
Relationships between Patient-Reported Outcome Measures and Clinical Measures in Naïve Neovascular Age-Related Macular Degeneration Patients Treated with Intravitreal Ranibizumab

 , , and
, , and 
Abstract
:1. Introduction
2. Results
2.1. Clinical Measures and Response Treatment Evolution
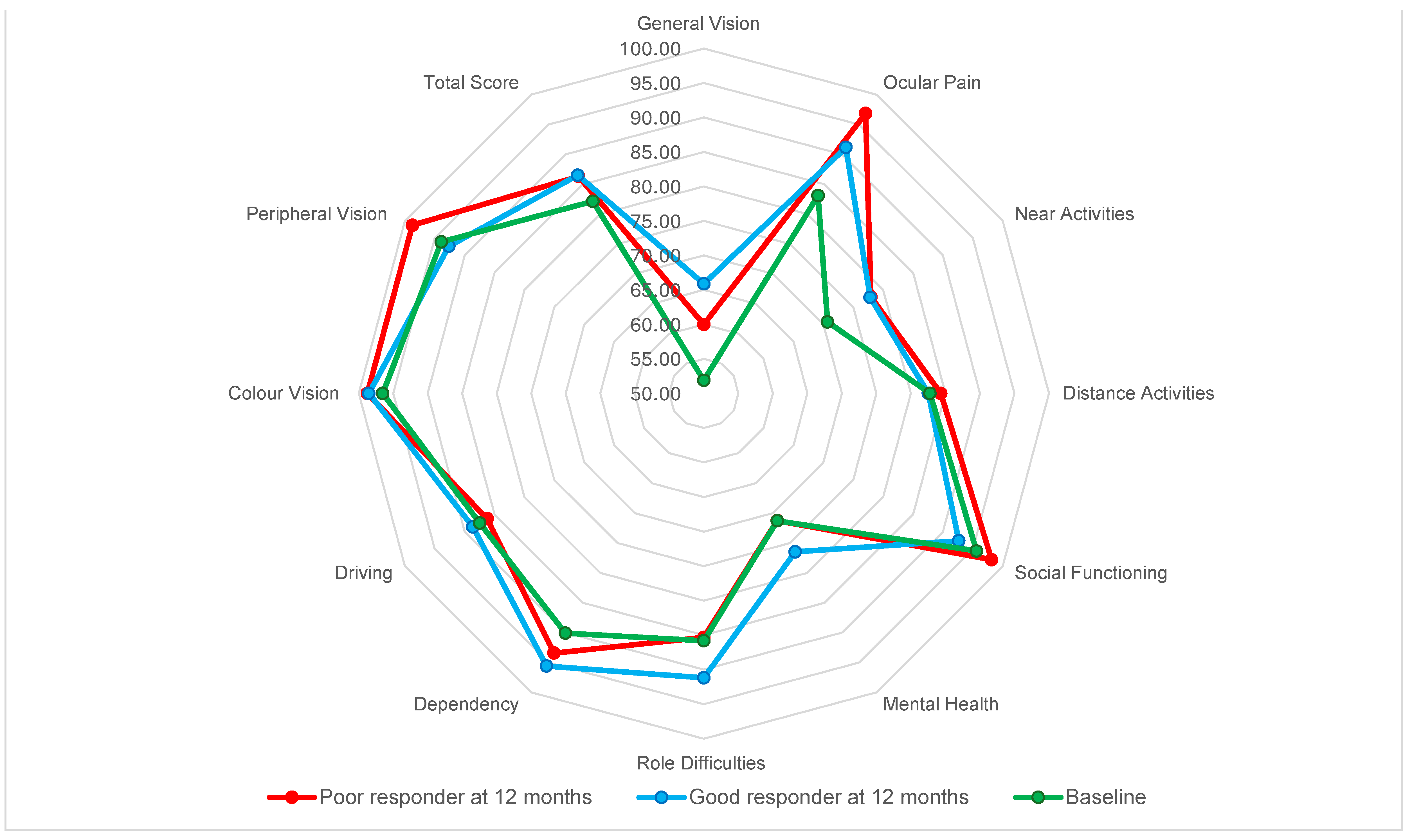
2.2. Patient-Report Outcomes
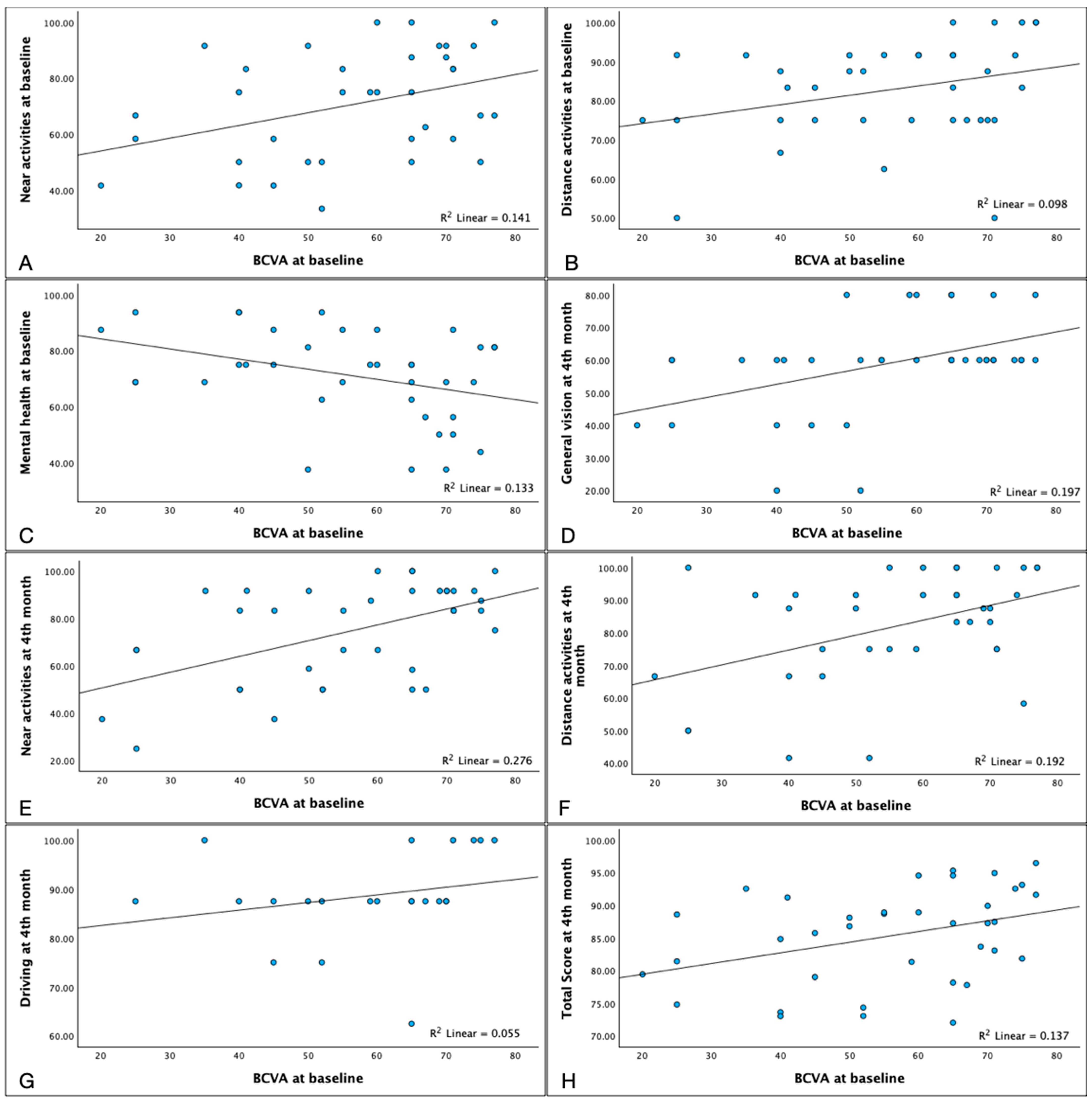
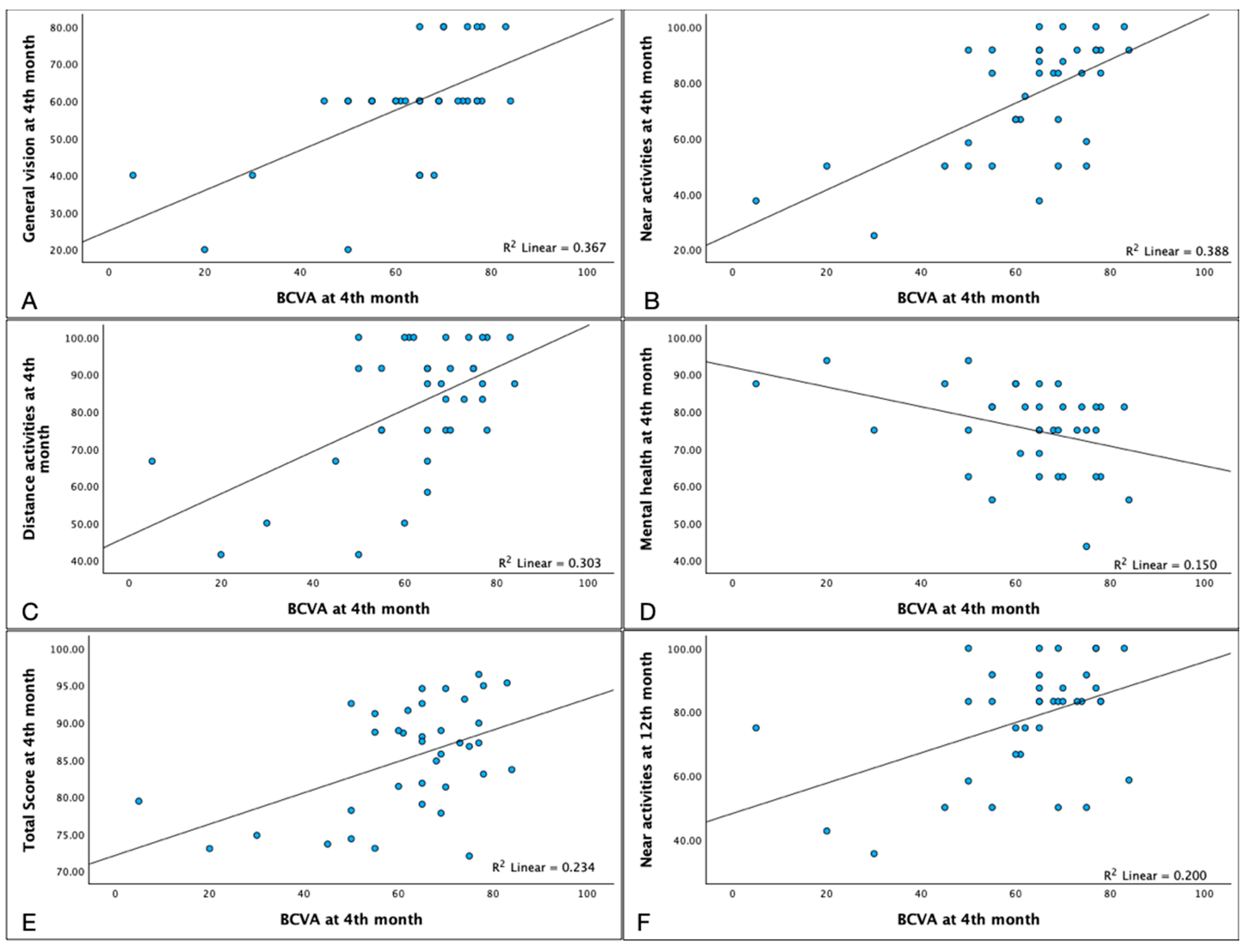
2.3. Relationship between Patient-Reported Outcome Measures and Clinical Measures
3. Discussion
4. Materials and Design
4.1. Patient Selection Criteria
4.2. Clinical Measures
4.3. Classification of Clinical Response
4.4. Patient-Reported Outcome Measures
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AMD | Age-Related Macular Degeneration. |
| EMA | European Medicines Agency |
| ETDRS | Early Treatment Diabetic Retinopathy Study |
| FDA | Food And Drug Administration |
| IRF | Intraretinal Fluid |
| MNV | Macular Neovascularization |
| nAMD | Neovascular Age-Related Macular Degeneration |
| NEI-VFQ 25 | National Eye Institute Visual Functioning Questionnaire–25 |
| OCT | Optical Coherence Tomography |
| PROMs | Patient Reported Outcome Measure |
| QoL | Quality of Life |
| RPE | Retinal Pigmented Epithelium |
| SRF | Subretinal Fluid |
| T&E | Treat and Extend |
| BCVA | Best Corrected Visual Acuity |
| VEGF | Vascular Endothelial Growth Factor |
References
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef]
- Li, J.Q.; Welchowski, T.; Schmid, M.; Mauschitz, M.M.; Holz, F.G.; Finger, R.P. Prevalence and incidence of age-related macular de-generation in Europe: A systematic review and meta-analysis. Br. J. Ophthalmol. 2020, 104, 1077–1084. [Google Scholar] [CrossRef]
- De Jong, P.T.V.M. Age-Related Macular Degeneration. N. Engl. J. Med. 2006, 355, 1474–1485. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Chong, V.; Loewenstein, A.; Larsen, M.; Souied, E.; Schlingemann, R.; Eldem, B.; Monés, J.; Richard, G.; Bandello, F. Guidelines for the management of neovascular age-related macular degeneration by the European Society of Retina Specialists (EURETINA). Br. J. Ophthalmol. 2014, 98, 1144–1167. [Google Scholar] [CrossRef]
- Finger, R.P.; Daien, V.; Eldem, B.M.; Talks, J.S.; Korobelnik, J.-F.; Mitchell, P.; Sakamoto, T.; Wong, T.Y.; Pantiri, K.; Carrasco, J. Anti-vascular endothelial growth factor in neovascular age-related macular degeneration—A systematic review of the impact of anti-VEGF on patient outcomes and healthcare systems. BMC Ophthalmol. 2020, 20, 294. [Google Scholar] [CrossRef] [PubMed]
- Li, E.; Donati, S.; Lindsley, K.B.; Krzystolik, M.G.; Virgili, G. Treatment regimens for administration of anti-vascular endothelial growth factor agents for neovascular age-related macular degeneration. Cochrane Database Syst. Rev. 2020, 2020, CD012208. [Google Scholar] [CrossRef]
- Solomon, S.D.; Lindsley, K.; Vedula, S.S.; Krzystolik, M.G.; Hawkins, B.S. Anti-vascular endothelial growth factor for neovascular age-related macular degeneration. Cochrane Database Syst. Rev. 2019, 2019, CD005139. [Google Scholar] [CrossRef] [PubMed]
- Coleman, A.L.; Yu, F.; Ensrud, K.E.; Stone, K.L.; Cauley, J.A.; Pedula, K.L.; Hochberg, M.C.; Mangione, C.M. Impact of age-related macular degeneration on vi-sion-specific quality of life: Follow-up from the 10-year and 15-year months of the study of osteoporotic fractures. Am. J. Ophthalmol. 2010, 150, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Caballe-Fontanet, D.; Alvarez-Peregrina, C.; Busquet-Duran, N.; Pedemonte-Sarrias, E.; Andreu-Vázquez, C.; Sánchez-Tena, M. Quality of Life and Anxiety in Age Macular Degeneration Patients: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 820. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.J.; Hobby, E.A.; Binns, A.M.; Crabb, D.P. How does age-related macular degeneration affect real-world visual ability and quality of life? A systematic review. BMJ Open 2016, 6, e011504. [Google Scholar] [CrossRef] [PubMed]
- Finger, R.P.; Fleckenstein, M.; Holz, F.G.; Scholl, H.P.N. Quality of life in age-related macular degeneration: A review of available vision-specific psychometric tools. Qual. Life Res. 2008, 17, 559–574. [Google Scholar] [CrossRef] [PubMed]
- Suñer, I.J.; Kokame, G.T.; Yu, E.; Ward, J.; Dolan, C.; Bressler, N.M. Responsiveness of NEI VFQ-25 to Changes in Visual Acuity in Neovascular AMD: Validation Studies from Two Phase 3 Clinical Trials. Investig. Opthalmol. Vis. Sci. 2009, 50, 3629–3635. [Google Scholar] [CrossRef] [PubMed]
- Revicki, D.A.; Rentz, A.M.; Harnam, N.; Thomas, V.S.; Lanzetta, P. Reliability and Validity of the National Eye Institute Visual Function Questionnaire-25 in Patients with Age-Related Macular Degeneration. Investig. Opthalmol. Vis. Sci. 2010, 51, 712–717. [Google Scholar] [CrossRef] [PubMed]
- Jelin, E.; Wisløff, T.; Moe, M.C.; Heiberg, T. Psychometric properties of the National Eye Institute Visual Function Questionnaire (NEI-VFQ 25) in a Norwegian population of patients with neovascular age-related macular degeneration compared to a control population. Health Qual. Life Outcomes 2019, 17, 140. [Google Scholar] [CrossRef] [PubMed]
- Gale, R.P.; Finger, R.P.; Eldem, B.; Aslam, T.; Barratt, J.; Daien, V.; Kodjikian, L.; Loewenstein, A.; Okada, M.; Yin Wong, T.; et al. The management of neovascular age-related macular degeneration: A systematic literature review of patient-reported outcomes, patient mental health and caregiver burden. Acta Ophthalmol. 2023, 101, e26–e42. [Google Scholar] [CrossRef] [PubMed]
- Inan, S.; Cetinkaya, E.; Duman, R.; Dogan, I.; Inan, U.Ü. Quality of life among patients with age-related severe macular degeneration assessed using the NEI-VFQ, HADS-A, HADS-D and SF-36 tests. A cross-sectional study. Sao Paulo Med. J. 2019, 137, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Oshima, Y.; Ishibashi, Y.; Umeda, N.; Nagata, T.; Yoshida, S.; Uchio, E.; Kondo, H.; Sonoda, K.-H.; Ishibashi, T. Correlation between improvement in visual acuity and QOL after Ranibizumab treatment for age-related macular degeneration patients: QUATRO study. BMC Ophthalmol. 2021, 21, 58. [Google Scholar] [CrossRef]
- Garin, N.; Olaya, B.; Lara, E.; Moneta, M.V.; Miret, M.; Ayuso-Mateos, J.L.; Haro, J.M. Visual impairment and multimorbidity in a representative sample of the Spanish population. BMC Public Health 2014, 14, 815. [Google Scholar] [CrossRef]
- Kim, S.; Park, S.J.; Byun, S.J.; Park, K.H.; Suh, H.S. Incremental economic burden associated with exudative age-related macular degeneration: A population-based study. BMC Health Serv. Res. 2019, 19, 828. [Google Scholar] [CrossRef]
- More, P.; Almuhtaseb, H.; Smith, D.; Fraser, S.; Lotery, A.J. Socio-economic status and outcomes for patients with age-related macular degeneration. Eye 2019, 33, 1224–1231. [Google Scholar] [CrossRef]
- Honda, S.; Yanagi, Y.; Koizumi, H.; Chen, Y.; Tanaka, S.; Arimoto, M.; Imai, K. Impact of neovascular age-related macular degeneration: Burden of patients receiving therapies in Japan. Sci. Rep. 2021, 11, 13152. [Google Scholar] [CrossRef]
- Smiddy, W.E. Relative Cost of a Line of Vision in Age-Related Macular Degeneration. Ophthalmology 2007, 114, 847–854. [Google Scholar] [CrossRef]
- Smith, S.E.; Lynch, A.M.; Auer, E.A.; Bol, K.A.; Christopher, K.L.; Mandava, N.; Patnaik, J.L. Visual Functioning and Mortality of Age-Related Macular Degeneration Patients in a Colorado Cohort. Ophthalmol. Retin. 2023, 7, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Wijeyakumar, W.; Syed, A.R.; Joachim, N.; Hong, T.; Broadhead, G.K.; Li, H.; Luo, K.; Chang, A. Vision-related quality of life: 12-month aflibercept treatment in patients with treatment-resistant neovascular age-related macular degeneration. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, A.; Rathinam, S.R.; Gonzales, J.A.; Kelly, N.K.; Thundikandy, R.; Kanakath, A.; Murugan, S.B.; Vedhanayaki, R.; Lim, L.L.; Suhler, E.B.; et al. Association between Quality of Life and Visual Acuity in a Randomized Clinical Trial of Patients with Uveitis Taking Antimetabolites. Ocul. Immunol. Inflamm. 2023, 1–9. [Google Scholar] [CrossRef]
- Sidhu, S.; Lynch, A.M.; Mandava, N.; Manoharan, N.; Mathias, M.T.; Patnaik, J.L. Gender Differences in Visual Functioning Questionnaire Scores among Patients with Age-Related Macular Degeneration. Ophthalmic Epidemiol. 2023, 30, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Pinelli, R.; Bertelli, M.; Scaffidi, E.; Fulceri, F.; Busceti, C.L.; Biagioni, F.; Fornai, F. Measurement of drusen and their correlation with visual symptoms in patients affected by age-related macular degeneration. Arch. Ital. Biol. 2021, 158, 82–104. [Google Scholar] [CrossRef] [PubMed]
- Joko, T.; Nagai, Y.; Mori, R.; Tanaka, K.; Oshima, Y.; Hikichi, Y.; Komori, T.; Carrasco, J.; Maculaitis, M.C.; Will, O.; et al. Patient Preferences for Anti-Vascular Endothelial Growth Factor Treatment for Wet Age-Related Macular Degeneration in Japan: A Discrete Choice Experiment. Patient Prefer. Adherence 2020, 14, 553–567. [Google Scholar] [CrossRef] [PubMed]
- Yuzawa, M.; Fujita, K.; Tanaka, E.; Wang, E.C.Y. Assessing quality of life in the treatment of patients with age-related macular degeneration: Clinical research findings and recommendations for clinical practice. Clin. Ophthalmol. 2013, 7, 1325–1332. [Google Scholar] [CrossRef]
- Chang, T.S.; Bressler, N.M.; Fine, J.T.; Dolan, C.M.; Ward, J.; Klesert, T.R.; MARINA Study Group. Improved vision-related function after ranibizumab treatment of neovascular age-related macular degeneration: Results of a randomized clinical trial. Arch. Ophthalmol. 2007, 125, 1460–1469. [Google Scholar] [CrossRef]
- Bressler, N.M.; Chang, T.S.; Suñer, I.J.; Fine, J.T.; Dolan, C.M.; Ward, J.; Ianchulev, T. Vision-Related Function after Ranibizumab Treatment by Better- or Worse-Seeing Eye: Clinical Trial Results from MARINA and ANCHOR. Ophthalmology 2010, 117, 747–756.e4. [Google Scholar] [CrossRef]
- Gomi, F.; Migita, H.; Sakaguchi, T.; Okada, H.; Sugawara, T.; Hikichi, Y. Vision-related quality of life in Japanese patients with wet age-related macular degeneration treated with intravitreal aflibercept in a real-world setting. Jpn. J. Ophthalmol. 2019, 63, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Submacular Surgery Trials Research Group Evaluation of Minimum Clinically Meaningful Changes in Scores on the National Eye Institute Visual Function Questionnaire (NEI-VFQ) SST Report Number 19. Ophthalmic Epidemiol. 2007, 14, 205–215. [CrossRef] [PubMed]
- Matonti, F.; Korobelnik, J.-F.; Dot, C.; Gualino, V.; Soler, V.; Mrejen, S.; Delyfer, M.-N.; Baillif, S.; Streho, M.; Gascon, P.; et al. Comparative Effectiveness of Intravitreal Anti-Vascular Endothelial Growth Factor Therapies for Managing Neovascular Age-Related Macular Degeneration: A Meta-Analysis. J. Clin. Med. 2022, 11, 1834. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.J.; Chen, C.Y.; Mrejen, S.; Gallego-Pinazo, R.; Xu, L.; Marsiglia, M.; Boddu, S.; Freund, K.B. The Incidence of Neovascular Subtypes in Newly Diagnosed Neovascular Age-Related Macular Degeneration. Arch. Ophthalmol. 2014, 158, 769–779.e2. [Google Scholar] [CrossRef] [PubMed]
- Sadda, S.R.; Guymer, R.; Holz, F.G.; Schmitz-Valckenberg, S.; Curcio, C.A.; Bird, A.C.; Blodi, B.A.; Bottoni, F.; Chakravarthy, U.; Chew, E.Y.; et al. Consensus Definition for Atrophy Associated with Age-Related Macular Degeneration on OCT. Ophthalmology 2018, 125, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Daniel, E.; Shaffer, J.; Ying, G.-S.; Grunwald, J.E.; Martin, D.F.; Jaffe, G.J.; Maguire, M.G. Outcomes in Eyes with Retinal Angiomatous Proliferation in the Comparison of Age-Related Macular Degeneration Treatments Trials (CATT). Ophthalmology 2016, 123, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, A.; Shen, L.L.; Priore, L.V.D. Central geographic atrophy vs. neovascular age—Related macular degeneration: Differences in longitudinal vision-related quality of life. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 307–316. [Google Scholar] [CrossRef]
- Hirneiss, C. The impact of a better-seeing eye and a worse-seeing eye on vision-related quality of life. Clin. Ophthalmol. 2014, 8, 1703–1709. [Google Scholar] [CrossRef]
- Patel, P.J.; Ziemssen, F.; Ng, E.; Muthutantri, A.; Silverman, D.; Tschosik, A.E.; Cantrell, A.R. Burden of Illness in Geographic Atrophy: A Study of Vision-Related Quality of Life and Health Care Resource Use. Clin. Ophthalmol. 2020, 14, 15–28. [Google Scholar] [CrossRef]
- Patnaik, J.L.; Lynch, A.M.; Pecen, P.E.; Jasso, M.; Hanson, K.; Mathias, M.T.; Palestine, A.G.; Mandava, N. The impact of advanced age-related macular de-generation on the National Eye Institute’s Visual Function Questionnaire-25. Acta Ophthalmol. 2021, 99, 750–755. [Google Scholar] [CrossRef]
- Skelly, A.; Taylor, N.; Fasser, C.; Malkowski, J.-P.; Goswami, P.; Downey, L. Patient Preferences in the Management of Wet Age-Related Macular Degeneration: A Conjoint Analysis. Adv. Ther. 2022, 39, 4808–4820. [Google Scholar] [CrossRef]
- Spaide, R.F.; Jaffe, G.J.; Sarraf, D.; Freund, K.B.; Sadda, S.R.; Staurenghi, G.; Chakravarthy, N.K.W.U.; Rosenfeld, P.J.; Holz, F.G.; Souied, E.H.; et al. Consensus Nomenclature for Reporting Neovascular Age-Related Macular Degeneration Data: Consensus on Neovascular Age-Related Macular Degeneration Nomenclature Study Group. Ophthalmology 2020, 127, 616–636. [Google Scholar] [CrossRef]
- Amoaku, W.M.; Chakravarthy, U.; Gale, R.; Gavin, M.; Ghanchi, F.; Gibson, J.; Harding, S.; Johnston, R.L.; Kelly, S.; Lotery, A.; et al. Defining response to anti-VEGF therapies in neovascular AMD. Eye 2015, 29, 721–731. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 37 | Poor Responder 12 Months n = 20 (54%) | Good Responder 12 Months n = 17 (46%) | p-Value | |
|---|---|---|---|---|
| Sex | Male 14 (38%) | Male 8 (40%) | Male 6 (35%) | 0.776 + |
| Female 23 (62%) | Female 12 (60%) | Female 11 (65%) | ||
| Age | 79.19 (±8.01) | 78.85 (±7.93) | 79.59 (±8.34) | 0.785 + |
| Total NEI-VFQ 25 score at baseline (Mean, SD) | 82.14 (±8.32) | 81.92 (±9.42) | 82.39 (±7.09) | 0.865 + |
| Total NEI-VFQ 25 score at month 4 (Mean, SD) | 85.30 (±7.26) | 85.52 (±7.62) | 85.05 (±7.05) | 0.846 + |
| Total NEI-VFQ 25 score at month 12 (Mean, SD) | 86.41 (±6.51) | 86.31 (±7.04) | 86.52 (±6.03) | 0.924 + |
| Response at month 4 | 0.743 * | |||
| Poor responder (n, %) | 13, 35% | 8, 40% | 6, 35% | |
| Good responder (n, %) | 24, 65% | 12, 60% | 11, 65% | |
| Total injections (Mean, IQR) | 9 (8–10) | 9 (8–10) | 9 (8–9) | 0.059 ‡ |
| Weeks between injection (Mean, IQR) | 8 (6–9) | 7 (6–8) | 9 (7–9) | 0.048 ‡ |
| Variables | Total n = 37 | Poor Responder 4 Months n = 13 (35%) | Good Responder 4 Months n = 24 (65%) | p-Value |
|---|---|---|---|---|
| BCVA at baseline (Median, IQR) | 60 (43–70) | 65 (45–72) | 57 (42–67) | 0.291 ‡ |
| BCVA at month 4 (Median, IQR) | 65 (55–75) | 65 (53–73) | 69 (56–75) | 0.369 ‡ |
| BCVA at month 12 (Median, IQR) | 71 (63–77) | 70 (61–80) | 71 (63–77) | 1.000 ‡ |
| CFT at baseline (Median µm, IQR) | 310 (267–364) | 333 (234–406) | 296 (266–354) | 0.743 ‡ |
| CFT at month 4 (Median µm, IQR) | 214 (200–250) | 205 (195–296) | 216 (201–247) | 0.888 ‡ |
| CFT at month 12 (Median µm, IQR) | 232 (212–274) | 229 (195–319) | 233 (214–261) | 0.987 ‡ |
| IRF at baseline (n, %) | 0.013 * | |||
| Absence | 13, 35% | 8, 62% | 5, 21% | |
| Present | 24, 65% | 5, 38% | 19, 79% | |
| IRF at month 4 (n, %) | 0.874 * | |||
| Absence | 29, 78% | 10, 77% | 19, 79% | |
| Present | 8, 22% | 3, 23% | 5, 21% | |
| SRF at baseline (n, %) | 0.896 * | |||
| Absence | 9, 24% | 3, 23% | 6, 25% | |
| Present | 28, 76% | 10, 77% | 18, 75% | |
| SRF at month 4 (n, %) | 0.002 * | |||
| Absence | 28, 76% | 6, 46% | 22, 92% | |
| Present | 9, 24% | 7, 54% | 2, 8% | |
| SRF at month 12 (n, %) | 0.320 * | |||
| Absence | 29,78% | 9, 69% | 20, 83% | |
| Present | 8, 22% | 4, 31% | 4, 17% | |
| Sub-RPE fluid at baseline (n, %) | 0.515 * | |||
| Absence | 11, 30% | 3, 23% | 8, 33% | |
| Present | 26, 70% | 10, 77% | 16, 67% | |
| Sub-RPE fluid at month 4 (n, %) | 0.047 * | |||
| Absence | 26, 70% | 6, 46% | 20, 83% | |
| Present | 11, 30% | 7, 54% | 4, 17% | |
| Sub-RPE fluid at month 12 (n, %) | 0.405 | |||
| Absence | 31, 84% | 10, 77% | 21, 88% | |
| Present | 6, 76% | 3, 23% | 3, 12% | |
| Fibrosis at baseline (n, %) | 1.000 | |||
| Absence | 37, 100% | 37, 100% | 37, 100% | |
| Present | 0, 0% | 0, 0% | 0, 0% | |
| Fibrosis at month 4 (n, %) | 0.806 * | |||
| Absence | 32, 86% | 11, 85% | 21, 88% | |
| Present | 5, 14% | 2, 15% | 3, 12% | |
| Fibrosis at month 12 (n, %) | 0.686 * | |||
| Absence | 30, 81% | 11, 85% | 19, 79% | |
| Present | 7, 19% | 2, 15% | 5, 21% |
| Variables | Total n = 37 | Poor Responder 12 Months n = 20 (54%) | Good Responder 12 Months n = 17 (46%) | p-Value |
|---|---|---|---|---|
| BCVA at baseline (median, IQR) | 60 (43–70) | 58 (41–65) | 65 (45–71) | 0.292 * |
| BCVA at month 4 (Median, IQR) | 65 (55–75) | 65 (55–69) | 69 (60–77) | 0.264 ‡ |
| BCVA at month 12 (Median, IQR) | 71 (63–77) | 68 (62–76) | 72 (65–80) | 0.306 ‡ |
| CFT at baseline (Median µm, IQR) | 310 (267–364) | 341 (256–372) | 290 (270–345) | 0.503 ‡ |
| CFT at month 4 (Median µm, IQR) | 214 (200–250) | 220 (193–249) | 211 (203–250) | 0.737 ‡ |
| CFT at months 12 (Median µm, IQR) | 232 (212–274) | 235 (223–261) | 224 (205–275) | 0.503 ‡ |
| IRF at baseline (n, %) | 0.501 * | |||
| Absence | 13, 35% | 8, 40% | 5, 29% | |
| Present | 24, 65% | 12, 60% | 12, 71% | |
| IRF at month 4 (n, %) | 0.179 * | |||
| Absence | 29, 78% | 14, 70% | 15, 88% | |
| Present | 8, 22% | 6, 30% | 2, 12% | |
| IRF at month 12 (n, %) | 0.016 * | |||
| Absence | 28, 76% | 12, 60% | 16, 94% | |
| Present | 9, 24% | 8, 40% | 1, 6% | |
| SRF at baseline (n, %) | 0.383 * | |||
| Absence | 9, 24% | 6, 30% | 3, 18% | |
| Present | 28, 76% | 14, 70% | 14, 82% | |
| SRF at month 4 (n, %) | 0.917 * | |||
| Absence | 28, 76% | 15, 75% | 13, 76 | |
| Present | 9, 24% | 5, 25% | 4, 24% | |
| SRF at month 12 (n, %) | 0.179 * | |||
| Absence | 29, 78% | 14, 70% | 15, 88% | |
| Present | 8, 22% | 6, 40% | 2, 12% | |
| Sub-RPE fluid at baseline (n, %) | 0.160 * | |||
| Absence | 11, 30% | 4, 20% | 7, 41% | |
| Present | 26, 70% | 16, 80% | 10, 59% | |
| Sub-RPE fluid at month 4 (n,%) | 0.138 * | |||
| Absence | 26, 70% | 12, 60% | 14, 82% | |
| Present | 11, 30% | 8, 40% | 3, 18% | |
| Sub-RPE fluid at month 4 (n,%) | 0.498 * | |||
| Absence | 31, 84% | 16, 80% | 15, 88% | |
| Present | 6, 76% | 4, 20% | 2, 12% | |
| Fibrosis at baseline (n,%) | 0.622 * | |||
| Absence | 37, 100% | 20, 100% | 17, 100% | |
| Present | 0, 0% | 0, 0% | 0, 0% | |
| Fibrosis at month 4 (n,%) | 0.211 * | |||
| Absence | 32, 86% | 16, 80% | 16, 94% | |
| Present | 5, 14% | 4, 20% | 1, 6% | |
| Fibrosis at month 4 (n,%) | 0.856 * | |||
| Absence | 30, 81% | 16, 80% | 14, 82% | |
| Present | 7, 19% | 4, 20% | 3, 18% |
| Variables | Total n = 37 | Poor Responder 12 Months n = 20 (54%) | Good Responder 12 Months n = 17 (46%) | p-Value |
|---|---|---|---|---|
| General Vision Mean, (SD) | 3.78 (±12.33) | 1.00 (±10.21) | 7.06 (±14.04) | 0.244 * |
| Ocular Pain Mean, (SD) | 2.70 (±8.40) | 4.38 (±7.34) | 0.74 (±9.34) | 0.341 * |
| Near Activities Mean, (SD) | 3.35 (±15.20) | 4.61 (±13.74) | 1.87 (±17.06) | 0.460 * |
| Distance Activities Mean, (SD) | 1.54 (±1.38) | −1.90 (±9.68) | 5.57 (±12.17) | 0.341 * |
| Social Functioning Mean, (SD) | −0.68 (±5.06) | 0.00 (±4.10) | −1.47 (±6.06) | 0.577 * |
| Mental Health Mean, (SD) | −1.69 (±8.54) | −3.12 (±9.62) | 0.00 (±6.99) | 0.357 * |
| Role Difficulties Mean, (SD) | 2.21 (±9.58) | 2.83 (±7.23) | 1.47 (±11.59) | 0.357 * |
| Dependency Mean, (SD) | 1.39 (±5.81) | 0.88 (±2.63) | 1.96 (±8.09) | 0.851 * |
| Driving Mean, (SD) | −1.19 (±3.76) | −1.25 (±3.95) | −1.14 (±3.77) | 0.973 * |
| Color Vision Mean, (SD) | −0.69 (±4.17) | 0.00 (±0.00) | −1.56 (±6.25) | 0.765 * |
| Peripheral Vision Mean, (SD) | 0.00 (±5.89) | 0.00 (±0.00) | 0.00 (±8.84) | 1.000 * |
| Total Score Mean, (SD) | 1.11 (±3.66) | 0.80 (±3.07) | 1.47 (±4.33) | 0.775 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almuiña-Varela, P.; García-Quintanilla, L.; Rodríguez-Cid, M.J.; Gil-Martínez, M.; Abraldes, M.J.; Gómez-Ulla, F.; Estany-Gestal, A.; Alcántara-Espinosa, J.M.; Fernández-Rodríguez, M.; Fernández-Ferreiro, A. Relationships between Patient-Reported Outcome Measures and Clinical Measures in Naïve Neovascular Age-Related Macular Degeneration Patients Treated with Intravitreal Ranibizumab. Pharmaceuticals 2024, 17, 157. https://doi.org/10.3390/ph17020157
Almuiña-Varela P, García-Quintanilla L, Rodríguez-Cid MJ, Gil-Martínez M, Abraldes MJ, Gómez-Ulla F, Estany-Gestal A, Alcántara-Espinosa JM, Fernández-Rodríguez M, Fernández-Ferreiro A. Relationships between Patient-Reported Outcome Measures and Clinical Measures in Naïve Neovascular Age-Related Macular Degeneration Patients Treated with Intravitreal Ranibizumab. Pharmaceuticals. 2024; 17(2):157. https://doi.org/10.3390/ph17020157
Chicago/Turabian StyleAlmuiña-Varela, Pablo, Laura García-Quintanilla, María José Rodríguez-Cid, María Gil-Martínez, Maximino J. Abraldes, Francisco Gómez-Ulla, Ana Estany-Gestal, Jorge Miguel Alcántara-Espinosa, Maribel Fernández-Rodríguez, and Anxo Fernández-Ferreiro. 2024. "Relationships between Patient-Reported Outcome Measures and Clinical Measures in Naïve Neovascular Age-Related Macular Degeneration Patients Treated with Intravitreal Ranibizumab" Pharmaceuticals 17, no. 2: 157. https://doi.org/10.3390/ph17020157
APA StyleAlmuiña-Varela, P., García-Quintanilla, L., Rodríguez-Cid, M. J., Gil-Martínez, M., Abraldes, M. J., Gómez-Ulla, F., Estany-Gestal, A., Alcántara-Espinosa, J. M., Fernández-Rodríguez, M., & Fernández-Ferreiro, A. (2024). Relationships between Patient-Reported Outcome Measures and Clinical Measures in Naïve Neovascular Age-Related Macular Degeneration Patients Treated with Intravitreal Ranibizumab. Pharmaceuticals, 17(2), 157. https://doi.org/10.3390/ph17020157