


Use of Nanocarriers Containing Antitrypanosomal Drugs for the Treatment of Chagas Disease

 , and
, and 
Abstract
:
1. Introduction
2. Results
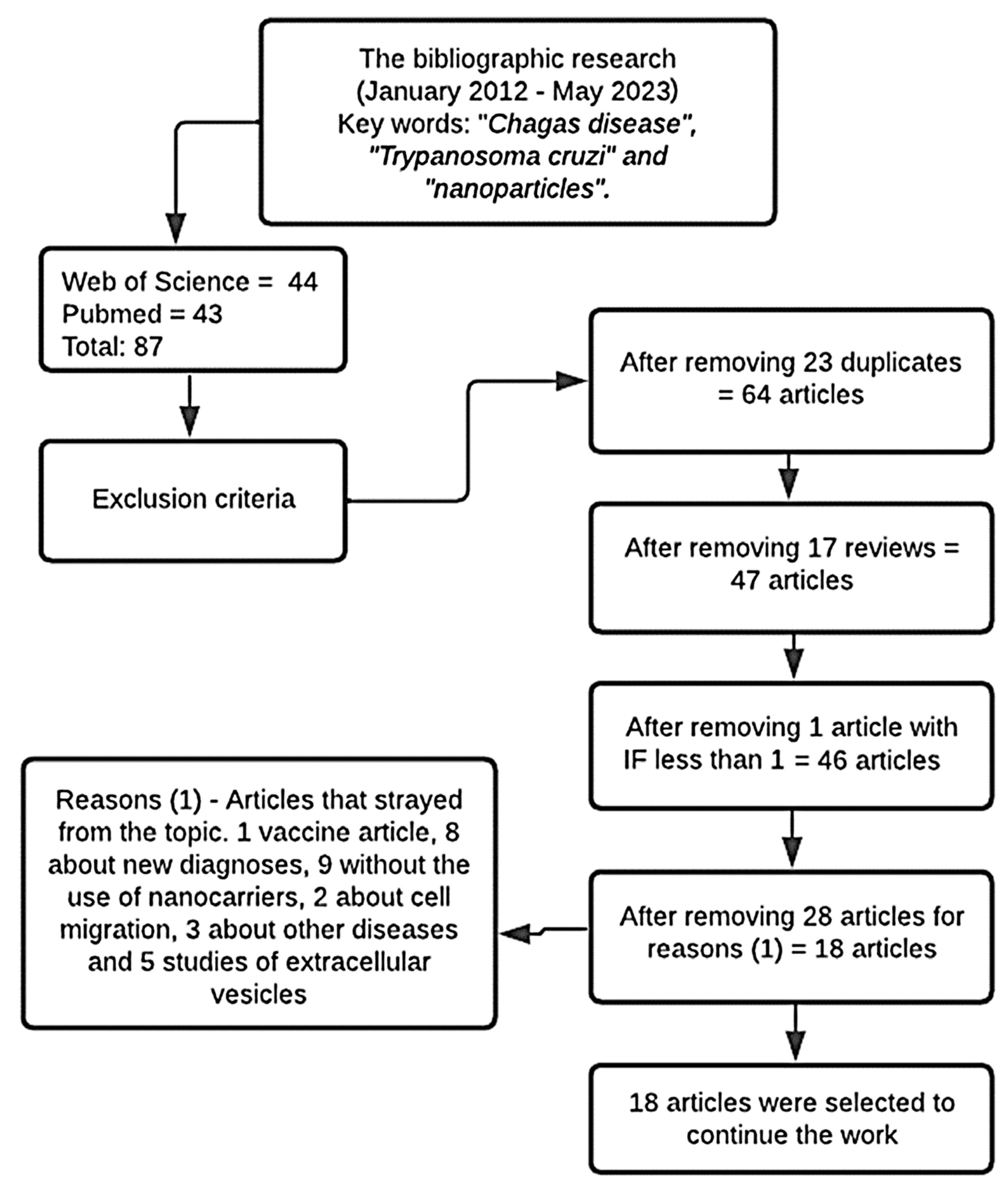
2.1. Bibliographic Research of Articles in the Databases
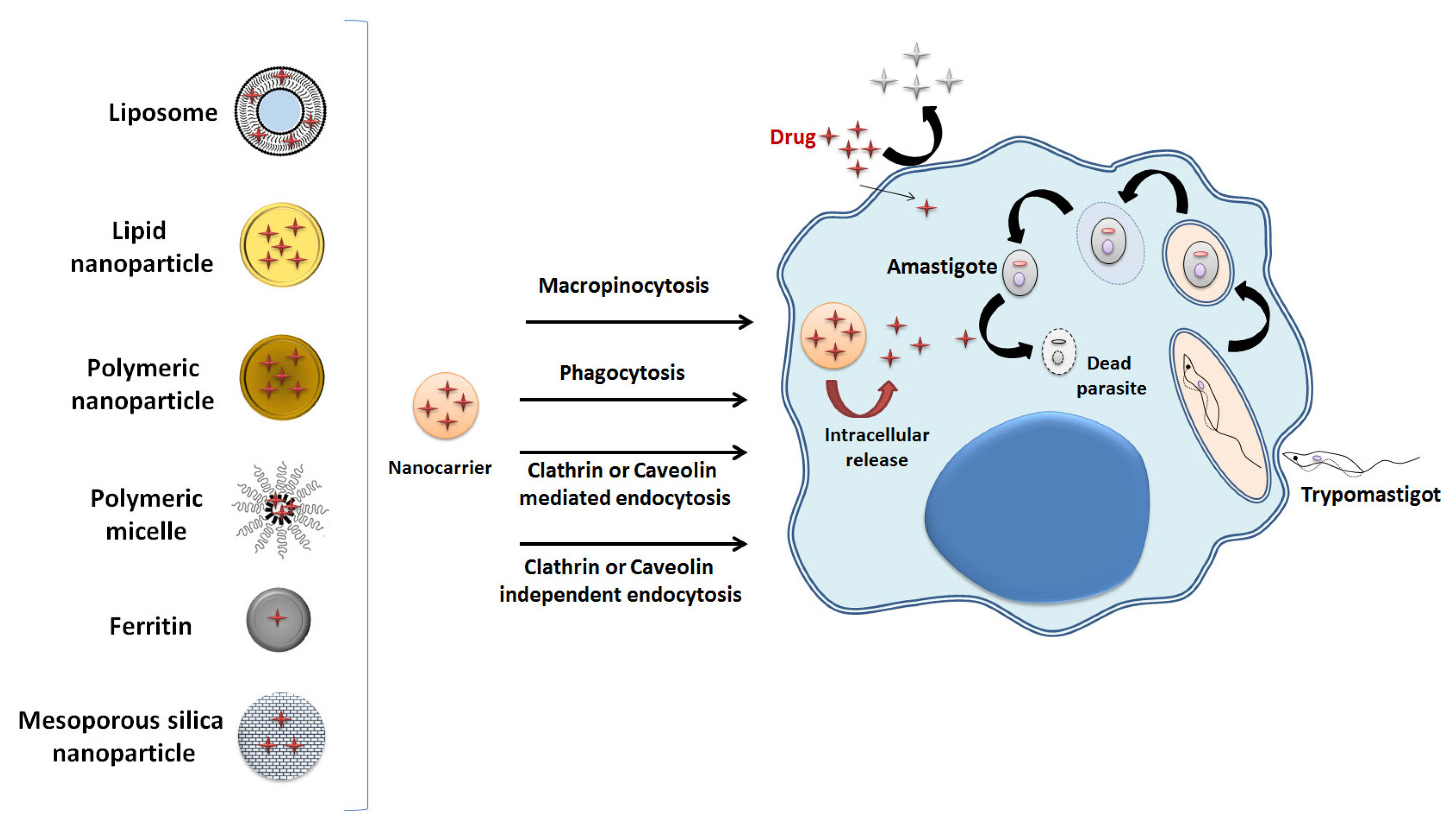
2.2. Nanocarriers
2.3. Components
2.4. Anti-T. cruzi Drugs
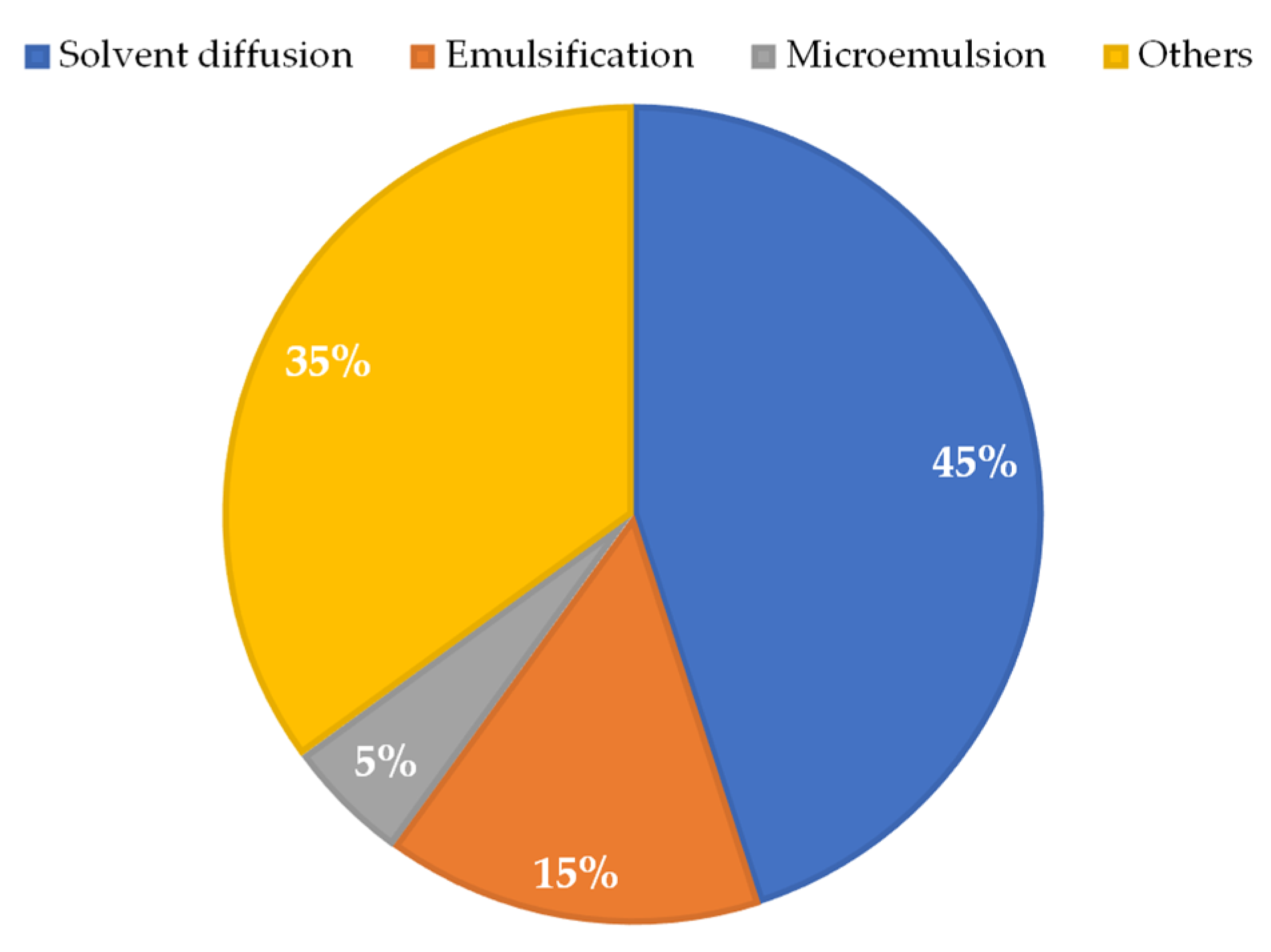
2.5. Preparation Method
2.6. Physicochemical Characterization
2.7. In Vitro Assays
2.8. In Vivo Assays
3. Discussion
3.1. In Vitro Data Discussion
3.1.1. Polymeric Nanoparticles
3.1.2. Lipid Nanoparticle
3.1.3. Other Nanoparticles
3.1.4. Liposomes and Vesicular Nanocarriers
3.2. In Vivo Data Discussion
3.2.1. Polymeric Nanoparticles
3.2.2. Lipid Nanoparticles
3.2.3. Polymeric Micelles
3.2.4. Liposomes
3.2.5. Nanocarriers of Drugs in the Chronic Phase of Chagas Disease
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, X.; Yi, S.; Scariot, D.B.; Martinez, S.J.; Falk, B.A.; Olson, C.L.; Romano, P.S.; Scott, E.A.; Engman, D.M. Nanocarrier-enhanced intracellular delivery of benznidazole for treatment of Trypanosoma cruzi infection. JCI Insight 2021, 6, e145523. [Google Scholar] [CrossRef]
- Vinuesa, T.; Herráez, R.; Oliver, L.; Elizondo, E.; Acarregui, A.; Esquisabel, A.; Pedraz, J.L.; Ventosa, N.; Veciana, J.; Viñas, M. Benznidazole Nanoformulates: A Chance to Improve Therapeutics for Chagas Disease. Am. J. Trop. Med. Hyg. 2017, 97, 1469–1476. [Google Scholar] [CrossRef] [Green Version]
- Nhavene, E.P.F.; da Silva, W.M.; Trivelato, R.R., Jr.; Gastelois, P.L.; Venâncio, T.; Nascimento, R.; Batista, R.J.C.; Machado, C.R.; Macedo, W.A.d.A.; de Sousa, E.M.B. Chitosan Grafted into Mesoporous Silica Nanoparticles as Benznidazol Carrier for Chagas Diseases Treatment. Microporous Mesoporous Mater. 2018, 272, 265–275. [Google Scholar] [CrossRef]
- Contreras Lancheros, C.A.; Pelegrino, M.T.; Kian, D.; Tavares, E.R.; Hiraiwa, P.M.; Goldenberg, S.; Nakamura, C.V.; Yamauchi, L.M.; Pinge-Filho, P.; Seabra, A.B.; et al. Selective Antiprotozoal Activity of Nitric Oxide-Releasing Chitosan Nanoparticles Against Trypanosoma cruzi: Toxicity and Mechanisms of Action. Curr. Pharm. Des. 2018, 24, 830–839. [Google Scholar] [CrossRef]
- Brito, T.K.; Silva Viana, R.L.; Gonçalves Moreno, C.J.; da Silva Barbosa, J.; Lopes de Sousa, F., Jr.; Campos de Medeiros, M.J.; Melo-Silveira, R.F.; Almeida-Lima, J.; de Lima Pontes, D.; Sousa Silva, M.; et al. Synthesis of Silver Nanoparticle Employing Corn Cob Xylan as a Reducing Agent with Anti-Trypanosoma cruzi Activity. Int. J. Nanomed. 2020, 15, 965–979. [Google Scholar] [CrossRef] [Green Version]
- Choudhury, S.D. Nano-Medicines a Hope for Chagas Disease! Front. Mol. Biosci. 2021, 8, 655435. [Google Scholar] [CrossRef]
- Branquinho, R.T.; Roy, J.; Farah, C.; Garcia, G.M.; Aimond, F.; le Guennec, J.Y.; Saude-Guimarães, D.A.; Grabe-Guimaraes, A.; Mosqueira, V.C.F.; de Lana, M.; et al. Biodegradable Polymeric Nanocapsules Prevent Cardiotoxicity of Anti-Trypanosomal Lychnopholide. Sci. Rep. 2017, 7, 44998. [Google Scholar] [CrossRef] [Green Version]
- Branquinho, R.T.; Mosqueira, V.C.F.; de Oliveira-Silva, J.C.V.; Simões-Silva, M.R.; Saúde-Guimarães, D.A.; de Lana, M. Sesquiterpene Lactone in Nanostructured Parenteral Dosage Form Is Efficacious in Experimental Chagas Disease. Antimicrob. Agents Chemother. 2014, 58, 2067–2075. [Google Scholar] [CrossRef] [Green Version]
- Sales, P.A.; Molina, I.; Murta, S.M.F.; Sánchez-Montalvá, A.; Salvador, F.; Corrêa-Oliveira, R.; Carneiro, C.M. Experimental and Clinical Treatment of Chagas Disease: A Review. Am. J. Trop. Med. Hyg. 2017, 97, 1289–1303. [Google Scholar] [CrossRef] [Green Version]
- Carneiro, Z.A.; Pedro, P.I.; Sesti-Costa, R.; Lopes, C.D.; Pereira, T.A.; Milanezi, C.M.; da Silva, M.A.P.; Lopez, R.F.V.; Silva, J.S.; Deflon, V.M. In Vitro and In Vivo Trypanocidal Activity of H2bdtc-Loaded Solid Lipid Nanoparticles. PLoS. Negl. Trop. Dis. 2014, 8, e2847. [Google Scholar] [CrossRef] [Green Version]
- Bayda, S.; Adeel, M.; Tuccinardi, T.; Cordani, M.; Rizzolio, F. The History of Nanoscience and Nanotechnology: From Chemical-Physical Applications to Nanomedicine. Molecules 2020, 25, 112. [Google Scholar] [CrossRef] [Green Version]
- Mora-Huertas, C.E.; Fessi, H.; Elaissari, A. Polymer-Based Nanocapsules for Drug Delivery. Int. J. Pharm. 2010, 385, 113–142. [Google Scholar] [CrossRef]
- Quezada, C.Q.; Azevedo, C.S.; Charneau, S.; Santana, J.M.; Chorilli, M.; Carneiro, M.B.; Bastos, I.M.D. Advances in Nanocarriers as Drug Delivery Systems in Chagas Disease. Int. J. Nanomed. 2019, 14, 6407–6424. [Google Scholar] [CrossRef]
- Volpedo, G.; Costa, L.; Ryan, N.; Halsey, G.; Satoskar, A.; Oghumu, S. Nanoparticulate Drug Delivery Systems for the Treatment of Neglected Tropical Protozoan Diseases. J. Venom. Anim. Toxins Incl. Trop. Dis. 2019, 25, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Foroozandeh, P.; Aziz, A. Insight into Cellular Uptake and Intracellular Trafficking of Nanoparticles. Nanoscale Res. Lett. 2018, 13, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Nsairat, H.; Khater, D.; Sayed, U.; Odeh, F.; al Bawab, A.; Alshaer, W. Liposomes: Structure, Composition, Types, and Clinical Applications. Heliyon 2022, 8, e09394. [Google Scholar] [CrossRef]
- Perumal, S.; Atchudan, R.; Lee, W. A Review of Polymeric Micelles and Their Applications. Polymers 2022, 14, 2510. [Google Scholar] [CrossRef]
- Wang, Z.; Gao, H.; Zhang, Y.; Liu, G.; Niu, G.; Chen, X. Functional ferritin nanoparticles for biomedical applications. Front. Chem. Sci. Eng. 2017, 11, 633–646. [Google Scholar] [CrossRef] [Green Version]
- Baiocco, P.; Ilari, A.; Ceci, P.; Orsini, S.; Gramiccia, M.; Di Muccio, T.; Colotti, G. Inhibitory Effect of Silver Nanoparticles on Trypanothione Reductase Activity and Leishmania infantum Proliferation. ACS Med. Chem. Lett. 2010, 2, 230–233. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Cruz, R.; Calasans-Maia, J.; Sartoretto, S.; Moraschini, V.; Rossi, A.M.; Louro, R.S.; Granjeiro, J.M.; Calasans-Maia, M.D. Does the Incorporation of Zinc into Calcium Phosphate Improve Bone Repair? A Systematic Review. Ceram. Int. 2018, 44, 1240–1249. [Google Scholar] [CrossRef]
- Tessarolo, L.D.; de Menezes, R.R.P.P.B.; Mello, C.P.; Lima, D.B.; Magalhães, E.P.; Bezerra, E.M.; Sales, F.A.M.; Barroso Neto, I.L.; Oliveira, M.D.F.; dos Santos, R.P.; et al. Nanoencapsulation of Benznidazole in Calcium Carbonate Increases Its Selectivity to Trypanosoma cruzi. Mineral. Mag. 2018, 145, 1191–1198. [Google Scholar] [CrossRef]
- Morales-Baez, M.; Rivera-Villanueva, J.M.; López-Monteon, A.; Peña-Rodríguez, R.; Trigos, Á.; Ramos-Ligonio, A. Trypanocidal Effect of Nano MOFs-EP on Circulating Forms of Trypanosoma cruzi. Iran. J. Parasitol. 2020, 15, 115–123. [Google Scholar] [CrossRef] [PubMed]
- de Freitas Oliveira, J.W.; da Silva, M.F.A.; Damasceno, I.Z.; Rocha, H.A.O.; da Silva Júnior, A.A.; Silva, M.S. In Vitro Validation of Antiparasitic Activity of PLA-Nanoparticles of Sodium Diethyldithiocarbamate against Trypanosoma cruzi. Pharmaceutics 2022, 14, 497. [Google Scholar] [CrossRef] [PubMed]
- Hernández, M.; Wicz, S.; Pérez Caballero, E.; Santamaría, M.H.; Corral, R.S. Dual Chemotherapy with Benznidazole at Suboptimal Dose plus Curcumin Nanoparticles Mitigates Trypanosoma cruzi-Elicited Chronic Cardiomyopathy. Parasitol. Int. 2021, 81, 102248. [Google Scholar] [CrossRef]
- Rial, M.S.; Arrúa, E.C.; Natale, M.A.; Bua, J.; Esteva, M.I.; Prado, N.G.; Laucella, S.A.; Salomon, C.J.; Fichera, L.E. Efficacy of Continuous versus Intermittent Administration of Nanoformulated Benznidazole during the Chronic Phase of Trypanosoma cruzi Nicaragua Infection in Mice. J. Antimicrob. Chemother. 2020, 75, 1906–1916. [Google Scholar] [CrossRef]
- Rial, M.S.; Scalise, M.L.; Arrúa, E.C.; Esteva, M.I.; Salomon, C.J.; Fichera, L.E. Elucidating the Impact of Low Doses of Nano-Formulated Benznidazole in Acute Experimental Chagas Disease. PLoS. Negl. Trop. Dis. 2017, 11, e0006119. [Google Scholar] [CrossRef] [Green Version]
- Scalise, M.L.; Arrúa, E.C.; Rial, M.S.; Esteva, M.I.; Salomon, C.J.; Fichera, L.E. Promising Efficacy of Benznidazole Nanoparticles in Acute Trypanosoma cruzi Murine Model: In-Vitro and in-Vivo Studies. Am. J. Trop. Med. Hyg. 2016, 95, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Abriata, J.P.; Eloy, J.O.; Riul, T.B.; Campos, P.M.; Baruffi, M.D.; Marchetti, J.M. Poly-Epsilon-Caprolactone Nanoparticles Enhance Ursolic Acid in Vivo Efficacy against Trypanosoma cruzi Infection. Mater. Sci. Eng. C 2017, 77, 1196–1203. [Google Scholar] [CrossRef]
- de Mello, C.G.C.; Branquinho, R.T.; Oliveira, M.T.; Milagre, M.M.; Saúde-Guimarães, D.A.; Mosqueira, V.C.F.; de Lana, M. Efficacy of Lychnopholide Polymeric Nanocapsules after Oral and Intravenous Administration in Murine Experimental Chagas Disease. Antimicrob. Agents Chemother. 2016, 60, 5215–5222. [Google Scholar] [CrossRef] [Green Version]
- Branquinho, R.T.; de Mello, C.G.C.; Oliveira, M.T.; Soares Reis, L.E.; de Abreu Vieira, P.M.; Saúde-Guimarães, D.A.; Furtado Mosqueira, V.C.; de Lana, M. Lychnopholide in Poly(D,L-Lactide)-Block-Polyethylene Glycol Nanocapsules Cures Infection with a Drug-Resistant Trypanosoma cruzi Strain at Acute and Chronic Phases. Antimicrob. Agents. Chemother. 2020, 64, 10–1128. [Google Scholar] [CrossRef]
- Branquinho, R.T.; Pound-Lana, G.; Marques Milagre, M.; Saúde-Guimarães, D.A.; Vilela, J.M.C.; Andrade, M.S.; de Lana, M.; Mosqueira, V.C.F. Increased Body Exposure to New Anti-Trypanosomal Through Nanoencapsulation. Sci. Rep. 2017, 7, 8429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, S.; Ghosh, S.; De, A.K.; Bera, T. Oral Delivery of Ursolic Acid-Loaded Nanostructured Lipid Carrier Coated with Chitosan Oligosaccharides: Development, Characterization, in Vitro and in Vivo Assessment for the Therapy of Leishmaniasis. Int. J. Biol. Macromol. 2017, 102, 996–1008. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, A.B.; Saúde, D.A.; Perry, K.S.P.; Duarte, D.S.; Raslan, S.; Amelia, M.; Boaventura, D.; Chiari, E. Trypanocidal Sesquiterpenes from Lychnophora Species. Phytother. Res. 1996, 10, 292–295. [Google Scholar] [CrossRef]
- Branquinho, R.T.; Mosqueira, V.C.F.; Kano, E.K.; de Souza, J.; Dorim, D.D.R.; Saúde-Guimarães, D.A.; de Lana, M. HPLC-DAD and UV-Spectrophotometry for the Determination of Lychnopholide in Nanocapsule Dosage Form: Validation and Application to Release Kinetic Study. J. Chromatogr. Sci. 2014, 52, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Fan, J.; Fang, G.; Wang, X.; Zeng, F.; Xiang, Y.; Wu, S. Targeted Anticancer Prodrug with Mesoporous Silica Nanoparticles as Vehicles. Nanotechnology 2011, 22, 455102. [Google Scholar] [CrossRef] [PubMed]
- Romero, L.; Morilla, J. Nanotechnological approaches against Chagas disease. Adv. Drug. Deliv. Ver. 2010, 62, 576–588. [Google Scholar] [CrossRef]
- Bustamante, J.M.; Lo Presti, M.S.; Rivarola, H.W.; Fernández, A.R.; Enders, J.E.; Fretes, R.E.; Paglini-Oliva, P. Treatment with benznidazole or thioridazine in the chronic phase of experimental Chagas disease improves cardiopathy. Int. J. Antimicrob. Agents 2007, 29, 733–737. [Google Scholar] [CrossRef]
- Montelione, N.; Loreni, F.; Nenna, A.; Catanese, V.; Scurto, L.; Ferrisi, C.; Jawabra, M.; Gabellini, T.; Codispoti, F.A.; Spinelli, F.; et al. Tissue Engineering and Targeted Drug Delivery in Cardiovascular Disease: The Role of Polymer Nanocarrier for Statin Therapy. Biomedicines 2023, 11, 798. [Google Scholar] [CrossRef]
- do Nascimento, T.; Todeschini, A.R.; Santos-Oliveira, R.; de Souza de Bustamante Monteiro, M.S.; de Souza, V.T.; Ricci-Junior, E. Trends in Nanomedicines for Cancer Treatment. Curr. Pharm. Des. 2020, 26, 3579–3600. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Keywords | PubMed | Web of Science | Total |
|---|---|---|---|
| Chagas disease and nanoparticles | 69 | 63 | 123 |
| Trypanosoma cruzi and nanoparticles | 49 | 71 | 120 |
| Chagas disease and Trypanosoma cruzi and nanoparticles | 43 | 44 | 87 |
| Reference | [22] | [23] | [24] | [2] | [25] | [4] | [3] | [10] | [1] | [26] | [5] | [27] | [28] | [29] | [8] | [30] | [31] | [7] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Title | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Abstract | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Introduction | ||||||||||||||||||
| Contextualization | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Objective | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Methods | ||||||||||||||||||
| Ethics statement | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Study design | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Complete physicochemical characterization | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 |
| Nanometric size | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Animals | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Sample size | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| In vitro study | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 |
| In vivo study | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Trypanocidal effect | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Statistics | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Results and discussion | ||||||||||||||||||
| Interpretation | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Limitations | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 |
| Conclusion | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Score | 11 | 10 | 12 | 10 | 14 | 12 | 9 | 17 | 17 | 15 | 12 | 16 | 16 | 16 | 14 | 15 | 16 | 16 |
| Reference | System | Composition | Drug | Drug Concentration | Preparation Method | Characterization | Size (nm)/PDI |
|---|---|---|---|---|---|---|---|
| Polymeric Nanoparticle | |||||||
| [4] | Chitosan polymeric nanoparticles (CS-NPs) and S-nitroso-MSA-CS NPs (NO-releasing nanoparticles) | CS, TPP, MSA, NaNO2, DTNB, EDTA, PBS, [3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl-2H-tetrazolium bromide] and acetic acid | Mercaptosuccinic acid (MSA) and NO for NaNO2 | 400 mmol/L of MSA and equimolar amount of NaNO2 | Ionotropic gelation, stirring and suspension | Mean hydrodynamic diameter, PDI, and zeta potential by DLS. MSA EE in CS-NPs and nitrosation of MSA-CS NPs by UV-Vis spectrophotometry. Kinetics of decomposition through linear regression. | 101.0 ± 2.535 nm/ PDI = 0.280 ± 0.006 |
| [7] | Biodegradable polymeric nanoparticles (NPs) with encapsulated LYC | LYC, monomethoxy-polyethylene glycol-block-poly(lactide) polymer, n-dimethylacetamide: polyethylene glycol 300 (DMA-PEG), isotonic glucose solution | LYC | 10 mg of LYC with 60 mg of PLA. | Interfacial polymer deposition followed by solvent displacement method. | Mean hydrodynamic diameter and PDI determined by DLS | 105.1 ± 4.4 nm/ PDI = Below 0.3 |
| [8] | LYC-loaded polymeric nanoparticles | LYC, DMA-PEG 300, Glucose, Acetone, Poloxamer 188, PLA-PEG Polymer, Resomer 203, Epikuron 170, Miglyol 810 N | LYC | 10 mg de LYC with 80 mg PCL Drug loading 95% to LYC-loaded in PCL-NP 10 mg de LYC with 80 mg (40 mg of PLA-Peg + 40 mg Resomer 203) Drug loading 100% to LYC-loaded in (PLA-Peg/PLA)-NP | Interfacial polymer deposition followed by solvent displacement method. | Mean size and PDI | 182.5 ± 3.2 nm/ PDI = Below 0.3 |
| [24] | Polymeric PLA nanoparticles containing DETC | DETC, acetone, ethanol, and PLA at 0.5% (w/v) | Diethyldithio-carbamate | 1:12 DETC/polymer ratios, which corresponds to 8.2% (w/w) of the drug in the system | Nanoprecipitation with solvent evaporation methodology | Physical characterization by DLS, SEM, and AFM. Particle diameter by DLS, zeta potential by electrophoretic mobility. EE, DL, UV-Vis spectrophotometry, and FTIR-ATR | 168 nm/ PDI below 0.3 |
| [25] | Polymeric nanoparticle | PLGA, curcumin, ethyl acetate, polyvinyl alcohol, 5% sucrose solution. (coating), miltefosine (co-release vehicle) | BZN and Curcumin | 500 mg of PLGA with 75 mg of Cur | Emulsification followed by evaporation | DLS size, zeta potential, and AFM morphology | 250–300 nm |
| [29] | Polymeric PCL nanoparticles | UA, PCL, acetone, and surfactant (Poloxamer™ 407). | Ursolic acid | 125 mg of PCL with 12.5 mg of ursolic acid | Nanoprecipitation | Size, zeta potential, PDI, EE, morphology by SEM, and thermal behavior by DSC | 1:1 = 197.6 ± 0.85 nm 1:2 = 173.2 ± 7.28 nm/ PDI = 0.09 ± 0.03 |
| [30] | Polymeric PEG nanoparticles containing LYC (LYC-NPs) | LYC, PCL, Miglyol 810 N, Epikuron, Acetone, Poloxamer 188, PLA-PEG and PLA | LYC | 20 mg of LYC with 80 mg of PCL. 20 mg of LYC with 60 mg of PLA-PEG diblock polymer blended with 60 mg of PLA homopolymer. | Interfacial polymer deposition followed by solvent displacement method. | Mean hydrodynamic diameter and PDI by DLS. Zeta potentials by laser Doppler anemometry associated with microelectrophoresis | LYC-PCL-NP 190.2 ± 5.7 nm LYC-PLA-PEG-NP 106.1 ± 6.3 nm/ PDI below 0.3 |
| [31] | Lychnopholide Polymeric Nanoparticles (LYC-PLA-PEG-NP) | LYC, PLA-PEG. Acetone, Epikuron, Miglyol, Poloxamer | LYC | 20 to 40 mg de LYC with 120 mg (60 mg of PLA-Peg + 60 mg Resomer 203) LYC loading in PLA-PEG-NP of 9 wt% | Interfacial polymer deposition followed by solvent displacement method. | Mean hydrodynamic diameter, PDI, zeta potential, HPLC-UV, AFM, and LYC loading. | 107 ± 8 nm PDI = Below 0.3 |
| Lipid Nanoparticles | |||||||
| [2] | SLNs, NLCs and liposomes. | BNZ, Precirol® dichloromethane solution, Poloxamer 188 at 1% and Polysorbate 80 for SLNs. Precirol® ATO 5, Miglyol® 812, Polysorbate 80 and Poloxamer 188 for NLCs. Cholesterol with PEG1000 for Liposomes. | BZN | - | Emulsification techniques for SLNs. Hot homogenization technique using high pressure homogenizer for NLCs. Fluid compression technique called DELOS-SUSP for liposomes. | Size, PDI, Zeta potential, EE, and cumulative release | SLNs (166 nm) NLCs (202 nm) Liposomes (118 nm) PDI SLNs (0.219 ± 0.02–0.263 ± 0.02) NLCs = 0.371 ± 0.03–0.447 ± 0.00) Liposomes (0.190 ± 0.005) |
| [10] | H2bdtc-loaded SLNs (H2bdtc-SLNs) | Sodium taurodeoxycholate, melted stearic acid, soy lecithin and H2bdtc | H2bdtc | 0.02% w/v of H2bdtc with 0.12% w/v of sodium taurodeoxycholate and 0.95% w/v of stearic acid | Microemulsion | D-stroke size by PCS. Zeta potential by mobility electrophoresis of the nanoparticles. Morphology by AFM. DL by UV-Vis spectroscopy. EE% | 127.4 ± 10.2 nm/ PDI = 0.229 ± 0.130 |
| Mesoporous Silica Nanoparticles | |||||||
| [3] | Mesoporous Silica Nanoparticles (MSNs) | BZN, CS, EtOH, GPTMS, NaOH, HCl, C4H4O3, TEOS, CTAB. | BZN | - | Positively charged CTAB model and NaOH catalyst in diluted aqueous conditions, through hydrolysis and condensation of tetraethoxysilane | Zeta potential, TEM, EFTEM, CHN, XPS, SS NMR and DFT | Not reported |
| Silver Nanoparticles | |||||||
| [5] | Silver nanoparticles | Iresine. herbstii leaves, corn cob xylan, silver nitrate | Xylan (bioactive polysaccharide) | 10 mg/mL (1:9 w/v) solution of xylan with a solution of 1.0 mM silver nitrate. | Green Synthesis process, continuous agitation, centrifugation and lyophilization | Ultraviolet-visible spectroscopy, FTIR, Raman spectroscopy, EDS, SEM, AFM, ICP-OES, DLS, PDI, and zeta potential | 55 nm mean size by SEM and AFM DLS showed 102 ± 1.7 nm PDI = 0.178 |
| Polymeric Micelles | |||||||
| [26] | Polymeric micelles (BZN-PMs) | BZN, ethanol and Lutrol F-68 (P188) | BZN | 200 mg of BZN dissolved in 10 mL of EtOH and 300 mg of P188 | Solvent diffusion method | Size, zeta potential, and PDI | 61–65 nm/ PDI = 3.35 ±0.1 |
| [27] | BNZ polymeric micelles (BZN-PMs) | BZN, EtOH (solvent), water (antisolvent), Lutrol F-68 (P188) | BZN | 200 mg of BZN dissolved in 10 mL of EtOH and 300 mg of P188 | Solvent diffusion method and nanoprecipitation technique with P188 as stabilizer | Size by DLS, PDI, ID, z mean diameter, and zeta potential (ζ). Saturation solubility studies | 63.30 ± 2.82 nm/ PDI = 3.35 ± 0.10 |
| [28] | Polymeric micelles (BZN-PMs) | BNZ, EtOH and Lutrol F-68 (P188) | BZN | 200 mg of BZN dissolved in 10 mL of EtOH and 300 mg of P188 | Solvent diffusion method and nanoprecipitation technique with P188 as stabilizer | Size (PCS), zeta potential measurement (electrophoretic mobility) and PDI | 63.3 ± 2.82 nm/ PDI = 3.35 ± 0.1 |
| Liposomes | |||||||
| [1] | BNZ-loaded polymerosomes | PEG thioacetate, PEG mesylate, propylene sulfide, BZN and tetrahydrofuran | BZN | 1.5 mg of BNZ with 30 mg of the copolymer (PEG17-PPS60-PEG17) | Anionic polymerization, methanol precipitation, and thin film rehydration. | NMR spectroscopy and gel permeation chromatography, TEM, DLS, LC-MS, liquid chromatography–coupled mass spectrometry, SEM. Loading efficiency, EE, size, zeta potential, and morphology | 115 nm/ PDI = 0.11 ± 0.02. |
| Others Nanocarriers | |||||||
| [22] | CaCO3 nanoparticles containing BZN (BZN@CaCO3) | Calcium chloride, Pluronic F-68, Sodium carbonate and BNZ. | BZN | 1 mg of BZN in a solution A containing 50 mL of calcium chloride which has been mixed with a solution B containing 50 mL of sodium carbonate and 50 mL of sodium citrate | Emulsification | Zeta potential, AFM, IR, and UV-Vis spectrophotometry. | 27.83–64.01 nm |
| [23] | MOF nanoparticles coupled to EP (MOFs-EP) | Zn (NO3)2·6H2O, L1, L2 and | EP | 50 mg of EP with 100 mg of Zn-MOFs | Heating and cooling for crystal formation (synthesis of MOF nanoparticles). Sensitized photo-oxygenation in methanol with eosin (synthesis of EP). Mechanochemistry for coupling. | IR, XRD, TEM, and SEM | 28.67–80.44 nm |
| Reference | Cells | Anti-Epimastigotes | Anti-Trypomastigotes | Anti-Amastigotes | CC50—Cells | IC50—Epimastigotes | IC50—Trypomastigotes | IC50—Amastigotes |
|---|---|---|---|---|---|---|---|---|
| Polymeric Nanoparticle | ||||||||
| [4] | LLCMK2 cells (kidney epithelial cells from Macaca mulatta, CCL-7). Cytotoxicity (MTT) in peritoneal macrophages. | Antiproliferative effect against epimastigotes by direct count in a hemocytometer. Scanning and transmission electron microscopy of epimastigotes. | Effect on trypomastigotes viability in hemocytometer under a light microscope. | - | 400 ± 5.7 μg/mL | 75.0 ± 6.5 μg/mL | IC50 = 25.0 ± 5.0 μg/mL | - |
| [7] | Potential toxicity of LIC by calcium homeostasis in isolated cardiomyocytes from healthy mice | - | - | - | - | - | - | - |
| [24] | MTT against three cell lines: RAW (ATCC number TIB-71), derived from macrophages, 3T3 (ATCC CRL-1658), derived from fibroblasts, and Vero (ATCC CCL-81), derived from renal epithelial cells. | Induction of ROS production by parasites in the epimastigote form exposed to DETC nanoparticles. | Antiparasitic activity against different of T. cruzi strains in trypomastigotes determined by resazurin reduction and ROS production. | - | - | - | (Dm28c strain) Nanoparticle IC50 = 15.47 ± 2.71 μM. Free BZN = 70.58 ± 6.87 μM. (Y strain) Nanoparticle IC50 = 45.15 ± 5.44 µM. Free BZN = 85.24 ± 5.22 μM. (Bolivia Strain) Nanoparticle IC50 = 47.89 ± 3.98 μM. Free BZN was 79.78 ± 6.18 μM. | - |
| [29] | Cytotoxicity by the resazurin method in LLCMK2 fibroblasts and Trypanosoma cruzi cells. | - | Cytotoxicity in Trypanosoma cruzi cells in the trypomastigote form by the resazurin method. | - | - | - | - | - |
| Lipid Nanoparticles | ||||||||
| [2] | WST (water soluble tetrazolium test) cytotoxicity in L-929 murine fibroblasts (NCTC 929 clone, ECACC 88102702) and human hepatocellular Hep G2 cell line (American Type Culture Collection (ATCC)) | Biological activity of SLNs, NLCs, and liposomes against epimastigotes. Growth inhibition assays. | Growth inhibition assays. | Growth inhibition assays. | - | SLNs (5, 10, 20): 48.8 ± 14.3 μM–123.9 ± 19.7 μM. NLCs: 41.3 ± 9.9 μM–256.0 ± 19.9 μM. BNZ: 17.7 ± 2.1 μM. Liposomes: It was not viable. | NLCs 20″: 17.6 ± 3.3 μM. BNZ: 0.8 ± 0.4 μM | NLCs 20″: 17.6 ± 3.3 μM BNZ: 0.8 ± 0.4 μM |
| [10] | Cytotoxicity by flow cytometry in spleen cells isolated from C57BL/6 mice previously cultured in fibroblasts (LLCMK2) | - | Evaluation of the trypanocidal activity of free H2bdtc, H2bdtc-SLNs, and BZN after 24h of incubation with trypomastigotes forms | - | - | - | Free H2bdtc—IC50 of 0.50 ± 0.12 μM, H2bdtc-SLNs of 1.8 ± 0.18 μM and BZN of 0.50 ± 0.39 μM. | - |
| Mesoporous Silica Nanoparticles | ||||||||
| [3] | Biological assays—trypanocides for the epimastigotes forms of the T. cruzi CL Brener strain. | - | - | - | - | - | - | |
| Silver Nanoparticles | ||||||||
| [5] | Cytotoxicity (MTT) on murine macrophages (RAW 264.7 ATCC TIB-71) and mouse fibroblasts (3T3 ATCC CCL-92). | Evaluation of the antiparasitic activity of nano xylan by colorimetric MTT. Flow cytometry. | - | - | - | - | - | - |
| Polymeric Micelles | ||||||||
| [27] | Quantification of reactive oxygen species (ROS) and T. cruzi-specific antibody production in cardiac tissue inflammation in Vero cells (African green monkey renal epithelial cells) by fluorescence assay. | - | - | - | - | - | - | - |
| [28] | Toxicity (MTT) in Vero cells. | - | - | Amastigote growth inhibition assay in mouse cardiac myocytes (CMs) and Vero cells. | - | - | - | - |
| Liposomes | ||||||||
| [1] | It did not assess cell cytotoxicity. Mouse myoblast H9C2 cells for trypanocidal effect | - | Trypanocidal efficacy against trypomastigotes | Trypanocidal efficacy against amastigotes | - | - | BNZ = 55.87 ± 11.39 μM. BNZ-PSs = 56.06 ± 12.21 μM | IC50 de BNZ = 33.07 ± 8.17 μM BNZ-PSs = 3.51 ± 0.79 μM. |
| Other Nanocarriers | ||||||||
| [22] | Cytotoxicity (MTT) in LLCMK2 mammalian cells (Rhesus monkey kidney epithelial cells) | Trypanocidal effect against epimastigotes (6.25–50 μg/mL) | Trypanocidal effect against trypomastigotes | Trypanocidal effect against amastigotes—Bz-NP (8.7 and 17.4 μg/mL) and Bz (56.7 and 113.4 μg/mL) | 55.35 ± 9.03 µg/mL for encapsulated BZN and 160.4 ± 75.09 µg/mL for free BZN | Encapsulated BZN—24 h of 8.72 μg/mL, 48 h of 8.02 μg/mL and 72 h of 4.8 μg/mL. For free BZN: 24 h of 56.7 μg/mL, 48 h of 15.91 μg/mL and 72 h of 4.3 μg/mL | Free BZN LC50: 66.9 ± 20.3 µg/mL. Encapsulated BZN: LC50 1.77 ± 0.58 µg/mL | BZN encapsulated IC50 (8.72 µg/mL). Free BZN IC50 (56.7 µg/mL) |
| [23] | Cytotoxicity (MTT) on NIH-3T3 mammalian cells (isolated mouse fibroblast cell line), J774A.1 (monocyte, mouse macrophage), and Vero (African green monkey renal epithelial cells). | Trypanocidal activity at the following concentrations: 5, 10, 20, 50, 100, and 500 µg/mL of MOFs and MOFs-EP. In addition to MOF suspensions in culture media. | Trypanocidal activity at the following concentrations: 5, 10, 20, 50, 100, and 500 µg/mL of MOFs and MOFs-EP. In addition to MOF suspensions in culture media. | - | (MOFs) CC50 of 392.0 µg/mL for NIH3T3 cells. CC50 of 593.6 µg/mL for J774A.1 cells. CC50 of 1030.0 µg/mL for Vero cells. (MOFs-EP) | Results not shown because they are like those found for trypomastigotes | (MOFs-EP) IC50 of 4.81 μg/mL and 3.0 μg/mL for 24 and 48 h | Not performed. |
| Reference | Animal Model | Infection | Treatment | Control Group | Assays |
|---|---|---|---|---|---|
| Polymeric Nanoparticles | |||||
| [7] | Male C57BL/6 mice aged seven weeks old | Daily intravenous injections of free LIC solution (2.0 mg/kg/day; 8 mice), LYC loaded in biodegradable polymeric NP (LYC-NP; 2.0 mg/kg/day, 10 mice), blank NP (10 mice), and vehicle (control group; 10 rats) for 20 consecutive days | Control group (vehicle, 10 mice) | Transthoracic echocardiography. Single-cell and real-time Ca2+ contracting—imaging. Studies of the cardio-toxicological effects of LYC on cardiac function. Effect of LYC encapsulation on NP. | |
| [8] | Swiss mice aged between 28 and 30 days old and weighing from 20 to 25 g | Infection by trypomastigotes injection 104—Intraperitoneal route | LYC—2 mg/kg/day for 10 and 20 days in the acute phase of the disease. Multiple doses of BZN, free LYC, LIY-PCL NP, unloaded NP, LYC-PLA-PEG NP, and DMA-PEG 300 (i.v. control solution) according to the strain and days. Route—intravenous | Untreated control (infected but untreated), NC unloaded control (UN-NP), and DMA-PEG 300 control (control solution) | Parasitemia level by the Filardi and Brener method. Evaluation of parasitological cure by parasitological methods (examination of fresh blood, blood culture, and PCR in peripheral blood) and conventional serology. |
| [25] | C57BL/6 mice (Female and male mice aged eight weeks old) | 10,000 Trypomastigotes/mouse—Intraperitoneal route | BZN + PLG-Cur. 0.15 mL by gavage/day. BZN. One quarter of 25 mg/kg/day. Cur nanoparticle—One 200 mg/kg daily dose | Uninfected and infected but untreated | (Quantitative PCR). Atrial natriuretic peptide measurements (ELISA). Serum creatine kinase (CK) activity (NADP-reduction photometric assay). Histopathological analysis of the heart (hematoxylin, eosin, and Masson’s trichrome). Myocardial cytokine and chemokine concentrations (ELISA). Enzyme activity by gelatin zymography and transmission densitometry. |
| [29] | Male C57BL/6 mice (20–22 g) | 1 × 103 trypomastigotes (Y strain)—Intraperitoneal route | BZN 2.5 μg/animal/day; blank polymeric nanoparticles; Polymeric PN-UA-2 (13.15 μg/animal/day)—Intra retro-orbital route of samples diluted in 50 μL of PBS | Control group not treated (negative control) | Trypanocidal activity, parasitemia by counting trypomastigote forms of the parasite per 5 µL. Liver markers. |
| [30] | Female Swiss mice aged 28–30 days and weighing 20–25 g. | 10,000 trypomastigotes (Y strain) for the acute phase—Intraperitoneal route. 500 trypomastigotes (Y strain) for chronic phase—Intraperitoneal route | For acute phase: LYC (free LYC, LYC-PCL-NP, and LYC-PLA-PEG-NP) 5 mg/kg for 20 days. A group with BZN for a murine model (100 mg/kg) orally via gavage (0.2 mL). For chronic phase: LIC (free LYC, LYC-PCL-NP, and LYC-PLA-PEG-NP) with LYC doses of 5 mg/kg/day. LYC at 2 mg/kg/day. Two groups received daily BZN doses of 100 mg/kg/day (0.1 mL) and 50 mg/kg/day (0.2 mL)—Orally (gavage) or intravenously (rear vein) | Untreated animals (infected and untreated), animals treated with solution excipients (DMA-PEG), and animals treated with blank NP | Therapeutic efficacy by fresh blood test, blood culture, PCR, and enzyme-linked immunosorbent assay (ELISA). Parasitemia level by FBE method, survival rates, blood culture (BC). |
| [31] | Female Swiss mice (age: 28–30 days; body weight: 20–25 g) | T. cruzi VL-10 strain. Acute phase model: 10,000 trypomastigotes—Intraperitoneal route. Chronic phase model: 500 blood trypomastigotes—Intraperitoneal route. | Free LYC (12 mg/kg of body weight/day), LYC-PLA-PEG-NP (8 or 12 mg/kg/day) or BZN at 100 mg/kg/day—via oral route | Infected and untreated | Treatment efficacy was evaluated by fresh blood test, blood culture, PCR, and enzyme-linked immunosorbent assay (ELISA). T. cruzi VL-10 strain DTU II. Survival rates and heart histopathology. |
| Lipid Nanoparticles | |||||
| [10] | Swiss mice (6–8 weeks old), weighing 20–25 g. | T. cruzi Y strain (Type II linage). 2.0 × 103 trypomastigotes—Intraperitoneal route | BZN, free H2bdtc and H2bdtc-SLNs administered orally at 4 μmol/kg (BZN 1.0 mg/kg/day; free H2bdtc and H2bdtc-SLNs 1.4 mg kg/day) per day for 10 consecutive days | Group 1 = PBS infected and untreated | Cytotoxicity and trypanocidal activity of free H2bdtc and H2bdtc-SLNs in Swiss mice (6–8 weeks old). Evaluation of parasitemia and mortality. Measurement of creatine kinase-MB (CK-MB) and glutamic–pyruvate transaminase levels. Histological analysis to assess inflammatory infiltration through light microscopy DP71. |
| Polymeric Micelles | |||||
| [26] | Female C57BL/6J mice aged 1 month old. | Chronic model of the Trypanosoma cruzi Nicaragua infection. Route—Intraperitoneal with 3000 trypomastigotes. | 30 BZN-MP daily doses at 50 mg/kg/day; 30 BZN-MP daily doses at 25 mg/kg/day; 13 BZN-MP intermittent doses at 75 mg/kg; 13 BZN-MP intermittent doses at 50 mg/kg. Intermittent—One dose every 7 days BZN-MP doses Via—Oral gavage | Infected and untreated (only oil) | Induction of immunosuppression and evaluation of parasitemia by DNA amplification. ECGs performed with electrocardiogram, measurement of IgG antibody response by ELISA, histopathological studies. |
| [27] | Female C3H/HeN mice aged 1 month old. | Trypanosoma cruzi Nicaragua. 1000 trypomastigotes. Route—Intraperitoneal | BZN 50 mg/kg for 30 days; BZN-MP 50 mg/kg/day for 30 days; BZN-MP 25 mg/kg/day for 30 days; BZN-MP 10 mg/kg/day for 30 days. Route—oral gavage | Infected without treatment | Monitoring of parasitemia and of the survival rates. Induction of immunosuppression with cyclophosphamide and estimated number of parasites as described by PCR. Analysis of IgG antibody levels by enzyme-linked immunosorbent assay (ELISA). Histopathological studies by microscopy. |
| [28] | Female C3H/HeN mice aged 1 month old. | 1000 trypomastigotes—Intraperitoneal route. | R-BZN and BZN-MPs were dispersed in olive oil and administered to mice via oral gavage. R-BZN 50 mg/kg/day for 15 days; BZN-MPs 50 mg/kg/day for 15 days; BZN-MPs 50 mg/kg/day for 30 days; BZN-MPs 25 mg/kg/day for 15 days; BZN-MPs 25 mg/kg/day for 30 days; BZN-MPs 10 mg/kg/day for 15 days; BZN-MPs 10 mg/kg/day for 30 days; BZN-MPs 50 mg/kg/day for 30 days (uninfected) | Infected without treatment | Assay in the acute phase of infected mice, parasitemia, antiparasitic effect of BNZ-MPs, survival curve during the acute phase, Kaplan–Meier test to differentiate the curves. |
| Liposomes | |||||
| [1] | Female BALB/c mice (4–6 weeks old) | Infected with the T. cruzi Y strain. 2 × 103—Intraperitoneal route. | PS 0.3 mg/mL by i.v. injection; BZN 100 mg/kg/day orally for 14 days; BZN-PS i.v. at a BZN dose of 1.5 mg/kg (2 doses); BZN-PS i.v. at a BZN dose of 0.15 mg/kg (2 doses), BZN-PS at a BZN dose of 0.03 mg/kg (2 doses) | Infected and untreated | Monitoring of parasitemia, cardiac parasitosis quantified by quantitative PCR, cardiac inflammation, and cardiac histology. Hepatotoxicity. Assessment of toxicity and determination of serum alanine aminotransferase. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paiva, D.d.F.; Matos, A.P.d.S.; Garófalo, D.d.A.; do Nascimento, T.; Monteiro, M.S.d.S.d.B.; Santos-Oliveira, R.; Ricci-Junior, E. Use of Nanocarriers Containing Antitrypanosomal Drugs for the Treatment of Chagas Disease. Pharmaceuticals 2023, 16, 1163. https://doi.org/10.3390/ph16081163
Paiva DdF, Matos APdS, Garófalo DdA, do Nascimento T, Monteiro MSdSdB, Santos-Oliveira R, Ricci-Junior E. Use of Nanocarriers Containing Antitrypanosomal Drugs for the Treatment of Chagas Disease. Pharmaceuticals. 2023; 16(8):1163. https://doi.org/10.3390/ph16081163
Chicago/Turabian StylePaiva, Diogo de Freitas, Ana Paula dos Santos Matos, Denise de Abreu Garófalo, Tatielle do Nascimento, Mariana Sato de Souza de Bustamante Monteiro, Ralph Santos-Oliveira, and Eduardo Ricci-Junior. 2023. "Use of Nanocarriers Containing Antitrypanosomal Drugs for the Treatment of Chagas Disease" Pharmaceuticals 16, no. 8: 1163. https://doi.org/10.3390/ph16081163
APA StylePaiva, D. d. F., Matos, A. P. d. S., Garófalo, D. d. A., do Nascimento, T., Monteiro, M. S. d. S. d. B., Santos-Oliveira, R., & Ricci-Junior, E. (2023). Use of Nanocarriers Containing Antitrypanosomal Drugs for the Treatment of Chagas Disease. Pharmaceuticals, 16(8), 1163. https://doi.org/10.3390/ph16081163