

Accuracy of Rhythm Diagnostic Systems’ MultiSense® in Detection of Arterial Oxygen Saturation and Respiratory Rate During Hypoxia in Humans: Effects of Skin Color and Device Localization

 , ,
, ,
Abstract
1. Introduction
2. Population and Methods
2.1. Population
2.2. Study Design
2.2.1. Study Time Frame
2.2.2. Investigational Device and Reference Monitor Descriptions
General Description of the Investigational Device
- An innovative multiparametric device in the form of a single miniaturized adhesive patch that is placed on the upper body to collect physiological data continuously;
- A phone, connected by Bluetooth to the patch, equipped with an application that receives the data collected and sends it to the cloud using a wireless connection (cellular network or Wi-Fi);
- A GDPR and ISO27000-compliant cloud infrastructure for data storage and interpretation, running proprietary algorithms that derivate clinical parameters from the raw data collected by the patch;
- A secured web portal for medical professionals that allows them to access recent and historical data for their patients.
General Description of the Reference Monitor
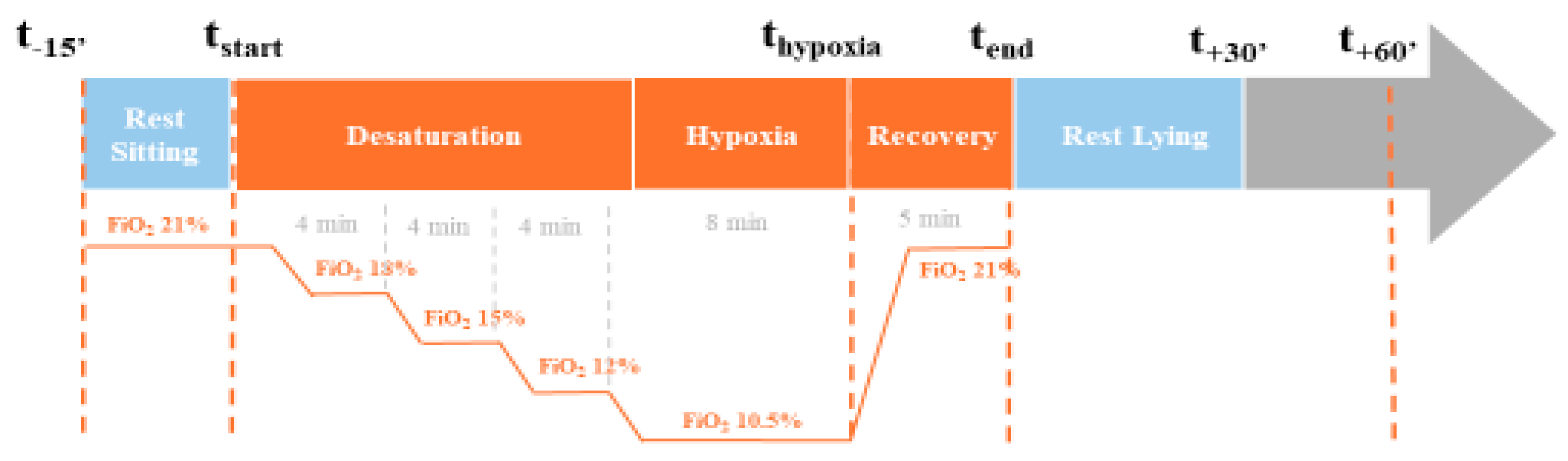
2.2.3. Description of the Hypoxia Test
2.3. Data Collection, Pre-Processing, and Quality Assessment
2.3.1. Data Collection
2.3.2. Data Pre-Processing
2.3.3. Assessment of the Quality of Data Acquisition
2.4. Statistical Analysis
3. Results
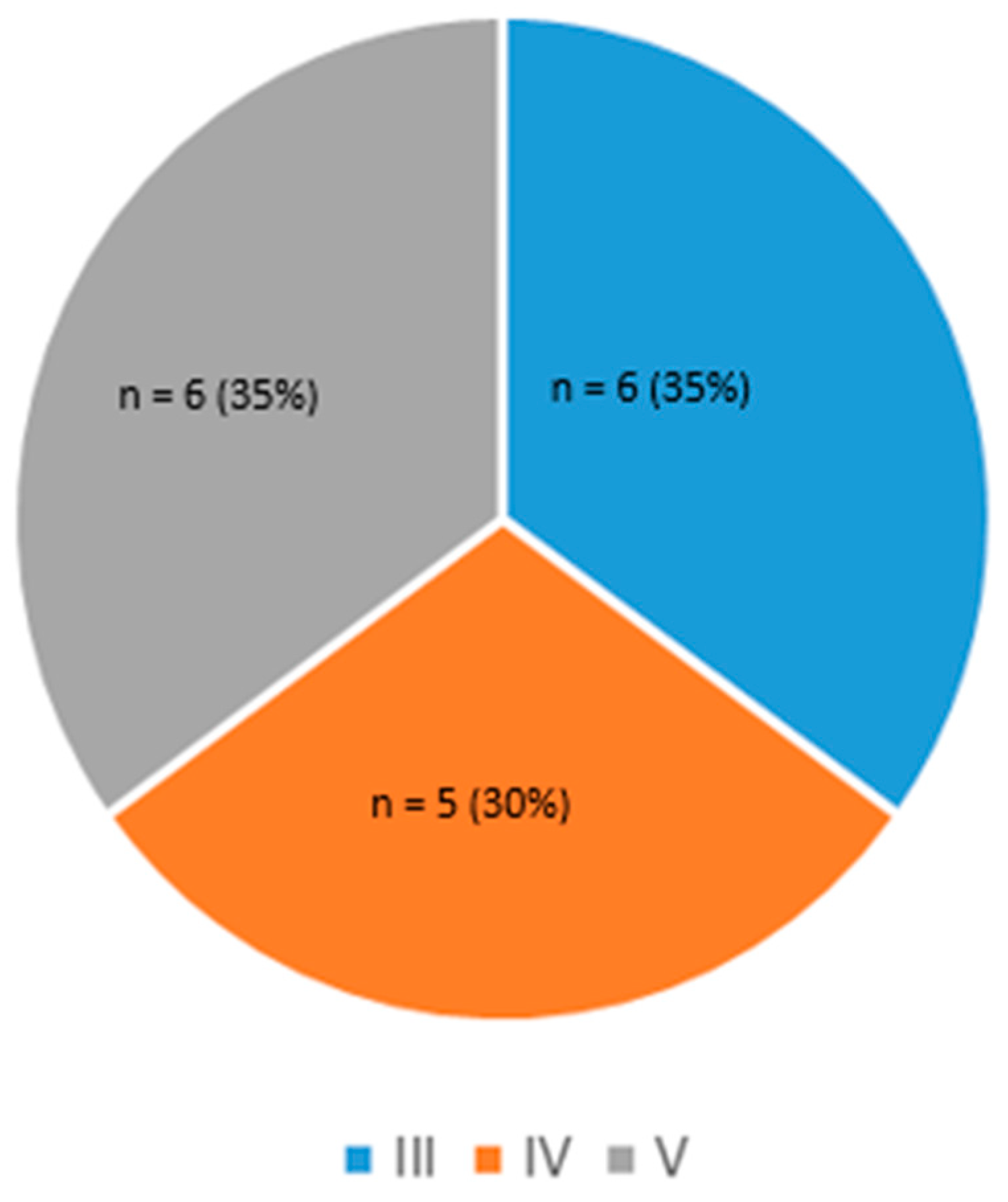
3.1. Population Characteristics
3.2. Comparisons Between the Two Devices
3.2.1. Considering the Entire Population and Regardless of Skin Pigmentation and Device Positions
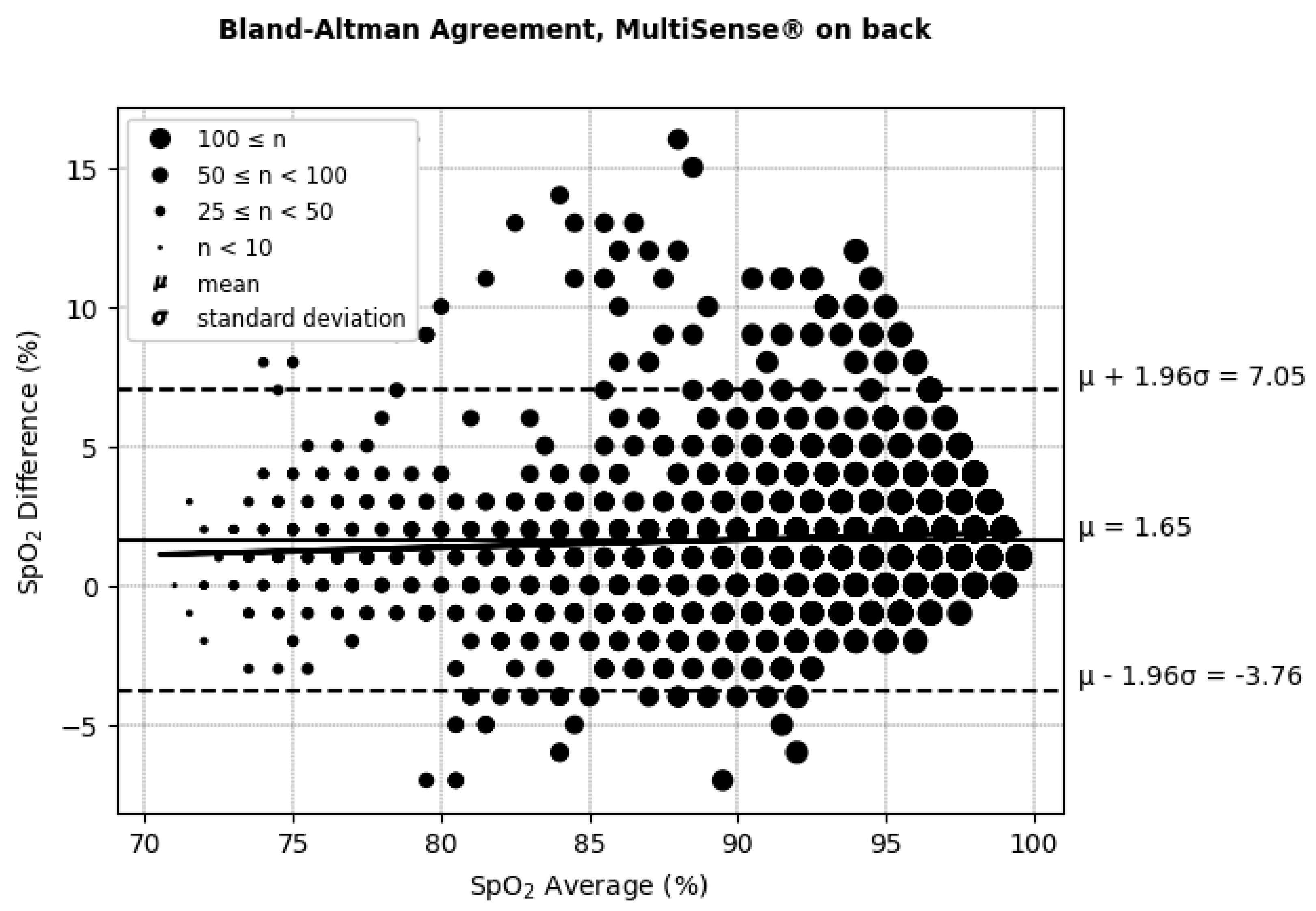
3.2.2. SpO2 Measurements
ARMS Accuracy and Device Placements
No Influence of Skin Color on ARMS
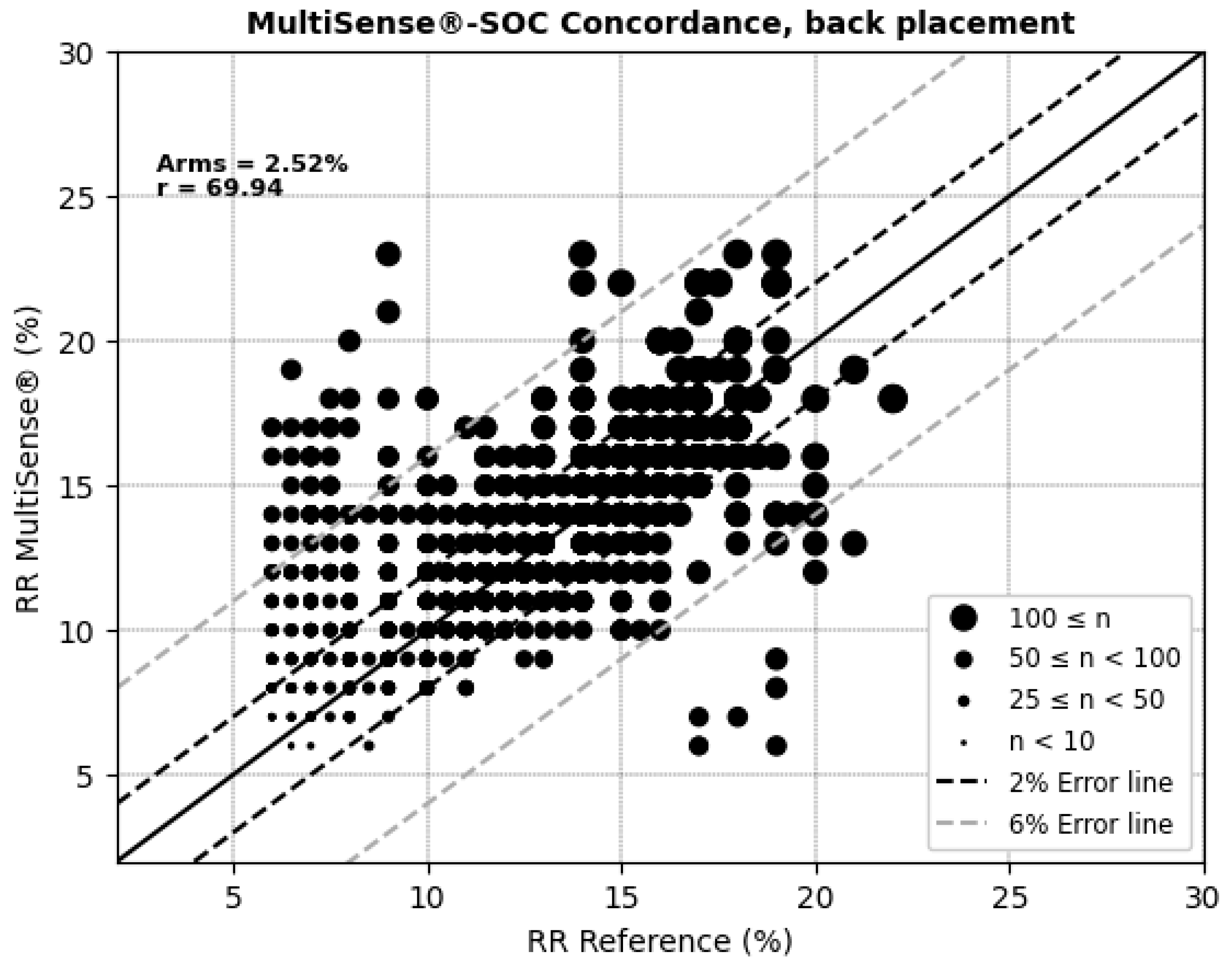
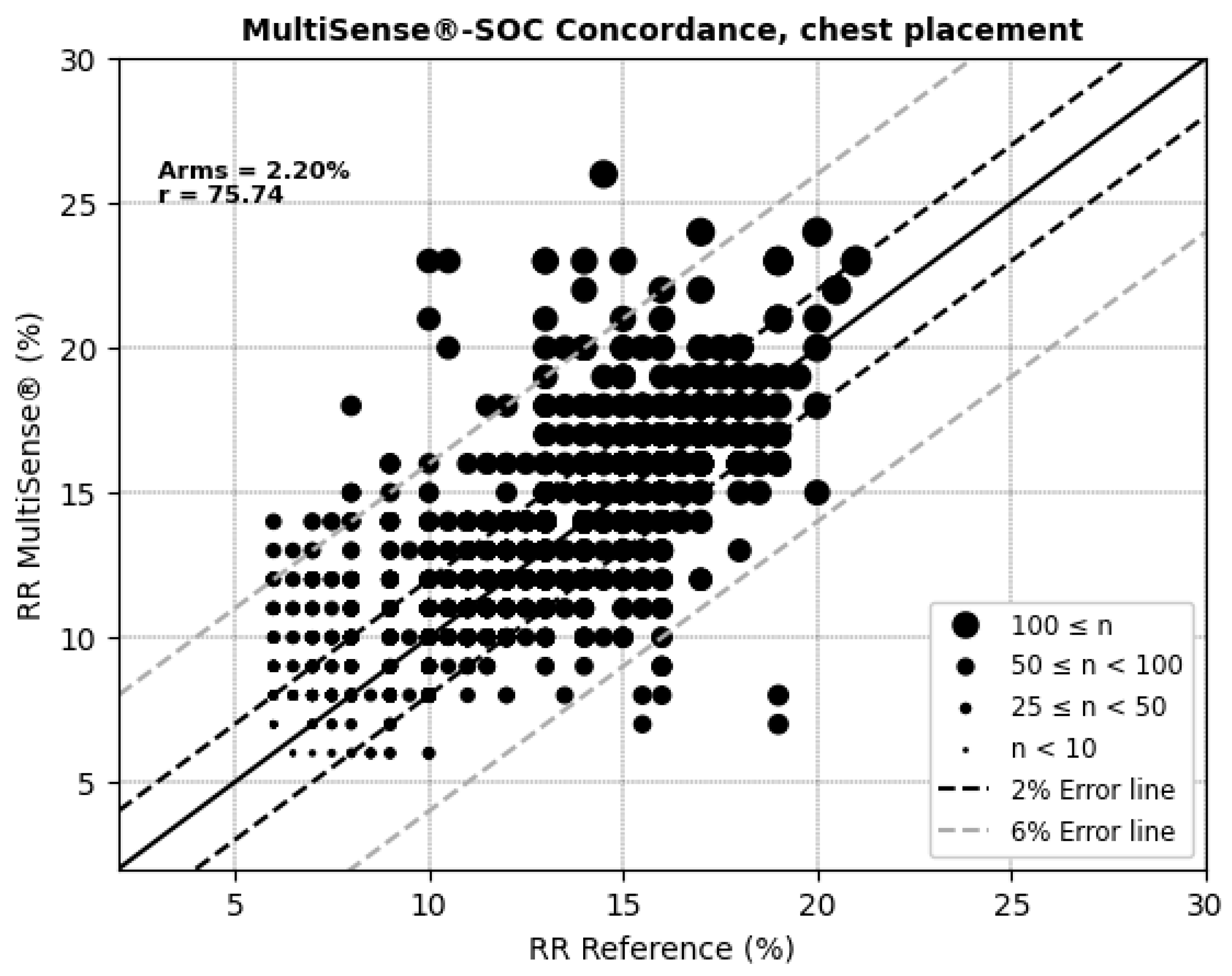
3.2.3. Respiratory Rate Measurements
ARMS Accuracy and Device Placements
3.2.4. Safety Assessment Considering Adverse Effects and Events
4. Discussion
4.1. Effectiveness and Safety of the Device MultiSense for SpO2 and Respiratory Rate Measurements
4.2. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Agarwal, S.K.; Heiss, G.; Barr, R.G.; Chang, P.P.; Loehr, L.R.; Chambless, L.E.; Shahar, E.; Kitzman, D.W.; Rosamond, W.D. Airflow Obstruction, Lung Function, and Risk of Incident Heart Failure: The Atherosclerosis Risk in Communities (ARIC) Study. Eur. J. Heart Fail. 2012, 14, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Prys-Picard, C.O.; Kellett, F.; Niven, R.M. Disproportionate Breathlessness Associated with Deep Sighing Breathing in a Patient Presenting with Difficult-to-Treat Asthma. Chest 2006, 130, 1723–1725. [Google Scholar] [CrossRef] [PubMed]
- Schiefer, L.M.; Treff, G.; Treff, F.; Schmidt, P.; Schäfer, L.; Niebauer, J.; Swenson, K.E.; Swenson, E.R.; Berger, M.M.; Sareban, M. Validity of Peripheral Oxygen Saturation Measurements with the Garmin Fēnix® 5X Plus Wearable Device at 4559 m. Sensors 2021, 21, 6363. [Google Scholar] [CrossRef] [PubMed]
- Quaresima, V.; Ferrari, M. COVID-19: Efficacy of Prehospital Pulse Oximetry for Early Detection of Silent Hypoxemia. Crit. Care 2020, 24, 501. [Google Scholar] [CrossRef] [PubMed]
- Massaroni, C.; Nicolò, A.; Lo Presti, D.; Sacchetti, M.; Silvestri, S.; Schena, E. Contact-Based Methods for Measuring Respiratory Rate. Sensors 2019, 19, 908. [Google Scholar] [CrossRef]
- Marinari, S.; Volpe, P.; Simoni, M.; Aventaggiato, M.; De Benedetto, F.; Nardini, S.; Sanguinetti, C.M.; Palange, P. Accuracy of a New Pulse Oximetry in Detection of Arterial Oxygen Saturation and Heart Rate Measurements: The SOMBRERO Study. Sensors 2022, 22, 5031. [Google Scholar] [CrossRef]
- Alvear-Catalán, M.; Montiglio, C.; Aravena-Nazif, D.; Viscor, G.; Araneda, O.F. Oxygen Saturation Curve Analysis in 2298 Hypoxia Awareness Training Tests of Military Aircrew Members in a Hypobaric Chamber. Sensors 2024, 24, 4168. [Google Scholar] [CrossRef] [PubMed]
- Paré, G.; Sicotte, C.; St-Jules, D.; Gauthier, R. Cost-Minimization Analysis of a Telehomecare Program for Patients with Chronic Obstructive Pulmonary Disease. Telemed. J. E Health 2006, 12, 114–121. [Google Scholar] [CrossRef]
- De San Miguel, K.; Smith, J.; Lewin, G. Telehealth Remote Monitoring for Community-Dwelling Older Adults with Chronic Obstructive Pulmonary Disease. Telemed. J. E Health 2013, 19, 652–657. [Google Scholar] [CrossRef]
- Hong, Y.; Lee, S.H. Effectiveness of Tele-Monitoring by Patient Severity and Intervention Type in Chronic Obstructive Pulmonary Disease Patients: A Systematic Review and Meta-Analysis. Int. J. Nurs. Stud. 2019, 92, 1–15. [Google Scholar] [CrossRef]
- Shah, N.B.; Der, E.; Ruggerio, C.; Heidenreich, P.A.; Massie, B.M. Prevention of Hospitalizations for Heart Failure with an Interactive Home Monitoring Program. Am. Heart J. 1998, 135, 373–378. [Google Scholar] [CrossRef]
- Andrès, E.; Talha, S.; Zulfiqar, A.-A.; Hajjam, M.; Ervé, S.; Hajjam, J.; Gény, B.; Hajjam El Hassani, A. Current Research and New Perspectives of Telemedicine in Chronic Heart Failure: Narrative Review and Points of Interest for the Clinician. J. Clin. Med. 2018, 7, 544. [Google Scholar] [CrossRef]
- Levitan, R.M. Pulse Oximetry as a Biomarker for Early Identification and Hospitalization of COVID-19 Pneumonia. Acad. Emerg. Med. 2020, 27, 785–786. [Google Scholar] [CrossRef]
- Luks, A.M.; Swenson, E.R. Pulse Oximetry for Monitoring Patients with COVID-19 at Home. Potential Pitfalls and Practical Guidance. Ann. Am. Thorac. Soc. 2020, 17, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Talha, S.; Lamrous, S.; Kassegne, L.; Lefebvre, N.; Zulfiqar, A.-A.; Tran Ba Loc, P.; Geny, M.; Meyer, N.; Hajjam, M.; Andrès, E.; et al. Early Hospital Discharge Using Remote Monitoring for Patients Hospitalized for COVID-19, Regardless of Need for Home Oxygen Therapy: A Descriptive Study. J. Clin. Med. 2023, 12, 5100. [Google Scholar] [CrossRef]
- Dünnwald, T.; Kienast, R.; Niederseer, D.; Burtscher, M. The Use of Pulse Oximetry in the Assessment of Acclimatization to High Altitude. Sensors 2021, 21, 1263. [Google Scholar] [CrossRef] [PubMed]
- García, I.; Drobnic, F.; Javierre, C.; Pons, V.; Viscor, G. Severe Hypoxic Exercise Does Not Impair Lung Diffusion in Elite Swimmers. High. Alt. Med. Biol. 2021, 22, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Woorons, X.; Faucher, C.; Dufour, S.P.; Brocherie, F.; Robach, P.; Connes, P.; Brugniaux, J.V.; Verges, S.; Gaston, A.F.; Millet, G.; et al. Hypoventilation Training Including Maximal End-Expiratory Breath Holding Improves the Ability to Repeat High-Intensity Efforts in Elite Judo Athletes. Front. Physiol. 2024, 15, 1441696. [Google Scholar] [CrossRef] [PubMed]
- Geny, M.; Andres, E.; Talha, S.; Geny, B. Liability of Health Professionals Using Sensors, Telemedicine and Artificial Intelligence for Remote Healthcare. Sensors 2024, 24, 3491. [Google Scholar] [CrossRef] [PubMed]
- Nitzan, M.; Nitzan, I.; Arieli, Y. The Various Oximetric Techniques Used for the Evaluation of Blood Oxygenation. Sensors 2020, 20, 4844. [Google Scholar] [CrossRef] [PubMed]
- Pretto, J.J.; Roebuck, T.; Beckert, L.; Hamilton, G. Clinical Use of Pulse Oximetry: Official Guidelines from the Thoracic Society of Australia and New Zealand. Respirology 2014, 19, 38–46. [Google Scholar] [CrossRef]
- Feiner, J.R.; Severinghaus, J.W.; Bickler, P.E. Dark Skin Decreases the Accuracy of Pulse Oximeters at Low Oxygen Saturation: The Effects of Oximeter Probe Type and Gender. Anesth. Analg. 2007, 105 (Suppl. 6), S18–S23. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.-K.I.; Charpignon, M.; Kim, H.; Josef, C.; de Hond, A.A.H.; Fojas, J.J.; Tabaie, A.; Liu, X.; Mireles-Cabodevila, E.; Carvalho, L.; et al. Analysis of Discrepancies Between Pulse Oximetry and Arterial Oxygen Saturation Measurements by Race and Ethnicity and Association with Organ Dysfunction and Mortality. JAMA Netw. Open 2021, 4, e2131674. [Google Scholar] [CrossRef]
- Wiles, M.D.; El-Nayal, A.; Elton, G.; Malaj, M.; Winterbottom, J.; Gillies, C.; Moppett, I.K.; Bauchmuller, K. The Effect of Patient Ethnicity on the Accuracy of Peripheral Pulse Oximetry in Patients with COVID-19 Pneumonitis: A Single-Centre, Retrospective Analysis. Anaesthesia 2022, 77, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Sjoding, M.W.; Dickson, R.P.; Iwashyna, T.J.; Gay, S.E.; Valley, T.S. Racial Bias in Pulse Oximetry Measurement. N. Engl. J. Med. 2020, 383, 2477–2478. [Google Scholar] [CrossRef]
- FDA. Pulse Oximeters—Premarket Notification Submissions [510(k)s]: Guidance for Industry and Food and Drug Administration Staff; Food and Drug Administration: Silver Spring, MD, USA, 2013. [Google Scholar]
- Bland, J.M.; Altman, D.G. Agreement between Methods of Measurement with Multiple Observations per Individual. J. Biopharm. Stat. 2007, 17, 571–582. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.; Charles, A.-L.; Zoll, J.; Guillot, M.; Lejay, A.; Singh, F.; Schlagowski, A.-I.; Isner-Horobeti, M.-E.; Pistea, C.; Charloux, A.; et al. Cryopreservation with Dimethyl Sulfoxide Prevents Accurate Analysis of Skinned Skeletal Muscle Fibers Mitochondrial Respiration. Biochimie 2014, 100, 227–233. [Google Scholar] [CrossRef]
- ANSI/AAMI/ISO 80601-2-55; Medical Electrical Equipment—Particular Requirements for the Basic Safety and Essential Performance of Respiratory Gas Monitors. AAMI: Arlington, VA, USA, 2013.
- Collins, J.-A.; Rudenski, A.; Gibson, J.; Howard, L.; O’Driscoll, R. Relating Oxygen Partial Pressure, Saturation and Content: The Haemoglobin-Oxygen Dissociation Curve. Breathe 2015, 11, 194–201. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Placement | ARMS % | Difference (SoC–MultiSense®) % (μmol/min/g) | Limit of Agreements (Bias ± 1.96SD) (μmol/min/g) | Correlation (Pearson’s Coefficient) Between the Difference and the Average of the SpO2 Measurements (%) (μmol/min/g) |
|---|---|---|---|---|
| Back | 2.94 | 1.65 [95% CI: 1.50, 1.74] | (−3.76, +7.05) | 6.85 |
| Chest | 2.98 | −0.12 [95% CI: −0.005, 0.265] | (−6.32, +6.08) | 5.17 |
| Placement | ARMS % | Difference (SoC–MultiSense®) % (μmol/min/g) | Limit of Agreements (Bias ± 1.96SD) (μmol/min/g) | Correlation (Pearson’s Coefficient) Between the Difference and Average of the SpO2 Measurements (%) (μmol/min/g) |
|---|---|---|---|---|
| Back | 2.52 | −0.82 [95% CI: −1.15, −0.97 | (−5.91, +4.26) | 20.51 |
| Chest | 2.20 | −0.50 [95% CI: −0.75, −0.55] | (−4.64, + 3.65) | 3.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evrard, C.; El Attaoui, A.; Pistea, C.; Enache, I.; Marriott, M.; Mayaud, L.; Charloux, A.; Geny, B. Accuracy of Rhythm Diagnostic Systems’ MultiSense® in Detection of Arterial Oxygen Saturation and Respiratory Rate During Hypoxia in Humans: Effects of Skin Color and Device Localization. Sensors 2025, 25, 127. https://doi.org/10.3390/s25010127
Evrard C, El Attaoui A, Pistea C, Enache I, Marriott M, Mayaud L, Charloux A, Geny B. Accuracy of Rhythm Diagnostic Systems’ MultiSense® in Detection of Arterial Oxygen Saturation and Respiratory Rate During Hypoxia in Humans: Effects of Skin Color and Device Localization. Sensors. 2025; 25(1):127. https://doi.org/10.3390/s25010127
Chicago/Turabian StyleEvrard, Charles, Amina El Attaoui, Cristina Pistea, Irina Enache, Mark Marriott, Louis Mayaud, Anne Charloux, and Bernard Geny. 2025. "Accuracy of Rhythm Diagnostic Systems’ MultiSense® in Detection of Arterial Oxygen Saturation and Respiratory Rate During Hypoxia in Humans: Effects of Skin Color and Device Localization" Sensors 25, no. 1: 127. https://doi.org/10.3390/s25010127
APA StyleEvrard, C., El Attaoui, A., Pistea, C., Enache, I., Marriott, M., Mayaud, L., Charloux, A., & Geny, B. (2025). Accuracy of Rhythm Diagnostic Systems’ MultiSense® in Detection of Arterial Oxygen Saturation and Respiratory Rate During Hypoxia in Humans: Effects of Skin Color and Device Localization. Sensors, 25(1), 127. https://doi.org/10.3390/s25010127