
Assessing Effectiveness of Passive Exoskeletons and Tool Selection on Ergonomic Safety in Manhole Cover Removal

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Passive Back-Support Exoskeleton
2.3. Experimental Procedure
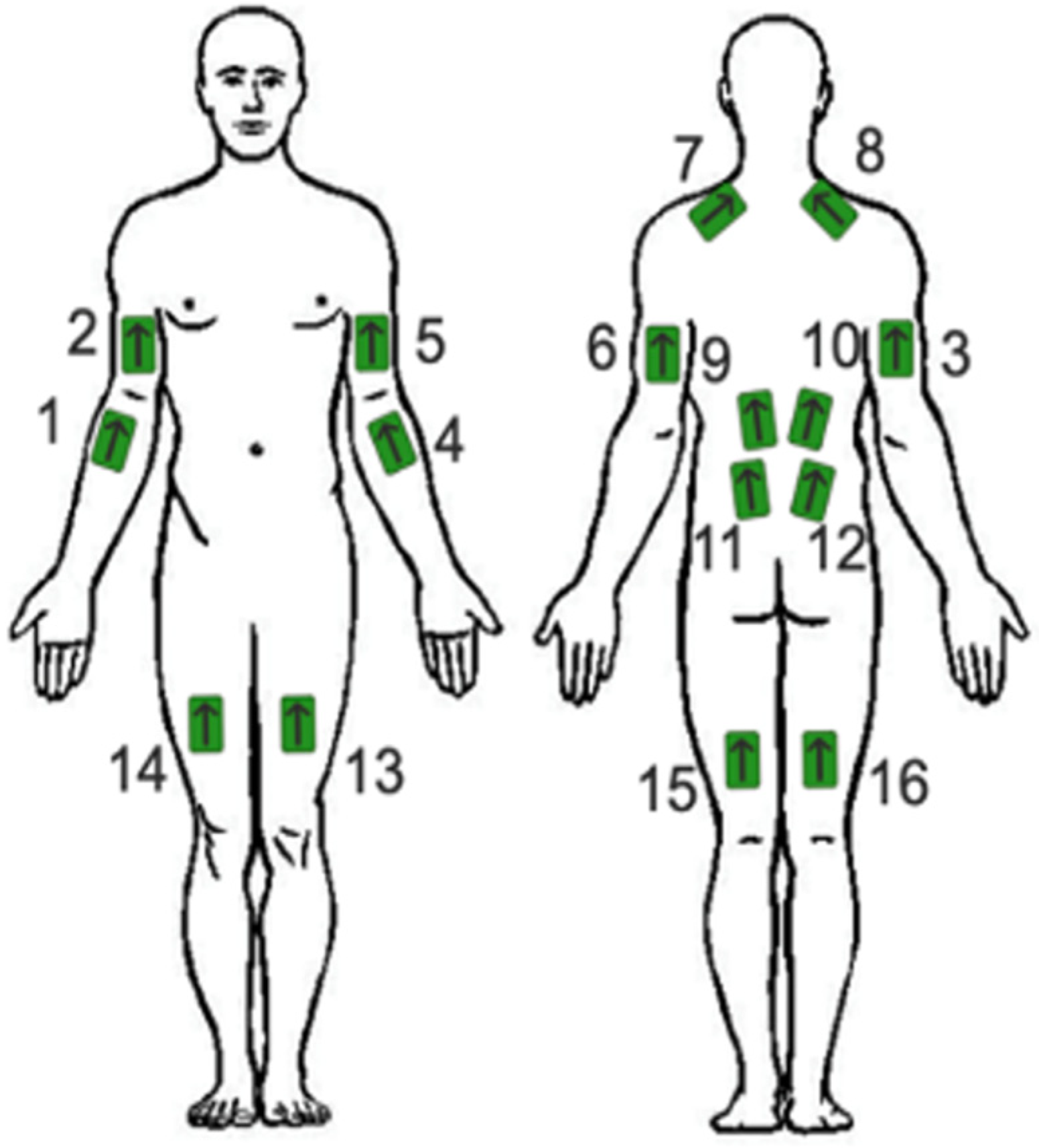
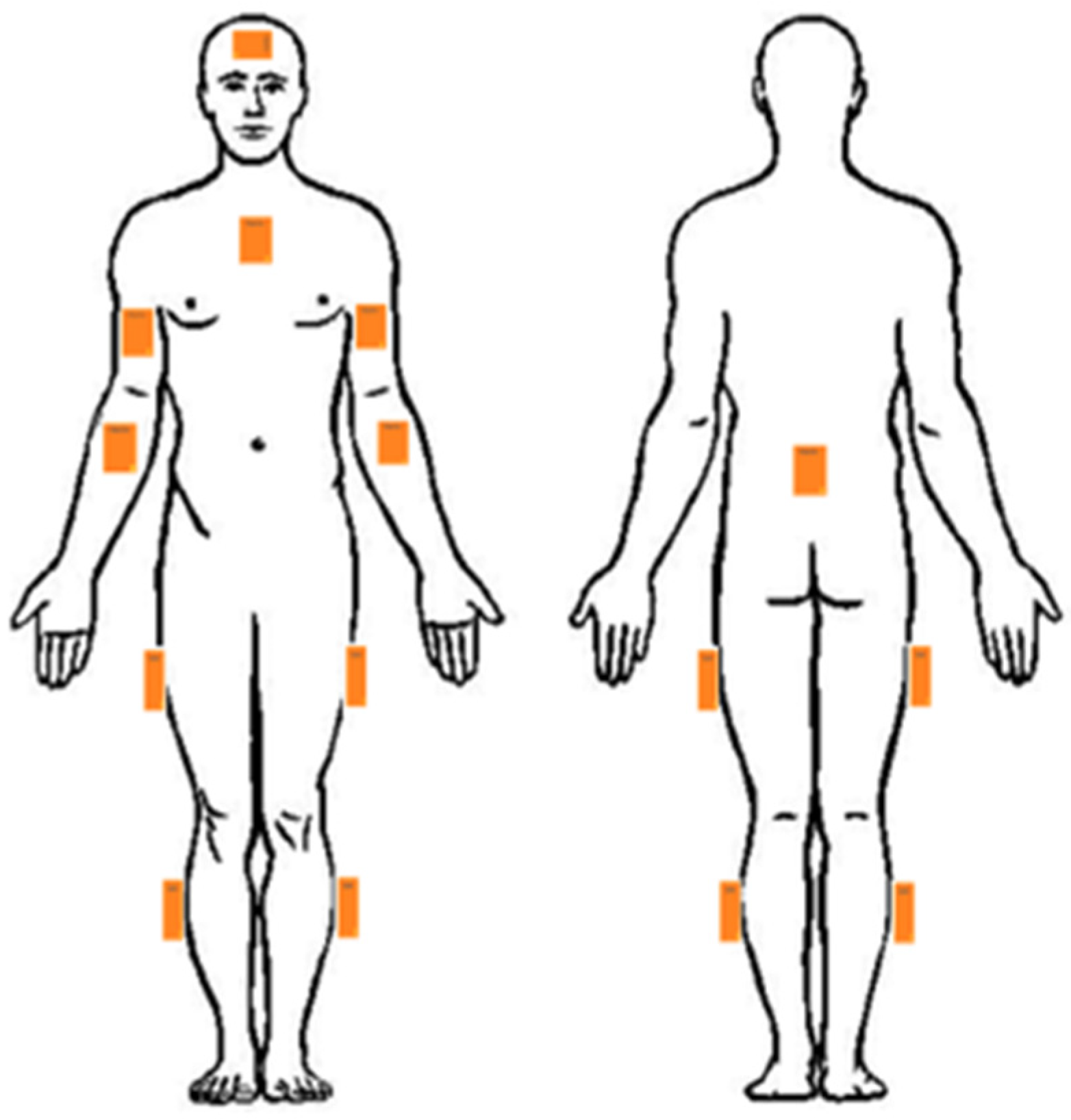
2.3.1. Muscle Activity Data Collection
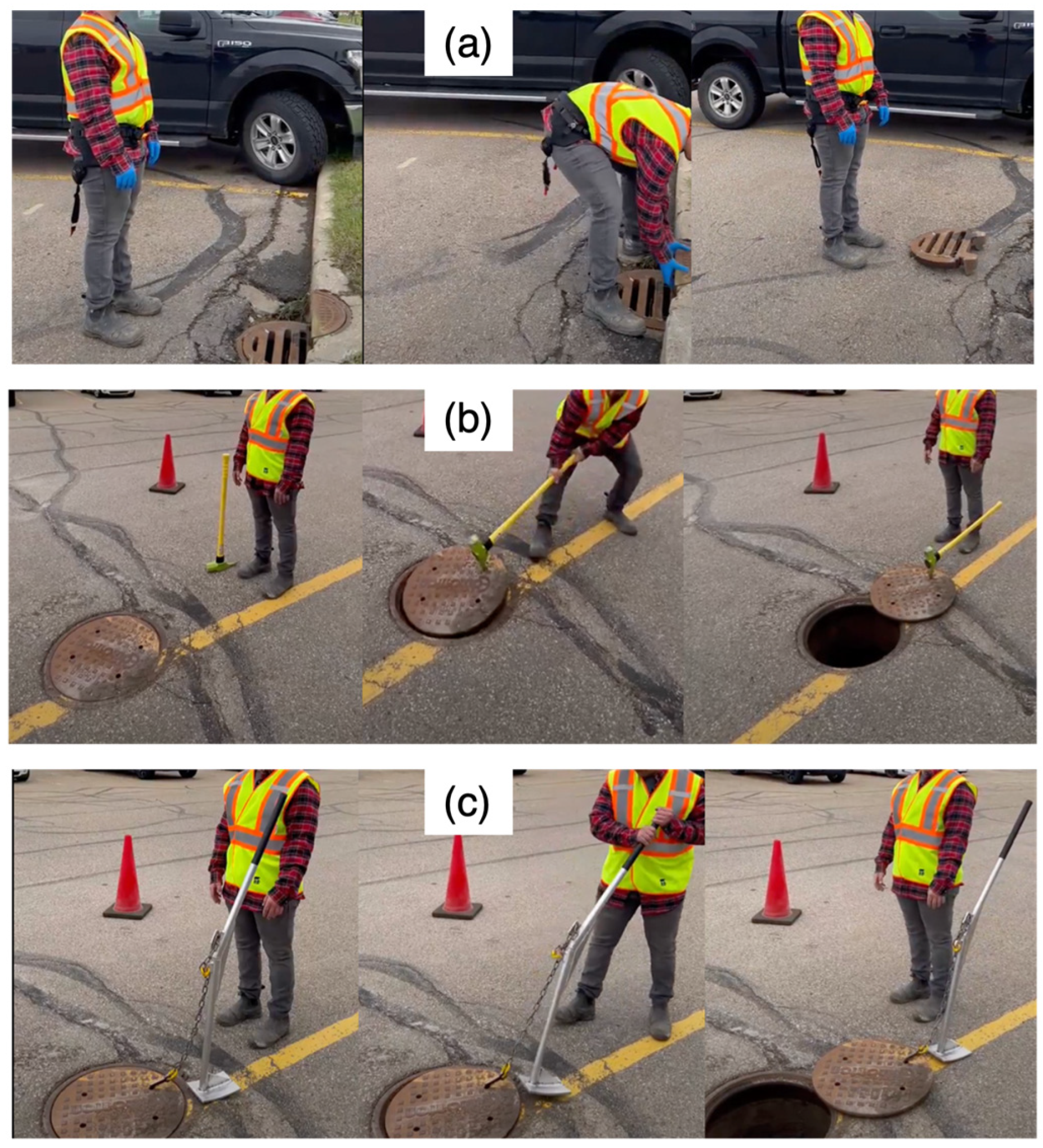
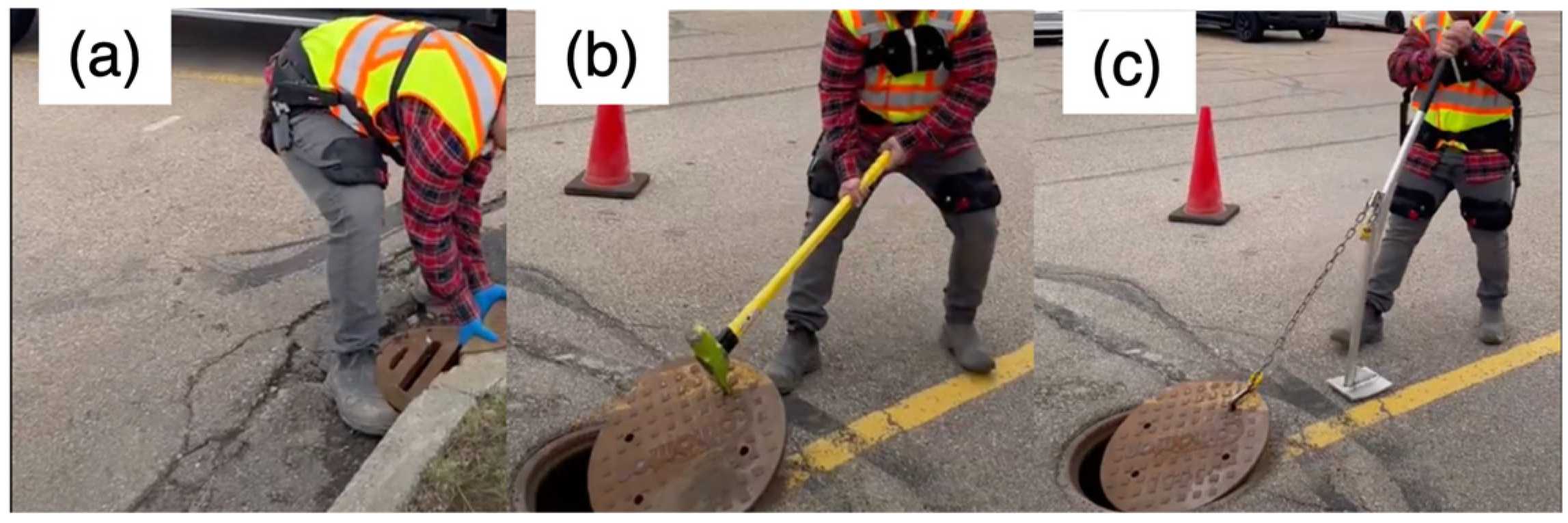
2.3.2. Task Description
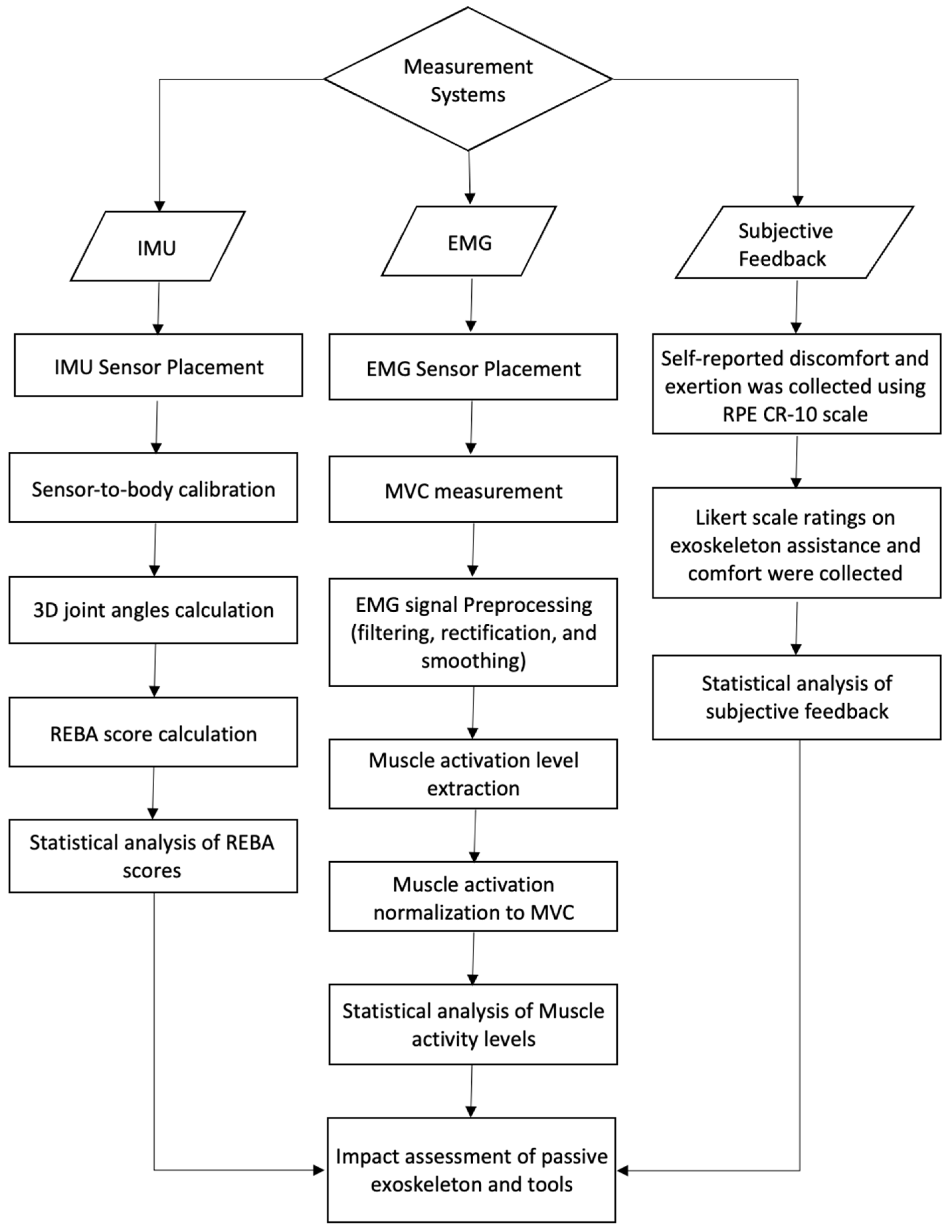
2.4. Measurement and Data Analysis
2.4.1. Muscle Activation Assessment
- The recorded sEMG signal was filtered using a 4th-order band-pass Butterworth filter with cut-off frequencies of 10 Hz and 500 Hz, as recommended by Konrad [20]. To ensure a stable signal baseline, the mean value of the signal was subtracted prior to further analysis.
- Full wave rectification was performed.
- To smooth the rectified signal, a moving average filter with a window length of 500 was applied to the data.
- The baseline error was rechecked and, if needed, eliminated.
- The RMS of the normalized sEMG amplitude was calculated during the working period.
2.4.2. Posture-Based Risk Assessment
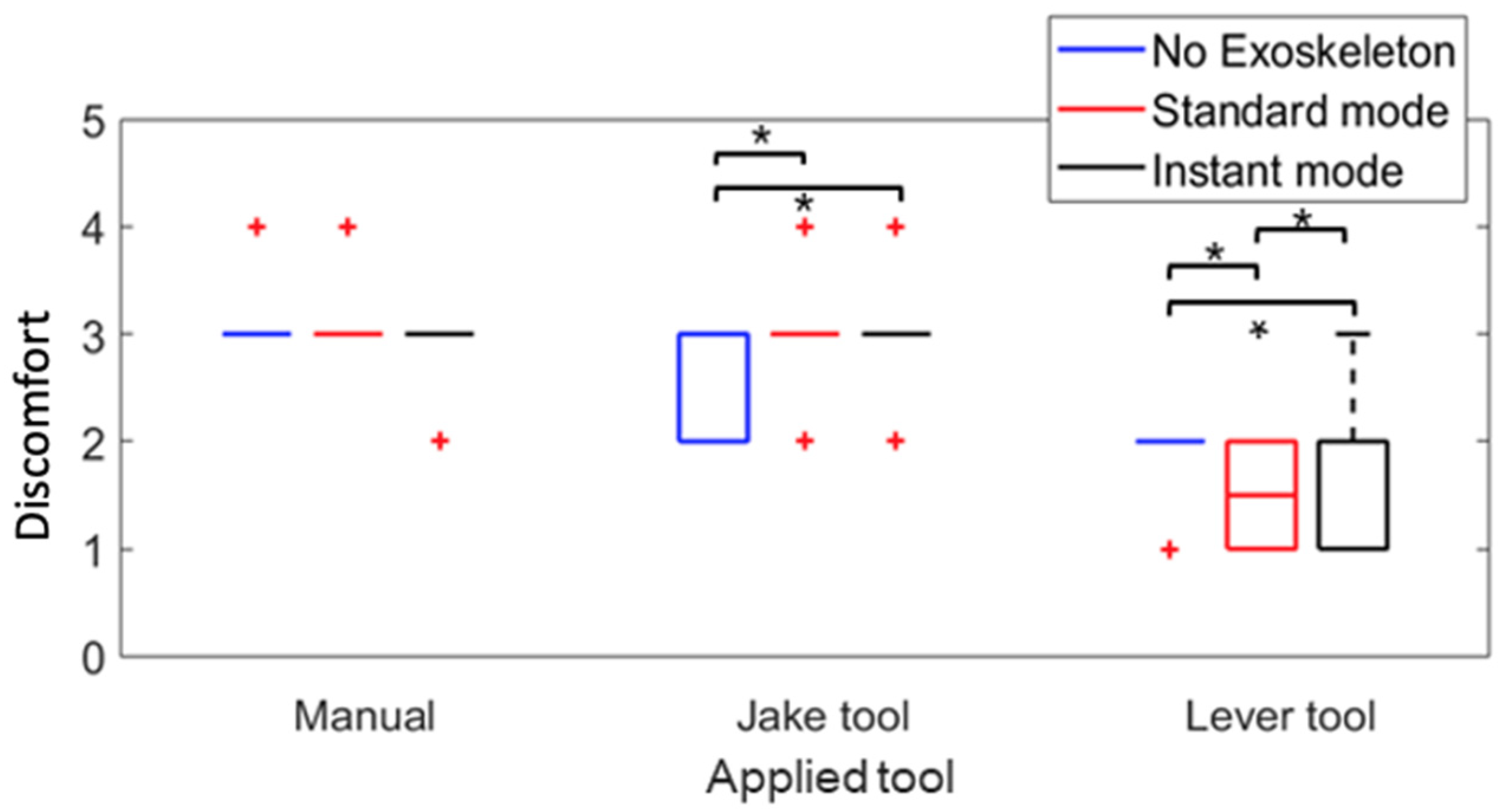
2.4.3. Usability and Wearer Comfort
2.5. Statistical Analysis
3. Results
3.1. Impact of Using the Jake and Lever Tool Without an Exoskeleton on Muscle Activation During Manhole Cover Removal
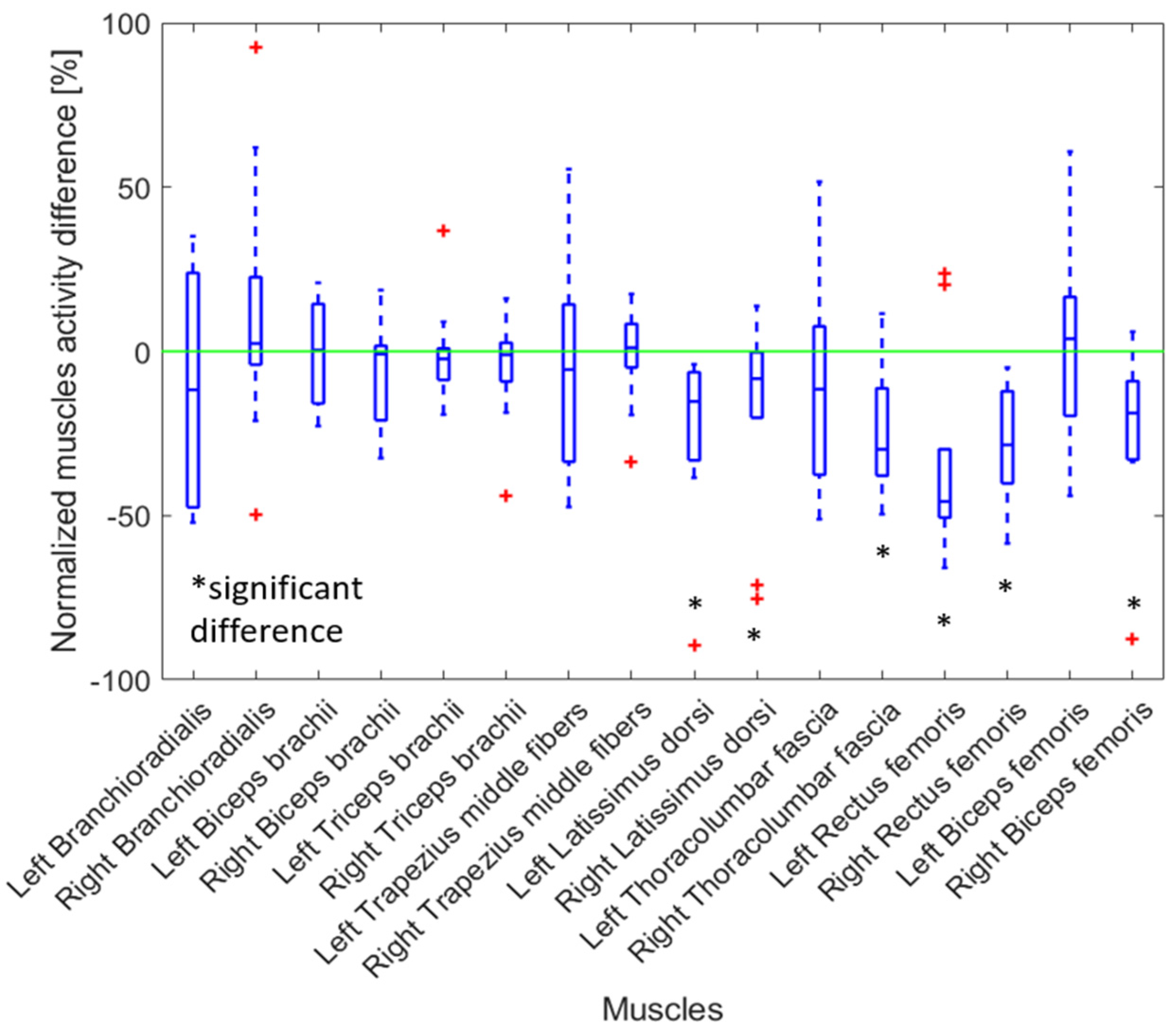
3.2. Impact of Using the Exoskeleton on Muscle Activity During Manhole Cover Removal Manually
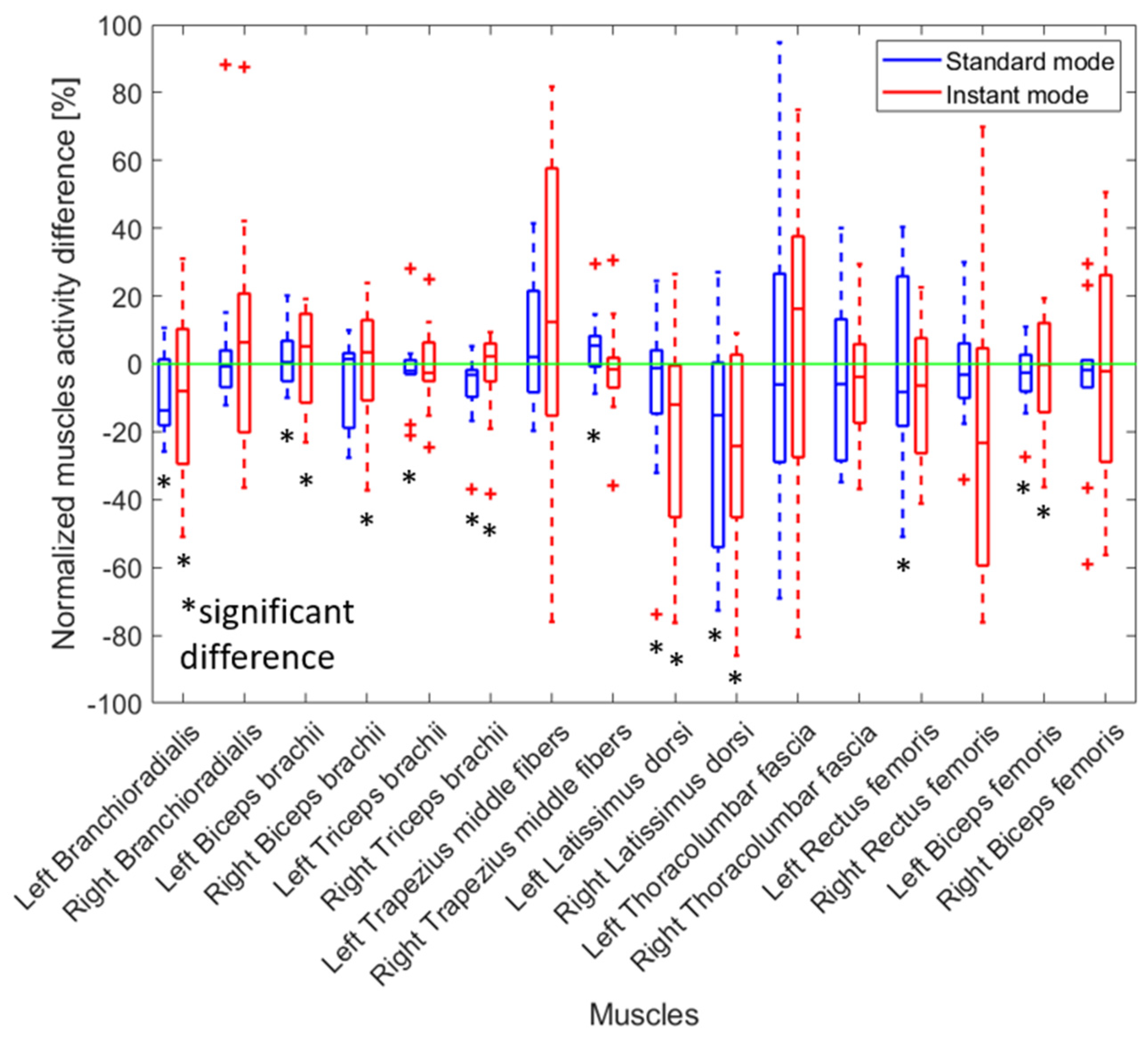
3.3. Impact of Using the Exoskeleton on Muscle Activity When a Jake or Lever Tool Was Used
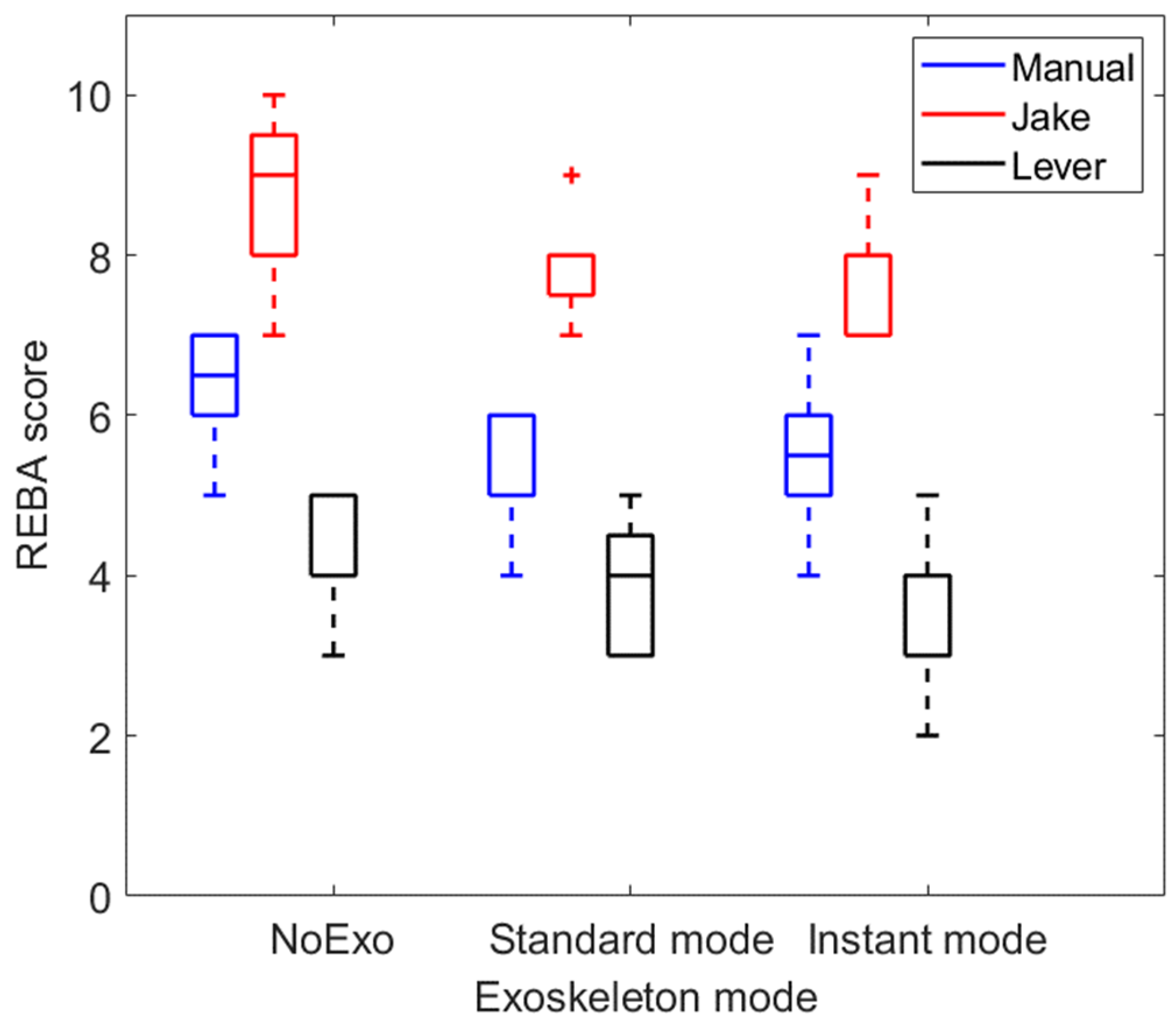
3.4. Impact of Exoskeleton on the Body Posture During Manhole Cover Removal
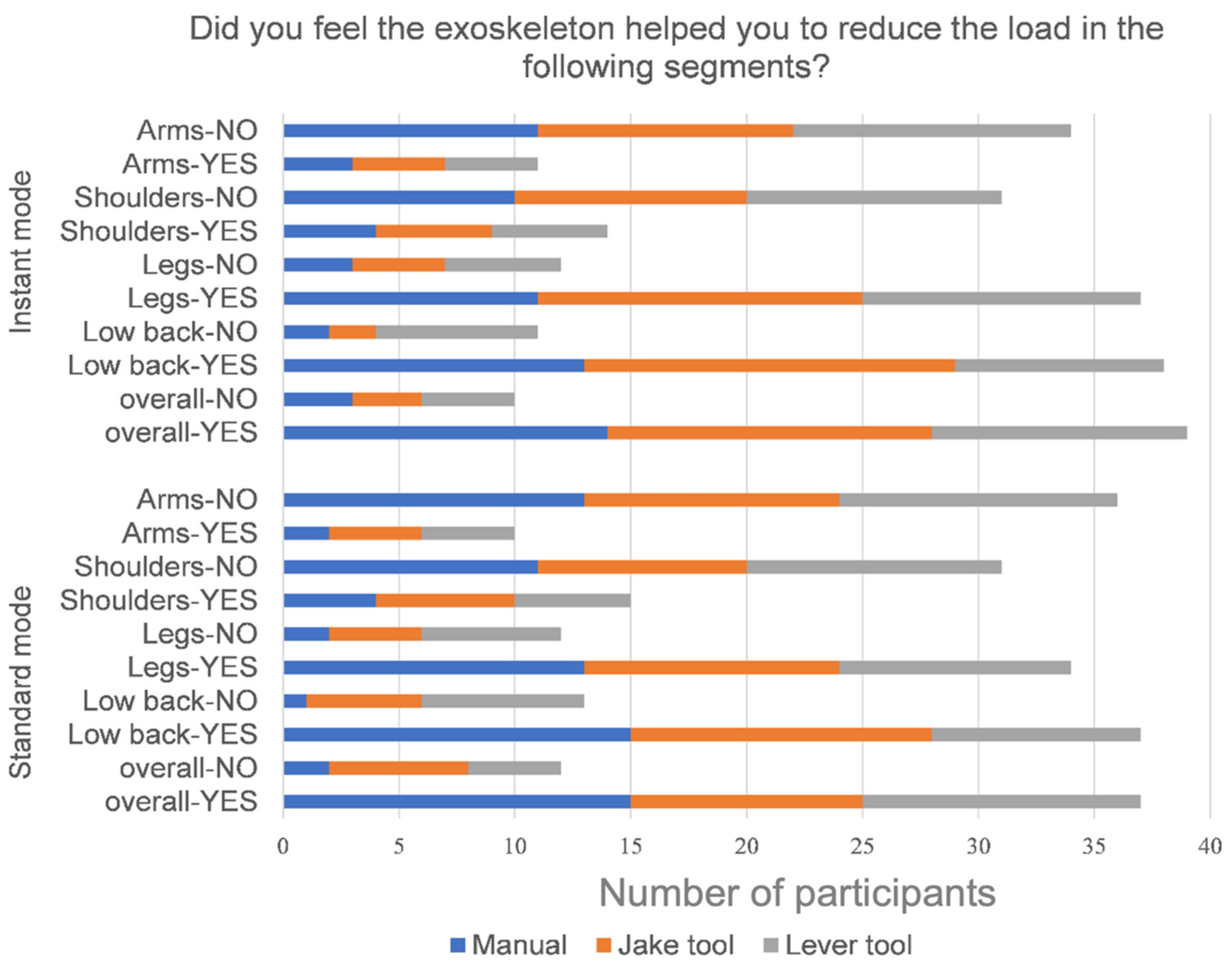
3.5. Questionnaire
4. Discussion
4.1. Comparison with Previous Research and Real-World Applications
4.2. Exoskeleton’s Effect on Removing the Manhole Cover Manually
4.3. Exoskeleton’s Effect on Removing the Manhole Cover Using the Lever Tool
4.4. Exoskeleton’s Effect on Removing the Manhole Cover Using the Jake Tool
4.5. Exoskeleton’s Effect on the User Feedback
4.6. Jake Tool Versus Lever Tool Effect on Removing the Manhole Cover
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, D.; Dai, F.; Ning, X. Risk assessment of work-related musculoskeletal disorders in construction: State-of-the-art review. J. Constr. Eng. Manag. 2015, 141, 04015008. [Google Scholar] [CrossRef]
- Major, M.-E.; Vézina, N. Analysis of worker strategies: A comprehensive understanding for the prevention of work-related musculoskeletal disorders. Int. J. Ind. Ergon. 2015, 48, 149–157. [Google Scholar] [CrossRef]
- Goldenhar, L.M.; Stafford, P. If you’ve seen one construction worksite stretch and flex program you’ve seen one construction worksite stretch and flex program. J. Saf. Res. 2015, 55, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Wami, S.D.; Abere, G.; Dessie, A.; Getachew, D. Work-related risk factors and the prevalence of low back pain among low-wage workers: Results from a cross-sectional study. BMC Public Health 2019, 19, 1072. [Google Scholar] [CrossRef]
- Da Costa, B.R.; Vieira, E.R. Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. Am. J. Ind. Med. 2010, 53, 285–323. [Google Scholar]
- Toxiri, S.; Näf, M.B.; Lazzaroni, M.; Fernández, J.; Sposito, M.; Poliero, T.; Ortiz, J. Back-support exoskeletons for occupational use: An overview of technological advances and trends. IISE Trans. Occup. Ergon. Hum. Factors 2019, 7, 237–249. [Google Scholar] [CrossRef]
- Back Pain in the Workplace. International Association for the Study of Pain (IASP). Available online: https://www.iasp-pain.org/resources/fact-sheets/back-pain-in-the-workplace/ (accessed on 18 December 2024).
- Back Injuries Prominent in Work-Related Musculoskeletal Disorder Cases in 2016: The Economics Daily. U.S. Bureau of Labor Statistics. Available online: https://www.bls.gov/opub/ted/2018/back-injuries-prominent-in-work-related-musculoskeletal-disorder-cases-in-2016.htm (accessed on 18 December 2024).
- Wang, J.; Vasconcelos, J.G. Manhole cover displacement caused by the release of entrapped air pockets. J. Water Manag. Model. 2018, 26, 1–6. [Google Scholar]
- Korhan, O.; Memon, A.A. Introductory chapter: Work-related musculoskeletal disorders. In Work-Related Musculoskeletal Disorders; IntechOpen: London, UK, 2019. [Google Scholar]
- Wai, E.K.; Roffey, D.M.; Bishop, P.; Kwon, B.K.; Dagenais, S. Causal assessment of occupational bending or twisting and low back pain: Results of a systematic review. Spine J. 2010, 10, 76–88. [Google Scholar] [CrossRef]
- Koopman, A.S.; Kingma, I.; Faber, G.S.; de Looze, M.P.; van Dieën, J.H. Effects of a passive exoskeleton on the mechanical loading of the low back in static holding tasks. J. Biomech. 2019, 83, 97–103. [Google Scholar] [CrossRef]
- Bogue, R. Exoskeletons–a review of industrial applications. Ind. Robot. 2018, 45, 585–590. [Google Scholar] [CrossRef]
- De Looze, M.P.; Bosch, T.; Krause, F.; Stadler, K.S.; O’Sullivan, L.W. Exoskeletons for industrial application and their potential effects on physical workload. Ergonomics 2016, 59, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Huysamen, K.; Bosch, T.; de Looze, M.; Stadler, K.S.; Graf, E.; O’Sullivan, L.W. Evaluation of a passive exoskeleton for static upper limb activities. Appl. Ergon. 2018, 70, 148–155. [Google Scholar] [CrossRef]
- Bosch, T.; van Eck, J.; Knitel, K.; de Looze, M. The effects of a passive exoskeleton on muscle activity, discomfort and endurance time in forward bending work. Appl. Ergon. 2016, 54, 212–217. [Google Scholar] [PubMed]
- Agrawal, S.K.; Fattah, A.; Bogue, R. A gravity balancing passive exoskeleton for the human leg. In Proceedings of the IEEE Conference on Robotics, Philadelphia, PA, USA, 16–19 August 2006; Volume 302. [Google Scholar]
- Theurel, J.; Desbrosses, K. Occupational exoskeletons: Overview of their benefits and limitations in preventing work-related musculoskeletal disorders. IISE Trans. Occup. Ergon. Hum. Factors 2019, 7, 264–280. [Google Scholar] [CrossRef]
- Shakourisalim, M.; Wang, X.; Beltran Martinez, K.; Golabchi, A.; Krell, S.; Tavakoli, M.; Rouhani, H. A Comparative Study of Biomechanical Assessments in Laboratory and Field Settings for Manual Material Handling Tasks Using Extractor Tools and Exoskeletons. Front. Bioeng. Biotechnol. 2024, 12, 1358670. [Google Scholar] [CrossRef] [PubMed]
- Konrad, P. The ABC of EMG. In A Practical Introduction to Kinesiological Electromyography; Noraxon INC: Scottsdale, AZ, USA, 2005; Available online: https://hermanwallace.com/download/The_ABC_of_EMG_by_Peter_Konrad.pdf (accessed on 18 December 2024).
- Wang, X.; Beltran Martinez, K.; Golabchi, A.; Tavakoli, M.; Rouhani, H. A Dynamic Procedure to Detect Maximum Voluntary Contractions in Low Back. Sensors 2023, 23, 4999. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Hägg, G.; Stegeman, D.F.; Blok, J.; Rau, G.; Disselhorst-Klug, C. SENIAM 8: European Recommendations for Surface ElectroMyoGraphy; Roessingh Research and Development: Enschede, The Netherlands, 1999; ISBN 90-75452-15. [Google Scholar]
- Hignett, S.; McAtamney, L. Rapid entire body assessment (REBA). Appl. Ergon. 2000, 31, 201–205. [Google Scholar] [CrossRef]
- Humadi, A.; Nazarahari, M.; Ahmad, R.; Rouhani, H. In-field instrumented ergonomic risk assessment: Inertial measurement units versus Kinect V2. Int. J. Ind. Ergon. 2021, 84, 103147. [Google Scholar]
- Martinez, K.B.; Nazarahari, M.; Rouhani, H. K-score: A novel scoring system to quantify fatigue-related ergonomic risk based on joint angle measurements via wearable inertial measurement units. Appl. Ergon. 2022, 102, 103757. [Google Scholar]
- Nazarahari, M.; Noamani, A.; Ahmadian, N.; Rouhani, H. Sensor-to-body calibration procedure for clinical motion analysis of lower limb using magnetic and inertial measurement units. J. Biomech. 2019, 85, 224–229. [Google Scholar] [CrossRef]
- Nazarahari, M.; Rouhani, H. Semi-automatic sensor-to-body calibration of inertial sensors on lower limb using gait recording. IEEE Sens. J. 2019, 19, 12465–12474. [Google Scholar]
- Humadi, A.; Nazarahari, M.; Ahmad, R.; Rouhani, H. Instrumented ergonomic risk assessment using wearable inertial measurement units: Impact of joint angle convention. IEEE Access 2020, 9, 7293–7305. [Google Scholar]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- RPE-Scale Innovative Physical Therapy Solutions in Motion. Available online: https://innovativept.net/beginners-resistance-training/rpe-scale/ (accessed on 18 December 2024).
- Wilcoxon, F. Individual comparisons by ranking methods. In Breakthroughs in Statistics: Methodology and Distribution; Springer: Berlin/Heidelberg, Germany, 1992; pp. 196–202. [Google Scholar]
- Schwartz, M.; Desbrosses, K.; Theurel, J.; Mornieux, G. Biomechanical consequences of using passive and active back-support exoskeletons during different manual handling tasks. Int. J. Environ. Res. Public Health 2023, 20, 6468. [Google Scholar] [CrossRef] [PubMed]
- Govaerts, R.; De Bock, S.; Provyn, S.; Vanderborght, B.; Roelands, B.; Meeusen, R.; De Pauw, K. The impact of an active and passive industrial back exoskeleton on functional performance. Ergonomics 2024, 67, 597–618. [Google Scholar] [CrossRef]
- Ahn, J.; Jung, H.; Moon, J.; Kwon, C.; Ahn, J. A comprehensive assessment of a passive back support exoskeleton for load handling assistance. Sci. Rep. 2025, 15, 3926. [Google Scholar]
- Baltrusch, S.J.; Houdijk, H.; Van Dieën, J.H.; Kruif, J.T.C. Passive trunk exoskeleton acceptability and effects on self-efficacy in employees with low-back pain: A mixed method approach. J. Occup. Rehabil. 2021, 31, 129–141. [Google Scholar]
- Kozinc, Ž.; Baltrusch, S.; Houdijk, H.; Šarabon, N. Short-term effects of a passive spinal exoskeleton on functional performance, discomfort, and user satisfaction in patients with low back pain. J. Occup. Rehabil. 2021, 31, 142–152. [Google Scholar] [PubMed]
- Grazi, L.; Trigili, E.; Proface, G.; Giovacchini, F.; Crea, S.; Vitiello, N. Design and experimental evaluation of a semi-passive upper-limb exoskeleton for workers with motorized tuning of assistance. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 2276–2285. [Google Scholar]
- Luger, T.; Seibt, R.; Cobb, T.J.; Rieger, M.A.; Steinhilber, B. Influence of a passive lower-limb exoskeleton during simulated industrial work tasks on physical load, upper body posture, postural control, and discomfort. Appl. Ergon. 2019, 80, 152–160. [Google Scholar]
- Golabchi, A.; Chao, A.; Tavakoli, M. A systematic review of industrial exoskeletons for injury prevention: Efficacy evaluation metrics, target tasks, and supported body postures. Sensors 2022, 22, 2714. [Google Scholar] [CrossRef]
- Bonakdar, A.; Houshmand, S.; Martinez, K.B.; Golabchi, A.; Tavakoli, M.; Rouhani, H. Fatigue assessment in multi-activity manual handling tasks through joint angle monitoring with wearable sensors. Biomed. Signal Process. Control 2025, 102, 107398. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trial | Tool | Exoskeleton Mode | Cover Weight |
|---|---|---|---|
| 1 | Manual | Without exoskeleton | 18.1 kg (40 lbs.) |
| 2 | Instant mode | 18.1 kg (40 lbs.) | |
| 3 | Standard mode | 18.1 kg (40 lbs.) | |
| 4 | Jake | Without exoskeleton | 56.7 kg (125 lbs.) |
| 5 | Instant mode | 56.7 kg (125 lbs.) | |
| 6 | Standard mode | 56.7 kg (125 lbs.) | |
| 7 | Lever | Without exoskeleton | 56.7 kg (125 lbs.) |
| 8 | Instant mode | 56.7 kg (125 lbs.) | |
| 9 | Standard mode | 56.7 kg (125 lbs.) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Golabchi, A.; Shakourisalim, M.; Beltran Martinez, K.; Estaji, Z.; Krell, S.; Tavakoli, M.; Rouhani, H. Assessing Effectiveness of Passive Exoskeletons and Tool Selection on Ergonomic Safety in Manhole Cover Removal. Sensors 2025, 25, 2027. https://doi.org/10.3390/s25072027
Wang X, Golabchi A, Shakourisalim M, Beltran Martinez K, Estaji Z, Krell S, Tavakoli M, Rouhani H. Assessing Effectiveness of Passive Exoskeletons and Tool Selection on Ergonomic Safety in Manhole Cover Removal. Sensors. 2025; 25(7):2027. https://doi.org/10.3390/s25072027
Chicago/Turabian StyleWang, Xun, Ali Golabchi, Maryam Shakourisalim, Karla Beltran Martinez, Zeinab Estaji, Sarah Krell, Mahdi Tavakoli, and Hossein Rouhani. 2025. "Assessing Effectiveness of Passive Exoskeletons and Tool Selection on Ergonomic Safety in Manhole Cover Removal" Sensors 25, no. 7: 2027. https://doi.org/10.3390/s25072027
APA StyleWang, X., Golabchi, A., Shakourisalim, M., Beltran Martinez, K., Estaji, Z., Krell, S., Tavakoli, M., & Rouhani, H. (2025). Assessing Effectiveness of Passive Exoskeletons and Tool Selection on Ergonomic Safety in Manhole Cover Removal. Sensors, 25(7), 2027. https://doi.org/10.3390/s25072027