

Hyaluronic Acid-Based Injective Medical Devices: In Vitro Characterization of Novel Formulations Containing Biofermentative Unsulfated Chondroitin or Extractive Sulfated One with Cyclodextrins

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Results
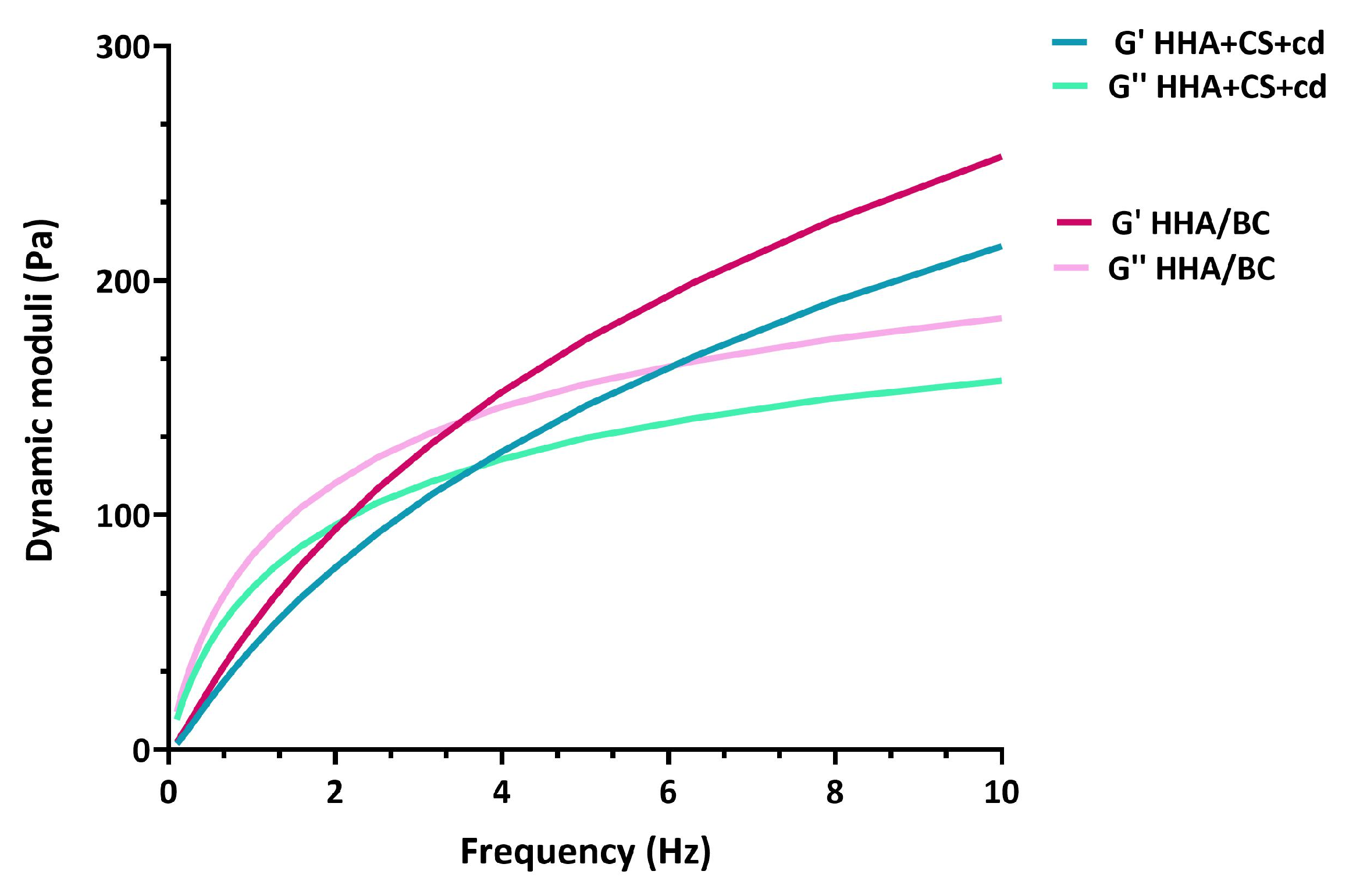
2.1. Rheological Characterization
2.2. Sample Enzymatic Degradation
2.3. Cellular Viability Assay
2.4. Gene Expression Analyses via qRT-PCR
2.5. Protein Analyses via Western Blotting
2.6. Immunofluorescence Analyses
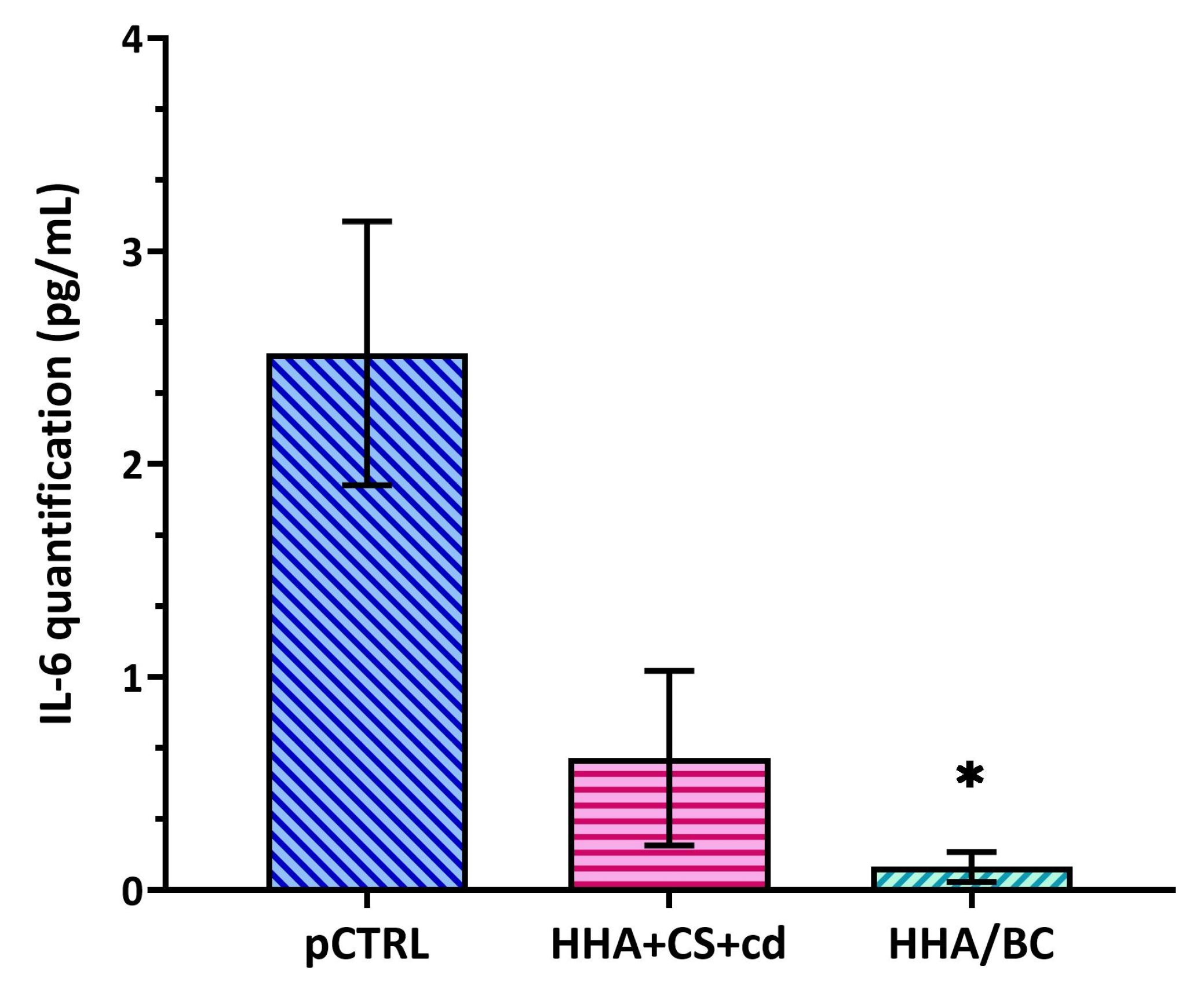
2.7. ELISA Assay
3. Discussion
4. Materials and Methods
4.1. Class III Medical Device Based on HA and CS or BC
4.2. Rheological Characterization
4.3. Gels Susceptibility to Hyaluronidases
4.4. OA In Vitro Model Setup
4.5. Cellular Viability Assay
4.6. Gene Expression Analyses via qRT-PCR
4.7. Protein Analyses via Western Blotting
4.8. Immunofluorescence Analyses
4.9. ELISA Assay
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Zhu, X.; Sang, L.; Wu, D.; Rong, J.; Jiang, L. Effectiveness and safety of glucosamine and chondroitin for the treatment of osteoarthritis: A meta-analysis of randomized controlled trials. J. Orthop. Surg. Res. 2018, 13, 17. [Google Scholar] [CrossRef] [PubMed]
- Majeed, M.H.; Sherazi, S.A.A.; Bacon, D.; Bajwa, Z.H. Pharmacological Treatment of Pain in Osteoarthritis: A Descriptive Review. Curr. Rheumatol. Rep. 2018, 20, 88. [Google Scholar] [CrossRef] [PubMed]
- McAlindon, T.E.; LaValley, M.P.; Gulin, J.P.; Felson, D.T. Glucosamine and chondroitin for treatment of osteoarthritis: A systematic quality assessment and meta-analysis. JAMA 2000, 283, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Sharma, L. Osteoarthritis of the Knee. N. Engl. J. Med. 2021, 384, 51–59. [Google Scholar] [CrossRef]
- Glyn-Jones, S.; Palmer, A.J.; Agricola, R.; Price, A.J.; Vincent, T.L.; Weinans, H.; Carr, A.J. Osteoarthritis. Lancet 2015, 386, 376–387. [Google Scholar] [CrossRef]
- Chen, Y.J.; Chang, W.A.; Wu, L.Y.; Huang, C.F.; Chen, C.H.; Kuo, P.L. Identification of Novel Genes in Osteoarthritic Fibroblast-Like Synoviocytes Using Next-Generation Sequencing and Bioinformatics Approaches. Int. J. Med. Sci. 2019, 16, 1057–1071. [Google Scholar] [CrossRef]
- Arden, N.K.; Perry, T.A.; Bannuru, R.R.; Bruyère, O.; Cooper, C.; Haugen, I.K.; Hochberg, M.C.; McAlindon, T.E.; Mobasheri, A.; Reginster, J.-Y. Non-surgical management of knee osteoarthritis: Comparison of ESCEO and OARSI 2019 guidelines. Nat. Rev. Rheumatol. 2021, 17, 59–66. [Google Scholar] [CrossRef]
- Russo, F.; D’Este, M.; Vadalà, G.; Cattani, C.; Papalia, R.; Alini, M.; Denaro, V. Platelet Rich Plasma and Hyaluronic Acid Blend for the Treatment of Osteoarthritis: Rheological and Biological Evaluation. PLoS ONE 2016, 16, 11. [Google Scholar] [CrossRef]
- Lei, Q.; Zhang, G.; Kuang, X.; Wang, Q.; Fan, F. Functional biomaterials for osteoarthritis treatment: From research to application. Smart Med. 2022, 1, e20220014. [Google Scholar] [CrossRef]
- Yang, L.; Sun, L.; Zhang, H.; Bian, F.; Zhao, Y. Ice-Inspired Lubricated Drug Delivery Particles from Microfluidic Electrospray for Osteoarthritis Treatment. ACS Nano 2021, 15, 20600–20606. [Google Scholar] [CrossRef]
- Liu, Z.; Fan, B.; Zhao, J.; Yang, B.; Zheng, X. Benzothiazole derivatives-based supramolecular assemblies as efficient corrosion inhibitors for copper in artificial seawater: Formation, interfacial release and protective mechanisms. Corros. Sci. 2023, 212, 110957. [Google Scholar] [CrossRef]
- Tamer, T.M. Hyaluronan and synovial joint: Function, distribution and healing. Interdiscip. Toxicol. 2013, 6, 111–125. [Google Scholar] [CrossRef] [PubMed]
- Balazs, E.A. Viscosupplementation for treatment of osteoarthritis: From initial discovery to current status and results. Surg. Technol. Online 2004, 12, 278–289. [Google Scholar]
- Lin, W.; Liu, Z.; Kampf, N.; Klein, J. The Role of Hyaluronic Acid in Cartilage Boundary Lubrication. Cells 2020, 9, 1606. [Google Scholar] [CrossRef]
- Volpi, N. Chondroitin Sulfate Safety and Quality. Molecules 2019, 24, 1447. [Google Scholar] [CrossRef]
- Volpi, N. Quality of different chondroitin sulfate preparations in relation to their therapeutic activity. J. Pharm. Pharmacol. 2009, 61, 1271–1280. [Google Scholar] [CrossRef] [PubMed]
- Esko, J.D.; Kimata, K.; Lindahl, U. Proteoglycans and Sulfated Glycosaminoglycans. In Essentials of Glycobiology, 2nd ed.; Varki, A., Cummings, R.D., Esko, J.D., Freeze, H.H., Stanley, P., Bertozzi, C.R., Hart, G.W., Etzler, M.E., Eds.; Cold Spring Harbor Laboratory Press: Cold Spring Harbor, NY, USA, 2009; Chapter 16. [Google Scholar]
- David-Raoudi, M.; Deschrevel, B.; Leclercq, S.; Galéra, P.; Boumediene, K.; Pujol, J.-P. Chondroitin sulfate increases hyaluronan production by human synoviocytes through differential regulation of hyaluronan synthases: Role of p38 and Akt. Arthritis Rheum. 2009, 60, 760–770. [Google Scholar] [CrossRef]
- Stellavato, A.; Restaino, O.F.; Vassallo, V.; Cassese, E.; Finamore, R.; Ruosi, C.; Schiraldi, C. Chondroitin Sulfate in USA Dietary Supplements in Comparison to Pharma Grade Products: Analytical Fingerprint and Potential Anti-Inflammatory Effect on Human Osteoartritic Chondrocytes and Synoviocytes. Pharmaceutics 2021, 13, 737. [Google Scholar] [CrossRef]
- Simental-Mendía, M.; Sánchez-García, A.; Vilchez-Cavazos, F.; Acosta-Olivo, C.A.; Peña-Martínez, V.M.; Simental-Mendía, L.E. Effect of glucosamine and chondroitin sulfate in symptomatic knee osteoarthritis: A systematic review and meta-analysis of randomized placebo-controlled trials. Rheumatol. Int. 2018, 38, 1413–1428. [Google Scholar] [CrossRef]
- Henrotin, Y.; Marty, M.; Mobasheri, A. What is the current status of chondroitin sulfate and glucosamine for the treatment of knee osteoarthritis? Maturitas 2014, 78, 184–187, Erratum in Maturitas 2014, 79, 487. [Google Scholar] [CrossRef]
- Mishra, S.; Ganguli, M. Functions of, and replenishment strategies for, chondroitin sulfate in the human body. Drug Discov. Today 2021, 26, 1185–1199. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.C.; Ke, Y.L.; Lai, Y.H.; Hsieh, W.C.; Lin, C.H.; Huang, S.S.; Peng, J.Y.; Chen, C.H. Chondroitin Sulfate Enhances Proliferation and Migration via Inducing β-Catenin and Intracellular ROS as Well as Suppressing Metalloproteinases through Akt/NFκB Pathway Inhibition in Human Chondrocytes. J. Nutr. Health Aging 2022, 26, 307–313. [Google Scholar] [CrossRef]
- Živanović, S.; Rackov, L.P.; Živanović, A.; Jevtić, M.; Nikolić, S.; Kocić, S. Cartilage Oligomeric Matrix Protein—Inflammation biomarker in knee osteoarthritis. Bosn. J. Basic Med. Sci. 2011, 11, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Vallières, M.; du Souich, P. Modulation of inflammation by chondroitin sulfate. Osteoarthr. Cartil. 2010, 18, S1–S6. [Google Scholar] [CrossRef]
- Iovu, M.; Dumais, G.; du Souich, P. Anti-inflammatory activity of chondroitin sulfate. Osteoarthr. Cartil. 2008, 16 (Suppl. S3), S14–S18. [Google Scholar] [CrossRef]
- Henrotin, Y.; Hauzeur, J.-P.; Bruel, P.; Appelboom, T. Intra-articular use of a medical device composed of hyaluronic acid and chondroitin sulfate (Structovial CS): Effects on clinical, ultrasonographic and biological parameters. BMC Res. Notes 2012, 5, 407. [Google Scholar] [CrossRef]
- Rivera, F.; Bertignone, L.; Grandi, G.; Camisassa, R.; Comaschi, G.; Trentini, D.; Zanone, M.; Teppex, G.; Vasario, G.; Fortina, G. Effectiveness of intra-articular injections of sodium hyaluronate-chondroitin sulfate in knee osteoarthritis: A multicenter prospective study. J. Orthop. Traumatol. 2016, 17, 27–33, Erratum in J. Orthop. Traumatol. 2016, 17, 95. [Google Scholar] [CrossRef] [PubMed]
- Pavelka, K.; Horváth, R.; Hurnáková, J.; Saracino, L.; Giordan, N.; Procházková, L.; Moster, E.; Dokoupilová, E. Clinical effectiveness and safety of intra-articular injection of HYALGO in the management of knee osteoarthritis symptoms: A multicenter prospective study. J. Clin. Orthop. Trauma 2021, 19, 75–80. [Google Scholar] [CrossRef]
- Laurent, C.; Hellström, S. Extracellular matrix components reflect the dynamics of a healing tympanic membrane perforation—A histochemical study. Int. J. Biochem. Cell Biol. 1997, 29, 221–229. [Google Scholar] [CrossRef]
- D’ambrosio, S.; Alfano, A.; Cassese, E.; Restaino, O.F.; Ferraiuolo, S.B.; Finamore, R.; Cammarota, M.; Schiraldi, C.; Cimini, D. Production and purification of higher molecular weight chondroitin by metabolically engineered Escherichia coli K4 strains. Sci. Rep. 2020, 10, 13200. [Google Scholar] [CrossRef]
- Vassallo, V.; Stellavato, A.; Russo, R.; Cimini, D.; Valletta, M.; Alfano, A.; Pedone, P.V.; Chambery, A.; Schiraldi, C. Molecular Fingerprint of Human Pathological Synoviocytes in Response to Extractive Sulfated and Biofermentative Unsulfated Chondroitins. Int. J. Mol. Sci. 2022, 23, 15865. [Google Scholar] [CrossRef] [PubMed]
- Papalia, R.; Salini, V.; Voglino, N.; Fortina, M.; Carta, S.; Sadile, F.; Costantino, C. Single-Dose Intra-Articular Administration of a Hybrid Cooperative Complex of Sodium Hyaluronate and Sodium Chondroitin in the Treatment of Symptomatic Hip Osteoarthritis: A Single-Arm, Open-Label, Pilot Study. Rheumatol. Ther. 2021, 8, 151–165. [Google Scholar] [CrossRef]
- Alessio, N.; Stellavato, A.; Aprile, D.; Cimini, D.; Vassallo, V.; Di Bernardo, G.; Galderisi, U.; Schiraldi, C. Timely Supplementation of Hydrogels Containing Sulfated or Unsulfated Chondroitin and Hyaluronic Acid Affects Mesenchymal Stromal Cells Commitment Toward Chondrogenic Differentiation. Front. Cell Dev. Biol. 2021, 9, 641529. [Google Scholar] [CrossRef]
- Vassallo, V.; Tsianaka, A.; Alessio, N.; Grübel, J.; Cammarota, M.; Tovar, G.E.M.; Southan, A.; Schiraldi, C. Evaluation of novel biomaterials for cartilage regeneration based on gelatin methacryloyl interpenetrated with extractive chondroitin sulfate or unsulfated biotechnological chondroitin. J. Biomed. Mater. Res. Part A 2022, 110, 1210–1223. [Google Scholar] [CrossRef] [PubMed]
- Agiba, A.M. Nutraceutical formulations containing glucosamine and chondroitin sulphate in the treatment of osteoarthritis: Emphasis on clinical efficacy and formulation challenges. Int. J. Curr. Pharm. Res. 2017, 9, 1. [Google Scholar] [CrossRef]
- Terencio, M.C.; Ferrándiz, M.L.; Carceller, M.C.; Ruhí, R.; Dalmau, P.; Vergés, J.; Montell, E.; Torrent, A.; Alcaraz, M.J. Chondroprotective effects of the combination chondroitin sulfate-glucosamine in a model of osteoarthritis induced by anterior cruciate ligament transection in ovariectomised rats. Biomed. Pharmacother. 2016, 79, 120–128. [Google Scholar] [CrossRef] [PubMed]
- La Gatta, A.; Stellavato, A.; Vassallo, V.; Di Meo, C.; Toro, G.; Iolascon, G.; Schiraldi, C. Hyaluronan and Derivatives: An In Vitro Multilevel Assessment of Their Potential in Viscosupplementation. Polymers 2021, 13, 3208. [Google Scholar] [CrossRef]
- Pomin, V.H.; Vignovich, W.P.; Gonzales, A.V.; Vasconcelos, A.A.; Mulloy, B. Galactosaminoglycans: Medical Applications and Drawbacks. Molecules 2019, 24, 2803. [Google Scholar] [CrossRef]
- Vázquez, J.A.; Fraguas, J.; Novoa-Carvallal, R.; Reis, R.L.; Antelo, L.T.; Pérez-Martín, R.I.; Valcarcel, J. Isolation and Chemical Characterization of Chondroitin Sulfate from Cartilage By-Products of Blackmouth Catshark (Galeus melastomus). Mar. Drugs 2018, 16, 344. [Google Scholar] [CrossRef] [PubMed]
- Vessella, G.; Traboni, S.; Laezza, A.; Iadonisi, A.; Bedini, E. (Semi)-Synthetic Fucosylated Chondroitin Sulfate Oligo- and Polysaccharides. Mar. Drugs 2020, 18, 293. [Google Scholar] [CrossRef] [PubMed]
- Volpi, N.; Maccari, F. Purification and characterization of hyaluronic acid from the mollusc bivalve Mytilus galloprovincialis. Biochimie 2003, 85, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Cimini, D.; Boccella, S.; Alfano, A.; Stellavato, A.; Paino, S.; Schiraldi, C.; Guida, F.; Perrone, M.; Donniacuo, M.; Tirino, V.; et al. Evaluation of unsulfated biotechnological chondroitin in a knee osteoarthritis mouse model as a potential novel functional ingredient in nutraceuticals and pharmaceuticals. Front. Bioeng. Biotechnol. 2022, 10, 934997. [Google Scholar] [CrossRef] [PubMed]
- Peck, J.; Slovek, A.; Miro, P.; Vij, N.; Traube, B.; Lee, C.; Berger, A.A.; Kassem, H.; Kaye, A.D.; Sherman, W.F.; et al. Comprehensive Review of Viscosupplementation in Osteoarthritis of the Knee. Orthop. Rev. 2021, 13, 25549. [Google Scholar] [CrossRef] [PubMed]
- Legré-Boyer, V. Viscosupplementation: Techniques, indications, results. Orthop. Traumatol. Surg. Res. 2015, 101 (Suppl. S1), S101–S108. [Google Scholar] [CrossRef]
- Dodero, A.; Williams, R.; Gagliardi, S.; Vicini, S.; Alloisio, M.; Castellano, M. A micro-rheological and rheological study of biopolymers solutions: Hyaluronic acid. Carbohydr. Polym. 2019, 203, 349–355. [Google Scholar] [CrossRef]
- Lapasin, R.; Segatti, F.; Mercuri, D.; De Conti, G.; Spagnul, C.; Fusi, S. Rheological studies dedicated to the development of a novel injectable polymeric blend for viscosupplementation treatment. Chem. Biochem. Eng. Q. 2015, 29, 511–518. [Google Scholar] [CrossRef]
- D’agostino, A.; La Gatta, A.; Stellavato, A.; Cimini, D.; Corsuto, L.; Cammarota, M.; D’agostino, M.; Schiraldi, C. Potential of Biofermentative Unsulfated Chondroitin and Hyaluronic Acid in Dermal Repair. Int. J. Mol. Sci. 2022, 23, 1686. [Google Scholar] [CrossRef]
- Vincent, T.L. Mechanoflammation in osteoarthritis pathogenesis. Semin. Arthritis Rheum. 2019, 49, S36–S38. [Google Scholar] [CrossRef]
- Martel-Pelletier, J.; Tat, S.K.; Pelletier, J.-P. Effects of chondroitin sulfate in the pathophysiology of the osteoarthritic joint: A narrative review. Osteoarthr. Cartil. 2010, 18 (Suppl. S1), S7–S11. [Google Scholar] [CrossRef]
- Gupta, R.C.; Lall, R.; Srivastava, A.; Sinha, A. Hyaluronic Acid: Molecular Mechanisms and Therapeutic Trajectory. Front. Veter. Sci. 2019, 6, 192. [Google Scholar] [CrossRef]
- Tak, P.P.; Firestein, G.S. NF-kappaB: A key role in inflammatory diseases. Clin. Investig. 2001, 107, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Mengshol, J.A.; Vincenti, M.P.; Coon, C.I.; Barchowsky, A.; Brinckerhoff, C.E. Interleukin-1 induction of collagenase 3 (matrix metalloproteinase 13) gene expression in chondrocytes requires p38, c-Jun N-terminal kinase, and nuclear factor κB: Differential regulation of collagenase 1 and collagenase 3. Arthritis Rheum. 2000, 43, 801–811. [Google Scholar] [CrossRef] [PubMed]
- Dojindo Cell Counting Kit-8 Handbook. Available online: https://goldbio.com/uploads/documents/429b0ad1486d8e41a337c3f3c2d3f44d.pdf (accessed on 6 September 2023).
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2−ΔΔCT Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Bradford, M.M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | G′ (Pa) | GG″ (Pa) | ||
|---|---|---|---|---|
| 0.5 Hz | 2.5 Hz | 0.5 Hz | 2.5 Hz | |
| HHA + CS + cd | 21.6 ± 0.7 | 92.3 ± 1.6 | 45.7 ± 1.0 | 105.3 ± 3.2 |
| HHA/BC | 26.4 ± 2.0 | 111.4 ± 3.9 | 55.3 ± 5.0 | 124.7 ± 9.7 |
| Sample | Tan δ | |
|---|---|---|
| 0.5 Hz | 2.5 Hz | |
| HHA + CS + cd | 2.1 ± 0.1 | 1.1 ± 0.1 |
| HHA/BC | 2.2 ± 0.2 | 1.1 ± 0.1 |
| Sample | η* (Pa × s) | |
|---|---|---|
| 0.5 Hz | 2.5 Hz | |
| HHA + CS + cd | 19.5 ± 0.7 | 16.0 ± 0.3 |
| HHA/BC | 37.1 ± 1.5 | 8.9 ± 0.2 |
| Gene Name | PCR Primer Sequence 5′→3′ |
|---|---|
| Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) | TGCACCACCAACTGCTTAGC GGCATGGACTGTGGTCATGAG |
| Aggrecan (AGN) | TCGAGGACAGCGAGGCC TCGAGGGTGTAGCGTGTAGAG |
| Type II collagen (COLII) | CAACACTGCCAACGTCCAGAT CTGCTTCGTCCAGATAGGCAA |
| Matrix metallopeptidase 13 (MMP-13) | TCCCTGAAGGGAAGGAGC CTCGTCCAGGATGGCGTAG |
| Interleukin-6 (IL-6) | GTGGAGATTGTTGCCATCAACG CAGTGGATGCAGGGATGATGTTCTG |
| Tumor necrosis factor alpha (TNF-α) | CGAGTGACAAGCCTGTAGC GGTGTGGGTGAGGAGCACAT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vassallo, V.; Di Meo, C.; Toro, G.; Alfano, A.; Iolascon, G.; Schiraldi, C. Hyaluronic Acid-Based Injective Medical Devices: In Vitro Characterization of Novel Formulations Containing Biofermentative Unsulfated Chondroitin or Extractive Sulfated One with Cyclodextrins. Pharmaceuticals 2023, 16, 1429. https://doi.org/10.3390/ph16101429
Vassallo V, Di Meo C, Toro G, Alfano A, Iolascon G, Schiraldi C. Hyaluronic Acid-Based Injective Medical Devices: In Vitro Characterization of Novel Formulations Containing Biofermentative Unsulfated Chondroitin or Extractive Sulfated One with Cyclodextrins. Pharmaceuticals. 2023; 16(10):1429. https://doi.org/10.3390/ph16101429
Chicago/Turabian StyleVassallo, Valentina, Celeste Di Meo, Giuseppe Toro, Alberto Alfano, Giovanni Iolascon, and Chiara Schiraldi. 2023. "Hyaluronic Acid-Based Injective Medical Devices: In Vitro Characterization of Novel Formulations Containing Biofermentative Unsulfated Chondroitin or Extractive Sulfated One with Cyclodextrins" Pharmaceuticals 16, no. 10: 1429. https://doi.org/10.3390/ph16101429
APA StyleVassallo, V., Di Meo, C., Toro, G., Alfano, A., Iolascon, G., & Schiraldi, C. (2023). Hyaluronic Acid-Based Injective Medical Devices: In Vitro Characterization of Novel Formulations Containing Biofermentative Unsulfated Chondroitin or Extractive Sulfated One with Cyclodextrins. Pharmaceuticals, 16(10), 1429. https://doi.org/10.3390/ph16101429