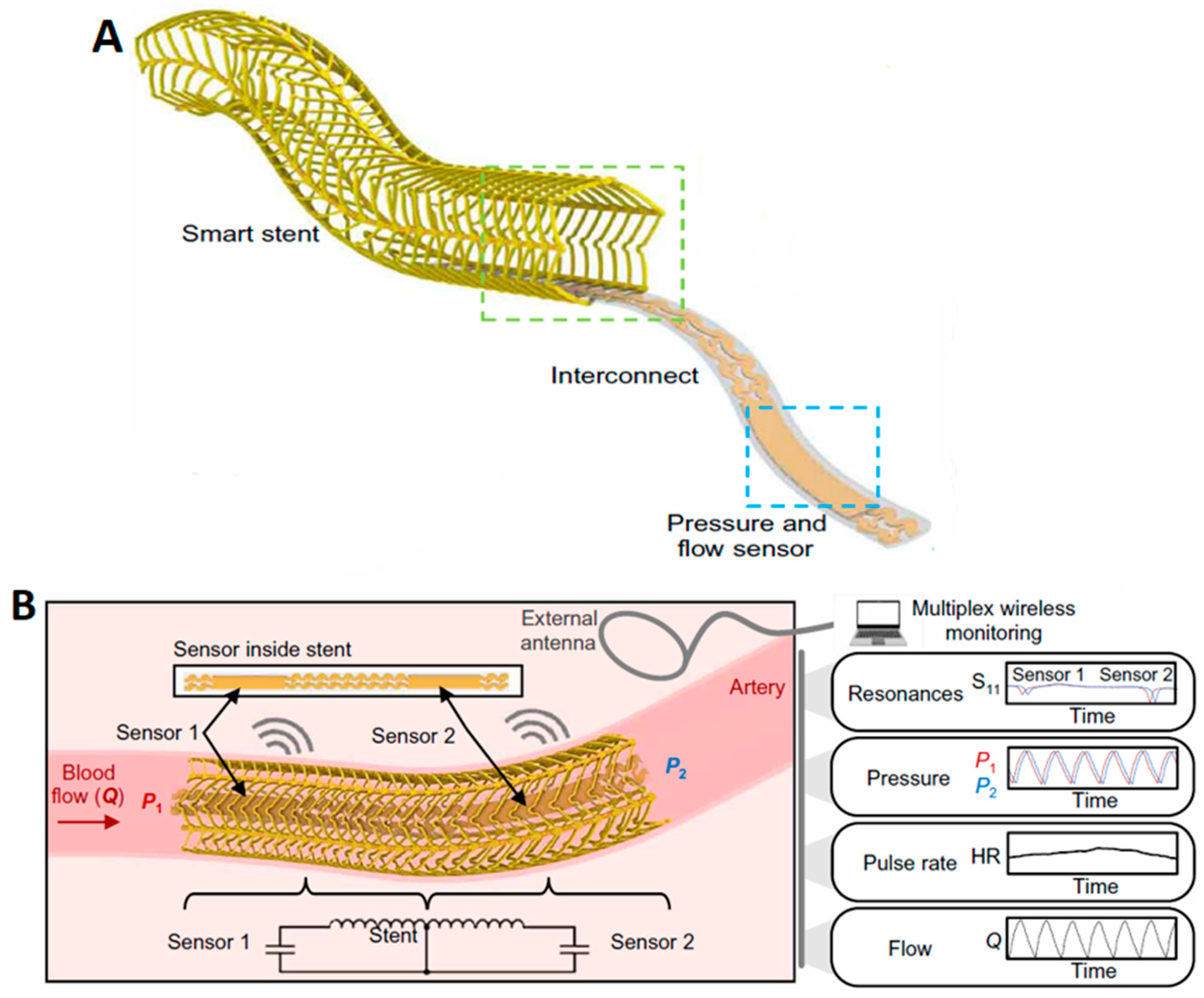
2.2.2. Haemodynamic Sensing via a Vascular Electronic System (Wireless Arterial Stent)
3. Non-Invasive Haemodynamic Monitoring
3.1. Cordella HF System (CHFS)
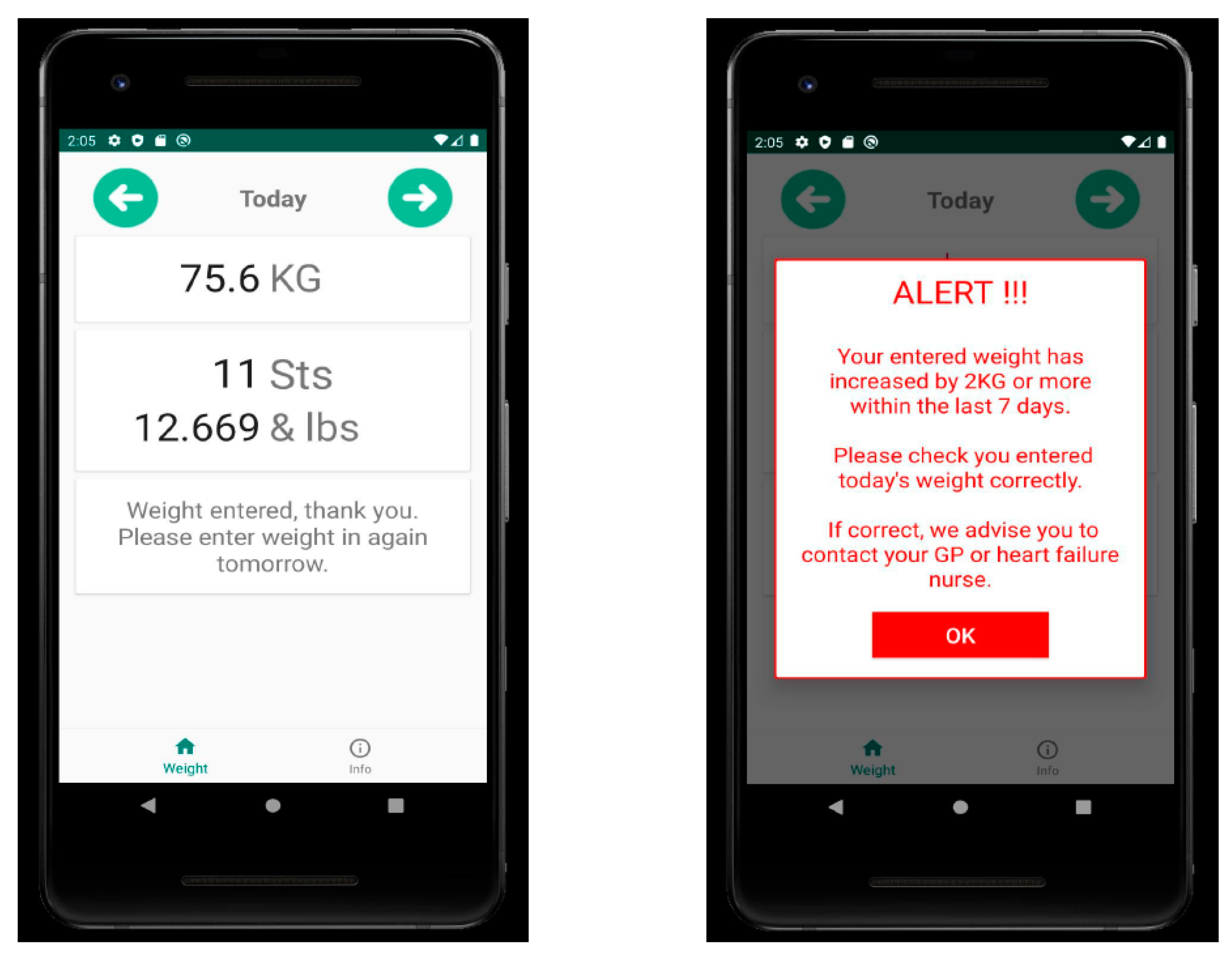
3.2. Fluid Heart Tracker App
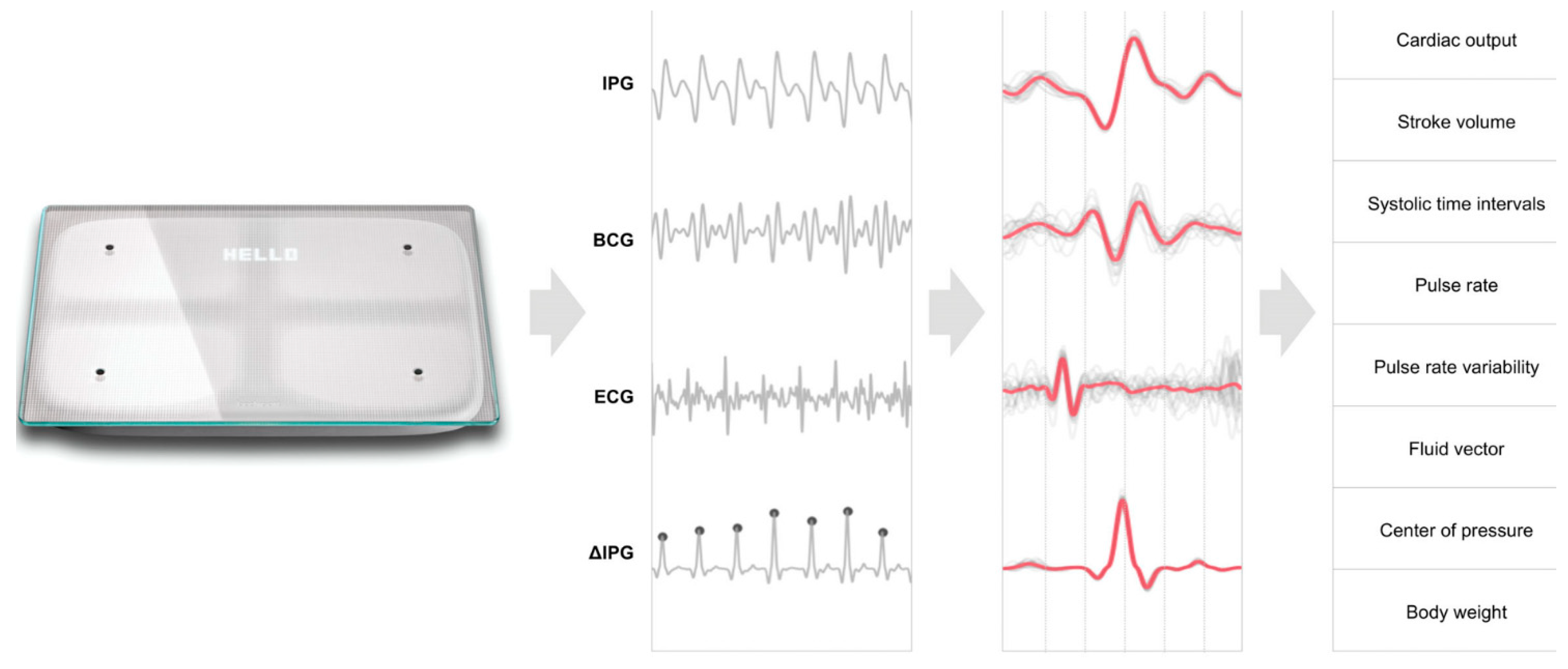
3.3. Scale-HF 1 Study
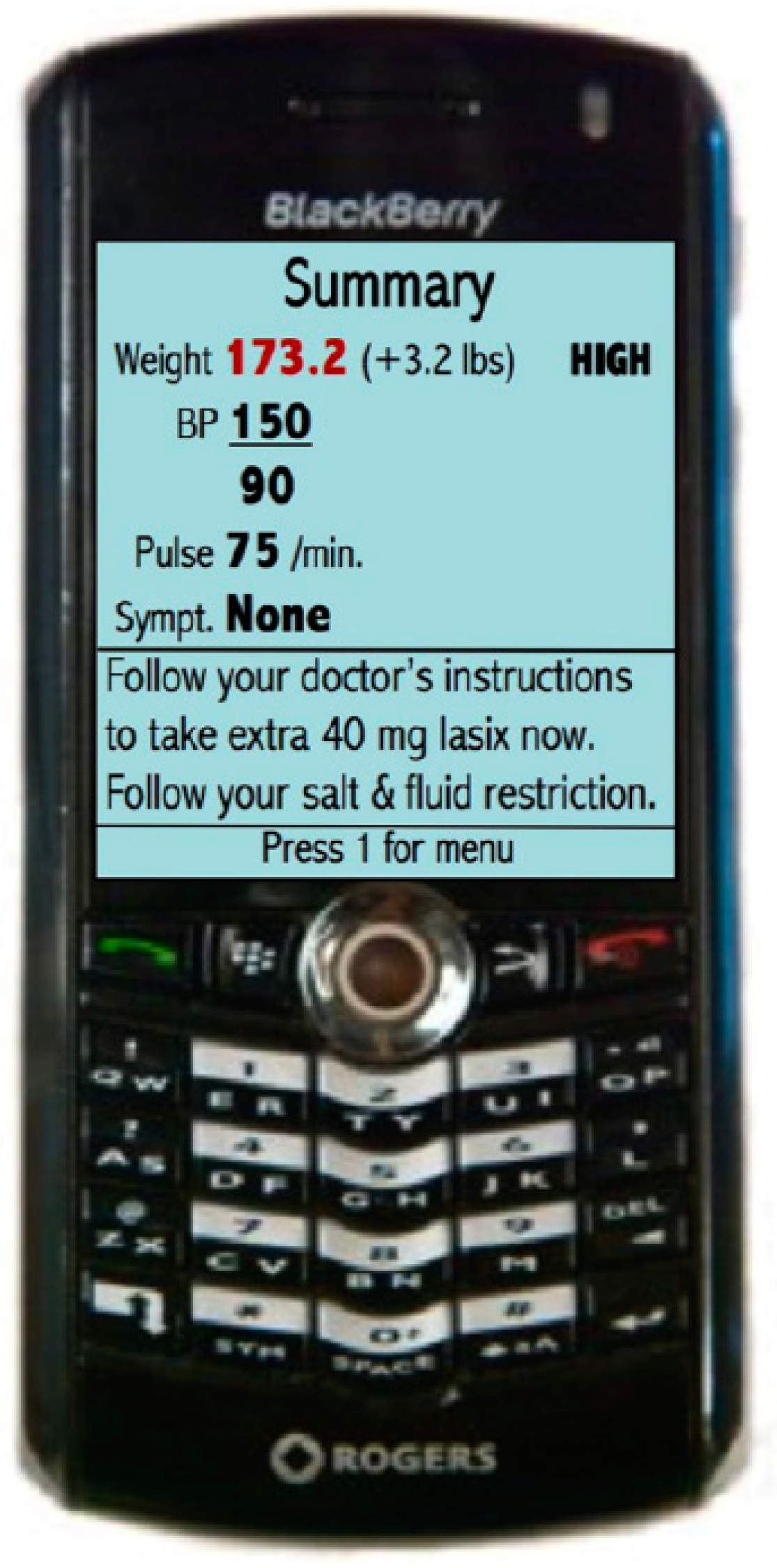
3.4. Mobile Phone-Based Telemonitoring
4. Conclusions and Future Outlook on Remote HF Management
- Digital health offers the potential for more personalized management of HF by enabling continuous monitoring for both patients and physicians.
- Digital solutions, including those leveraging data from implantable devices, will aid in managing HF effectively.
- These tools are intended for patient use and warrant thorough investigation.
- Emerging clinical workflows, such as remote management and decision-making by utilizing data from telehealth platforms, demand further research and development [79].
Author Contributions
Funding
Conflicts of Interest
References
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Rosano, G.M.C.; Coats, A.J.S. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc. Res. 2022, 118, 3272–3287. [Google Scholar] [CrossRef]
- United States Department of Health and Human Services; National Center for Health Statistics. Multiple Cause of Death, 1999; United States Department of Health and Human Services; National Center for Health Statistics: Hyattsville, MD, USA, 2007. [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics—2023 Update: A Report from the American Heart Association. Circulation 2023, 147, e93–e621, Correction in Circulation 2023, 147, e622. [Google Scholar] [CrossRef]
- Jones, N.R.; Roalfe, A.K.; Adoki, I.; Hobbs, F.D.R.; Taylor, C.J. Survival of patients with chronic heart failure in the community: A systematic review and meta-analysis. Eur. J. Heart Fail. 2019, 21, 1306–1325. [Google Scholar] [CrossRef]
- Rossignol, P.; Hernandez, A.F.; Solomon, S.D.; Zannad, F. Heart failure drug treatment. Lancet 2019, 393, 1034–1044. [Google Scholar] [CrossRef]
- Corry, S.E.; McDonald, K.; Kennelly, B. Cost of Illness: Heart Failure in Ireland. Value Health 2014, 17, A484. [Google Scholar] [CrossRef][Green Version]
- Health Service Executive. Chronic Disease Management Programme. 2021. Available online: https://www.hse.ie/eng/about/who/gmscontracts/2019agreement/chronic-disease-management-programme (accessed on 11 December 2023).
- Eisenberg, E.; Di Palo, K.E.; Piña, I.L. Sex differences in heart failure. Clin. Cardiol. 2018, 41, 211–216. [Google Scholar] [CrossRef]
- Bottle, A.; Kim, D.; Hayhoe, B.; Majeed, A.; Aylin, P.; Clegg, A.; Cowie, M.R. Frailty and co-morbidity predict first hospitalisation after heart failure diagnosis in primary care: Population-based observational study in England. Age Ageing 2019, 48, 347–354. [Google Scholar] [CrossRef]
- Lindmark, K.; Boman, K.; Stålhammar, J.; Olofsson, M.; Lahoz, R.; Studer, R.; Proudfoot, C.; Corda, S.; Fonseca, A.F.; Costa-Scharplatz, M.; et al. Recurrent heart failure hospitalizations increase the risk of cardiovascular and all-cause mortality in patients with heart failure in Sweden: A real-world study. ESC Heart Fail. 2021, 8, 2144–2153. [Google Scholar] [CrossRef]
- Bello, N.A.; Claggett, B.; Desai, A.S.; McMurray, J.J.V.; Granger, C.B.; Yusuf, S.; Swedberg, K.; Pfeffer, M.A.; Solomon, S.D. Influence of previous heart failure hospitalization on cardiovascular events in patients with reduced and preserved ejection fraction. Circ. Heart Fail. 2014, 7, 590–595. [Google Scholar] [CrossRef]
- Sueta, C.A.; Rodgers, J.E.; Chang, P.P.; Zhou, L.; Thudium, E.M.; Kucharska-Newton, A.M.; Stearns, S.C. Medication Adherence Based on Part D Claims for Patients with Heart Failure after Hospitalization (from the Atherosclerosis Risk in Communities Study). Am. J. Cardiol. 2015, 116, 413–419. [Google Scholar] [CrossRef]
- Zito, A.; Princi, G.; Romiti, G.F.; Galli, M.; Basili, S.; Liuzzo, G.; Sanna, T.; Restivo, A.; Ciliberti, G.; Trani, C.; et al. Device-based remote monitoring strategies for congestion-guided management of patients with heart failure: A systematic review and meta-analysis. Eur. J. Heart Fail. 2022, 24, 2333–2341. [Google Scholar] [CrossRef] [PubMed]
- Silva, P.; Gomes, P.V.; Condeço, J.M.; Curado, H.; Veloso, R. Telemonitoring in heart failure patient management. In Handbook of Research on Advances in Digital Technologies to Promote Rehabilitation and Community Participation; IGI Global: Pennsylvania, PA, USA, 2023; pp. 228–245. [Google Scholar]
- Ikumapayi, O.; Kayode, J.; Afolalu, A.; Nnochiri, E.; Olowe, K.; Bodunde, O. Telehealth and Telemedicine—An Overview. In Proceedings of the 3rd African International Conference on Industrial Engineering and Operations Management, Nsukka, Nigeria, 5–7 April 2022. [Google Scholar] [CrossRef]
- Allely, E.B. Synchronous and asynchronous telemedicine. J. Med. Syst. 1995, 19, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Koehler, F.; Abraham, W.T. Telemedicine and remote management of patients with heart failure. Lancet 2011, 378, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Brahmbhatt, D.H.; Cowie, M.R. Remote Management of Heart Failure: An Overview of Telemonitoring Technologies. Card. Fail. Rev. 2019, 5, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Dierckx, R.; Pellicori, P.; Cleland, J.G.F.; Clark, A.L. Telemonitoring in heart failure: Big Brother watching over you. Heart Fail. Rev. 2014, 20, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Karamichalakis, N.; Parissis, J.; Bakosis, G.; Bistola, V.; Ikonomidis, I.; Sideris, A.; Filippatos, G. Implantable devices to monitor patients with heart failure. Heart Fail. Rev. 2018, 23, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Bekfani, T.; Fudim, M.; Cleland, J.G.F.; Jorbenadze, A.; von Haehling, S.; Lorber, A.; Rothman, A.M.K.; Stein, K.; Abraham, W.T.; Sievert, H.; et al. A current and future outlook on upcoming technologies in remote monitoring of patients with heart failure. Eur. J. Heart Fail. 2020, 23, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Inglis, S.C.; Clark, R.A.; McAlister, F.A.; Ball, J.; Lewinter, C.; Cullington, D.; Stewart, S.; Cleland, J.G.F. Structured telephone support or telemonitoring programmes for patients with chronic heart failure. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2010. [Google Scholar] [CrossRef]
- Koehler, F.; Koehler, K.; Prescher, S.; Kirwan, B.-A.; Wegscheider, K.; Vettorazzi, E.; Lezius, S.; Winkler, S.; Moeller, V.; Fiss, G.; et al. Mortality and morbidity 1 year after stopping a remote patient management intervention: Extended follow-up results from the telemedical interventional management in patients with heart failure II (TIM-HF2) randomised trial. Lancet Digit. Health 2020, 2, e16–e24. [Google Scholar] [CrossRef] [PubMed]
- Winkler, S.; Koehler, K.; Prescher, S.; Koehler, M.; Kirwan, B.-A.; Tajsic, M.; Koehler, F. Is 24/7 remote patient management in heart failure necessary? Results of the telemedical emergency service used in the TIM-HF and in the TIM-HF2 trials. ESC Heart Fail. 2021, 8, 3613–3620. [Google Scholar] [CrossRef]
- Hindricks, G.; Taborsky, M.; Glikson, M.; Heinrich, U.; Schumacher, B.; Katz, A.; Brachmann, J.; Lewalter, T.; Goette, A.; Block, M.; et al. Implant-based multiparameter telemonitoring of patients with heart failure (IN-TIME): A randomised controlled trial. Lancet 2014, 384, 583–590. [Google Scholar] [CrossRef]
- Boehmer, J.P.; Hariharan, R.; Devecchi, F.G.; Smith, A.L.; Molon, G.; Capucci, A.; An, Q.; Averina, V.; Stolen, C.M.; Thakur, P.H.; et al. A Multisensor Algorithm Predicts Heart Failure Events in Patients with Implanted Devices. JACC Heart Fail. 2017, 5, 216–225. [Google Scholar] [CrossRef]
- Virani, S.A.; Sharma, V.; McCann, M.; Koehler, J.; Tsang, B.; Zieroth, S. Prospective evaluation of integrated device diagnostics for heart failure management: Results of the TRIAGE-HF study. ESC Heart Fail. 2018, 5, 809–817. [Google Scholar] [CrossRef]
- Whellan, D.J.; Ousdigian, K.T.; Al-Khatib, S.M.; Pu, W.; Sarkar, S.; Porter, C.B.; Pavri, B.B.; O’Connor, C.M. Combined Heart Failure Device Diagnostics Identify Patients at Higher Risk of Subsequent Heart Failure Hospitalizations. J. Am. Coll. Cardiol. 2010, 55, 1803–1810. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Follath, F.; Ponikowski, P.; Barsuk, J.H.; Blair, J.E.A.; Cleland, J.G.; Dickstein, K.; Drazner, M.H.; Fonarow, G.C.; Jaarsma, T.; et al. Assessing and grading congestion in acute heart failure: A scientific statement from the Acute Heart Failure Committee of the Heart Failure Association of the European Society of Cardiology and endorsed by the European Society of Intensive Care Medicine. Eur. J. Heart Fail. 2010, 12, 423–433. [Google Scholar] [CrossRef]
- Sarasohn-Kahn, J. How Smartphones are Changing Health Care for Consumers and Providers; California Health Care Foundation: Oakland, CA, USA, 2010. [Google Scholar]
- Merchant, F.M.; Dec, G.W.; Singh, J.P. Implantable sensors for heart failure. Circ. Arrhythm. Electrophysiol. 2010, 3, 657–667. [Google Scholar] [CrossRef]
- Thomas, L.; Abhayaratna, W.P. Left Atrial Reverse Remodeling. JACC Cardiovasc. Imaging 2017, 10, 65–77. [Google Scholar] [CrossRef]
- Abraham, W.T.; Perl, L. Implantable Hemodynamic Monitoring for Heart Failure Patients. J. Am. Coll. Cardiol. 2017, 70, 389–398. [Google Scholar] [CrossRef]
- Abraham, W.T.; Adamson, P.B.; Costanzo, M.R.; Eigler, N.; Gold, M.; Klapholz, M.; Maurer, M.; Saxon, L.; Singh, J.; Troughton, R. Hemodynamic Monitoring in Advanced Heart Failure: Results from the LAPTOP-HF Trial. J. Card. Fail. 2016, 22, 940. [Google Scholar] [CrossRef]
- Ritzema, J.; Melton, I.C.; Richards, A.M.; Crozier, I.G.; Frampton, C.; Doughty, R.N.; Whiting, J.; Kar, S.; Eigler, N.; Krum, H.; et al. Direct Left Atrial Pressure Monitoring in Ambulatory Heart Failure Patients. Circulation 2007, 116, 2952–2959. [Google Scholar] [CrossRef]
- Ritzema, J.; Troughton, R.; Melton, I.; Crozier, I.; Doughty, R.; Krum, H.; Walton, A.; Adamson, P.; Kar, S.; Shah, P.K.; et al. Physician-Directed Patient Self-Management of Left Atrial Pressure in Advanced Chronic Heart Failure. Circulation 2010, 121, 1086–1095. [Google Scholar] [CrossRef]
- Pretorius, V.; Birgersdotter-Green, U.; Heywood, J.T.; Hafelfinger, W.; Gutfinger, D.E.; Eigler, N.L.; Love, C.J.; Abraham, W.T. An implantable left atrial pressure sensor lead designed for percutaneous extraction using standard techniques. Pacing Clin. Electrophysiol. 2013, 36, 570–577. [Google Scholar] [CrossRef]
- Casimir Ahn, H.; Delshad, B. An Implantable Pressure Sensor for Long-term Wireless Monitoring of Cardiac Function-First Study in Man. J. Cardiovasc. Dis. Diagn. 2016, 4, 1000252. [Google Scholar] [CrossRef]
- Hubbert, L.; Baranowski, J.; Delshad, B.; Ahn, H. Left Atrial Pressure Monitoring with an Implantable Wireless Pressure Sensor after Implantation of a Left Ventricular Assist Device. ASAIO J. 2017, 63, e60–e65. [Google Scholar] [CrossRef]
- Grose, R.; Strain, J.; Cohen, M.V. Pulmonary arterial V waves in mitral regurgitation: Clinical and experimental observations. Circulation 1984, 69, 214–222. [Google Scholar] [CrossRef]
- Klein, A.L.; Stewart, W.J.; Bartlett, J.; Cohen, G.I.; Kahan, F.; Pearce, G.; Husbands, K.; Bailey, A.S.; Salcedo, E.E.; Cosgrove, D.M. Effects of mitral regurgitation on pulmonary venous flow and left atrial pressure: An intraoperative transesophageal echocardiographic study. J. Am. Coll. Cardiol. 1992, 20, 1345–1352. [Google Scholar] [CrossRef] [PubMed]
- Ritzema-Carter, J.L.T.; Smyth, D.; Troughton, R.W.; Crozier, I.G.; Melton, I.C.; Richards, A.M.; Eigler, N.; Whiting, J.; Kar, S.; Krum, H.; et al. Dynamic Myocardial Ischemia Caused by Circumflex Artery Stenosis Detected by a New Implantable Left Atrial Pressure Monitoring Device. Circulation 2006, 113, e705–e706. [Google Scholar] [CrossRef]
- D’Amario, D.; Restivo, A.; Merkin, D.; Crea, F.; Ince, H.; Sievert, H.; Schaefer, U.; Trani, C.; Di Mario, C.; Anker, S.; et al. Safety, usability, and performance of a wireless left atrial pressure monitoring system in patients with heart failure: The VECTOR-HF trial (final results). Eur. Heart J. 2023, 44 (Suppl. S2), 902–911. [Google Scholar] [CrossRef] [PubMed]
- Perl, L.; Soifer, E.; Bartunek, J.; Erdheim, D.; Köhler, F.; Abraham, W.T.; Meerkin, D. A Novel Wireless Left Atrial Pressure Monitoring System for Patients with Heart Failure, First Ex-Vivo and Animal Experience. J. Cardiovasc. Transl. Res. 2019, 12, 290–298. [Google Scholar] [CrossRef]
- Magalski, A.; Adamson, P.; Gadler, F.; Böehm, M.; Steinhaus, D.; Reynolds, D.; Vlach, K.; Linde, C.; Cremers, B.; Sparks, B.; et al. Continuous ambulatory right heart pressure measurements with an implantable hemodynamic monitor: A multicenter, 12-month follow-up study of patients with chronic heart failure. J. Card. Fail. 2002, 8, 63–70. [Google Scholar] [CrossRef]
- Reynolds, D.W.; Bartelt, N.; Taepke, R.; Bennett, T.D. Measurement of pulmonary artery diastolic pressure from the right ventricle. J. Am. Coll. Cardiol. 1995, 25, 1176–1182. [Google Scholar] [CrossRef]
- Adamson, P.B.; Magalski, A.; Braunschweig, F.; Böhm, M.; Reynolds, D.; Steinhaus, D.; Luby, A.; Linde, C.; Ryden, L.; Cremers, B.; et al. Ongoing right ventricular hemodynamics in heart failure. J. Am. Coll. Cardiol. 2003, 41, 565–571. [Google Scholar] [CrossRef]
- Bourge, R.C.; Abraham, W.T.; Adamson, P.B.; Aaron, M.F.; Aranda, J.M.; Magalski, A.; Zile, M.R.; Smith, A.L.; Smart, F.W.; O’Shaughnessy, M.A.; et al. Randomized Controlled Trial of an Implantable Continuous Hemodynamic Monitor in Patients with Advanced Heart Failure. J. Am. Coll. Cardiol. 2008, 51, 1073–1079. [Google Scholar] [CrossRef]
- Klapholz, M.; Mauer, M.; Lowe, A.M. Hospitalization for heart failure in the presence of a normal left ventricular ejection fraction. Results of the New York Heart Failure Registry. ACC Curr. J. Rev. 2004, 13, 37. [Google Scholar] [CrossRef]
- Owan, T.E.; Hodge, D.O.; Herges, R.M.; Jacobsen, S.J.; Roger, V.L.; Redfield, M.M. Trends in Prevalence and Outcome of Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2006, 355, 251–259. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Smith, G.L.; Masoudi, F.A.; Vaccarino, V.; Radford, M.J.; Krumholz, H.M. Outcomes in heart failure patients with preserved ejection fraction mortality, readmission and functional decline. ACC Curr. J. Rev. 2003, 12, 61. [Google Scholar] [CrossRef]
- Abraham, W.T.; Adamson, P.B.; Bourge, R.C.; Aaron, M.F.; Costanzo, M.R.; Stevenson, L.W.; Strickland, W.; Neelagaru, S.; Raval, N.; Krueger, S.; et al. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: A randomised controlled trial. Lancet 2011, 377, 658–666. [Google Scholar] [CrossRef]
- Adamson, P.B.; Abraham, W.T.; Aaron, M.; Aranda, J.M.; Bourge, R.C.; Smith, A.; Stevenson, L.W.; Bauman, J.G.; Yadav, J.S. CHAMPION∗ Trial Rationale and Design: The Long-Term Safety and Clinical Efficacy of a Wireless Pulmonary Artery Pressure Monitoring System. J. Card. Fail. 2011, 17, 3–10. [Google Scholar] [CrossRef]
- Abraham, W.T.; Stevenson, L.W.; Bourge, R.C.; Lindenfeld, J.A.; Bauman, J.G.; Adamson, P.B. Sustained efficacy of pulmonary artery pressure to guide adjustment of chronic heart failure therapy: Complete follow-up results from the CHAMPION randomised trial. Lancet 2016, 387, 453–461. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Stevenson, L.W.; Adamson, P.B.; Desai, A.S.; Heywood, J.T.; Bourge, R.C.; Bauman, J.; Abraham, W.T. Interventions Linked to Decreased Heart Failure Hospitalizations during Ambulatory Pulmonary Artery Pressure Monitoring. JACC Heart Fail. 2016, 4, 333–344. [Google Scholar] [CrossRef]
- Lindenfeld, J.; Zile, M.R.; Desai, A.S.; Bhatt, K.; Ducharme, A.; Horstmanshof, D.; Krim, S.R.; Maisel, A.; Mehra, M.R.; Paul, S.; et al. Haemodynamic-guided management of heart failure (GUIDE-HF): A randomised controlled trial. Lancet 2021, 398, 991–1001. [Google Scholar] [CrossRef]
- Angermann, C.E.; Assmus, B.; Anker, S.D.; Asselbergs, F.W.; Brachmann, J.; Brett, M.E.; Brugts, J.J.; Ertl, G.; Ginn, G.; Hilker, L.; et al. Pulmonary artery pressure-guided therapy in ambulatory patients with symptomatic heart failure: CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF). Eur. J. Heart Fail. 2020, 22, 1891–1901. [Google Scholar] [CrossRef]
- Shavelle, D.M.; Desai, A.S.; Stevenson, L.W. Response by Shavelle et al. to Letters Regarding Article, “Lower Rates of Heart Failure and All-Cause Hospitalizations During Pulmonary Artery Pressure-Guided Therapy for Ambulatory Heart Failure: One-Year Outcomes from the CardioMEMS Post-Approval Study”. Circ. Heart Fail. 2021, 14, e008046. [Google Scholar] [CrossRef]
- Heywood, J.T.; Zalawadiya, S.; Bourge, R.C.; Costanzo, M.R.; Desai, A.S.; Rathman, L.D.; Raval, N.; Shavelle, D.M.; Henderson, J.D.; Brett, M.-E.; et al. Sustained Reduction in Pulmonary Artery Pressures and Hospitalizations During 2 Years of Ambulatory Monitoring. J. Card. Fail. 2023, 29, 56–66. [Google Scholar] [CrossRef]
- Abraham, J.; Bharmi, R.; Jonsson, O.; Oliveira, G.H.; Artis, A.; Valika, A.; Capodilupo, R.; Adamson, P.B.; Roberts, G.; Dalal, N.; et al. Association of Ambulatory Hemodynamic Monitoring of Heart Failure with Clinical Outcomes in a Concurrent Matched Cohort Analysis. JAMA Cardiol. 2019, 4, 556–563. [Google Scholar] [CrossRef]
- Desai, A.S.; Bhimaraj, A.; Bharmi, R.; Jermyn, R.; Bhatt, K.; Shavelle, D.; Redfield, M.M.; Hull, R.; Pelzel, J.; Davis, K.; et al. Ambulatory Hemodynamic Monitoring Reduces Heart Failure Hospitalizations in “Real-World” Clinical Practice. J. Am. Coll. Cardiol. 2017, 69, 2357–2365. [Google Scholar] [CrossRef]
- Kishino, Y.; Kuno, T.; Malik, A.H.; Lanier, G.M.; Sims, D.B.; Ruiz Duque, E.; Briasoulis, A. Effect of pulmonary artery pressure-guided therapy on heart failure readmission in a nationally representative cohort. ESC Heart Fail. 2022, 9, 2511–2517. [Google Scholar] [CrossRef]
- Cowie, M.R.; Flett, A.; Cowburn, P.; Foley, P.; Chandrasekaran, B.; Loke, I.; Critoph, C.; Gardner, R.S.; Guha, K.; Betts, T.R.; et al. Real-world evidence in a national health service: Results of the UK CardioMEMS HF System Post-Market Study. ESC Heart Fail. 2022, 9, 48–56. [Google Scholar] [CrossRef]
- Veenis, J.F.; Manintveld, O.C.; Constantinescu, A.A.; Caliskan, K.; Birim, O.; Bekkers, J.A.; van Mieghem, N.M.; den Uil, C.A.; Boersma, E.; Lenzen, M.J.; et al. Design and rationale of haemodynamic guidance with CardioMEMS in patients with a left ventricular assist device: The HEMO-VAD pilot study. ESC Heart Fail. 2019, 6, 194–201. [Google Scholar] [CrossRef]
- Veenis, J.F.; Radhoe, S.P.; van Mieghem, N.M.; Manintveld, O.C.; Bekkers, J.A.; Caliskan, K.; Bogers, A.J.J.C.; Zijlstra, F.; Brugts, J.J. Safety and feasibility of hemodynamic pulmonary artery pressure monitoring using the CardioMEMS device in LVAD management. J. Card. Surg. 2021, 36, 3271–3280. [Google Scholar] [CrossRef]
- Veenis, J.F.; Radhoe, S.P.; van Mieghem, N.M.; Manintveld, O.C.; Caliskan, K.; Birim, O.; Bekkers, J.A.; Boersma, E.; Lenzen, M.J.; Zijlstra, F.; et al. Remote hemodynamic guidance before and after left ventricular assist device implantation: Short-term results from the HEMO-VAD pilot study. Future Cardiol. 2021, 17, 885–898. [Google Scholar] [CrossRef]
- Brugts, J.J.; Radhoe, S.P.; Clephas, P.R.D.; Aydin, D.; van Gent, M.W.F.; Szymanski, M.K.; Rienstra, M.; van den Heuvel, M.H.; da Fonseca, C.A.; Linssen, G.C.M.; et al. Remote haemodynamic monitoring of pulmonary artery pressures in patients with chronic heart failure (MONITOR-HF): A randomised clinical trial. Lancet 2023, 401, 2113–2123. [Google Scholar] [CrossRef]
- Mullens, W.; Sharif, F.; Dupont, M.; Rothman, A.M.K.; Wijns, W. Digital health care solution for proactive heart failure management with the Cordella Heart Failure System: Results of the SIRONA first-in-human study. Eur. J. Heart Fail. 2020, 22, 1912–1919. [Google Scholar] [CrossRef]
- Sharif, F.; Rosenkranz, S.; Bartunek, J.; Kempf, T.; Assmus, B.; Mahon, N.G.; Mullens, W. Safety and efficacy of a wireless pulmonary artery pressure sensor: Primary endpoint results of the SIRONA 2 clinical trial. ESC Heart Fail. 2022, 9, 2862–2872. [Google Scholar] [CrossRef]
- Guichard, J.L.; Cowger, J.A.; Chaparro, S.V.; Kiernan, M.S.; Mullens, W.; Mahr, C.; Mullin, C.; Forouzan, O.; Hiivala, N.J.; Sauerland, A.; et al. Rationale and Design of the Proactive-HF Trial for Managing Patients with NYHA Class III Heart Failure by Using the Combined Cordella Pulmonary Artery Sensor and the Cordella Heart Failure System. J. Card. Fail. 2023, 29, 171–180. [Google Scholar] [CrossRef]
- Ivey-Miranda, J.B.; Wetterling, F.; Gaul, R.; Sheridan, S.; Asher, J.L.; Rao, V.S.; Maulion, C.; Mahoney, D.; Mebazaa, A.; Gray, A.P.; et al. Changes in inferior vena cava area represent a more sensitive metric than changes in filling pressures during experimental manipulation of intravascular volume and tone. Eur. J. Heart Fail. 2022, 24, 455–462. [Google Scholar] [CrossRef]
- Sheridan, W.S.; Wetterling, F.; Testani, J.M.; Borlaug, B.A.; Fudim, M.; Damman, K.; Gray, A.; Gaines, P.; Poloczek, M.; Madden, S.; et al. Safety and performance of a novel implantable sensor in the inferior vena cava under acute and chronic intravascular volume modulation. Eur. J. Heart Fail. 2023, 25, 754–763. [Google Scholar] [CrossRef]
- Anand, I.S. Cardiorenal syndrome: A cardiologist’s perspective of pathophysiology. Clin. J. Am. Soc. Nephrol. 2013, 8, 1800–1807. [Google Scholar] [CrossRef]
- Drazner, M.H.; Rame, J.E.; Stevenson, L.W.; Dries, D.L. Prognostic Importance of Elevated Jugular Venous Pressure and a Third Heart Sound in Patients with Heart Failure. N. Engl. J. Med. 2001, 345, 574–581. [Google Scholar] [CrossRef]
- Manavi, T.; Vazquez, P.; O’Grady, H.; Martina, J.; Rose, M.; Nielsen, D.; Fitzpatrick, D.; Forouzan, O.; Nagy, M.; Sharif, F.; et al. A novel wireless implant for central venous pressure measurement: First animal experience. Cardiovasc. Digit. Health J. 2020, 1, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Manavi, T.; Vazquez, P.; Tubassam, M.; Zafar, J.; Sharif, F.; Zafar, H. Determination of optimal implantation site in central venous system for wireless hemodynamic monitoring. Int. J. Cardiol. Heart Vasc. 2020, 27, 100510. [Google Scholar] [CrossRef]
- Manavi, T.; Ijaz, M.; O’Grady, H.; Nagy, M.; Martina, J.; Finucane, C.; Sharif, F.; Zafar, H. Design and Haemodynamic Analysis of a Novel Anchoring System for Central Venous Pressure Measurement. Sensors 2022, 22, 8552. [Google Scholar] [CrossRef]
- Raj, L.M.; Saxon, L.A. Haemodynamic Monitoring Devices in Heart Failure: Maximising Benefit with Digitally Enabled Patient Centric Care. Arrhythm. Electrophysiol. Rev. 2018, 7, 294–298. [Google Scholar] [CrossRef]
- Schmier, J.K.; Ong, K.L.; Fonarow, G.C. Cost-Effectiveness of Remote Cardiac Monitoring With the CardioMEMS Heart Failure System. Clin. Cardiol. 2017, 40, 430–436. [Google Scholar] [CrossRef]
- Herbert, R.; Lim, H.-R.; Rigo, B.; Yeo, W.-H. Fully implantable wireless batteryless vascular electronics with printed soft sensors for multiplex sensing of hemodynamics. Sci. Adv. 2022, 8, eabm1175. [Google Scholar] [CrossRef]
- Craig, W.; Ohlmann, S.E. Remote Patient Management Facilitates Guideline Directed Medical Therapy Improving Outcomes. J. Card. Fail. 2022, 28, S49. [Google Scholar] [CrossRef]
- Manavi, G.S.T.; Barton, J.; Coen, E.; Zafar, H.; Sharif, F. Remote Patient Management of Chronic Heart Failure during COVID-19. Health Promotion through E-Health: Challenges and Opportunities, Conference Proceeding 2021. Available online: https://www.researchgate.net/publication/363272741_Remote_Patient_Management_of_Chronic_Heart_Failure_during_COVID-19#fullTextFileContent (accessed on 6 February 2024).
- Manavi, G.S.T.; Barton, J.; Coen, E.; Fitzpatrick, D.; Finucane, C.; Williams, M.; Zafar, H.; Sharif, F. Remote Patient Management of Chronic Heart Failure in West Ireland. In Proceedings of the EuroPCR 2023, Conference Presentation, Paris, France, 16 May 2023; Available online: https://eposter.europa-organisation.com/2023/europcr/index/slide/abstract/143 (accessed on 6 February 2024).
- Caples, N. Fluid Heart Tracker. Health Innovation Hub Ireland. Available online: https://hih.ie/downloads/case-studies/Spark-Ignite-case-study_Norma-Caples.pdf (accessed on 6 February 2024).
- Caples, N. The Fluid Heart Tracker App-Knowing When to Make Contact for Early Medical Intervention for Deteriorating Heart Failure. Health Summit. 19 February 2023. Available online: https://healthsummit.ie/wp-content/uploads/2023/02/19th-National-Health-Summit.pptx.pdf (accessed on 6 February 2024).
- Fudim, M.; Yazdi, D.; Egolum, U.; Haghighat, A.; Kottam, A.; Sauer, A.J.; Shah, H.; Kumar, P.; Rakita, V.; Centen, C.; et al. Use of a Cardiac Scale to Predict Heart Failure Events: Design of SCALE-HF 1. Circ Heart Fail 2023, 16, e010012. [Google Scholar] [CrossRef]
- Seto, E.; Leonard, K.J.; Cafazzo, J.A.; Barnsley, J.; Masino, C.; Ross, H.J. Mobile phone-based telemonitoring for heart failure management: A randomized controlled trial. J. Med. Internet Res. 2012, 14, e31. [Google Scholar] [CrossRef]
- Bouabida, K.; Malas, K.; Talbot, A.; Desrosiers, M.-È.; Lavoie, F.; Lebouché, B.; Taguemout, M.; Rafie, E.; Lessard, D.; Pomey, M.-P. Remote Patient Monitoring Program for COVID-19 Patients Following Hospital Discharge: A Cross-Sectional Study. Front. Digit. Health 2021, 3, 721044. [Google Scholar] [CrossRef]
- Silva-Cardoso, J.; Juanatey, J.R.G.; Comin-Colet, J.; Sousa, J.M.; Cavalheiro, A.; Moreira, E. The Future of Telemedicine in the Management of Heart Failure Patients. Card. Fail. Rev. 2021, 7, e11. [Google Scholar] [CrossRef]
- D’Amario, D.; Canonico, F.; Rodolico, D.; Borovac, J.A.; Vergallo, R.; Montone, R.A.; Galli, M.; Migliaro, S.; Restivo, A.; Massetti, M.; et al. Telemedicine, Artificial Intelligence and Humanisation of Clinical Pathways in Heart Failure Management: Back to the Future and Beyond. Card. Fail. Rev. 2020, 6, e16. [Google Scholar] [CrossRef]
- Ganguli, I.; Gordon, W.J.; Lupo, C.; Sands-Lincoln, M.; George, J.; Jackson, G.; Rhee, K.; Bates, D.W. Machine Learning and the Pursuit of High-Value Health Care. NEJM Catal. 2020, 1. [Google Scholar] [CrossRef]
- Hillmann, H.A.K.; Hansen, C.; Przibille, O.; Duncker, D. The patient perspective on remote monitoring of implantable cardiac devices. Front. Cardiovasc. Med. 2023, 10, 1123848. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device | Target Location | Parameters Measured | Indications | No. of Clinical Trials | No. of Pre-Clinical Trials | Data Collection |
|---|---|---|---|---|---|---|
| TitanTM pressure sensor (ISS Inc., Ypsilanti, MI, USA) [38,39] | Left atrium | Left atrial pressure |
| Two
| >60 animal studies tested the sensor in all four chambers of the heart, as well as the aortic and pulmonary arteries. | External reader device that captures pressure signals and stores them on a computer that transmits data to a central server. |
| V-LAPTM (Vectorious Medical Technologies), HeartPOD (St. Jude Medical, Minneapolis, MN, USA) [33,36,43] | Interatrial septum | Left atrial pressure, atrial ECG, body temperature |
| Three
| NA | External reader device (wearable belt) that transmits data to a secure cloud server. |
| Chronicle IHM (Medtronic, Inc., Minneapolis, MN, USA) [45,47,48] | Upper chest with a sensor attached to the right ventricle | Right ventricular pressure |
|
| NA | Pressure data is captured by the monitor’s sensing circuitry, stored in the memory, and transmitted via radiofrequency-linked telemetry to a programmer in the clinic. |
| CardioMEMS (Abbott) [54,57,58,64,65,68] | Pulmonary artery | Pulmonary artery pressure |
| Six
| NA | External reader device (pillow) that transmits data to a secure cloud server. |
| Cordella (Endotronix, Inc. Lisle, IL, USA) [69,70,71] | Right pulmonary artery | Pulmonary artery pressure |
|
| NA | External reader device (handheld monitor) that transmits data to a secure cloud server. |
| Fire1 (Foundry Innovation and Research 1 Ltd., Dublin, Ireland) [72,73] | Inferior vena cava | Inferior vena cava area and fluid volume |
| One
| Two
| External reader device (belt) that transmits data to a secure cloud server. |
| Central venous pressure sensor (University of Galway, Ireland—Endotronix Inc., Lisle, IL, USA) [76] | Inferior vena cava | Central venous pressure |
| NA | One
| External reader device (handheld monitor) that transmits data to a secure cloud server. |
| Vascular electronic system/Wireless stent [81] | Right iliac artery | Arterial pressure, pulse rate, and flow | Coronary artery disease | NA | One
| NA |
| Study | Technology Used | Parameters Measured | Indications | Study Specifics (Pilot/Prospective/Retrospective/Observational/Experimental) | Patient Access |
|---|---|---|---|---|---|
| TIM-HF2 [23,24] | Smart-phone/ Application integrated with a secure cloud server | ECG, BP, SPO2, weight |
| Prospective, randomized multicentre trial | Yes |
| CHFS Ireland, CHFS US [82,83,84] | Smart-phone/ Application integrated with a secure cloud server | BP, HR, SPO2, weight |
| Prospective, single-center, observational study (Galway, Ireland), Retrospective multi-center study (Seguin, San Antonio, TX, USA). | Yes |
| Fluid Heart Tracker [85,86] | Smart-phone/ Application | Weight |
| Pilot, observational study | Yes |
| Scale-HF [87] | Smart scale integrated with smart phone-application (patient-end) and a clinical dashboard | ECG, BCG, IPG |
| Prospective, multicentre study | Restricted to weight, pulse rate, and fluid status only. |
| Mobile phone-based telemonitoring [88] | Mobile phone-based messaging (not app-based) | ECG (weekly), weight and BP (daily) |
| Single-center, randomized controlled trial | Yes |
| Telecare and CareSimple-COVID [89] | Phone calls, Smart-phone/ Application | COVID-19 progression, medications, and follow-ups |
| Single-center, cross-sectional study | No, Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manavi, T.; Zafar, H.; Sharif, F. An Era of Digital Healthcare—A Comprehensive Review of Sensor Technologies and Telehealth Advancements in Chronic Heart Failure Management. Sensors 2024, 24, 2546. https://doi.org/10.3390/s24082546
Manavi T, Zafar H, Sharif F. An Era of Digital Healthcare—A Comprehensive Review of Sensor Technologies and Telehealth Advancements in Chronic Heart Failure Management. Sensors. 2024; 24(8):2546. https://doi.org/10.3390/s24082546
Chicago/Turabian StyleManavi, Tejaswini, Haroon Zafar, and Faisal Sharif. 2024. "An Era of Digital Healthcare—A Comprehensive Review of Sensor Technologies and Telehealth Advancements in Chronic Heart Failure Management" Sensors 24, no. 8: 2546. https://doi.org/10.3390/s24082546
APA StyleManavi, T., Zafar, H., & Sharif, F. (2024). An Era of Digital Healthcare—A Comprehensive Review of Sensor Technologies and Telehealth Advancements in Chronic Heart Failure Management. Sensors, 24(8), 2546. https://doi.org/10.3390/s24082546