
Evaluation of Hydroxychloroquine Blood Concentrations and Effects in Childhood-Onset Systemic Lupus Erythematosus

 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Data Analysis
2.2. Association between HCQ Treatment and SLEDAI Score
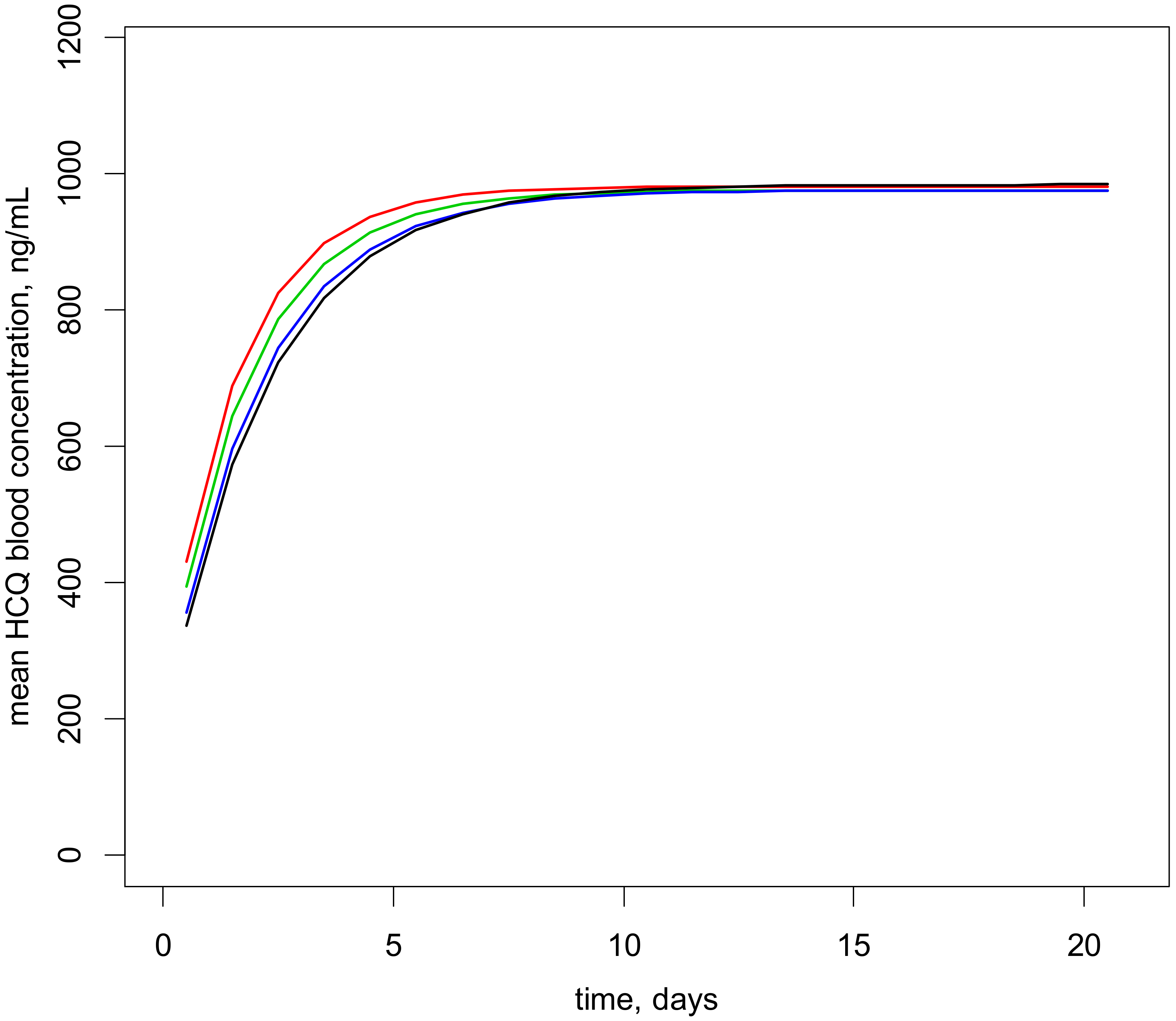
2.3. Dosage Recommendations
2.4. Blood HCQ Concentrations and Retinal Toxicity
3. Discussion
4. Materials and Methods
4.1. Patients and Drug Assay
4.2. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pineles, D.; Valente, A.; Warren, B.; Peterson, M.G.; Lehman, T.J.; Moorthy, L.N. Worldwide incidence and prevalence of pediatric onset systemic lupus erythematosus. Lupus 2011, 20, 1187–1192. [Google Scholar] [CrossRef] [PubMed]
- Hersh, A.O.; von Scheven, E.; Yazdany, J.; Panopalis, P.; Trupin, L.; Julian, L.; Katz, P.; Criswell, L.A.; Yelin, E. Differences in long-term disease activity and treatment of adult patients with childhood- and adult-onset systemic lupus erythematosus. Arthritis Rheum. 2009, 61, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Brunner, H.I.; Gladman, D.D.; Ibanez, D.; Urowitz, M.D.; Silverman, E.D. Difference in disease features between childhood-onset and adult-onset systemic lupus erythematosus. Arthritis Rheum. 2008, 58, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canadian Hydroxychloroquine Study Group. A randomized study of the effect of withdrawing hydroxychloroquine sulfate in systemic lupus erythematosus. N. Engl. J. Med. 1991, 324, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Van Vollenhoven, R.F.; Mosca, M.; Bertsias, G.; Isenberg, D.; Kuhn, A.; Lerstrom, K.; Aringer, M.; Bootsma, H.; Boumpas, D.; Bruce, I.N.; et al. Treat-to-target in systemic lupus erythematosus: Recommendations from an international task force. Ann. Rheum. Dis. 2014, 73, 958–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koneru, S.; Kocharla, L.; Higgins, G.C.; Ware, A.; Passo, M.H.; Farhey, Y.D.; Mongey, A.B.; Graham, T.B.; Houk, J.L.; Brunner, H.I. Adherence to medications in systemic lupus erythematosus. J. Clin. Rheumatol. 2008, 14, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Serrano, J.; Cardiel, M.H. Lupus patients in an emergency unit. Causes of consultation, hospitalization and outcome. A cohort study. Lupus 2000, 9, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Groot, N.; de Graeff, N.; Avcin, T.; Bader-Meunier, B.; Brogan, P.; Dolezalova, P.; Feldman, B.; Kone-Paut, I.; Lahdenne, P.; Marks, S.D.; et al. European evidence-based recommendations for diagnosis and treatment of childhood-onset systemic lupus erythematosus: The SHARE initiative. Ann. Rheum. Dis. 2017, 76, 1788–1796. [Google Scholar] [CrossRef] [Green Version]
- Tett, S.E.; Cutler, D.J.; Day, R.O.; Brown, K.F. A dose-ranging study of the pharmacokinetics of hydroxy-chloroquine following intravenous administration to healthy volunteers. Br. J. Clin. Pharmacol. 1988, 26, 303–313. [Google Scholar] [CrossRef] [Green Version]
- Jallouli, M.; Galicier, L.; Zahr, N.; Aumaitre, O.; Frances, C.; Le Guern, V.; Liote, F.; Smail, A.; Limal, N.; Perard, L.; et al. Determinants of hydroxychloroquine blood concentration variations in systemic lupus erythematosus. Arthritis Rheumatol. 2015, 67, 2176–2184. [Google Scholar] [CrossRef] [PubMed]
- Morita, S.; Takahashi, T.; Yoshida, Y.; Yokota, N. Population pharmacokinetics of hydroxychloroquine in Japanese patients with cutaneous or systemic lupus erythematosus. Ther. Drug Monit. 2016, 38, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Tett, S.E.; Cutler, D.J.; Beck, C.; Day, R.O. Concentration-effect relationship of hydroxychloroquine in patients with rheumatoid arthritis—A prospective, dose ranging study. J. Rheumatol. 2000, 27, 1656–1660. [Google Scholar] [PubMed]
- Munster, T.; Gibbs, J.P.; Shen, D.; Baethge, B.A.; Botstein, G.R.; Caldwell, J.; Dietz, F.; Ettlinger, R.; Golden, H.E.; Lindsley, H.; et al. Hydroxychloroquine concentration-response relationships in patients with rheumatoid arthritis. Arthritis Rheum. 2002, 46, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Costedoat-Chalumeau, N.; Amoura, Z.; Hulot, J.S.; Hammoud, H.A.; Aymard, G.; Cacoub, P.; Frances, C.; Wechsler, B.; Huong Du, L.T.; Ghillani, P.; et al. Low blood concentration of hydroxychloroquine is a marker for and predictor of disease exacerbations in patients with systemic lupus erythematosus. Arthritis Rheum. 2006, 54, 3284–3290. [Google Scholar] [CrossRef]
- Garg, S.; Unnithan, R.; Hansen, K.E.; Costedoat-Chalumeau, N.; Bartels, C.M. The Clinical significance of monitoring hydroxychloroquine levels in patients with systemic lupus erythematosus: A systematic review and meta-analysis. Arthritis Care Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Noël, Z.; Saik, U.; Benoit, L.; Valérie, P.; Olivier, P.; Alexandre, B.; Julien, M.; Estelle, G.; Guillaume, H.; Alain, C.; et al. Pharmacokinetics and pharmacodynamics of hydroxychloroquine in hospitalized patients with COVID-19. Therapies 2021. [Google Scholar] [CrossRef]
- Chasset, F.; Arnaud, L.; Costedoat-Chalumeau, N.; Zahr, N.; Bessis, D.; Frances, C. The effect of increasing the dose of hydroxychloroquine (HCQ) in patients with refractory cutaneous lupus erythematosus (CLE): An open-label prospective pilot study. J. Am. Acad. Dermatol. 2016, 74, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.J.; Holford, N.H. Mechanism-based concepts of size and maturity in pharmacokinetics. Annu. Rev. Pharmacol. Toxicol. 2008, 48, 303–332. [Google Scholar] [CrossRef]
- Monostory, K.; Dvorak, Z. Steroid regulation of drug-metabolizing cytochromes P450. Curr. Drug Metab. 2011, 12, 154–172. [Google Scholar] [CrossRef]
- Carmichael, S.J.; Day, R.O.; Tett, S.E. A cross-sectional study of hydroxychloroquine concentrations and effects in people with systemic lupus erythematosus. Intern. Med. J. 2013, 43, 547–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noe, G.; Amoura, Z.; Combarel, D.; Lori, L.; Tissot, N.; Seycha, A.; Funck-Brentano, C.; Zahr, N. Development and validation of a fast ultra-high performance liquid chromatography-fluorescent method for the quantification of hydroxychloroquine and its metabolites in patients with lupus. Ther. Drug Monit. 2019, 41, 476–482. [Google Scholar] [CrossRef] [PubMed]
- McCune, J.S.; Bemer, M.J.; Barrett, J.S.; Scott Baker, K.; Gamis, A.S.; Holford, N.H. Busulfan in infant to adult hematopoietic cell transplant recipients: A population pharmacokinetic model for initial and Bayesian dose personalization. Clin. Cancer Res. 2014, 20, 754–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Covariate | Mean ± Standard Deviation | Min | Max |
|---|---|---|---|
| Age, years | 15 ± 2 | 5.5 | 18 |
| Weight, kg | 51 ± 18 | 18.8 | 120 |
| Sex, (F) (n/N) | 151/168 | NA | NA |
| Schwartz, mL/min/1.73 m2 | 116 ± 26 | 34 | 201 |
| Creatinine, µmol/L | 50 ± 14 | 25 | 163 |
| Albumin, g/L | 38 ± 6 | 11 | 68 |
| Hb, g/dL | 12 ± 1.5 | 7 | 17.7 |
| Platelet, 109/L | 267 ± 75 | 76 | 674 |
| Proteinuria, g/L | 1.2 ± 1.5 | 0 | 7.5 |
| White blood cells, 109/L | 5.28 ± 2.1 | 2 | 10.8 |
| C3 (mg/L) | 887 ± 253 | 126 | 1460 |
| SLEDAI score | 4.4 ± 3.9 | 0 | 25 |
| Dose HCQ, mg/kg/day | 5.7 ± 2.1 | 2 | 15.7 |
| Comedications: | |||
| Corticosteroids (n/N) | 136/168 | NA | NA |
| Immunosuppressant (n/N) | 104/168 | NA | NA |
| Concentration HCQ, ng/mL | 665 ± 433 | 100 | 2509 |
| Sampling time, day | 1100 ± 830 | 10 | 3674 |
| Fixed Effects Parameters | Estimate | RSE (%) |
|---|---|---|
| Blood Clearance #, CL/FPOP (L/h standardized to 70 kg) | 19.6 | 5.35 |
| Weight effect on CL/F, (WT/70)WT | 0.75→fixed | NA |
| Platelet effect on CL/F, (Platelet/250,000)PLAT | −0.648 | 25 |
| Effect on disease, SLEDAI score > 6 units ## | ||
| intercept | 5.55 | 30 |
| bHCQ, slope for log10 (HCQ concentration) effect | −2.41 | 24 |
| Variabilities | ||
| ωCL | 0.263 | 22 |
| σ, proportional | 0.385 | 8 |
| ωintercept | 1.88 | 18 |
| Bodyweight Band kg | Dosage mg/kg/Day | Prob (C > 750) ng/mL |
|---|---|---|
| 15–21.9 | 9 | 53.4 |
| 22–34.9 | 8 | 55 |
| 35–60.9 | 7 | 54.4 |
| 61–71 | 6.5 | 52.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zahr, N.; Urien, S.; Funck-Brentano, C.; Vantomme, H.; Garcelon, N.; Melki, I.; Boistault, M.; Boyer, O.; Bader-Meunier, B. Evaluation of Hydroxychloroquine Blood Concentrations and Effects in Childhood-Onset Systemic Lupus Erythematosus. Pharmaceuticals 2021, 14, 273. https://doi.org/10.3390/ph14030273
Zahr N, Urien S, Funck-Brentano C, Vantomme H, Garcelon N, Melki I, Boistault M, Boyer O, Bader-Meunier B. Evaluation of Hydroxychloroquine Blood Concentrations and Effects in Childhood-Onset Systemic Lupus Erythematosus. Pharmaceuticals. 2021; 14(3):273. https://doi.org/10.3390/ph14030273
Chicago/Turabian StyleZahr, Noël, Saik Urien, Christian Funck-Brentano, Hélène Vantomme, Nicolas Garcelon, Isabelle Melki, Margaux Boistault, Olivia Boyer, and Brigitte Bader-Meunier. 2021. "Evaluation of Hydroxychloroquine Blood Concentrations and Effects in Childhood-Onset Systemic Lupus Erythematosus" Pharmaceuticals 14, no. 3: 273. https://doi.org/10.3390/ph14030273
APA StyleZahr, N., Urien, S., Funck-Brentano, C., Vantomme, H., Garcelon, N., Melki, I., Boistault, M., Boyer, O., & Bader-Meunier, B. (2021). Evaluation of Hydroxychloroquine Blood Concentrations and Effects in Childhood-Onset Systemic Lupus Erythematosus. Pharmaceuticals, 14(3), 273. https://doi.org/10.3390/ph14030273