
A Review of the Role of Natural Products as Treatment Approaches for Xerostomia

 ,
,  ,
,  , and
, and 
Abstract
:1. General
1.1. Xerostomia
Innervation of the Salivary Glands
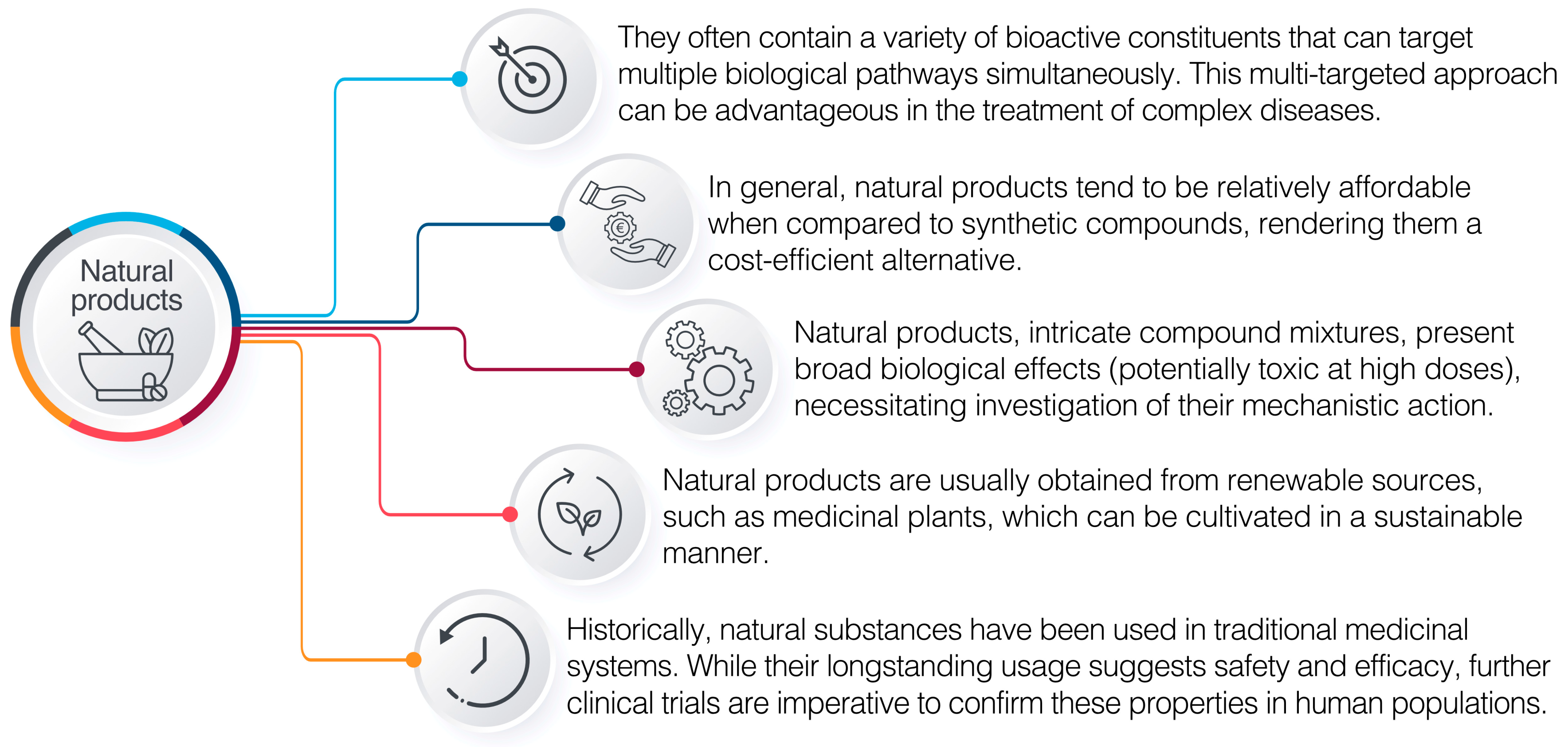
1.2. Natural Products Used in Pharmaceuticals
2. Approach of the Review
3. Natural Products Used for the Treatment of Xerostomia
3.1. In Vivo Studies
3.1.1. Apigenin
3.1.2. Ixeris dentata (Thunb.) Nakai Extract
3.1.3. Lycium barbarum L.
3.2. Clinical Trials
3.2.1. Camellia sinensis (L.) (Green Tea)
3.2.2. Thymus L. (Thyme Honey)
3.2.3. Fermented Lingonberry Juice
3.2.4. Cocos nucifera L. (Coconut Oil)
3.2.5. Lycopene-Enriched Olive Oil
3.2.6. Zingiber officinale Roscoe (Ginger)
3.2.7. Aloe vera (L.) Burm.f. and Mentha L. (Peppermint)
3.2.8. Glucosylceramide Extracted from Ananas comosus (L.) Merr. (Pineapple)
3.2.9. Linum usitatissimum L. (Linseed)
3.2.10. Matricaria chamomilla L. (Chamomile) and Linum usitatissimum L. (Linseed)
3.2.11. Hibiscus sabdariffa
3.2.12. Malva sylvestris L. and Alcea digitata (Boiss.)
3.2.13. Vitamin C/E Complex
3.2.14. Plantago ovata Forssk.
3.2.15. Pilocarpine
Systemic Administration of Pilocarpine
Topical Administration of Pilocarpine
Ginger on Pilocarpine-Stimulated Salivary Flow Rate
4. Summary and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Femiano, F.; Rullo, R.; Di Spirito, F.; Lanza, A.; Festa, V.M.; Cirillo, N. A Comparison of Salivary Substitutes versus a Natural Sialogogue (Citric Acid) in Patients Complaining of Dry Mouth as an Adverse Drug Reaction: A Clinical, Randomized Controlled Study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 112, e15–e20. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Cao, T.; Pathak, J.L.; Liu, X.; Mao, T.; Watanabe, N.; Li, X.; Zhang, M.; Li, J. Apigenin, a Single Active Component of Herbal Extract, Alleviates Xerostomia via ERα-Mediated Upregulation of AQP5 Activation. Front. Pharmacol. 2022, 13, 818116. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-M.; Chu, H.-T.; Wei, Y.-H.; Chen, F.-P.; Wang, S.; Wu, P.-C.; Yen, H.-R.; Chen, T.-J.; Chang, H.-H. The Core Pattern Analysis on Chinese Herbal Medicine for Sjögren’s Syndrome: A Nationwide Population-Based Study. Sci. Rep. 2015, 5, 9541. [Google Scholar] [CrossRef] [Green Version]
- Stankeviciene, I.; Puriene, A.; Mieliauskaite, D.; Stangvaltaite-Mouhat, L.; Aleksejuniene, J. Detection of Xerostomia, Sicca, and Sjogren’s Syndromes in a National Sample of Adults. BMC Oral Health 2021, 21, 552. [Google Scholar] [CrossRef] [PubMed]
- Iorgulescu, G. Saliva between Normal and Pathological. Important Factors in Determining Systemic and Oral Health. J. Med. Life 2009, 2, 303–307. [Google Scholar]
- Bulthuis, M.S.; Jan Jager, D.H.; Brand, H.S. Relationship among Perceived Stress, Xerostomia, and Salivary Flow Rate in Patients Visiting a Saliva Clinic. Clin. Oral Investig. 2018, 22, 3121–3127. [Google Scholar] [CrossRef] [Green Version]
- Bustillos, H.; Indorf, A.; Alwan, L.; Thompson, J.; Jung, L. Xerostomia: An Immunotherapy-Related Adverse Effect in Cancer Patients. Support. Care Cancer 2022, 30, 1681–1687. [Google Scholar] [CrossRef]
- Epstein, J.B.; Beier Jensen, S. Management of Hyposalivation and Xerostomia: Criteria for Treatment Strategies. Compend. Contin. Educ. Dent. 2015, 36, 600–603. [Google Scholar] [PubMed]
- Kapourani, A.; Kontogiannopoulos, K.N.; Manioudaki, A.-E.; Poulopoulos, A.K.; Tsalikis, L.; Assimopoulou, A.N.; Barmpalexis, P. A Review on Xerostomia and Its Various Management Strategies: The Role of Advanced Polymeric Materials in the Treatment Approaches. Polymers 2022, 14, 850. [Google Scholar] [CrossRef]
- Napeñas, J.J.; Brennan, M.T.; Fox, P.C. Diagnosis and Treatment of Xerostomia (Dry Mouth). Odontology 2009, 97, 76–83. [Google Scholar] [CrossRef]
- Soutome, S.; Yanamoto, S.; Nishii, M.; Kojima, Y.; Hasegawa, T.; Funahara, M.; Akashi, M.; Saito, T.; Umeda, M. Risk Factors for Severe Radiation-Induced Oral Mucositis in Patients with Oral Cancer. J. Dent. Sci. 2021, 16, 1241–1246. [Google Scholar] [CrossRef] [PubMed]
- Kapourani, A.; Kontogiannopoulos, K.N.; Barmpalexis, P. A Review on the Role of Pilocarpine on the Management of Xerostomia and the Importance of the Topical Administration Systems Development. Pharmaceuticals 2022, 15, 762. [Google Scholar] [CrossRef]
- Millsop, J.W.; Wang, E.A.; Fazel, N. Etiology, Evaluation, and Management of Xerostomia. Clin. Dermatol. 2017, 35, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, T.; Costa, K.C.D.; Guerra, L.D.F.C. Current Alternatives in the Prevention and Treatment of Xerostomia in Cancer Therapy. RGO Rev. Gaúch. Odontol. 2020, 68, e20200016. [Google Scholar] [CrossRef]
- Łysik, D.; Niemirowicz-Laskowska, K.; Bucki, R.; Tokajuk, G.; Mystkowska, J. Artificial Saliva: Challenges and Future Perspectives for the Treatment of Xerostomia. Int. J. Mol. Sci. 2019, 20, 3199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanasiewicz, M.; Hildebrandt, T.; Obersztyn, I. Xerostomia of Various Etiologies: A Review of the Literature. Adv. Clin. Exp. Med. 2016, 25, 199–206. [Google Scholar] [CrossRef] [Green Version]
- Nadig, S.D.; Ashwathappa, D.T.; Manjunath, M.; Krishna, S.; Annaji, A.G.; Shivaprakash, P.K. A Relationship between Salivary Flow Rates and Candida Counts in Patients with Xerostomia. J. Oral Maxillofac. Pathol. 2017, 21, 316. [Google Scholar] [CrossRef] [Green Version]
- Quilici, D.; Zech, K.N. Prevention and Treatment Options for Medication-Induced Xerostomia. Gen. Dent. 2019, 67, 52–57. [Google Scholar]
- Seo, K.; Kim, H.-N. Effects of Oral Health Programmes on Xerostomia in Community-Dwelling Elderly: A Systematic Review and Meta-Analysis. Int. J. Dent. Hyg. 2020, 18, 52–61. [Google Scholar] [CrossRef]
- Fleming, M.; Craigs, C.L.; Bennett, M.I. Palliative Care Assessment of Dry Mouth: What Matters Most to Patients with Advanced Disease? Support. Care Cancer 2020, 28, 1121–1129. [Google Scholar] [CrossRef] [Green Version]
- Salum, F.G.; Medella-Junior, F.d.A.C.; Figueiredo, M.A.Z.; Cherubini, K. Salivary Hypofunction: An Update on Therapeutic Strategies. Gerodontology 2018, 35, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Andablo-Reyes, E.; Mighell, A.; Pavitt, S.; Sarkar, A. Dry Mouth Diagnosis and Saliva Substitutes—A Review from a Textural Perspective. J. Texture Stud. 2021, 52, 141–156. [Google Scholar] [CrossRef]
- Liu, G.; Qiu, X.; Tan, X.; Miao, R.; Tian, W.; Jing, W. Efficacy of a 1% Malic Acid Spray for Xerostomia Treatment: A Systematic Review and Meta-Analysis. Oral Dis. 2023, 29, 862–872. [Google Scholar] [CrossRef]
- Ghannam, M.G.; Singh, P. Anatomy, Head and Neck, Salivary Glands. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Bernardini, S.; Tiezzi, A.; Laghezza Masci, V.; Ovidi, E. Natural Products for Human Health: An Historical Overview of the Drug Discovery Approaches. Nat. Prod. Res. 2018, 32, 1926–1950. [Google Scholar] [CrossRef]
- Thomford, N.; Senthebane, D.; Rowe, A.; Munro, D.; Seele, P.; Maroyi, A.; Dzobo, K. Natural Products for Drug Discovery in the 21st Century: Innovations for Novel Drug Discovery. Int. J. Mol. Sci. 2018, 19, 1578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atanasov, A.G.; Zotchev, S.B.; Dirsch, V.M.; Orhan, I.E.; Banach, M.; Rollinger, J.M.; Barreca, D.; Weckwerth, W.; Bauer, R.; Bayer, E.A.; et al. Natural Products in Drug Discovery: Advances and Opportunities. Nat. Rev. Drug Discov. 2021, 20, 200–216. [Google Scholar] [CrossRef]
- Dzobo, K. The Role of Natural Products as Sources of Therapeutic Agents for Innovative Drug Discovery. In Comprehensive Pharmacology; Elsevier: Amsterdam, The Netherlands, 2022; pp. 408–422. ISBN 978-0-12-820876-2. [Google Scholar]
- Li, Z.; Chen, K.; Rose, P.; Zhu, Y.Z. Natural Products in Drug Discovery and Development: Synthesis and Medicinal Perspective of Leonurine. Front. Chem. 2022, 10, 1036329. [Google Scholar] [CrossRef]
- Leonti, M.; Verpoorte, R. Traditional Mediterranean and European Herbal Medicines. J. Ethnopharmacol. 2017, 199, 161–167. [Google Scholar] [CrossRef]
- Li, F.-S.; Weng, J.-K. Demystifying Traditional Herbal Medicine with Modern Approach. Nat. Plants 2017, 3, 17109. [Google Scholar] [CrossRef]
- He, G.; Yin, Y.; Yan, X.; Wang, Y. Semi-Bionic Extraction of Effective Ingredient from Fishbone by High Intensity Pulsed Electric Fields. J. Food Process Eng. 2017, 40, e12392. [Google Scholar] [CrossRef]
- Harvey, A.L.; Edrada-Ebel, R.; Quinn, R.J. The Re-Emergence of Natural Products for Drug Discovery in the Genomics Era. Nat. Rev. Drug Discov. 2015, 14, 111–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Jiang, Y.; Ding, M.; Li, J.; Hao, J.; He, J.; Wang, H.; Gao, X.-M.; Chang, Y.-X. Simultaneous Determination and Qualitative Analysis of Six Types of Components in Naoxintong Capsule by Miniaturized Matrix Solid-Phase Dispersion Extraction Coupled with Ultra High-Performance Liquid Chromatography with Photodiode Array Detection and Quadrupole Time-of-Flight Mass Spectrometry. J. Sep. Sci. 2018, 41, 2064–2084. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Ge, Y.; Li, J.; Hao, J.; Wang, H.; He, J.; Gao, X.; Chang, Y. Simultaneous Determination of Columbianetin-β-d-Glucopyranoside and Columbianetin in a Biological Sample by High-Performance Liquid Chromatography with Fluorescence Detection and Identification of Other Columbianetin-β-d-Glucopyranoside Metabolites by Ultra High-Performance Liquid Chromatography Coupled with Quadrupole-Time of Flight Mass Spectrometry. J. Pharm. Biomed. Anal. 2018, 153, 221–231. [Google Scholar] [CrossRef]
- Kim, E.; Moore, B.S.; Yoon, Y.J. Reinvigorating Natural Product Combinatorial Biosynthesis with Synthetic Biology. Nat. Chem. Biol. 2015, 11, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Medema, M.H.; Fischbach, M.A. Computational Approaches to Natural Product Discovery. Nat. Chem. Biol. 2015, 11, 639–648. [Google Scholar] [CrossRef]
- Bhattarai, K.; Lee, H.-Y.; Kim, S.-H.; Kim, H.-R.; Chae, H.-J. Ixeris dentata Extract Increases Salivary Secretion through the Regulation of Endoplasmic Reticulum Stress in a Diabetes-Induced Xerostomia Rat Model. Int. J. Mol. Sci. 2018, 19, 1059. [Google Scholar] [CrossRef] [Green Version]
- Bhattarai, K.; Lee, H.Y.; Kim, S.H.; Park, J.S.; Kim, H.R.; Chae, H.J. Potential Application of Ixeris dentata in the Prevention and Treatment of Aging-Induced Dry Mouth. Nutrients 2018, 10, 1989. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Xiao, J.; Duan, Y.; Miao, M.; Huang, B.; Chen, J.; Cheng, G.; Zhou, X.; Jin, Y.; He, J.; et al. Lycium barbarum Polysaccharide Ameliorates Sjögren’s Syndrome in a Murine Model. Mol. Nutr. Food Res. 2021, 65, 2001118. [Google Scholar] [CrossRef]
- De Rossi, S.S.; Thoppay, J.; Dickinson, D.P.; Looney, S.; Stuart, M.; Ogbureke, K.U.E.; Hsu, S. A Phase II Clinical Trial of a Natural Formulation Containing Tea Catechins for Xerostomia. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 447–454.e3. [Google Scholar] [CrossRef]
- Charalambous, A.; Lambrinou, E.; Katodritis, N.; Vomvas, D.; Raftopoulos, V.; Georgiou, M.; Paikousis, L.; Charalambous, M. The Effectiveness of Thyme honey for the Management of Treatment-Induced Xerostomia in Head and Neck Cancer Patients: A Feasibility Randomized Control Trial. Eur. J. Oncol. Nurs. 2017, 27, 1–8. [Google Scholar] [CrossRef]
- Pärnänen, P.; Lomu, S.; Räisänen, I.T.; Tervahartiala, T.; Sorsa, T. Effects of Fermented Lingonberry Juice Mouthwash on Salivary Parameters—A One-Year Prospective Human Intervention Study. Dent. J. 2022, 10, 69. [Google Scholar] [CrossRef]
- Quimby, A.E.; Hogan, D.; Khalil, D.; Hearn, M.; Nault, C.; Johnson-Obaseki, S. Coconut Oil as a Novel Approach to Managing Radiation-Induced Xerostomia: A Primary Feasibility Study. Int. J. Otolaryngol. 2020, 2020, 8537643. [Google Scholar] [CrossRef] [PubMed]
- Navarro Morante, A.; Wolff, A.; Bautista Mendoza, G.R.; López-Jornet, P. Natural Products for the Management of Xerostomia: A Randomized, Double-Blinded, Placebo-Controlled Clinical Trial. J. Oral Pathol. Med. 2017, 46, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Mardani, H.; Ghannadi, A.; Rashnavadi, B.; Kamali, R. The Effect of Ginger Herbal Spray on Reducing Xerostomia in Patients with Type II Diabetes. Orig. Res. Artic. 2017, 7, 308–316. [Google Scholar]
- Chamani, G.; Zarei, M.R.; Mehrabani, M.; Nakhaee, N.; Kalaghchi, B.; Aghili, M.; Alaee, A. Assessment of Systemic Effects of Ginger on Salivation in Patients with Post-Radiotherapy Xerostomia. J. Oral Health Oral Epidemiol. 2017, 6, 130–137. [Google Scholar] [CrossRef]
- Badooei, F.; Imani, E.; Hosseini-Teshnizi, S.; Banar, M.; Memarzade, M. Comparison of the Effect of Ginger and Aloe Vera Mouthwashes on Xerostomia in Patients with Type 2 Diabetes: A Clinical Trial, Triple-Blind. Med. Oral 2021, 26, e408–e413. [Google Scholar] [CrossRef]
- Atashi, V.; Yazdannik, A.; Mahjobipoor, H.; Ghafari, S.; Bekhradi, R.; Yousefi, H. The Effects of Aloe Vera-Peppermint (Veramin) Moisturizing Gel on Mouth Dryness and Oral Health among Patients Hospitalized in Intensive Care Units: A Triple-Blind Randomized Placebo-Controlled Trial. J. Res. Pharm. Pract. 2018, 7, 104. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Nishi, Y.; Harada, K.; Masuzaki, T.; Minemoto, Y.; Yanagisawa, T.; Shimizu, T.; Tsuboi, A.; Hamada, T.; Nishimura, M. Impact of Oral Intake of Glucosylceramide Extracted from Pineapple on Xerostomia: A Double-Blind Randomized Cross-Over Trial. Nutrients 2019, 11, 2020. [Google Scholar] [CrossRef] [Green Version]
- Andersson, G.; Johansson, G.; Attström, R.; Edwardsson, S.; Glantz, P.-O.; Larsson, K. Comparison of the Effect of the Linseed Extract Salinum® and a Methyl Cellulose Preparation on the Symptoms of Dry Mouth. Gerodontology 1995, 12, 12–17. [Google Scholar] [CrossRef]
- Morales-Bozo, I.; Ortega-Pinto, A.; Rojas Alcayaga, G.; Aitken Saavedra, J.P.; Salinas Flores, O.; Lefimil Puente, C.; Lozano Moraga, C.; Manríquez Urbina, J.M.; Urzúa Orellana, B. Evaluation of the Effectiveness of a Chamomile (Matricaria chamomilla) and Linseed (Linum usitatissimum) Saliva Substitute in the Relief of Xerostomia in Elders. Gerodontology 2017, 34, 42–48. [Google Scholar] [CrossRef]
- Levrini, L.; Azzi, L.; Bossi, S. The Efficacy of a Dietary Supplement with Carnosine and Hibiscus Sabdariffa L. (AqualiefTM) in Patients with Xerostomia: A Randomized, Placebo-Controlled, Double-Blind Trial. Clin. Ter. 2020, 171, E295–E301. [Google Scholar] [CrossRef]
- Ameri, A.; Heydarirad, G.; Rezaeizadeh, H.; Choopani, R.; Ghobadi, A.; Gachkar, L. Evaluation of Efficacy of an Herbal Compound on Dry Mouth in Patients with Head and Neck Cancers: A Randomized Clinical Trial. J. Evid. Based Complement. Altern. Med. 2016, 21, 30–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, M.K.; Kim, D.H.; Ahn, Y.C.; Choi, J.Y.; Kim, E.H.; Son, Y. Randomized Trial of Vitamin C/E Complex for Prevention of Radiation-Induced Xerostomia in Patients with Head and Neck Cancer. Otolaryngol.—Head Neck Surg. 2016, 155, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Hasheminasab, F.S.; Hashemi, S.M.; Dehghan, A.; Sharififar, F.; Setayesh, M.; Sasanpour, P.; Tasbandi, M.; Raeiszadeh, M. Effects of a Plantago Ovata-Based Herbal Compound in Prevention and Treatment of Oral Mucositis in Patients with Breast Cancer Receiving Chemotherapy: A Double-Blind, Randomized, Controlled Crossover Trial. J. Integr. Med. 2020, 18, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Santos-Silva, A.R.; Rosa, G.B.; Eduardo, C.P.; Dias, R.B.; Brandao, T.B. Increased Risk for Radiation-Related Caries in Cancer Patients Using Topical Honey for the Prevention of Oral Mucositis. Int. J. Oral Maxillofac. Surg. 2011, 40, 1335–1336. [Google Scholar] [CrossRef]
- Bowen, W.H.; Lawrence, R.A. Comparison of the Cariogenicity of Cola, Honey, Cow Milk, Human Milk, and Sucrose. Pediatrics 2005, 116, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Ganjre, A.; Kathariya, R.; Bagul, N.; Pawar, V. Anti-Carcinogenic and Anti-Bacterial Properties of Selected Spices: Implications in Oral Health. Clin. Nutr. Res. 2015, 4, 209–215. [Google Scholar] [CrossRef] [Green Version]
- Pushpalatha, C.; Shakir, A. Potential Benefits of Ginger in Maintenance of Oral Health. In Ginger and Its Health Benefits; Nova Publishers: New York, NY, USA, 2022; p. 29. ISBN 978-1-68507-695-5. [Google Scholar]
- Carl, W.; Emrich, L.S. Management of Oral Mucositis during Local Radiation and Systemic Chemotherapy: A Study of 98 Patients. J. Prosthet. Dent. 1991, 66, 361–369. [Google Scholar] [CrossRef]
- Abrams, P.; Andersson, K.-E.; Buccafusco, J.J.; Chapple, C.; de Groat, W.C.; Fryer, A.D.; Kay, G.; Laties, A.; Nathanson, N.M.; Pasricha, P.J.; et al. Muscarinic Receptors: Their Distribution and Function in Body Systems, and the Implications for Treating Overactive Bladder. Br. J. Pharmacol. 2006, 148, 565–578. [Google Scholar] [CrossRef] [Green Version]
- Rieke, J.W.; Hafermann, M.D.; Johnson, J.T.; LeVeque, F.G.; Iwamoto, R.; Steiger, B.W.; Muscoplat, C.; Gallagher, S.C. Oral Pilocarpine for Radiation-Induced Xerostomia: Integrated Efficacy and Safety Results from Two Prospective Randomized Clinical Trials. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, N.; Sasano, N.; Yamashita, H.; Igaki, H.; Shiraishi, K.; Terahara, A.; Asakage, T.; Nakao, K.; Ebihara, Y.; Ohtomo, K.; et al. Oral Pilocarpine (5 mg t.i.d.) Used for Xerostomia Causes Adverse Effects in Japanese. Auris Nasus Larynx 2009, 36, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Noaiseh, G.; Baker, J.F.; Vivino, F.B. Comparison of the Discontinuation Rates and Side-Effect Profiles of Pilocarpine and Cevimeline for Xerostomia in Primary Sjögren’s Syndrome. Clin. Exp. Rheumatol. 2014, 32, 575–577. [Google Scholar] [PubMed]
- Chainani-Wu, N.; Gorsky, M.; Mayer, P.; Bostrom, A.; Epstein, J.B.; Silverman, S., Jr. Assessment of the Use of Sialogogues in the Clinical Management of Patients with Xerostomia. Spec. Care Dent. 2006, 26, 164–170. [Google Scholar] [CrossRef]
- Rhodus, N.L.; Schuh, M.J. Effects of Pilocarpine on Salivary Flow in Patients with Sjijgren’s Syndrome. Oral Surg. Oral Med. Oral Pathol. 1991, 72, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.N.; Singer, J. A comparison of Artificial Saliva and Pilocarpine in Radiation Induced Xerostomia. J. Laryngol. Otol. 1994, 108, 663–665. [Google Scholar] [CrossRef]
- Bernardi, R.; Perin, C.; Becker, F.L.; Ramos, G.Z.; Gheno, G.Z.; Lopes, L.R.; Pires, M.; Barros, H.M.T. Effect of Pilocarpine Mouthwash on Salivary Flow. Braz. J. Med. Biol. Res. 2002, 35, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Ahn, H.-J.; Choi, J.-H.; Jung, D.W.; Kwon, J.-S. Effect of 0.1% Pilocarpine Mouthwash on Xerostomia: Double-Blind, Randomised Controlled Trial. J. Oral Rehabil. 2014, 41, 226–235. [Google Scholar] [CrossRef]
- Tanigawa, T.; Yamashita, J.; Sato, T.; Shinohara, A.; Shibata, R.; Ueda, H.; Sasaki, H. Efficacy and Safety of Pilocarpine Mouthwash in Elderly Patients with Xerostomia: Pilocarpine Mouthwash and Xerostomia. Spec Care Dent. 2015, 35, 164–169. [Google Scholar] [CrossRef]
- Park, J.-E.; Song, C.-W.; Kim, K.-S.; Kim, M.-E. Comparison of the Effects of Pilocarpine Solution and Tablet on Salivary Flow Rate. J. Oral Med. Pain 2015, 40, 10–16. [Google Scholar] [CrossRef]
- Song, J.-I.; Park, J.-E.; Kim, H.-K.; Kim, M.-E.; Kim, K.-S. Dose- and Time-Related Effects of Pilocarpine Mouthwash on Salivation. J. Oral Med. Pain 2017, 42, 72–80. [Google Scholar] [CrossRef]
- Martins, V.B.; Cielo, C.A.; Santana, M.G.; Paim, É.D.; Barros, H.M. The Effects of Pilocarpine Mouthwash on Vocal Quality. IOSR J. Pharm. Biol. Sci. 2018, 13, 30–35. [Google Scholar]
- Santos Polvora, T.L.; De Sousa Pereira, R.M.; Macedo, A.P.; De Macedo, L.D.; Motta, A.C.F.; Tirapelli, C.; Pedrazzi, V. Pilocarpine Spray for the Treatment of Xerostomia: A Randomized, Double-Blind, Placebo-Controlled Trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, e47. [Google Scholar] [CrossRef]
- Pereira, R.M.D.S.; Bastos, M.D.R.; Ferreira, M.P.; Freitas, O.; Macedo, L.D.; Oliveira, H.F.; Ricz, H.M.A.; Motta, A.C.F.; Macedo, A.P.; Tirapelli, C.; et al. Topical Pilocarpine for Xerostomia in Patients with Head and Neck Cancer Treated with Radiotherapy. Oral Dis. 2020, 26, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
- Muthumariappan, S.; Ng, W.; Adine, C.; Ng, K.; Davoodi, P.; Wang, C.-H.; Ferreira, J. Localized Delivery of Pilocarpine to Hypofunctional Salivary Glands through Electrospun Nanofiber Mats: An Ex Vivo and In Vivo Study. Int. J. Mol. Sci. 2019, 20, 541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kan, C.Y.; H’ng, J.X.; Goh, A.; Smales, F.; Tan, E.L.; Zhang, S.; Pichika, M.R.; Parolia, A. Effect of Sustained Systemic Administration of Ginger (Z officinale) Rhizome Extracts on Salivary Flow in Mice. Int. Dent. J. 2023, 73, 63–70. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Natural Product/Compound | Product Form | Study on | Outcome/Results | Year of Publication | Reference |
|---|---|---|---|---|---|
| Apigenin | Apigenin powder | 24 female ICR mice (6-week-old, 30 ± 2 g) | Apigenin treatment increased the salivary secretion index and decreased water consumption in mice. Dose: 50 mg/kg/day, dissolved in 0.5% carboxymethyl cellulose sodium. | 2022 | [2] |
| Ixeris dentata (Thunb.) Nakai [Asteraceae] (IXD) | IXD ethanolic extract | 40 Sprague-Dawley male rats | Diabetic rats treated with IXD showed lower saliva and blood glucose concentrations, improved total body weight, and higher expression of salivary α-amylase. Dose: 100 mg/kg body weight ethanolic extract. | 2018 | [38] |
| Ixeris dentata (Thunb.) Nakai [Asteraceae] (IXD) | IXD methanolic suspended in H2O | 85 Sprague-Dawley adult male rats | In ageing rats, the administration of IXD extract at a dosage of 100 mg/kg led to a significant increase in total saliva compared to younger rats under the same treatment conditions. | 2018 | [39] |
| Lycium barbarum L. polysaccharide (LBP) | LBP powder (>95% purity) | 32 female non-obese diabetic (NOD) mice (7-week-old, 18 ± 2 g) | Low-dose LBP improves the salivary flow rates and alleviates inflammation in submandibular glands (SMGs), positively impacting primary Sjögren’s syndrome disease progression in NOD mice. Dose: 5 and 10 mg kg−1 d−1 | 2021 | [40] |
| Natural Product/Compound | Product Form | Number of Patients | Outcome/Results | Year of Publication | Reference |
|---|---|---|---|---|---|
| Camellia sinensis (L.) | Camellia sinensis (L.) (green tea) extract lozenge | 60 | The green tea extract lozenge showed a statistically significant increase in both SWSFR and UWSFR, but no significant difference in the quality of life (QoL). | 2014 | [41] |
| Thymus L. | Thyme honey | 72 | Thyme honey was found to be effective in reducing or stabilizing the degree of xerostomia, and also positively affected other symptoms, such as pain, taste loss, dysphagia (difficulty swallowing), QoL, and general satisfaction. Dose: Oral rinses (20 mL of thyme honey diluted in 100 mL of purified water). | 2017 | [42] |
| Vaccinium vitis-idaea L. (Common name: lingonberry) | Fermented lingonberry juice (FLJ) (Lingora®, Vantaa, Finland) | 21 | FLJ mouthwash positively affected all five salivary parameters (resting and stimulated saliva secretion rates, resting saliva pH, and stimulated saliva buffering capacity), with statistically significant improvements. Dose: 10 mL daily for 30 s. | 2022 | [43] |
| Cocos nucifera L. (Common name: coconut) | Coconut oil | 30 | There was no significant difference in xerostomia quality of life scale (XeQoLS) scores pre- and post-treatment among the entire study group and participants who continued coconut oil beyond the study period. Dose: Coating patient’s mouth with coconut oil prior to meals and at bedtime. | 2020 | [44] |
| Lycopene enriched Olea europaea L. (olive) | Lycopene enriched olive oil spray | 60 | Patient-assessed benefits and satisfaction with the spray were higher in the treatment group but the difference between treatment and placebo groups was not statistically significant. Dose: 1.5 mL spray to the mouth, three times per day. | 2017 | [45] |
| Zingiber officinale Roscoe (Common name: ginger) | Ginger ethanolic extract in a form of oral spray | 20 | The ginger herbal spray effectively increased salivation and reduced the severity of dry mouth in patients with type II diabetes. | 2017 | [46] |
| Zingiber officinale Roscoe (Common name: ginger) | Ginger capsule (Zintoma, Goldaru Company, Iran) | 61 | Marginally significant improvement in xerostomia symptoms with ginger treatment. Still, there were no significant differences between the groups regarding improvement of dry mouth symptoms and quality of life issues, except for dry mouth experience throughout the day. Dose: three capsules daily. | 2017 | [47] |
| Zingiber officinale Roscoe (Common name: ginger) | Ginger mouthwash (25% ginger) | 105 | Ginger mouthwashes significantly reduced all xerostomia symptoms (need to drink water to swallow dry foods, decreased salivation, mouth dryness upon waking, dry mouth during travel, and burning mouth sensation. Dose: 20 mL three times daily for 14 consecutive days. | 2021 | [48] |
| Aloe vera (L.) Burm.f. (Common name: Aloe vera) | Aloe vera mouthwash (50% aloe vera) | 105 | Aloe vera mouthwashes significantly reduced all xerostomia symptoms (need to drink water to swallow dry foods, decreased salivation, mouth dryness upon waking, dry mouth during travel, and burning mouth sensation. Dose: 20 mL three times daily for 14 consecutive days. | 2021 | [48] |
| Aloe vera (L.) Burm.f. and Mentha L. (Peppermint) | Moisturizing gel (Veramin) | 80 | The results indicated that the gel (Veramin) had significant effects on reducing mouth dryness and improving oral health. Dose: Apply gel to all surfaces of the oral mucosa, the gum, and the tongue after brushing, every 4 h. | 2018 | [49] |
| Glucosylceramide | Tablets containing Glucosylceramide Extracted from Ananas comosus (L.) Merr. (Common name: Pineapple) (GCP) | 16 | GCP administration significantly increased the oral moisture level of the lingual mucosa and the visual analog scale value related to xerostomia. Dose: one tablet per day (1.2 mg GCP per tablet). | 2019 | [50] |
| Linum usitatissimum L. (also known as linseed) | Linseed extracts: Salinum by Camurus AB, Sweden and MAS-84 | 20 | Both tested preparations had a beneficial effect on dry mouth symptoms, with Salinum showing improved results and performance. Dose: 2 mL. | 1995 | [51] |
| Matricaria chamomilla L. (Common name: Chamomile) and Linum usitatissimum L. (also known as linseed) | Chamomile and linseed saliva substitute | 74 | The chamomile and linseed saliva substitute positively affected four out of five xerostomia symptoms, while the conventional saliva substitute only impacted two of them. Dose: 2 mL, four times per day. | 2017 | [52] |
| Hibiscus sabdariffa | Aqualief™ (Helsinn Healthcare SA, Lugano, Switzerland) tablets | 60 | Aqualief™ significantly improved dry mouth symptoms compared to the placebo (normalizing saliva pH and significantly increase the saliva flow rate). Dose: Three times/day (after meals) for six consecutive days. | 2020 | [53] |
| Malva sylvestris L. and Alcea digitata (Boiss.) | Malva sylvestris and Alcea digitata in powdered form | 62 | The experimental and control groups revealed a significant decrease in the visual analog scale (VAS) score for the experimental group at four weeks when compared to the control group. Dose: Three times per day for four weeks. | 2016 | [54] |
| Vitamin C/E Complex | Antioxidant supplements | 45 | Short-term supplementation with an antioxidant vitamin E/C complex protects against RT-induced xerostomia in patients with head and neck cancer. Dose: Twice per day. | 2016 | [55] |
| Plantago ovata Forssk. | Plantago ovata husk in water as mouthwash | 28 | The herbal compound significantly mitigated oral mucositis, pain, xerostomia, and improved life quality versus placebo (p < 0.05); the oral care protocol likewise reduced oral mucositis. Dose: Three times per day. | 2020 | [56] |
| Pilocarpine | Oral tablets (systemic administration) | Systemic administration of pilocarpine increases resting and stimulated salivary flow, decreases subjective oral dryness, and improves chewing and speaking abilities of patients. Dose: Ranging from 2.5 to 10 mg, taken orally three or four times daily | 2022 | [12] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kontogiannopoulos, K.N.; Kapourani, A.; Gkougkourelas, I.; Anagnostaki, M.-E.; Tsalikis, L.; Assimopoulou, A.N.; Barmpalexis, P. A Review of the Role of Natural Products as Treatment Approaches for Xerostomia. Pharmaceuticals 2023, 16, 1136. https://doi.org/10.3390/ph16081136
Kontogiannopoulos KN, Kapourani A, Gkougkourelas I, Anagnostaki M-E, Tsalikis L, Assimopoulou AN, Barmpalexis P. A Review of the Role of Natural Products as Treatment Approaches for Xerostomia. Pharmaceuticals. 2023; 16(8):1136. https://doi.org/10.3390/ph16081136
Chicago/Turabian StyleKontogiannopoulos, Konstantinos N., Afroditi Kapourani, Ioannis Gkougkourelas, Maria-Emmanouela Anagnostaki, Lazaros Tsalikis, Andreana N. Assimopoulou, and Panagiotis Barmpalexis. 2023. "A Review of the Role of Natural Products as Treatment Approaches for Xerostomia" Pharmaceuticals 16, no. 8: 1136. https://doi.org/10.3390/ph16081136
APA StyleKontogiannopoulos, K. N., Kapourani, A., Gkougkourelas, I., Anagnostaki, M.-E., Tsalikis, L., Assimopoulou, A. N., & Barmpalexis, P. (2023). A Review of the Role of Natural Products as Treatment Approaches for Xerostomia. Pharmaceuticals, 16(8), 1136. https://doi.org/10.3390/ph16081136