Abstract
Various autoimmune diseases, including autoimmune hypothyroidism (AHT), are associated with a higher risk of developing mood disorders throughout life. Depression is accompanied by the changes in the levels of inflammatory and trophic factors, including interleukins (IL-1beta, IL-2, IL-6), interferon alpha (IFN-alpha), tumor necrosis factor alpha (TNF-alpha), C-reactive protein (CRP), and brain derived neurotrophic factor (BDNF). Disclosure of the relationship between the coexistence of depression and AHT indicates that the pathomechanism of depression may be related to the changes in the immune system, it is also possible that both conditions may be caused by the same immune processes. The above hypothesis is indirectly supported by the observations that the treatment with both antidepressants and levothyroxine leads to a decrease in the levels of proinflammatory cytokines with an increase in BDNF concentrations, simultaneously correlating with an improvement in the clinical parameters. However, so far there are no long-term studies determining the causal relationship between depression, thyroid autoantibodies, and cytokine profile, which could bring us closer to understanding the interrelationships between them and facilitate the use of an adequate pharmacotherapy, not necessarily psychiatric. We consider the above issues to be insufficiently investigated but of great importance. This article is an overview of the available literature as well as an introduction to our research project.
1. Introduction
The relationship between thyroid function and depression has been known for a long time [1,2,3]. It was first described in 1825 by Parry, who noted an increased number of “nerve strokes” in thyroid disease. Seagull in 1873 showed a link between myxedema and psychosis, which was confirmed in 1888 by the Committee of the Clinical Society. In 1949 Asher introduced the term “myxedema madness” to describe mental state changes in patients with hypothyroidism [4]. It is currently well known that thyroid dysfunction can significantly affect the mental state, including emotions and cognitive functions. Both the excess and the deficiency of thyroid hormones can cause mood disorders, including depressive disorders, which can be usually resolved with an appropriate treatment of dysthyreosis. Depression may, in turn, be accompanied by various degrees of thyroid dysfunction. An overt hypothyroidism is present in 1–4% of patients with affective disorders, while subclinical hypothyroidism occurs in 4–40% of this population. According to Boswell, the frequency of depressive symptoms in patients with hypothyroidism reaches 50% [5], while depression of significant clinical severity occurs in over 40% of people suffering from hypothyroidism [6]. What is practically very important, and what prompted us to undertake the research, is that the depressive states associated with broadly understood thyroid dysfunction are usually at least partially resistant to antidepressant treatment, with the causal treatment being the key here. Thyroid hormones are also usually recommended as an adjunctive therapy in the treatment of depression in treatment algorithms [7,8]. The interdependence of thyroid disorders and depression, as well as their coexistence, is of great clinical importance, but knowledge about it is very limited. In the article, we want to summarize the current knowledge and raise topics related to the issue and which may indicate new directions of research.
Autoimmune Hypothyroidism (AHT) and Depression
AHT is a progressive disease of the thyroid gland. Dense lymphocytic infiltration covering the gland is involved in the pathogenesis of this type of chronic thyroiditis [9]. Activated B cells produce antibodies against several major thyroid antigens. AHT is characterized by a combination of typical clinical features (Table 1) [10], increased serum thyroid-stimulating hormone (TSH) levels; decreased free thyroxine (fT4) levels; the presence of antibodies to thyroid antigens; and decreased ultrasonographic echogenicity of the thyroid parenchyma [11].

Table 1.
Autoimmune hypothyroidism—symptoms, assessment, and diagnostic findings.
AHT is the most common organ autoimmune disorder, with an estimated prevalence of approximately 2%, women suffer more frequently. Thyroid peroxidase (TPO) is the main autoantigen, and antibodies to TPO (Anti-TPO) are present in almost all AHT patients and may precede onset of the clinical phase by up to several years. Subclinical AHT (with the presence of Anti-TPO, elevated TSH and normal fT4 levels) is more frequent and affects approximately 9% of the general population [11].
Depression, including severe depression, is more common in patients with euthyroid chronic AHT compared to subjects without this condition [9]. Frequent simultaneous presence of depressive and anxiety disorders in patients with Hashimoto’s disease (over 90% of AHT) in the euthyroid stage has also been confirmed [12]. A large Danish epidemiological study has shown that various autoimmune diseases, including AHT, are associated with a higher occurrence of mood disorders throughout life [13]. It has been shown that it is not only the decreased level of thyroid hormones that determines the occurrence of mood disorders. We also know that even in patients with normal thyroid function but with elevated Anti-TPO antibodies, their presence correlates with a higher risk of anxiety and mood disorders [14]. An increased level of anti-thyroid antibodies has been documented in 20% of patients with depression, while the incidence in the general population ranges from 5% to 10% [15,16]. In patients with bipolar disorder, regardless of the use of lithium (having “anti-thyroid” properties), the presence of Anti-TPO and AHT is also more frequent [17,18]. Also, the offspring of people with bipolar disorder have a higher incidence of Anti-TPO, even if they do not have mental disorders [19,20]. There are also data showing an increased level of Anti-TPO and antibodies blocking the TSH receptor in patients with depressive disorders without thyroid dysfunction, but who were resistant to antidepressant treatment [21]. Several hypotheses are proposed to explain the above observations. A decrease in the secretion of thyroid hormones is interpreted as a result of the dysregulation of the TSH secretion circadian rhythm (physiologically TSH levels are higher at night). This suggests that some depressed patients may have central hypothyroidism (pituitary and hypothalamus dependent, secondary, and tertiary, respectively). Moreover, sleep deprivation used in the treatment of depression leads to the restoration of the nocturnal rise in TSH levels and, consequently, an increase in free triiodothyronine (fT3) and fT4 levels. According to another hypothesis, autoimmune thyroid diseases are associated with the hypothalamic–pituitary–adrenal axis and are mediated by changes in the concentration of pro-inflammatory and anti-inflammatory cytokines. TNF-alpha (tumor necrosis factor) and interleukins IL-1 and IL-6 (all pro-inflammatory agents) increase the release of CRH (corticoliberin) and AVP (arginine vasopressin) leading to increase of glucocorticosteroid (GC) secretion from the adrenal cortex. Chronically high GC levels induce receptor resistance to GC, subsequently causing further increase in their secretion and disturbances in the functioning of the hypothalamic–pituitary–adrenal axis, increasing the susceptibility to autoimmune processes and depression [22,23]. The next hypothesis connects the frequent postpartum recurrence of depression with the end of the immune tolerance present in pregnancy [24,25]. Unfortunately, currently there are no studies showing a relationship between postpartum thyroiditis and postpartum depression and convincingly explaining the etiopathogenetic relationships but indicate the existence of common elements of the immune pathogenesis of both AHT and mood disorders.
The results of the summary on depression, anxiety, and AHT indicate that, in the United States, the prevalence of AHT is 4–13%, AHT more often affects women, and its occurrence increases with age, reaching 20% in the group of older women [26]. Prevalence of depression reached 6.6%, and anxiety disorders 18.1% in this study. It was also found that depression occurs in 16.8% of patients suffering from AHT, while the criteria for anxiety disorders were met by 35.7% of patients. The recently published meta-analysis of the comorbidity of hypothyroidism and depression did not show a statistically significant relationship between the autoimmunity of the thyroid gland and the incidence of depressive disorders [27]. The study of the relationship between morphological changes in the central nervous system in AHT patients with hypothyroidism using positron emission tomography (PET) also did not show any direct relationship between specific changes caused by AHT and the development of depressive disorders [2,28].
2. Methods
2.1. Review Question
Patients with autoimmune hypothyroidism have a potentially higher risk of depression. While coexistence of these health problems is of great clinical importance, the knowledge linking these issues is very limited. The purpose of this article is summarizing the current knowledge, and raising topics related to the issue which may indicate new directions of research. All data included in the review should meet high methodological requirements.
2.2. Searches
The literature search was completed on 8 March 2022. We searched five databases: EMBASE; PubMed; Cochrane Library; Scopus; and Web of Science. The search was restricted to peer-reviewed publications of original research written in English and German from 1990 to 2022, both years included. Both authors checked all the databases and collected the data separately. The inclusion of the study into the list was preceded by a discussion and the consent of both researchers.
2.3. Search Strategy
An example of a search strategy for PubMed database: “autoimmune hypothyroidism” and “depression”; “autoimmune hypothyroidism” and “depression” and “BDNF”; “autoimmune hypothyroidism” and “depression” and “interleukin”, autoimmune hypothyroidism” and “depression” and “gene”; autoimmune hypothyroidism” and “depression” and “treatment”.
2.4. Condition or Domain Being Studied
All aspects of autoimmune hypothyroidism (AHT) and depression comorbidity.
2.5. Participants/Population
For the purposes of this review, we included all studies that studied various aspects of depression in a population of patients with autoimmune disorders of the thyroid gland. From the scientific perspective, we were most interested in the works on autoimmune hypothyroidism (AHT), but already while writing the protocol, we noted that some literature did not use the term AHT, however, important data for us were described in patients with Hashimoto disease (at least 90% of AHT). For obvious reasons, we decided to include both diseases, remembering to follow the terminology used by the authors in the description of the results. Due to the fact that the literature in this area was limited, we tried to include all original studies on the subject. Our search included available data on changes in clinical and biochemical parameters of coexisting AHT and depression, and the effect of treatment of mental disorders and thyroid gland on changes in these parameters.
2.6. Intervention(s), Exposure(s)
We described all relevant data from studies focused on the relationship of autoimmune hypothyroidism (including Hashimoto disease), thyroid parameters (TSH, triiodothyronine, thyroxine, antibodies including anti-TPO, ultrasonography findings) with depression (symptomatology, drug effects incl. antidepressants); morphological; functional changes in imaging techniques (e.g., magnetic resonance imaging); differences in gene polymorphisms and gene activity; levels of interleukins; BDNF; and other relevant proteins.
2.7. Comparator(s)/Control
Majority of the results included in the review were compared to the control group or between groups.
2.8. Types of Study to Be Included
We accepted all studies that documented methodologically correct co-occurrence of disorders, which included patients with depression and hypothyroidism in accordance with the ICD or DSM terminology.
2.9. Main Outcomes
Correlations between parameters of autoimmune hypothyroidism as TSH; triiodothyronine; thyroxine; antibodies (including anti-TPO) levels; ultrasonography findings and parameters linked to depression (severity of symptoms, effects of treatment, incl. antidepressants and thyroid hormones) were our main outcomes. We also planned to identify and analyze morphological and functional changes in brain imaging techniques (e.g., magnetic resonance imaging); differences in gene polymorphisms and gene activity; levels of BDNF; interleukins; and other relevant proteins in patients with AHT and depression.
2.10. Measures of Effect
Our systematic review discusses the effect measure(s) for the main outcome(s) e.g., relative risks, odds ratios, risk difference, and/or number needed to treat if possible.
2.11. Data Extraction
We extracted data from the included studies for simultaneous assessment of study quality and summary of the evidence. Extracted information that can be used in a tabular form includes author; year; sample size; characteristic of participants; results and conclusions; and reference. Both authors independently extracted the data, any incongruities were resolved through discussion.
2.12. Risk of Bias (Quality) Assessment
We assessed quality of studies to review.
2.13. Certainty Assessment
All articles cited and discussed were published in peer-reviewed journals.
2.14. Strategy for Data Synthesis
Due to the nature of the research described, descriptive analysis was the main method used in our work.
2.15. Registration
PROSPERO ID 314540.
Figure 1 shows the PRISMA flow chart for screening and selection of studies researching the comorbidity of AHT and depression.
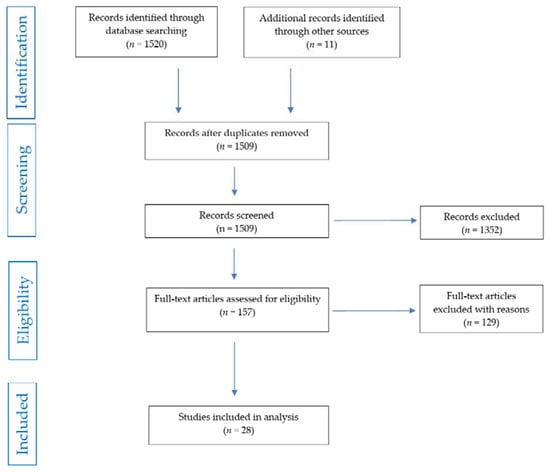
Figure 1.
PRISMA flow chart of studies selection.
3. Results and Discussion
We present summarized characteristics of all included studies covering population with a simultaneous diagnosis of depression and autoimmune hypothyroidism in Table 2.
Table 2.
Studies investigating various aspects of depression and AHT comorbidity.
3.1. Inflammatory Processes, Cytokines and Growth Factors
Common etiological basis for both thyroid autoimmunity and mood disorders are also seen in similar changes of growth and differentiation in the hematopoietic and neuronal system cells and similar changes in the cytokine profile [10]. Numerous studies indicate that depression activates the inflammatory response system through increased production of well-known pro-inflammatory cytokines such as IL-1beta, IL-2, IL-6, IFN-alpha (interferon alpha), TNF-alpha, and their receptors (IL-6R, IL-1RA) [53]. It was also observed that patients with Hashimoto’s disease (HD) had higher levels of IL-17 and IL-23 compared to the control group without thyroiditis and the highest levels were obtained in HD patients in euthyrosis. TSH was negatively correlated and fT4 was positively correlated with IL-17 and IL-23 levels, whereas there was no correlation between thyroid volume calculated from ultrasonography and levels of IL-17 and IL-23. There was also a strong association between IL-17 expression and stromal fibrosis in thyroid epithelial cells, suggesting that the proinflammatory effects of IL-17 are directing thyroid tissue development towards fibrosis specific for Hashimoto’s disease that distinguishes this disease from other benign thyroid disorders [54].
The pathophysiological effects of thyroid autoantibodies in depression may depend on cytokines. Th17 lymphocytes and their primary cytokine, interleukin 17, play an important role in autoimmune diseases—IL-17 is a key signaling molecule that induces the release of pro-inflammatory cytokines and chemokines. However, to date, little is known about whether IL-17 is related to depression. One study [55] showed that IL-17 levels did not differ between controls and depressed individuals. IL-17 levels were not associated with either antithyroid antibody levels or depression severity scale. IL-17 was also not associated with age, thyroid hormone levels, or other thyroid autoantibody levels.
As we mentioned, stress induces production of pro-inflammatory cytokines leading to neuroendocrine and neurotransmitter changes resembling symptoms of depression. IFN-alpha immunotherapy (e.g., used previously in hepatitis C) often causes depressive symptoms and autoimmune thyroid disorders with the appearance of anti-TPO and anti-thyroglobulin (anti-TG) antibodies [56]. The presence of acute phase proteins and cytokines may be associated with inflammation within the brain. Peripherally produced cytokines can cross the blood-brain barrier [57,58]. After crossing the barrier they are able to participate in stress response modulation and regulation of neurogenesis [56].
Cytokines act on the brain in two successive stages: the first is triggered by activation of primary afferent neurons innervating the area of the body where the inflammatory response is taking place. The second involves the slow diffusion of cytokines from the periventricular organs and choroid plexus to target brain parts, such as the amygdala complex. Although disease behavior is a normal host response to pathogens that are recognized by the innate immune system, there is evidence that the mechanisms that contribute to the development of disease behavior may play a role in the pathophysiology of depression [59]. Mood can be attenuated also by the influence of cytokines on neurogenesis within hippocampal neurons, which is believed to be a key mechanism in the pathophysiology of depression and its treatment [60,61,62]. The weakening of neurogenesis may, over time, contribute to the reduction of the gray matter volume in the hippocampus, often observed in depression [63]. It is still unclear whether the presence of acute phase proteins may be the cause, consequence or only accompanying the depression. Studies of changes in cytokines and other inflammatory parameters in the population with the concomitant occurrence of AHT with depression (also during pharmacological interventions) are very limited.
Similarly, the direct pathophysiological relevance of antithyroid antibodies to neuropsychiatric disorders is not established yet. In one study, anti-TPO antibodies were shown to bind to cerebellar astrocytes. Another study suggested that cerebral vascular smooth muscle cells may be target structures for anti-TG antibodies. However, replication of these findings is still pending, and their relevance to the pathophysiology of depressive syndromes is unclear. Therefore, most authors consider anti-thyroid antibodies only as an epiphenomenon indicating an autoimmune predisposition. The occurrence of antibodies in healthy individuals and the independence of serum concentrations from the clinical symptoms’ expression in patients with Hashimoto’s encephalopathy indicates no direct pathophysiological significance of these antibodies [49]. On the other hand, the presence of anti-TPO antibodies during pregnancy and in the weeks after childbirth increases the risk of developing post-partum depression [50] and increases the risk of anxiety in the postpartum period [64].
A study conducted in patients with hypothyroidism after thyroidectomy due to cancer showed increased levels of the pro-inflammatory cytokines IL-6; IL-10; IL-17; TNF-alpha; and C-reactive protein (CRP). Levothyroxine therapy (used in hypothyroidism) resulted in a decrease in the level of these cytokines, but their levels were still higher than in healthy subjects [65]. In patients treated with levothyroxine, a simultaneous reduction in the level of pro-inflammatory cytokines and an increase in the levels of anti-inflammatory cytokines has been also demonstrated [66]. Interestingly, primary AHT is characterized by increased values of pro-inflammatory cytokines such as IL-2; IL-6; IL-15; TNF-alpha; and CRP [7,54,66,67]. During treatment with levothyroxine, a significant decrease in the levels of IL-1; IL-2; IL-6; IL-12; IFN-gamma; TNF-alpha; and a significant increase in IL-10 (anti-inflammatory cytokine) was observed [7,66]. In the Polish study the incidence of mild and moderate depression among patients with hypothyroidism was initially 57%. After six months of levothyroxine therapy and achieving euthyroidism, nearly half of the group (42%) remitted depressive symptoms [7].
Use of selective serotonin reuptake inhibitors (SSRI), our most frequently used group of antidepressants, reduces the promoting-depression effect of pro-inflammatory cytokines. Fluoxetine has been shown to reduce the expression of IL-1beta, IL-6, and TNF-alpha, but, interestingly, subsequently increasing the level of IL-10 [68]. Desipramine (a tricyclic antidepressant, (TCA)) reduces the levels of TNF-alpha in the hippocampus and brainstem [69], and its clinical efficacy has been associated with its ability to alter the sensitivity of noradrenergic neurons to TNF-alpha [70]. In conclusion, studies evaluating the effects of SSRIs and other antidepressive drugs indicate that inflammatory factors contribute to the pathogenesis of depression, and that various antidepressants have ability to reduce the release of pro-inflammatory cytokines, such as e.g., IL-1beta.
The results of the few published studies indicate that various antidepressants affect the level of thyroid hormones differently in patients with depression, which is probably due to differences in mechanisms of action between the drugs [71]. The results of a study evaluating the effects of reboxetine, venlafaxine and sertraline on TSH and thyroid hormones (T4—thyroxine and fT4) levels before and after treatment in severely depressed patients showed large discrepancies between drugs, although improvement in depressive symptoms occurred in all groups. A decrease in TSH levels and an increase in fT4 and T4 was observed in patients treated with reboxetine, no changes in hormone levels were observed in those treated with venlafaxine, while patients taking sertraline had an increase in TSH levels, a decrease in fT4, and T4 levels [72]. The effect of SSRIs on thyroid function was summarized by a meta-analysis that included clinical studies that measured levels of thyroid parameters (TSH, T4, fT4, or fT3) before and after treatment with SSRIs (as a group). It was shown that after treatment with these drugs, patients had lower levels of T4, fT4 and fT3 with no change in TSH values [73]. So far, the mechanism of inducing hypothyroidism during SSRI treatment has not been established. One hypothesis is that SSRIs stimulate the activity of the type 2 iodothyronine deiodinase enzyme, which converts T4 to T3 (trioiodothyronine) in various tissues, including the brain [74]. Also, the relief of depressive symptoms causes biological effects that may modulate the thyroid axis. It has been documented that there is an association of the effect of venlafaxine treatment with polymorphisms in the NR3C2 gene and elevated TSH levels [75] in a mechanism to restore normal function of the hypothalamic–pituitary–adrenal axis through regulation of the mineralocorticoid receptor (MR) and the glucocorticoid receptor (GCR), encoded by the NR3C2 and NR3C1 genes. The NR3C2 gene provides instructions for the formation of a protein called the mineralocorticoid receptor. This protein plays the important role in regulating the amount of sodium in the body. Sodium co-regulates blood pressure control and fluid balance. Mineralocorticoids attach (bind) and switch on (activate) the mineralocorticoid receptor. Aldosterone is one of the mineralocorticoids that activates the mineralocorticoid receptor. Activated mineralocorticoid receptor acts as a transcription factor, a protein that binds to specific DNA regions and helps control the activity (transcription) of particular genes. The mineralocorticoid receptor regulates specialized proteins in the cell membrane that control the transport of sodium or potassium into cells. In response to signals that sodium levels in the body are low, the mineralocorticoid receptor increases the number and activity of these proteins in the cell membrane, especially in selected kidney cells. One of these proteins transports sodium into the cell, while another protein simultaneously transports sodium out of the cell and potassium into the cell. These proteins help keep sodium in the body (reabsorption) and remove potassium from the body (secretion) [76].
Studies on the effect of thyroid hormones on the speed of action of antidepressants indicate that accelerating the response to antidepressants is not possible for all classes of antidepressants. T3 accelerates responses to TCAs (tricyclic antidepressants) but does not have the same effect when used with SSRIs. In a meta-analysis of four RCTs of controlled depression patients, there was no evidence of a faster onset of response when T3 was added to SSRIs [77]. The reasons for a discrepancy between the effects of T3 on TCA versus SSRIs remain unknown [78]. However, we do not have data on the effect of treatment with antidepressants on the biochemical parameters of the thyroid gland, including the levels of anti-thyroid antibodies in patients with AHT. Figure 2 summarizes the interrelationships between treatment, biochemical parameters and clinical outcome.
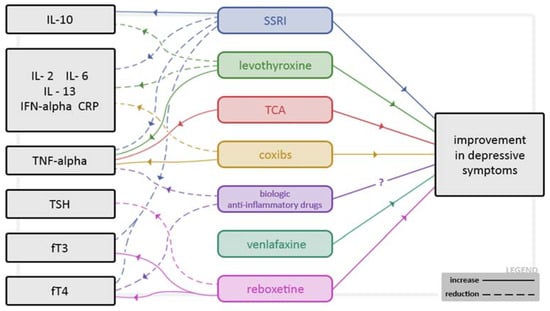
Figure 2.
Potential mechanisms of relation between depressive symptoms and selected drugs and their influence on the values of selected hormonal and inflammatory parameters.
It is worth noting that preliminary data suggest that anti-inflammatory drugs may be useful in mood disorders—it has been reported that in patients treated with rofecoxib and celecoxib, the depressive symptoms’ improvement was more pronounced than in the group not treated with these drugs [79,80]. This effect, at least partially, may be related to the analgesic effect of the COX-2 inhibitors, but studies on rats showed that use of rofecoxib leads to a serotonin increase in the frontal, parietal, and temporal cortexes, which may indicate their other-than-analgesic mechanism of action [79]. So far, no studies have been conducted to assess the effect of anti-inflammatory drugs on the biochemical parameters of thyroid function in AHT. Even if not all depressive states have an inflammatory etiology, according to the available data there is possibly a separate subtype of depression of inflammatory origin, or a manifestation of an inflammatory process is able to clinically mimic depression. Biological anti-inflammatory drugs, including anti-TNF-alpha antibodies such as e.g., infliximab, adalimumab, and guselkumab potentially may be useful to treat those types of depression. Those particles have an ability to reduce the severity of inflammation (e.g., in rheumatic diseases, psoriasis, and Crohn’s disease) very effectively. However, the conclusions from limited depression trials are ambiguous, although patients with high initial levels of pro-inflammatory cytokines may have more benefit with this treatment [81,82,83]. Tocilizumab (IL-6 receptor blocker) studies show its potential to decrease the levels of depressive symptoms in patients with rheumatoid arthritis [84,85], but in patients with haematological problems the results were completely different—depressive symptoms were exacerbated with this drug [86]. Interestingly, hallucinogens (increasingly studied in depression) and bupropion have an ability to block TNF-alpha or decrease its production [87].
Scarce data from studies concerning the thyroid gland function during use of TNF-alpha antibodies showed mostly neutral results (no changes in TSH, T3, anti-TPO and anti-TG antibodies levels, decrease in fT4 levels) [88]. We need to underline here that depression (also with increased suicidal risk) and thyroiditis (new onset or its exacerbation) are among common side effects of TNF-alpha blockers.
Studies involving relatives of patients with AHT force even deeper reflections about the common origin of both AHT and depression. Euthyroid women being relatives of AHT patients have abnormal serum levels of hematopoietic and neural growth and differentiation factors important in the etiology of depression—BDNF (Brain-derived neurotrophic factor); IGFBP-2 (insulin-like growth factor binding protein); EGF (epidermal growth factor); and SCF (stem cell factor) [11]. Serum levels of the other growth factor TGF-beta1 (a polypeptide member of the transforming growth factor beta superfamily of cytokines) are lowered in patients with HD [89].
It is also worth noting the increasing research on the impact of gut microflora and translocation of bacteria from the gut to the blood in patients with depressive disorders. The relationship between gut barrier dysfunction, bacterial translocation, and the immune system in depressed patients and the expression of activated monocytes in depressed patients has been established. Treg lymphocytes (which play a role in regulating the activation and effector activity of innate and adaptive immune response cells, as well as in controlling and suppressing the immune response against their own antigens) play an important role in this mechanism. There is an increased proportion of Treg cells in depressed patients. Moreover, there is a significant association between the gut microbiota and Treg. The reduction of Treg expansion may suppress the intestinal migration of these cells. Reduction of Treg of systemic origin may compromise the total number of intestinal Treg. Reduction of Treg in the intestinal mucosa may promote intestinal barrier damage and increased bacterial translocation found in some depressed patients. Furthermore, the presence of depression is associated with increased intestinal permeability or ‘leaky gut’ and increased bacterial translocation. There is also evidence that the microbiota affects the immune system and vice versa [9].
Depressed patients had significantly elevated levels of circulating intestinal fatty acid-binding protein, a marker of intestinal barrier function in peripheral blood (I-FABP) and lipopolysaccharide-binding protein (LBP). In addition, depressed patients with high LBP levels showed a significant reduction in circulating Treg compared to depressed patients with normal LBP. The balance of effector lymphoid cells and Treg cells may have a profound effect on how the intestinal mucosa responds to stressors that cause damage. Although there is no direct evidence for causality, this study supports the existence of a so-called gut–brain axis, linking gastrointestinal and immune system functions to the emotional and cognitive areas of the brain [90].
3.2. Brain-Derived Neurotrophic Factor (BDNF) and Depression, AHT and Gender
BDNF needs a broader description as a crucial element in the current understanding of the development and dynamics of depressive symptomatology. This particle belongs to the group of neurotrophins, proteins synthesized in the cells of the central and peripheral nervous system and involved in the development, function, and protection of nerve cells. It regulates many processes in our body, including the development and growth of neurons, inhibiting apoptosis, promoting neurogenesis, neuroregeneration, and stimulating the formation of dendritic connections. BDNF participates in the regulation of neuronal plasticity related to learning and memory processes, influencing the process of synaptic long-term potentiation and long-term depression in the hippocampus. It also influences the development of serotonergic, dopaminergic, noradrenergic, and cholinergic neurons. Dopaminergic neurons of the substantia nigra and striatum have been found to be the main source of BDNF secretion. BNDF easily crosses the blood-brain barrier [91].
Preclinical studies show that stress reduces BDNF expression in the rat hippocampus, while a single two-sided direct infusion of BDNF into the rat hippocampus has an antidepressant effect in animal models of depression [92]. In humans, BDNF plays a significant role in the pathophysiology of mental disorders, especially depression, where its key role is undisputable. Patients with severe depressive symptoms show lower levels of BDNF compared to controls. Moreover, BDNF levels are correlated with the reduction of the hippocampal volume [93]. We also know that BDNF expression is lower in the prefrontal cortex and hippocampus of people who died by suicide compared to the control group matched in terms of sex and age [94]. The use of sertraline, escitalopram, and venlafaxine in the study by Matrisciano et al. resulted in significant clinical improvement despite varying effects on the peripheral BDNF levels. A relationship was also found between an increase in BDNF serum levels and an improvement in the Hamilton Depression Rating Scale, thus indicating that a higher BDNF level in the blood serum corresponds to recovery [93]. It has been shown that BDNF levels were directly related to antidepressant responses, and people who responded well to treatment (>50% improvement in the scores of depression severity scales) had higher BDNF levels before treatment than non-responders, indicating that BDNF can be also a potential predictor of the antidepressant response [95]. It was also confirmed that the concentration of BDNF and its changes are not rigidly correlated with improvement in depression, but that the level of BDNF generally increases during antidepressant treatment. Studies on rapid-acting antidepressant—ketamine—having different mechanisms of action than SSRIs and TCAs, showed that the rapid antidepressant response after its administration is mediated by an increase in BDNF levels [96].
Research directly linking BDNF to thyroid disorders is scarce at present. Rats with early-onset hypothyroidism exhibited lower levels of BDNF in the brain [97]. Preclinical studies conducted by Hung indicate that thyroxine protects against white matter damage by increasing the level of BDNF [98]. In clinical trials, higher TSH levels were associated with a more discrete increase in serum BDNF levels in depressed patients during antidepressant therapy [99], and lower baseline TSH levels correlated with greater improvements after fluoxetine and sertraline [100]. It has also been shown that observed clinical results were better among patients who had lower TSH levels during sertraline and triiodothyronine therapy [98]. On the other hand, the only study evaluating the effect of thyroid hormones on changes in BDNF in serum, plasma, and platelets over the 3-month period of treatment with antidepressants in patients without thyroid disease showed that higher TSH levels correlated with a lower increase in serum levels of BDNF during antidepressant treatment. It was additionally indicated that with an increase in TSH, BDNF concentrations decreased within the observation period [99]. In patients participating in this study, no such relationship was found between the levels of triiodothyronine (T3); thyroxine (T4); corticotropic hormone (ACTH); cortisol; prolactin (PRL); luteinizing hormone (LH); follicle stimulating hormone (FSH); estrogen; and progesterone. A study evaluating similar relationships in patients with hypothyroidism and subclinical hypothyroidism has not been conducted so far.
In conclusion, it can be hypothesized that thyroid hormones may affect the response to antidepressant therapy through its influence on BDNF, but so far there are not sufficient data to confirm this hypothesis unequivocally.
Due to the epidemiology of depression and AHT, it is worth emphasizing that the relationship between the level of BDNF and depression may depend on gender. It has been shown that reduced BDNF values are more pronounced in women with depression, and long-term antidepressant use selectively raises its concentration in women. Therefore, it is possible that the more frequent occurrence of depression in women may be related to this mechanism and interactions with female sex hormones, especially since it has been shown that BDNF expression can be reduced by higher levels of estradiol in animal model [101].
It is still an open question: what is the cause of the increased incidence of depression in patients with AHT? Is it the influence of hormonal disorders or changes in cytokine profile, BDNF levels, or antithyroid antibodies accompanying AHT?
Trying to answer these questions we analyzed another autoimmune disease that is not accompanied by hormonal changes. In rheumatoid arthritis prevalence of depression is significantly higher than in the general population and is estimated at 15–34%. Studies investigating the associations of disease intensity, levels of pro-inflammatory cytokines, and neurotrophic factors with depression in patients with RA found that pro-inflammatory cytokine levels were not associated with depression, and only BDNF levels were associated with depression. Considering the above, we conclude that the reason for the higher prevalence of depression in AHT patients is endocrine disruption rather than increased levels of pro-inflammatory cytokines.
Figure 3 summarize the current knowledge on postulated pathogenetic mechanisms and relationships of depression, thyroid dysfunction, and inflammation.
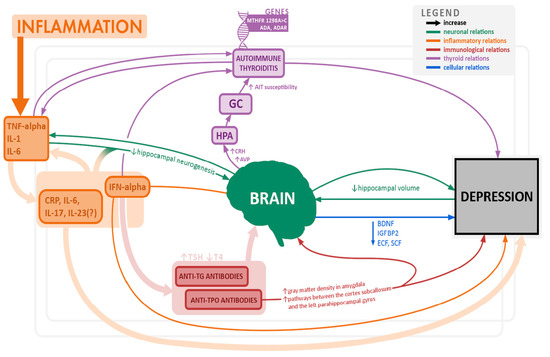
Figure 3.
Overview of potential pathomechanisms associated with depression and thyroid dysfunction.
4. Conclusions
People with a higher risk of developing mood disorders, including depressive disorders, are at the same time more likely to develop autoimmune thyroid disease and vice versa, which may indicate common pathogenetic roots. An abnormal profile of haemopoietic and neuronal growth factors, including BDNF, is observed in patients with mood disorders as well as in those at risk of developing AHT. Similar observations apply to the cytokine profile in patients with both diseases, in whom we observe an increase in the concentrations of pro-inflammatory interleukins, e.g., IL-1beta, IL-2, IL-6, and TNF-alpha. From the clinical perspective, the conclusion that seems to be of particular importance is that in euthyroid patients with autoimmune thyroiditis and elevated levels of anti-thyroid antibodies, the incidence and severity of depression is significantly higher [8]. Treatment with both antidepressants and levothyroxine leads to a decrease in the level of pro-inflammatory cytokines, an increase in the level of BDNF, correlating with an improvement in clinical parameters of depression. Hence one of the hypotheses that depression may belong to the spectrum of inflammatory and degenerative disorders [102].
For the above reasons, patients with depression and anxiety disorders should be tested for autoimmune hypothyroidism, and patients with AHT should be screened for psychiatric symptoms [26]. However, it is necessary to broaden the scope and in-depth research, also conduct long-term studies (as our team is planning now) to determine the causal relationship between depression, thyroid autoantibodies, and cytokine levels, which would help us bring us closer to understanding the interrelationships between them and facilitate the use of adequate pharmacotherapy, not necessarily psychiatric. At the same time, it would be possible to identify groups at a higher risk of the occurrence of both frequent and very burdensome diseases, from a psychiatric perspective to help prevent the development of full-blown depression, and finally to predict the therapeutic response to treatment (drugs or groups of drugs).
Finally, we want to emphasize that our article has limitations: the results of the summary do not provide grounds for drawing clear conclusions due mainly to the fragmentary nature of the available data.
Author Contributions
Conceptualization, D.S.; methodology, D.S. and Z.K.; validation, D.S.; formal analysis, D.S. and Z.K.; investigation, Z.K. and D.S.; data curation, Z.K. and D.S.; writing—original draft preparation, Z.K. and D.S.; writing—review and editing, Z.K. and D.S.; visualization, Z.K. and D.S.; supervision, D.S.; project administration, Z.K. and D.S.; funding acquisition, D.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- van Boxtel, M.P.J.; Menheere, P.P.C.A.; Bekers, O.; Hogervorst, E.; Jolles, J. Thyroid Function, Depressed Mood, and Cognitive Performance in Older Individuals: The Maastricht Aging Study. Psychoneuroendocrinology 2004, 29, 891–898. [Google Scholar] [CrossRef]
- Hage, M.P.; Azar, S.T. The Link between Thyroid Function and Depression. J. Thyroid Res. 2012, 2012, 590648. [Google Scholar] [CrossRef]
- Kirkegaard, C.; Faber, J. The Role of Thyroid Hormones in Depression. Eur. J. Endocrinol. 1998, 138, 1–9. [Google Scholar] [CrossRef]
- Bhagwat, N.M.; Tayde, P.S.; Sharma, P.; Sharma, B.; Dalwadi, P.P.; Sonawane, A.; Subramanyam, A.; Chadha, M.; Varthakavi, P.K. Hypothyroidism and Depression: Are Cytokines the Link? Indian J. Endocrinol. Metab. 2017, 21, 886. [Google Scholar] [CrossRef] [PubMed]
- Boswell, E.B.; Anfinson, T.H.; Nemeroff, C.B. Depression Associated with Endocrine Disorder. In Depression and Physical Illness (Perspectives in Psychiatry Volume 6); Robertson, M.M., Katona, C.L.E., Eds.; John Wiley and Sons: Chichester, UK, 1996; pp. 256–292. [Google Scholar]
- Cleare, A.J.; McGregor, A.; O’Keane, V. Neuroendocrine Evidence for an Association between Hypothyroidism, Reduced Central 5-HT Activity and Depression. Clin. Endocrinol. (Oxf.) 1995, 43, 713–719. [Google Scholar] [CrossRef]
- Łojko, D.; Rybakowski, J. L-Thyroxine Augmentation of Serotonergic Antidepressants in Female Patients with Refractory Depression. J. Affect. Disord. 2007, 103, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Cooper-Kazaz, R.; Apter, J.T.; Cohen, R.; Karagichev, L.; Muhammed-Moussa, S.; Grupper, D.; Drori, T.; Newman, M.E.; Sackeim, H.A.; Glaser, B.; et al. Combined treatment with sertraline and liothyronine in major depression: A randomized, double-blind, placebo-controlled trial. Arch. Gen. Psychiatry 2007, 64, 679–688. [Google Scholar] [CrossRef]
- Kirim, S.; Keskek, S.Ö.; Köksal, F.; Haydardedeoglu, F.E.; Bozkirli, E.; Toledano, Y. Depression in Patients with Euthyroid Chronic Autoimmune Thyroiditis. Endocrine J. 2012, 59, 705–708. [Google Scholar] [CrossRef] [PubMed]
- Dunn, D.; Turner, C. Hypothyroidism in Women. Nurs. Womens Health 2016, 20, 93–98. [Google Scholar] [CrossRef]
- Massolt, E.T.; Effraimidis, G.; Korevaar, T.I.; Wiersinga, W.M.; Visser, W.E.; Peeters, R.P.; Drexhage, H.A. Aberrant Levels of Hematopoietic/Neuronal Growth and Differentiation Factors in Euthyroid Women at Risk for Autoimmune Thyroid Disease. PLoS ONE 2016, 11, e0153892. [Google Scholar] [CrossRef]
- Carta, M.G.; Hardoy, M.C.; Carpiniello, B.; Murru, A.; Marci, A.R.; Carbone, F.; Deiana, L.; Cadeddu, M.; Mariotti, S. A Case Control Study on Psychiatric Disorders in Hashimoto Disease and Euthyroid Goitre: Not Only Depressive but Also Anxiety Disorders are Associated with thyroid autoimmunity. Clin. Pract. Epidemiol. Ment. Health 2005, 1, 23. [Google Scholar] [CrossRef] [PubMed]
- Benros, M.E.; Waltoft, B.L.; Nordentoft, M.; Østergaard, S.D.; Eaton, W.W.; Krogh, J.; Mortensen, P.B. Autoimmune Diseases and Severe Infections as Risk Factors for Mood Disorders. JAMA Psychiatry 2013, 70, 812. [Google Scholar] [CrossRef] [PubMed]
- Carta, M.G.; Loviselli, A.; Hardoy, M.C.; Massa, S.; Cadeddu, M.; Sardu, C.; Carpiniello, B.; Dell’Osso, L.; Mariotti, S. The Link between Thyroid Autoimmunity (Antithyroid Peroxidase Autoantibodies) with Anxiety and Mood Disorders in the Community: A Field of Interest for Public Health in the Future. BMC Psychiatry 2004, 4, 25. [Google Scholar] [CrossRef] [PubMed]
- Nemeroff, C.B.; Simon, J.S.; Haggerty, J.J.; Evans, D.L. Antithyroid Antibodies in Depressed Patients. Am. J. Psychiatry 1985, 142, 840–843. [Google Scholar] [CrossRef]
- Joffe, R.T. Antithyroid Antibodies in Major Depression. Acta Psychiatr. Scand. 1987, 76, 598–599. [Google Scholar] [CrossRef] [PubMed]
- Kupka, R.W.; Nolen, W.A.; Post, R.M.; McElroy, S.L.; Altshuler, L.L.; Denicoff, K.D.; Frye, M.A.; Keck, P.E.; Leverich, G.S.; Rush, A.J.; et al. High Rate of Autoimmune Thyroiditis in Bipolar Disorder: Lack of Association with Lithium Exposure. Biol. Psychiatry 2002, 51, 305–311. [Google Scholar] [CrossRef]
- Padmos, R.C.; Bekris, L.; Knijff, E.M.; Tiemeier, H.; Kupka, R.W.; Cohen, D.; Nolen, W.A.; Lernmark, Å.; Drexhage, H.A. A High Prevalence of Organ-Specific Autoimmunity in Patients with Bipolar Disorder. Biol. Psychiatry 2004, 56, 476–482. [Google Scholar] [CrossRef]
- Vonk, R.; van der Schot, A.C.; Kahn, R.S.; Nolen, W.A.; Drexhage, H.A. Is Autoimmune Thyroiditis Part of the Genetic Vulnerability (or an Endophenotype) for Bipolar Disorder? Biol. Psychiatry 2007, 62, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Hillegers, M.H.J.; Reichart, C.G.; Wals, M.; Verhulst, F.C.; Ormel, J.; Nolen, W.A.; Drexhage, H.A. Signs of a Higher Prevalence of Autoimmune Thyroiditis in Female Offspring of Bipolar Parents. Eur. Neuropsychopharmacol. 2007, 17, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.N.; Iacovides, A.; Grammaticos, P.; St Kaprinis, G.; Bech, P. Thyroid Function in Clinical Subtypes of Major Depression: An Exploratory Study. BMC Psychiatry 2004, 4, 6. [Google Scholar] [CrossRef] [PubMed]
- Tsigos, C.; Chrousos, G.P. Hypothalamic–Pituitary–Adrenal Axis, Neuroendocrine Factors and Stress. J. Psychosom. Res. 2002, 53, 865–871. [Google Scholar] [CrossRef]
- Maes, M.; Meltzer, H.; Cosyns, P.; Suy, E.; Schotte, C. An Evaluation of Basal Hypothalamic-Pituitary-Thyroid Axis Function in Depression: Results of a Large-Scaled and Controlled Study. Psychoneuroendocrinology 1993, 18, 607–620. [Google Scholar] [CrossRef]
- Kuijpens, J.L.; Vader, H.L.; Drexhage, H.A.; Wiersinga, W.M.; van Son, M.J.; Pop, V.J. Thyroid Peroxidase Antibodies during Gestation Are a Marker for Subsequent Depression Postpartum. Eur. J. Endocrinol. 2001, 145, 579–584. [Google Scholar] [CrossRef]
- Elenkov, I.J.; Wilder, R.L.; Bakalov, V.K.; Link, A.A.; Dimitrov, M.A.; Fisher, S.; Crane, M.; Kanik, K.S.; Chrousos, G.P. IL-12, TNF-α, and Hormonal Changes during Late Pregnancy and Early Postpartum: Implications for Autoimmune Disease Activity during These Times. J. Clin. Endocrinol. Metabol. 2001, 86, 4933–4938. [Google Scholar] [CrossRef]
- Siegmann, E.-M.; Müller, H.H.; Luecke, C.; Philipsen, A.; Kornhuber, J.; Grömer, T.W. Association of Depression and Anxiety Disorders with Autoimmune Thyroiditis. A Systematic Review and Meta-analysis. JAMA Psychiatry 2018, 75, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Bode, H.; Ivens, B.; Bschor, T.; Schwarzer, G.; Henssler, J.; Baethge, C. Association of Hypothyroidism and Clinical Depression: A Systematic Review and Meta-Analysis. JAMA Psychiatry. 2021, 78, 1375–1383. [Google Scholar] [CrossRef] [PubMed]
- Shojaie, M.; Eshraghian, A. Primary Hypothyroidism Presenting with Torsades De Pointes Type Tachycardia: A Case Report. Cases J. 2008, 1, 298. [Google Scholar] [CrossRef] [PubMed]
- Pop, V.J.; Maartens, L.H.; Leusink, G.; van Son, M.J.; Knottnerus, A.A.; Ward, A.M.; Metcalfe, R.; Weetman, A.P. Are Autoimmune Thyroid Dysfunction and Depression Related? J. Clin. Endocrinol. Metab. 1998, 83, 3194–3197. [Google Scholar] [CrossRef] [PubMed]
- Zettinig, G.; Asenbaum, S.; Fueger, B.J.; Hofmann, A.; Diemling, M.; Mittlboeck, M.; Dudczak, R. Increased Prevalence of Sublinical Brain Perfusion Abnormalities in Patients with Autoimmune Thyroiditis: Evidence of Hashimoto’s Encephalitis? Clin. Endocrinol. (Oxf.) 2003, 59, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Engum, A.; Bjøro, T.; Mykletun, A.; Dahl, A.A. Thyroid Autoimmunity, Depression and Anxiety; Are There Any Connections? an Epidemiological Study of a Large Population. J. Psychosom. Res. 2005, 59, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Gulseren, S.; Gulseren, L.; Hekimsoy, Z.; Cetinay, P.; Ozen, C.; Tokatlioglu, B. Depression, Anxiety, Health-related Quality of Life, and Disability in Patients with Overt and Subclinical Thyroid Dysfunction. Arch. Med. Res. 2006, 37, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Bunevicius, R.; Peceliuniene, J.; Mickuviene, N.; Bunevicius, A.; Pop, V.J.; Girdler, S.S. Mood and Thyroid Immunity Assessed by Ultrasonographic Imaging in a Primary Health Care. J. Affect. Disord. 2007, 97, 85–90. [Google Scholar] [CrossRef][Green Version]
- van der Deure, W.M.; Appelhof, B.C.; Peeters, R.P.; Wiersinga, W.M.; Wekking, E.M.; Huyser, J.; Schene, A.H.; Tijssen, J.G.; Hoogendijk, W.J.; Visser, T.J.; et al. Polymorphisms in the Brain-specific Thyroid Hormone Transporter OATP1C1 are Associated with Fatigue and Depression in Hypothyroid Patients. Clin. Endocrinol. (Oxf.) 2008, 69, 804–811. [Google Scholar] [CrossRef]
- Schinhammer, S. Untersuchung Möglicher Zusammenhänge Zwischen Hashimoto-Thyreoiditis, Psychischen Störungen und Genetischen Varianten des Adenosinsystems; Friedrich-Alexander-Universität: Erlangen-Nürnberg, Germany, 2010. [Google Scholar]
- Watt, T.; Hegedüs, L.; Bjorner, J.B.; Groenvold, M.; Bonnema, S.J.; Rasmussen, A.K.; Feldt-Rasmussen, U. Is Thyroid Autoimmunity per se a Determinant of Quality of Life in Patients with Autoimmune Hypothyroidism? Eur. Thyroid J. 2012, 1, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Franke, J.C. Untersuchungen zur Entwicklung von Depression und Angststörungen bei Hashimoto-Thyreoiditis; Friedrich-Alexander-Universität: Erlangen-Nürnberg, Germany, 2013. [Google Scholar]
- Giynas Ayhan, M.; Uguz, F.; Askin, R.; Gonen, M.S. The Prevalence of Depression and Anxiety Disorders in Patients with Euthyroid Hashimoto’s Thyroiditis: A Comparative Study. Gen. Hosp. Psychiatry 2014, 36, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Medici, M.; Direk, N.; Visser, W.E.; Korevaar, T.I.; Hofman, A.; Visser, T.J.; Tiemeier, H.; Peeters, R.P. Thyroid Function within the Normal Range and the Risk of Depression: A Population-based Cohort Study. J. Clin. Endocrinol. Metab. 2014, 99, 1213–1219. [Google Scholar] [CrossRef] [PubMed]
- Demartini, B.; Ranieri, R.; Masu, A.; Selle, V.; Scarone, S.; Gambini, O. Depressive Symptoms and Major Depressive Disorder in Patients Affected by Subclinical Hypothyroidism: A Cross-sectional Study. J. Nerv. Ment. Dis. 2014, 202, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Quinque, E.M. Brain, Mood and Cognition in Hypothyroidism; Max-Planck-Institut für Kognitions-und Neurowissenschaften: Leipzig, Germany, 2015. [Google Scholar]
- Ittermann, T.; Völzke, H.; Baumeister, S.E.; Appel, K.; Grabe, H.J. Diagnosed Thyroid Disorders are Associated with Depression and Anxiety. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1417–1425. [Google Scholar] [CrossRef]
- Fjaellegaard, K.; Kvetny, J.; Allerup, P.N.; Bech, P.; Ellervik, C. Well-being and Depression in Individuals with Subclinical Hypothyroidism and Thyroid Autoimmunity—A General Population Study. Nord. J. Psychiatry 2015, 69, 73–78. [Google Scholar] [CrossRef] [PubMed]
- van de Ven, A.C. Towards an Optimal TSH Level: Different Goals for Different Outcomes and for Different Populations? Radboud Universiteit Nijmegen: Nijmegen, The Netherlands, 2016. [Google Scholar]
- Krysiak, R.; Drosdzol-Cop, A.; Skrzypulec-Plinta, V.; Okopien, B. Sexual Function and Depressive Symptoms in Young Women with Thyroid Autoimmunity and Subclinical Hypothyroidism. Clin. Endocrinol. (Oxf.) 2016, 84, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Delitala, A.P.; Terracciano, A.; Fiorillo, E.; Orrù, V.; Schlessinger, D.; Cucca, F. Depressive Symptoms, Thyroid Hormone and Autoimmunity in a Population-based Cohort from Sardinia. J. Affect. Disord. 2016, 191, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Yalcin, M.M.; Altinova, A.E.; Cavnar, B.; Bolayir, B.; Akturk, M.; Arslan, E.; Ozkan, C.; Cakir, N.; Balos Toruner, F. Is Thyroid Autoimmunity Itself Associated with Psychological Well-being in Euthyroid Hashimoto’s Thyroiditis? Endocr. J. 2017, 64, 425–442. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Oh, S.S.; Park, E.C.; Jang, S.I. Sex Differences in the Association Between Thyroid-Stimulating Hormone Levels and Depressive Symptoms among the General Population with Normal Free T4 Levels. J. Affect. Disord. 2019, 249, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Dersch, R.; van Elst, L.T.; Hochstuhl, B.; Fiebich, B.L.; Stich, O.; Robinson, T.; Matysik, M.; Michel, M.; Runge, K.; Nickel, K.; et al. Anti-Thyroid Peroxidase and Anti-Thyroglobulin Autoantibodies in the Cerebrospinal Fluid of Patients with Unipolar Depression. J. Clin. Med. 2020, 9, 2391. [Google Scholar] [CrossRef] [PubMed]
- Minaldi, E.; D’Andrea, S.; Castellini, C.; Martorella, A.; Francavilla, F.; Francavilla, S.; Barbonetti, A. Thyroid Autoimmunity and Risk of Post-partum Depression: A Systematic Review and Meta-analysis of Longitudinal Studies. J. Endocrinol. Investig. 2020, 43, 271–277. [Google Scholar] [CrossRef]
- Hirtz, R.; Föcker, M.; Libuda, L.; Antel, J.; Öztürk, D.; Kiewert, C.; Munteanu, M.; Peters, T.; Führer, D.; Zwanziger, D.; et al. Increased Prevalence of Subclinical Hypothyroidism and Thyroid Autoimmunity in Depressed Adolescents: Results from a Clinical Cross-Sectional Study in Comparison to the General Pediatric Population. J. Clin. Psychiatry 2021, 82, 20m13511. [Google Scholar] [CrossRef] [PubMed]
- Kamyshna, I.I.; Pavlovych, L.B.; Kamyshnyi, A.M. Association Between NMDA Gene Polymorphism (rs4880213) and GRIN2B Blood Serum Levels in Thyroid Pathology Patients. J. Med. Life 2022, 15, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctôt, K.L. A Meta-Analysis of Cytokines in Major Depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef]
- Konca Degertekin, C.; Aktas Yilmaz, B.; Balos Toruner, F.; Kalkanci, A.; Turhan Iyidir, O.; Fidan, I.; Yesilyurt, E.; Cakır, N.; Kustimur, S.; Arslan, M. Circulating Th17 Cytokine Levels Are Altered in Hashimoto’s Thyroiditis. Cytokine 2016, 80, 13–17. [Google Scholar] [CrossRef]
- Fam, J.; Rush, A.J.; Burt, T.; Chan, E.S.; Siddiqui, F.J.; Assam, P.N.; Lai, O.F.; Chan, H.N.; Ng, B.Y.; Khoo, D.H. Thyroid Autoimmune Antibodies and Major Depressive Disorder in Women. Ann. Acad. Med. Singap. 2015, 44, 284–289. [Google Scholar]
- Ajjan, R.A.; Weetman, A.P. Cytokines in Thyroid Autoimmunity. Autoimmunity 2003, 36, 351–359. [Google Scholar] [CrossRef]
- Banks, W.A.; Kastin, A.J.; Broadwell, R.D. Passage of Cytokines Across the Blood-Brain Barrier. Neuroimmunomodulation 1995, 2, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Banks, W.A.; Farr, S.A.; Morley, J.E. Entry of Blood-Borne Cytokines into the Central Nervous System: Effects on Cognitive Processes. Neuroimmunomodulation 2002, 10, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Dantzer, R. Cytokine-induced Sickness Behavior: Where Do We Stand? Brain Behav. Immun. 2001, 15, 7–24. [Google Scholar] [CrossRef] [PubMed]
- Malberg, J.E.; Eisch, A.J.; Nestler, E.J.; Duman, R.S. Chronic Antidepressant Treatment Increases Neurogenesis in Adult Rat Hippocampus. J. Neurosci. 2000, 20, 9104–9110. [Google Scholar] [CrossRef]
- Saarelainen, T.; Hendolin, P.; Lucas, G.; Koponen, E.; Sairanen, M.; MacDonald, E.; Agerman, K.; Haapasalo, A.; Nawa, H.; Aloyz, R.; et al. Activation of the TrkB Neurotrophin Receptor Is Induced by Antidepressant Drugs and Is Required for Antidepressant-Induced Behavioral Effects. J. Neurosci. 2003, 23, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Ekdahl, C.T.; Claasen, J.-H.; Bonde, S.; Kokaia, Z.; Lindvall, O. Inflammation Is Detrimental for Neurogenesis in Adult Brain. Proc. Natl. Acad. Sci. USA 2003, 100, 13632–13637. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.; Marriott, M.; Nahmias, C.; MacQueen, G.M. Lower Hippocampal Volume in Patients Suffering From Depression: A Meta-Analysis. Am. J. Psychiatry 2004, 161, 598–607. [Google Scholar] [CrossRef]
- Seeler, M.J.; Christiansen, K.; Wegmann, R.; Bohnet, H.G. Persönlichkeitsmerkmale, körperliche Beschwerden und mikrosomaler Schilddrüsen-Antikörper-Titer bei frisch entbundenen Frauen [Personality markers, physical complaints and microsomal thyroid antibody titer in postpartum women]. Z. Geburtshilfe Neonatol. 1996, 200, 138–143. (In German) [Google Scholar]
- Baldissarelli, J.; Mânica, A.; Pillat, M.M.; Bagatini, M.D.; Leal, D.B.; Abdalla, F.H.; Morsch, V.M.; Ulrich, H.; Bornemann, C.P.; Chitolina Schetinger, M.R. Increased Cytokines Production and Oxidative Stress Are Related with Purinergic Signaling and Cell Survival in Post-Thyroidectomy Hypothyroidism. Mol. Cell. Endocrinol. 2020, 499, 110594. [Google Scholar] [CrossRef]
- Marchiori, R.C.; Pereira, L.A.; Naujorks, A.A.; Rovaris, D.L.; Meinerz, D.F.; Duarte, M.M.; Rocha, J.B. Improvement of Blood Inflammatory Marker Levels in Patients with Hypothyroidism under Levothyroxine Treatment. BMC Endocr. Disord. 2015, 15, 32. [Google Scholar] [CrossRef] [PubMed]
- Mikoś, H.; Mikoś, M.; Obara-Moszyńska, M.; Niedziela, M. The Role of the Immune System and Cytokines Involved in the Pathogenesis of Autoimmune Thyroid Disease (AITD). Endokrynol. Pol. 2014, 65, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Chiou, S.-H.; Chen, S.-J.; Peng, C.-H.; Chang, Y.-L.; Ku, H.-H.; Hsu, W.-M.; Ho, L.L.-T.; Lee, C.-H. Fluoxetine Up-Regulates Expression of Cellular FLICE-Inhibitory Protein and Inhibits LPS-Induced Apoptosis in Hippocampus-Derived Neural Stem Cell. Biochem. Biophys. Res. Commun. 2006, 343, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, J.L.; Ignatowski, T.A.; Sud, R.; Spengler, R.N. An Antidepressant Mechanism of Desipramine Is to Decrease Tumor Necrosis Factor-α Production Culminating in Increases in Noradrenergic Neurotransmission. Neuroscience 2005, 133, 519–531. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, J.L.; Ignatowski, T.A.; Sud, R.; Spengler, R.N. Brain-Derived Tumor Necrosis Factor-α and Its Involvement in Noradrenergic Neuron Functioning Involved in the Mechanism of Action of an Antidepressant. J. Pharmacol. Exp. Ther. 2004, 310, 1216–1225. [Google Scholar] [CrossRef]
- Karakatsoulis, G.N.; Tsapakis, E.M.; Mitkani, C.; Fountoulakis, K.N. Subclinical Thyroid Dysfunction and Major Depressive Disorder. Hormones (Athens) 2021, 20, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Eker, S.S.; Akkaya, C.; Sarandol, A.; Cangur, S.; Sarandol, E.; Kirli, S. Effects of Various Antidepressants on Serum Thyroid Hormone Levels in Patients with Major Depressive Disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Caye, A.; Pilz, L.K.; Maia, A.L.; Hidalgo, M.P.; Furukawa, T.A.; Kieling, C. The Impact of Selective Serotonin Reuptake Inhibitors on the Thyroid Function Among Patients with Major Depressive Disorder: A Systematic Review and Meta-Analysis. Eur. Neuropsychopharmacol. 2020, 33, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Maia, A.L.; Goemann, I.M.; Meyer, E.L.; Wajner, S.M. Deiodinases: The Balance of Thyroid Hormone: Type 1 Iodothyronine Deiodinase in Human Physiology and Disease. J. Endocrinol. 2011, 209, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Yuan, F.; Yuan, R.; Ren, D.; Bi, Y.; Niu, W.; Guo, Z.; Wu, X.; Xu, F.; Sun, Q.; Ma, G.; et al. A Novel NR3C2 Polymorphism and The Increased Thyroid-Stimulating Hormone Concentration are Associated with Venlafaxine Treatment Outcome in Chinese Han MDD Patients. Psychiatry Res. 2020, 284, 112690. [Google Scholar] [CrossRef] [PubMed]
- Riepe, F.G.; Finkeldei, J.; de Sanctis, L.; Einaudi, S.; Testa, A.; Karges, B.; Peter, M.; Viemann, M.; Grötzinger, J.; Sippell, W.G.; et al. Elucidating the Underlying Molecular Pathogenesis of NR3C2 Mutants Causing Autosomal Dominant Pseudohypoaldosteronism Type 1. J. Clin. Endocrinol. Metab. 2006, 91, 4552–4561. [Google Scholar] [CrossRef] [PubMed]
- Papakostas, G.I.; Cooper-Kazaz, R.; Appelhof, B.C.; Posternak, M.A.; Johnson, D.P.; Klibanski, A.; Lerer, B.; Fava, M. Simultaneous Initiation (Coinitiation) of Pharmacotherapy with Triiodothyronine and A Selective Serotonin Reuptake Inhibitor for Major Depressive Disorder: A Quantitative Synthesis of Double-Blind Studies. Int. Clin. Psychopharmacol. 2009, 24, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, J.B.; Aftab, A.; Radhakrishnan, R.; Widge, A.; Rodriguez, C.I.; Carpenter, L.L.; Nemeroff, C.B.; McDonald, W.M.; Kalin, N.H. APA Council of Research Task Force on Novel Biomarkers and Treatments. Hormonal Treatments for Major Depressive Disorder: State of the Art. Am. J. Psychiatry 2020, 177, 686–705. [Google Scholar] [CrossRef]
- Müller, N.; Riedel, M.; Schwarz, M.J. Psychotropic Effects of COX-2 Inhibitors—A Possible New Approach for the Treatment of Psychiatric Disorders. Pharmacopsychiatry 2004, 37, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Müller, N.; Schwarz, M.J.; Dehning, S.; Douhe, A.; Cerovecki, A.; Goldstein-Müller, B.; Spellmann, I.; Hetzel, G.; Maino, K.; Kleindienst, N.; et al. The Cyclooxygenase-2 Inhibitor Celecoxib Has Therapeutic Effects in Major Depression: Results of a Double-Blind, Randomized, Placebo Controlled, Add-on Pilot Study to Reboxetine. Mol. Psychiatry 2006, 11, 680–684. [Google Scholar] [CrossRef] [PubMed]
- Bavaresco, D.V.; Uggioni, M.; Ferraz, S.D.; Marques, R.; Simon, C.S.; Dagostin, V.S.; Grande, A.J.; da Rosa, M.I. Efficacy of Infliximab in Treatment-Resistant Depression: A Systematic Review and Meta-Analysis. Pharmacol. Biochem. Behav. 2020, 188, 172838. [Google Scholar] [CrossRef] [PubMed]
- Menter, A.; Augustin, M.; Signorovitch, J.; Yu, A.P.; Wu, E.Q.; Gupta, S.R.; Bao, Y.; Mulani, P. The Effect of Adalimumab on Reducing Depression Symptoms in Patients with Moderate to Severe Psoriasis: A Randomized Clinical Trial. J. Am. Acad. Dermatol. 2010, 62, 812–818. [Google Scholar] [CrossRef]
- Gordon, K.B.; Armstrong, A.W.; Han, C.; Foley, P.; Song, M.; Wasfi, Y.; You, Y.; Shen, Y.K.; Reich, K. Anxiety and Depression in Patients with Moderate-to-Severe Psoriasis and Comparison of Change from Baseline After Treatment with Guselkumab vs. Adalimumab: Results from The Phase 3 VOYAGE 2 Study. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1940–1949. [Google Scholar] [CrossRef] [PubMed]
- Tiosano, S.; Yavne, Y.; Watad, A.; Langevitz, P.; Lidar, M.; Feld, J.; Tishler, M.; Aamar, S.; Elkayam, O.; Balbir-Gurman, A.; et al. The Impact of Tocilizumab on Anxiety and Depression in Patients with Rheumatoid Arthritis. Eur. J. Clin. Investig. 2020, 50, e13268. [Google Scholar] [CrossRef] [PubMed]
- Behrens, F.; Burmester, G.R.; Feuchtenberger, M.; Kellner, H.; Kuehne, C.; Liebhaber, A.; Wassenberg, S.; Gerlach, J.; Zortel, M.; Hofmann, M.W.; et al. Characterisation of Depressive Symptoms in Rheumatoid Arthritis Patients Treated with Tocilizumab During Routine Daily Care. Clin. Exp. Rheumatol. 2021; Online ahead of print. [Google Scholar]
- Knight, J.M.; Costanzo, E.S.; Singh, S.; Yin, Z.; Szabo, A.; Pawar, D.S.; Hillard, C.J.; Rizzo, J.D.; D’Souza, A.; Pasquini, M.; et al. The IL-6 Antagonist Tocilizumab is Associated with Worse Depression and Related Symptoms in The Medically Ill. Transl. Psychiatry 2021, 11, 58. [Google Scholar] [CrossRef] [PubMed]
- Steeland, S.; Libert, C.; Vandenbroucke, R.E. A New Venue of TNF Targeting. Int. J. Mol. Sci. 2018, 19, 1442. [Google Scholar] [CrossRef] [PubMed]
- Paschou, S.A.; Palioura, E.; Kothonas, F.; Myroforidis, A.; Loi, V.; Poulou, A.; Goumas, K.; Effraimidis, G.; Vryonidou, A. The Effect of Anti-TNF Therapy on Thyroid Function in Patients with Inflammatory Bowel Disease. Endocr. J. 2018, 65, 1121–1125. [Google Scholar] [CrossRef] [PubMed]
- Akinci, B.; Comlekci, A.; Yener, S.; Bayraktar, F.; Demir, T.; Ozcan, M.A.; Yuksel, F.; Yesil, S. Hashimoto’s Thyroiditis, but not Treatment of Hypothyroidism, is Associated with Altered TGF-beta1 Levels. Arch. Med. Res. 2008, 39, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Mon, M.A.; Gomez-Lahoz, A.M.; Orozco, A.; Lahera, G.; Sosa-Reina, M.D.; Diaz, D.; Albillos, A.; Quintero, J.; Molero, P.; Monserrat, J.; et al. Blunted Expansion of Regulatory T Lymphocytes Is Associated with Increased Bacterial Translocation in Patients with Major Depressive Disorder. Front. Psychiatry 2021, 11, 591962. [Google Scholar] [CrossRef] [PubMed]
- Małczyńska, P.; Piotrowicz, Z.; Drabarek, D.; Langfort, J.; Chalimoniuk, M. The Role of the Brain-Derived Neurotrophic Factor (BDNF) in Neurodegenerative Processes and in the Neuroregeneration Mechanisms Induced by Increased Physical Activity. Postepy Biochem. 2019, 65, 2–8. [Google Scholar] [CrossRef]
- Shirayama, Y.; Chen, A.C.-H.; Nakagawa, S.; Russell, D.S.; Duman, R.S. Brain-Derived Neurotrophic Factor Produces Antidepressant Effects in Behavioral Models of Depression. J. Neurosci. 2002, 22, 3251–3261. [Google Scholar] [CrossRef] [PubMed]
- Matrisciano, F.; Bonaccorso, S.; Ricciardi, A.; Scaccianoce, S.; Panaccione, I.; Wang, L.; Ruberto, A.; Tatarelli, R.; Nicoletti, F.; Girardi, P.; et al. Changes in BDNF Serum Levels in Patients with Major Depression Disorder (MDD) after 6 Months Treatment with Sertraline, Escitalopram, or Venlafaxine. J. Psychiatr. Res. 2009, 43, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, Y.; Rizavi, H.S.; Conley, R.R.; Roberts, R.C.; Tamminga, C.A.; Pandey, G.N. Altered Gene Expression of Brain-Derived Neurotrophic Factor and Receptor Tyrosine Kinase B in Postmortem Brain of Suicide Subjects. Arch. Gen. Psychiatry 2003, 60, 804–815. [Google Scholar] [CrossRef]
- Huang, T.-L.; Lee, C.-T.; Liu, Y.-L. Serum Brain-Derived Neurotrophic Factor Levels in Patients with Major Depression: Effects of Antidepressants. J. Psychiatr. Res. 2008, 42, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Kavalali, E.T.; Monteggia, L.M. Synaptic Mechanisms Underlying Rapid Antidepressant Action of Ketamine. Am. J. Psychiatry 2012, 169, 1150–1156. [Google Scholar] [CrossRef] [PubMed]
- Lasley, S.M.; Gilbert, M.E. Developmental Thyroid Hormone Insufficiency Reduces Expression of Brain-Derived Neurotrophic Factor (BDNF) in Adults but Not in Neonates. Neurotoxicol. Teratol. 2011, 33, 464–472. [Google Scholar] [CrossRef]
- Hung, P.-L.; Huang, C.-C.; Huang, H.-M.; Tu, D.-G.; Chang, Y.-C. Thyroxin Treatment Protects Against White Matter Injury in The Immature Brain via Brain-Derived Neurotrophic Factor. Stroke 2013, 44, 2275–2283. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.H.; Kang, E.-S.; Fava, M.; Mischoulon, D.; Nierenberg, A.A.; Lee, D.; Heo, J.-Y.; Jeon, H.J. Thyroid Stimulating Hormone and Serum, Plasma, and Platelet Brain-Derived Neurotrophic Factor during a 3-Month Follow-up in Patients with Major Depressive Disorder. J. Affect. Disord. 2014, 169, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, M.; Altshuler, L.L.; Frye, M.A.; Suri, R.; Huynh, E.L.; Fairbanks, L.; Bauer, M.; Korenman, S. Peripheral Thyroid Hormones and Response to Selective Serotonin Reuptake Inhibitors. J. Psychiatry Neurosci. 2004, 29, 383–386. [Google Scholar] [PubMed]
- Cavus, I.; Duman, R.S. Influence of Estradiol, Stress, and 5-HT2A Agonist Treatment on Brain-Derived Neurotrophic Factor Expression in Female Rats. Biol. Psychiatry 2003, 54, 59–69. [Google Scholar] [CrossRef]
- Maes, M.; Bosmans, E.; Meltzer, H.Y.; Scharpé, S.; Suy, E. Interleukin-1 Beta: A Putative Mediator of HPA Axis Hyperactivity in Major Depression? Am. J. Psychiatry 1993, 150, 1189–1193. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).