


The Effects of Decreasing Foot Strike Angle on Lower Extremity Shock Attenuation Measured with Wearable Sensors

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
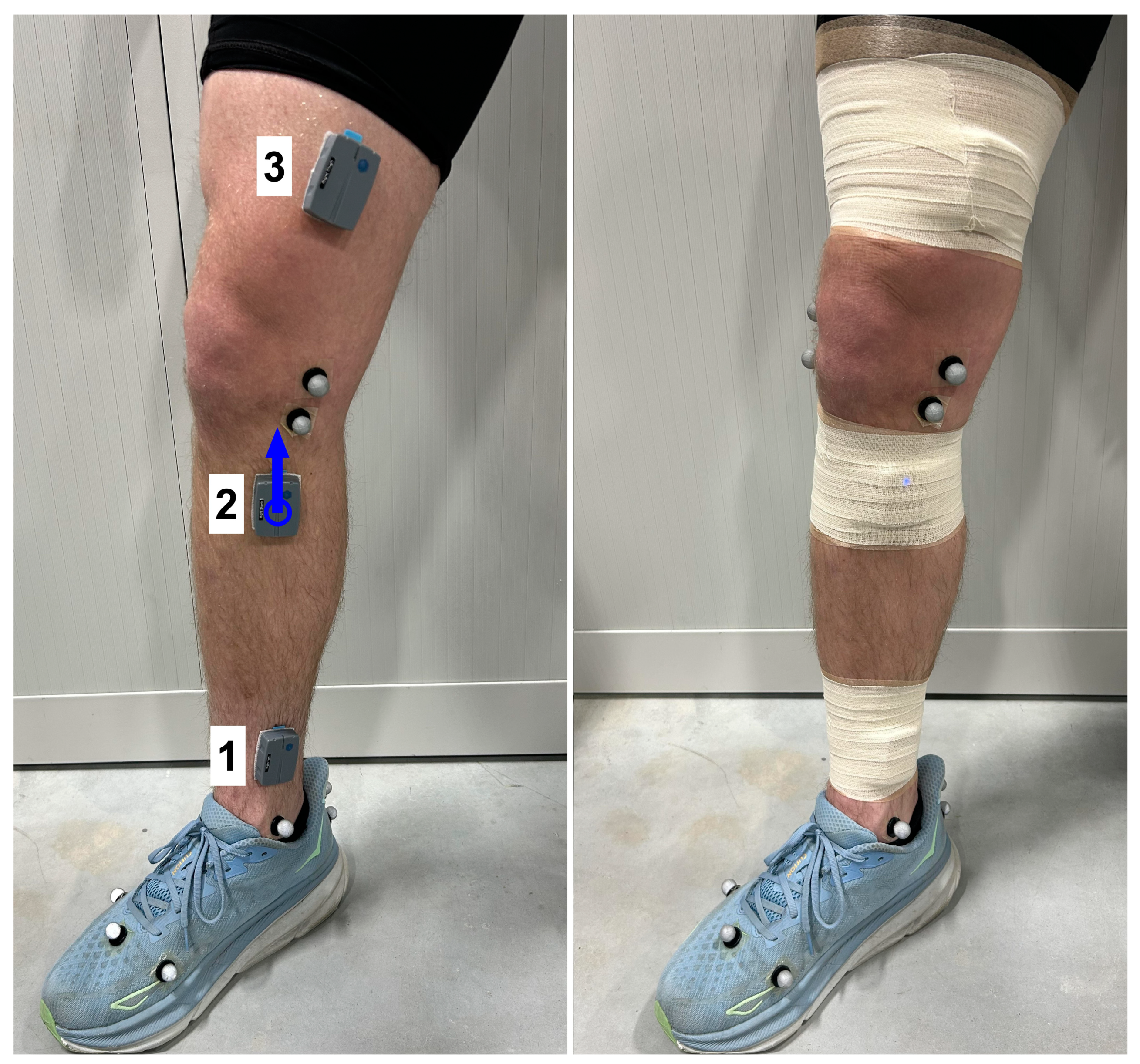
2.2. Procedures
2.3. Data Reduction and Analysis
3. Results
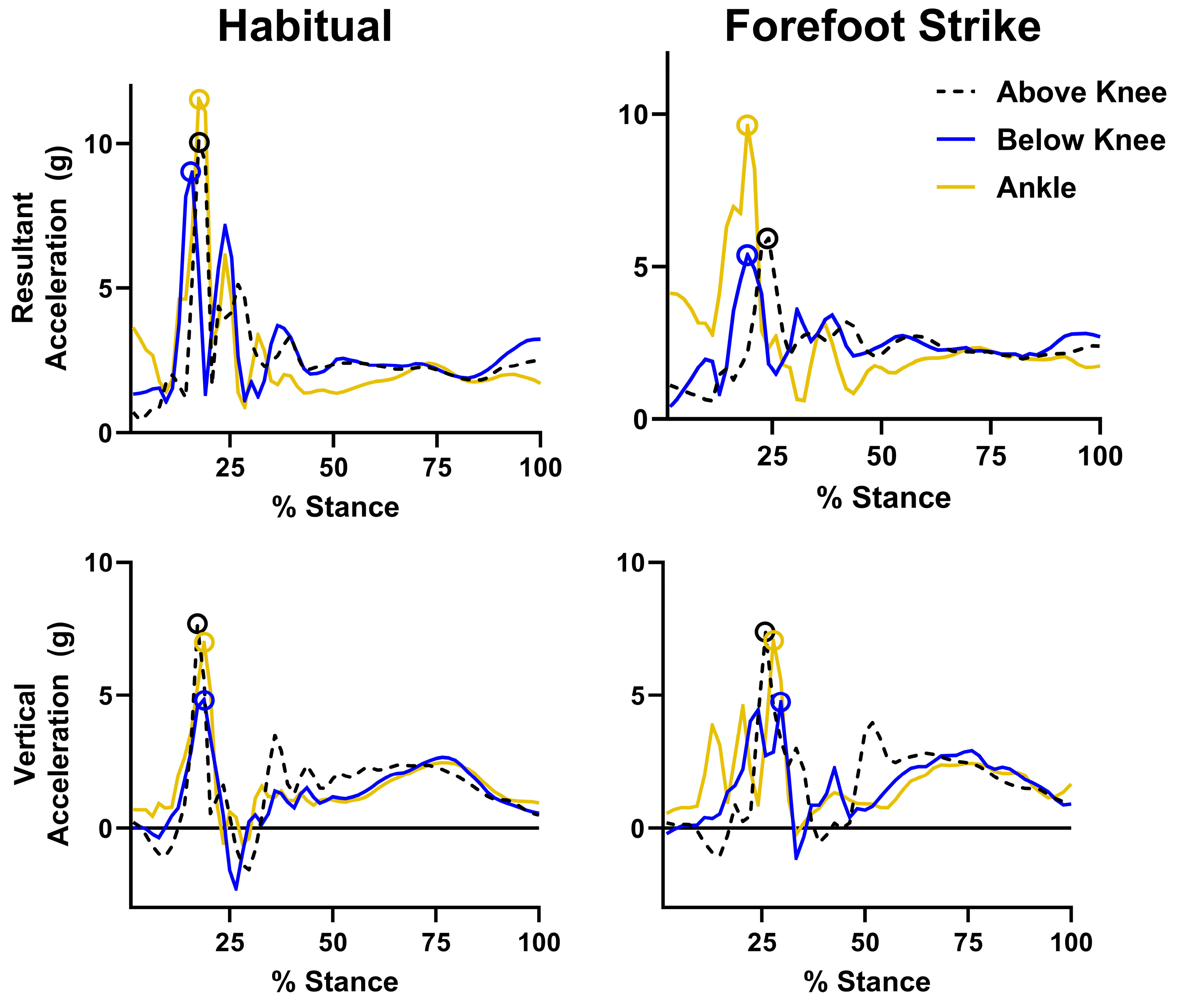
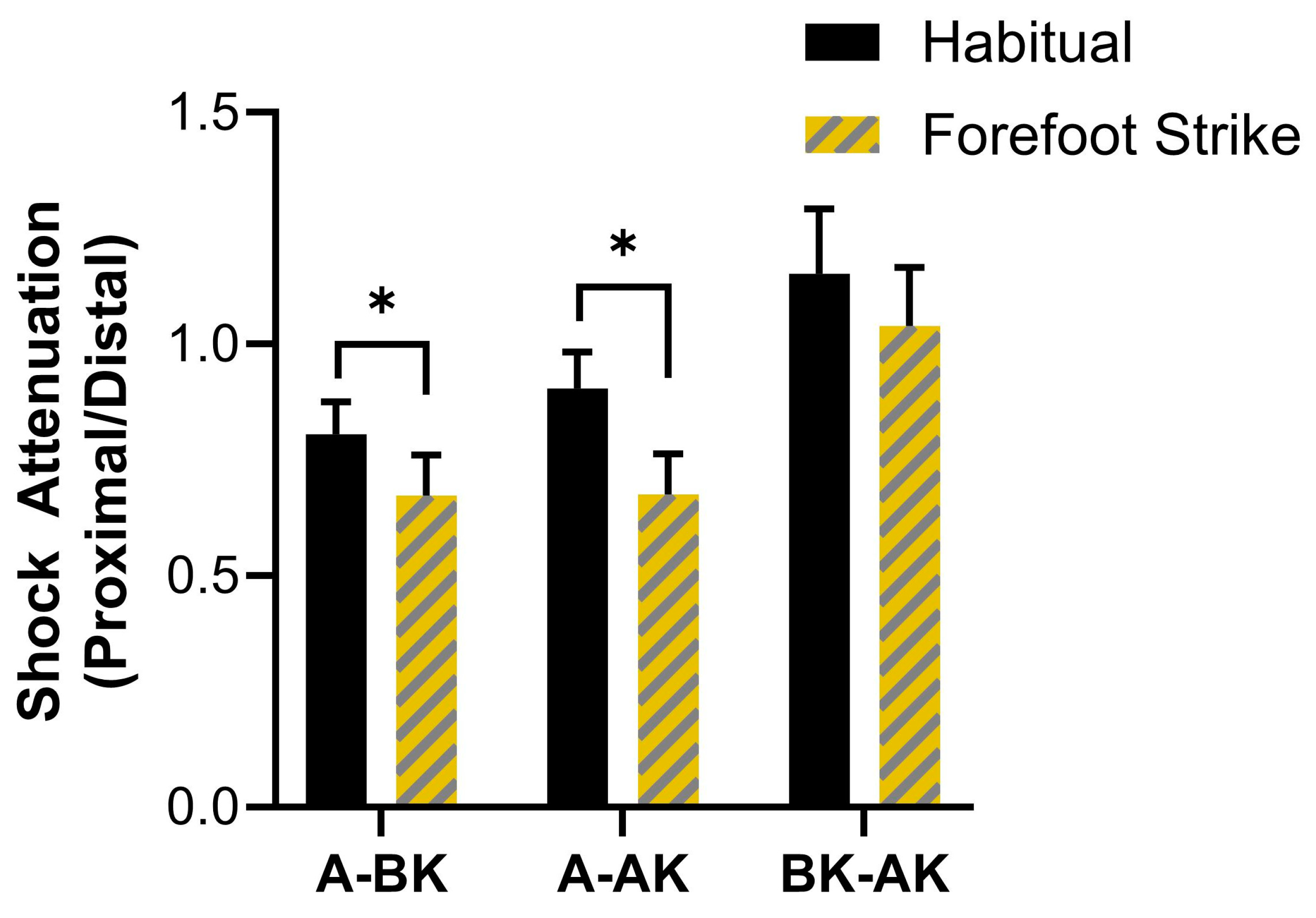
3.1. Resultant Acceleration Results
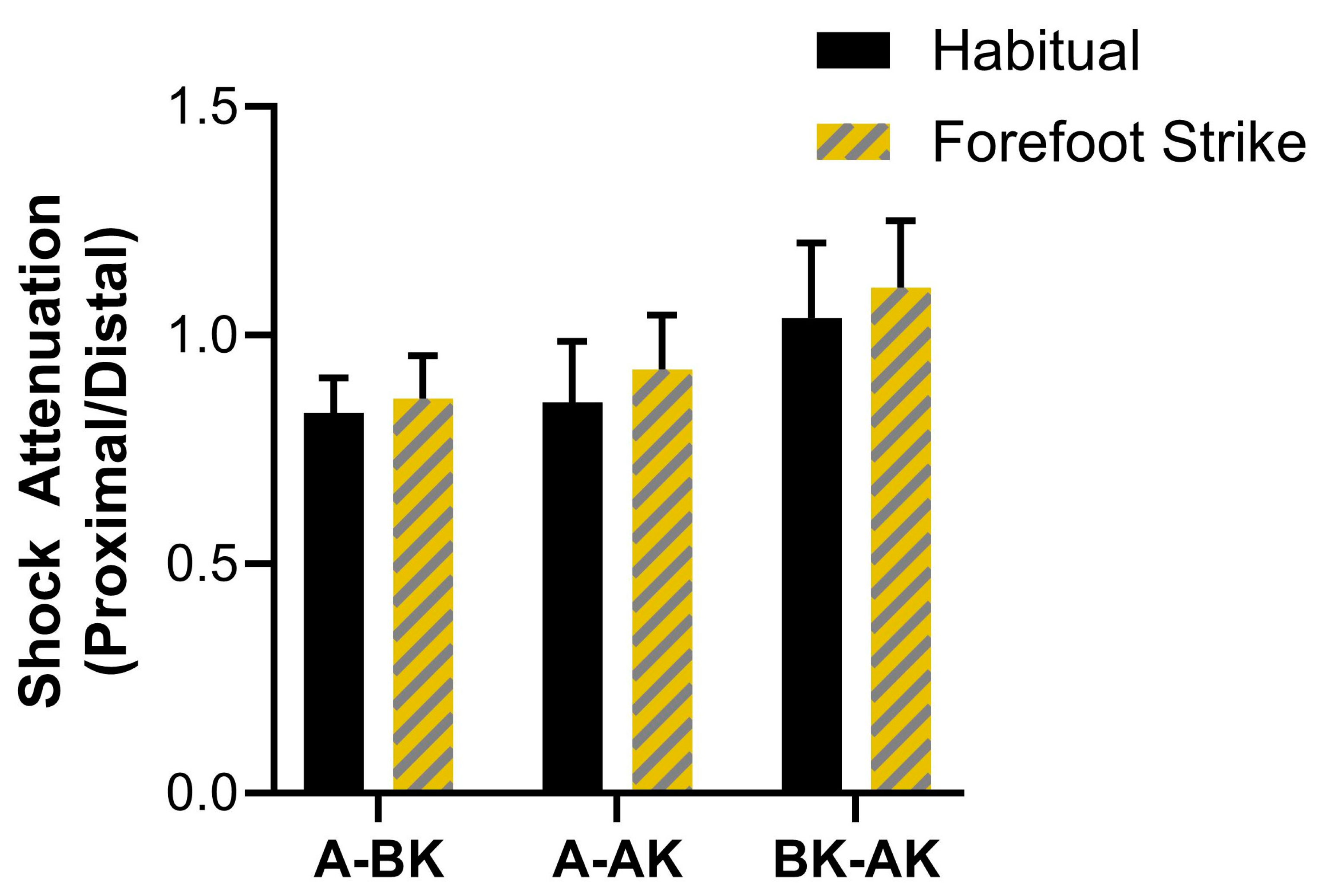
3.2. Vertical Acceleration Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AK/A | Above knee/ankle |
| BK/A | Below knee/ankle |
| AK/BK | Above knee/below knee |
| GRF | Ground reaction force |
| IMU | Inertial measurement unit |
| MSKI | Musculoskeletal injury |
References
- Fields, K.B. Running Injuries-Changing Trends and Demographics. Curr. Sports Med. Rep. 2011, 10, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Francis, P.; Whatman, C.; Sheerin, K.; Hume, P.; Johnson, M.I. The proportion of lower limb running injuries by gender, anatomical location and specific pathology: A systematic review. J. Sports Sci. Med. 2019, 18, 21. [Google Scholar]
- Cowan, D.N.; Jones, B.H.; Shaffer, R.A. Musculoskeletal injuries in the military training environment. In Military Preventative Medicine: Mobilization and Deployment; Department of the Army, Office of the Surgeon General: Washington, DC, USA, 2003; pp. 195–210. [Google Scholar]
- Jones, B.H.; Cowan, D.N.; Tomlinson, J.P.; Robinson, J.R.; Polly, D.W.; Frykman, P.N. Epidemiology of injuries associated with physical training among young men in the army. Med. Sci. Sports Exerc. 1993, 25, 197–203. [Google Scholar] [CrossRef]
- Hauschild, V.D.; Barnes, S.; Hauret, K.; Lee, T.; Forrest, L.; Jones, B.H. The Etiology of Injuries in US Army Initial Entry Training. US Army Med. Dep. J. 2018, 2-18, 22–29. [Google Scholar]
- Kaufman, K.R.; Brodine, S.; Shaffer, R. Military training-related injuries: Surveillance, research, and prevention. Am. J. Prev. Med. 2000, 18 (Suppl. 3), 54–63. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.H.; Hauschild, V.D. Physical training, fitness, and injuries: Lessons learned from military studies. J. Strength Cond. Res. 2015, 29 (Suppl. 11), S57–S64. [Google Scholar] [CrossRef]
- Johnson, C.D.; Tenforde, A.S.; Outerleys, J.; Reilly, J.; Davis, I.S. Impact-related ground reaction forces are more strongly associated with some running injuries than others. Am. J. Sports Med. 2020, 48, 3072–3080. [Google Scholar] [CrossRef]
- Davis, I.S.; Bowser, B.J.; Mullineaux, D.R. Greater vertical impact loading in female runners with medically diagnosed injuries: A prospective investigation. Br. J. Sports Med. 2016, 50, 887–892. [Google Scholar] [CrossRef]
- Messier, S.P.; Martin, D.F.; Mihalko, S.L.; Ip, E.; DeVita, P.; Cannon, D.W.; Love, M.; Beringer, D.; Saldana, S.; Fellin, R.E. A 2-year prospective cohort study of overuse running injuries: The runners and injury longitudinal study (TRAILS). Am. J. Sports Med. 2018, 46, 2211–2221. [Google Scholar] [CrossRef]
- Dudley, R.I.; Pamukoff, D.N.; Lynn, S.K.; Kersey, R.D.; Noffal, G.J. A prospective comparison of lower extremity kinematics and kinetics between injured and non-injured collegiate cross country runners. Hum. Mov. Sci. 2017, 52, 197–202. [Google Scholar] [CrossRef]
- Futrell, E.E.; Gross, K.D.; Reisman, D.; Mullineaux, D.R.; Davis, I.S. Transition to forefoot strike reduces load rates more effectively than altered cadence. J. Sport. Health Sci. 2020, 9, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Kleindienst, F.; Campe, S.; Graf, E.; Michel, K.; Witte, K. Differences between fore-and rearfoot strike running patterns based on kinetics and kinematics. In Proceedings of the International Society of Biomechanics in Sport, Ouro Preto, Brazil, 23–27 August 2007. [Google Scholar]
- Stearne, S.M.; Alderson, J.A.; Green, B.A.; Donnelly, C.J.; Rubenson, J. Joint kinetics in rearfoot versus forefoot running: Implications of switching technique. Med. Sci. Sports Exerc. 2014, 46, 1578–1587. [Google Scholar] [CrossRef]
- Kulmala, J.-P.; Avela, J.; Pasanen, K.; Parkkari, J. Forefoot strikers exhibit lower running-induced knee loading than rearfoot strikers. Med. Sci. Sports Exerc. 2013, 45, 2306–2313. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, A.F.; Nakagawa, T.H.; Serrão, F.V.; Ferber, R. Patellofemoral joint stress measured across three different running techniques. Gait Posture 2019, 68, 37–43. [Google Scholar] [CrossRef]
- de Almeida, M.O.; Saragiotto, B.T.; Yamato, T.P.; Lopes, A.D. Is the rearfoot pattern the most frequently foot strike pattern among recreational shod distance runners? Phys. Ther. Sport. 2015, 16, 29–33. [Google Scholar] [CrossRef]
- Warr, B.J.; Fellin, R.E.; Sauer, S.G.; Goss, D.L.; Frykman, P.N.; Seay, J.F. Characterization of foot-strike patterns: Lack of an association with injuries or performance in soldiers. Mil. Med. 2015, 180, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Hamill, J.; Derrick, T.R.; Holt, K.G. Shock attenuation and stride frequency during running. Hum. Mov. Sci. 1995, 14, 45–60. [Google Scholar] [CrossRef]
- Xiang, L.; Gu, Y.; Rong, M.; Gao, Z.; Yang, T.; Wang, A.; Shim, V.; Fernandez, J. Shock acceleration and attenuation during running with minimalist and maximalist shoes: A time-and frequency-domain analysis of tibial acceleration. Bioengineering 2022, 9, 322. [Google Scholar] [CrossRef]
- Mercer, J.A.; Devita, P.; Derrick, T.R.; Bates, B.T. Individual Effects of Stride Length and Frequency on Shock Attenuation during Running. Med. Sci. Sports Exerc. 2003, 35, 307–313. [Google Scholar] [CrossRef]
- Gruber, A.H.; Boyer, K.A.; Derrick, T.R.; Hamill, J. Impact shock frequency components and attenuation in rearfoot and forefoot running. J. Sport. Health Sci. 2014, 3, 113–121. [Google Scholar] [CrossRef]
- ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2018; p. 472.
- Johnson, C.D.; Davis, I.S. What differentiates rearfoot strike runners with low and high vertical load rates? Gait Posture 2022, 96, 149–153. [Google Scholar] [CrossRef]
- Cain, S.M.; McGinnis, R.S.; Davidson, S.P.; Vitali, R.V.; Perkins, N.C.; McLean, S.G. Quantifying performance and effects of load carriage during a challenging balancing task using an array of wireless inertial sensors. Gait Posture 2016, 43, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Bradach, M.M.; Gaudette, L.W.; Tenforde, A.S.; Outerleys, J.; de Souza Júnior, J.R.; Johnson, C.D. The effects of a simple sensor reorientation procedure on peak tibial accelerations during running and correlations with ground reaction forces. Sensors 2023, 23, 6048. [Google Scholar] [CrossRef] [PubMed]
- Napier, C.; MacLean, C.L.; Maurer, J.; Taunton, J.E.; Hunt, M.A. Kinetic Risk Factors of Running-Related Injuries in Female Recreational Runners. Scand. J. Med. Sci. Sports 2018, 28, 2164–2172. [Google Scholar] [CrossRef] [PubMed]
- Bredeweg, S.W.; Kluitenberg, B.; Bessem, B.; Buist, I. Differences in kinetic variables between injured and noninjured novice runners: A prospective cohort study. J. Sci. Med. Sports 2013, 16, 205–210. [Google Scholar] [CrossRef]
- Van den Berghe, P.; Six, J.; Gerlo, J.; Leman, M.; De Clercq, D. Validity and reliability of peak tibial accelerations as real-time measure of impact loading during over-ground rearfoot running at different speeds. J. Biomech. 2019, 86, 238–242. [Google Scholar] [CrossRef]
- Diss, C.E. The reliability of kinetic and kinematic variables used to analyse normal running gait. Gait Posture 2001, 14, 98–103. [Google Scholar] [CrossRef]
- Altman, A.R.; Davis, I.S. A kinematic method for footstrike pattern detection in barefoot and shod runners. Gait Posture 2012, 35, 298–300. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavior Science, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Napier, C.; Fridman, L.; Blazey, P.; Tran, N.; Michie, T.V.; Schneeberg, A. Differences in peak impact accelerations among foot strike patterns in recreational runners. Front. Sports Act. Living 2022, 4, 802019. [Google Scholar] [CrossRef]
- Johnson, C.D.; Outerleys, J.; Tenforde, A.S.; Davis, I.S. A comparison of attachment methods of skin mounted inertial measurement units on tibial accelerations. J. Biomech. 2020, 113, 110118. [Google Scholar] [CrossRef]
- Mercer, J.A.; Vance, J.; Hreljac, A.; Hamill, J. Relationship between shock attenuation and stride length during running at different velocities. Eur. J. Appl. Physiol. 2002, 87, 403–408. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarantos, L.; Zeppetelli, D.J.; Dempsey, C.A.; Nagai, T.; Johnson, C.D. The Effects of Decreasing Foot Strike Angle on Lower Extremity Shock Attenuation Measured with Wearable Sensors. Sensors 2025, 25, 2656. https://doi.org/10.3390/s25092656
Sarantos L, Zeppetelli DJ, Dempsey CA, Nagai T, Johnson CD. The Effects of Decreasing Foot Strike Angle on Lower Extremity Shock Attenuation Measured with Wearable Sensors. Sensors. 2025; 25(9):2656. https://doi.org/10.3390/s25092656
Chicago/Turabian StyleSarantos, Lucas, David J. Zeppetelli, Cole A. Dempsey, Takashi Nagai, and Caleb D. Johnson. 2025. "The Effects of Decreasing Foot Strike Angle on Lower Extremity Shock Attenuation Measured with Wearable Sensors" Sensors 25, no. 9: 2656. https://doi.org/10.3390/s25092656
APA StyleSarantos, L., Zeppetelli, D. J., Dempsey, C. A., Nagai, T., & Johnson, C. D. (2025). The Effects of Decreasing Foot Strike Angle on Lower Extremity Shock Attenuation Measured with Wearable Sensors. Sensors, 25(9), 2656. https://doi.org/10.3390/s25092656