
Switching from Beraprost to Selexipag in the Treatment of Pulmonary Arterial Hypertension: Insights from a Phase IV Study of the Japanese Registry (The EXCEL Study: EXChange from bEraprost to seLexipag Study)

 , , and
, , and 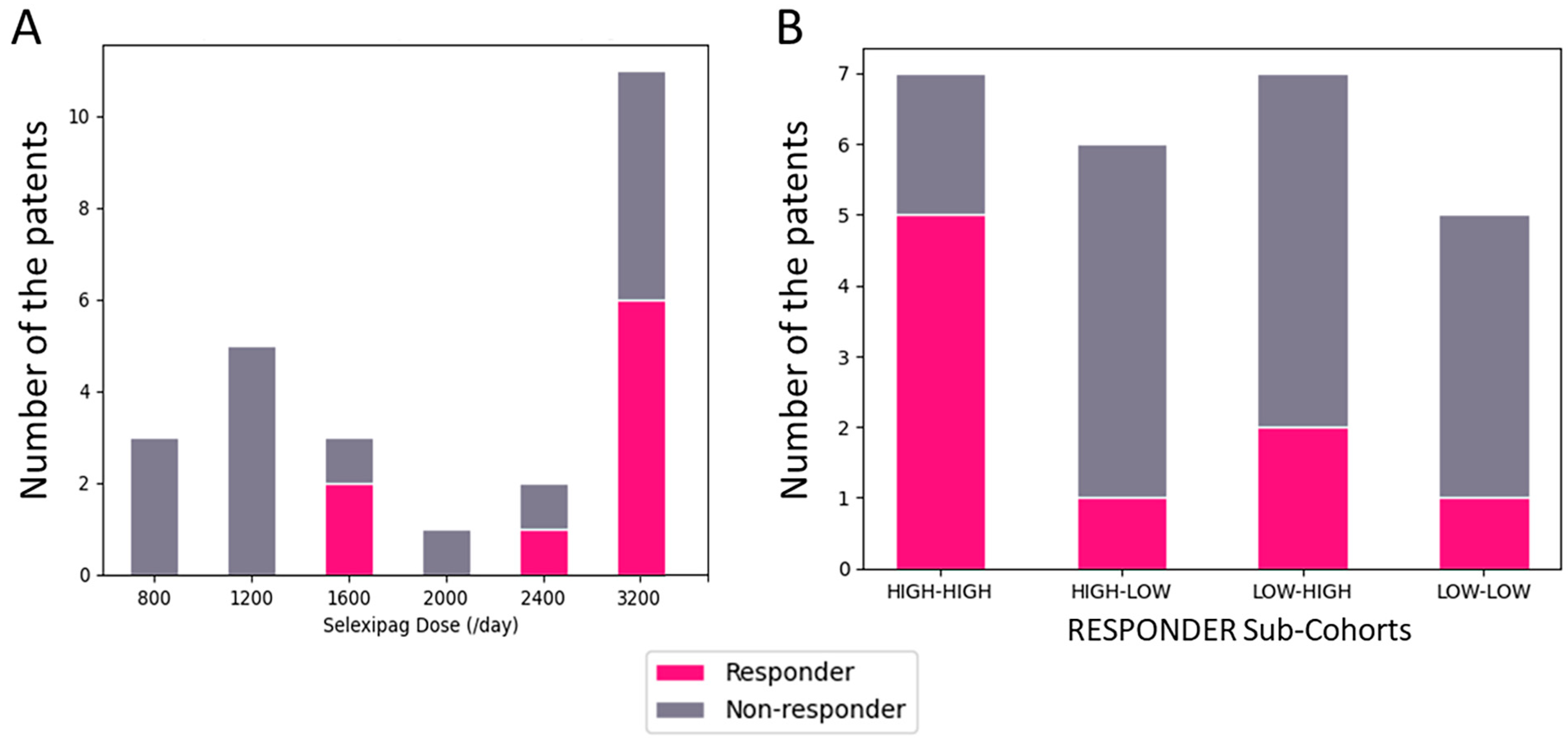{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Dosing of Selexipag and Tolerability
2.3. Hemodynamic and Exercise Capacity Outcomes
2.4. Responder Analysis
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Inclusion Criteria
4.3. Data Collection
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Humbert, M.; Guignabert, C.; Bonnet, S.; Dorfmüller, P.; Klinger, J.R.; Nicolls, M.R.; Olschewski, A.J.; Pullamsetti, S.S.; Schermuly, R.T.; Stenmark, K.R.; et al. Pathology and Pathobiology of Pulmonary Hypertension: State of the Art and Research Perspectives. Eur. Respir. J. Off. J. Eur. Soc. Clin. Respir. Physiol. 2019, 53, 1801887. [Google Scholar] [CrossRef]
- Galiè, N.; Channick, R.N.; Frantz, R.P.; Grünig, E.; Jing, Z.C.; Moiseeva, O.; Preston, I.R.; Pulido, T.; Safdar, Z.; Tamura, Y.; et al. Risk Stratification and Medical Therapy of Pulmonary Arterial Hypertension. Eur. Respir. J. Off. J. Eur. Soc. Clin. Respir. Physiol. 2019, 53, 1801889. [Google Scholar] [CrossRef] [PubMed]
- Tamura, Y.; Kumamaru, H.; Inami, T.; Matsubara, H.; Hirata, K.-I.; Tsujino, I.; Suda, R.; Miyata, H.; Nishimura, S.; Sigel, B.; et al. Changes in the Characteristics and Initial Treatments of Pulmonary Hypertension between 2008 and 2020 in Japan. JACC Asia 2022, 2, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Tamura, Y.; Kumamaru, H.; Nishimura, S.; Nakajima, Y.; Matsubara, H.; Taniguchi, Y.; Tsujino, I.; Shigeta, A.; Kinugawa, K.; Kimura, K.; et al. Initial Triple Combination Therapy Including Intravenous Prostaglandin I2 for the Treatment of Patients with Severe Pulmonary Arterial Hypertension. Int. Heart J. 2023, 64, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Humbert, M.; Lau, E.M.; Montani, D.; Jaïs, X.; Sitbon, O.; Simonneau, G. Advances in therapeutic interventions for patients with pulmonary arterial hypertension. Circulation 2014, 130, 2189–2208. [Google Scholar] [CrossRef] [PubMed]
- Shao, D.; Park, J.E.; Wort, S.J. The role of endothelin-1 in the pathogenesis of pulmonary arterial hypertension. Pharmacol. Res. 2011, 63, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Humbert, M.; Ghofrani, H.A. The molecular targets of approved treatments for pulmonary arterial hypertension. Thorax 2016, 71, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Rubin, L.J.; Badesch, D.B.; Barst, R.J.; Galiè, N.; Black, C.M.; Keogh, A.; Pulido, T.; Frost, A.; Roux, S.; Leconte, I.; et al. Bosentan therapy for pulmonary arterial hypertension. N. Engl. J. Med. 2002, 346, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; Olschewski, H.; Oudiz, R.J.; Torres, F.; Frost, A.; Ghofrani, H.A.; Badesch, D.B.; McGoon, M.D.; McLaughlin, V.V.; Roecker, E.B.; et al. Ambrisentan for the treatment of pulmonary arterial hypertension: Results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, efficacy (ARIES) study 1 and 2. Circulation 2008, 117, 3010–3019. [Google Scholar] [CrossRef] [PubMed]
- Pulido, T.; Adzerikho, I.; Channick, R.N.; Delcroix, M.; Galiè, N.; Ghofrani, A.; Jansa, P.; Jing, Z.-C.; Le Brun, F.-O.; Mehta, S.; et al. Macitentan and morbidity and mortality in pulmonary arterial hypertension. N. Engl. J. Med. 2013, 369, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Follmann, M.; Griebenow, N.; Hahn, M.G.; Hartung, I.; Mais, F.; Mittendorf, J.; Schäfer, M.; Schirok, H.; Stasch, J.; Stoll, F.; et al. The chemistry and biology of soluble guanylate cyclase stimulators and activators. Angew. Chem. Int. Ed. 2013, 52, 9442–9462. [Google Scholar] [CrossRef] [PubMed]
- Klinger, J.R.; Abman, S.H.; Gladwin, M.T. Nitric oxide deficiency and endothelial dysfunction in pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 2013, 188, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Ghofrani, H.-A.; Galiè, N.; Grimminger, F.; Grünig, E.; Humbert, M.; Jing, Z.-C.; Keogh, A.M.; Langleben, D.; Kilama, M.O.; Fritsch, A.; et al. Riociguat for the treatment of pulmonary arterial hypertension. N. Engl. J. Med. 2013, 369, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Nagaya, N.; Uematsu, M.; Okano, Y.; Satoh, T.; Kyotani, S.; Sakamaki, F.; Nakanishi, N.; Miyatake, K.; Kunieda, T. Effect of Orally Active Prostacyclin Analogue on Survival of Outpatients with Primary Pulmonary Hypertension. J. Am. Coll. Cardiol. 1999, 34, 1188–1192. [Google Scholar] [CrossRef] [PubMed]
- Barst, R.J.; McGoon, M.; McLaughlin, V.; Tapson, V.; Oudiz, R.; Shapiro, S.; Robbins, I.M.; Channick, R.; Badesch, D.; Rayburn, B.K.; et al. Beraprost Therapy for Pulmonary Arterial Hypertension. J. Am. Coll. Cardiol. 2003, 41, 2119–2125. [Google Scholar] [CrossRef] [PubMed]
- Sitbon, O.; Channick, R.; Chin, K.M.; Frey, A.; Gaine, S.; Galiè, N.; Ghofrani, H.-A.; Hoeper, M.M.; Lang, I.M.; Preiss, R.; et al. Selexipag for the Treatment of Pulmonary Arterial Hypertension. N. Engl. J. Med. 2015, 373, 2522–2533. [Google Scholar] [CrossRef] [PubMed]
- Takatsuki, S.; Nakayama, T.; Shimizu, Y.; Kawai, R.; Matsuura, H. Clinical Efficacy and Safety of Selexipag in Children and Young Adults with Idiopathic and Heritable Pulmonary Arterial Hypertension. Cardiol. Young 2023, 33, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, N.; Ikeda, S.; Tahara, N.; Fukuda, K.; Hatano, M.; Ito, H.; Nakayama, T.; Anzai, T.; Hashimoto, A.; Inoue, T.; et al. Efficacy and Safety of an Orally Administered Selective Prostacyclin Receptor Agonist, Selexipag, in Japanese Patients with Pulmonary Arterial Hypertension. Circ. J. Off. J. Jpn. Circ. Soc. 2017, 81, 1360–1367. [Google Scholar] [CrossRef] [PubMed]
- Tamura, Y.; Kumamaru, H.; Abe, K.; Satoh, T.; Miyata, H.; Ogawa, A.; Tanabe, N.; Hatano, M.; Yao, A.; Tsujino, I.; et al. Improvements in French Risk Stratification Score Were Correlated with Reductions in Mean Pulmonary Artery Pressure in Pulmonary Arterial Hypertension: A Subanalysis of the Japan Pulmonary Hypertension Registry (JAPHR). BMC Pulm. Med. 2021, 21, 28. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamura, Y.; Kumamaru, H.; Tsujino, I.; Suda, R.; Abe, K.; Inami, T.; Horimoto, K.; Adachi, S.; Yasuda, S.; Sera, F.; et al. Switching from Beraprost to Selexipag in the Treatment of Pulmonary Arterial Hypertension: Insights from a Phase IV Study of the Japanese Registry (The EXCEL Study: EXChange from bEraprost to seLexipag Study). Pharmaceuticals 2024, 17, 555. https://doi.org/10.3390/ph17050555
Tamura Y, Kumamaru H, Tsujino I, Suda R, Abe K, Inami T, Horimoto K, Adachi S, Yasuda S, Sera F, et al. Switching from Beraprost to Selexipag in the Treatment of Pulmonary Arterial Hypertension: Insights from a Phase IV Study of the Japanese Registry (The EXCEL Study: EXChange from bEraprost to seLexipag Study). Pharmaceuticals. 2024; 17(5):555. https://doi.org/10.3390/ph17050555
Chicago/Turabian StyleTamura, Yuichi, Hiraku Kumamaru, Ichizo Tsujino, Rika Suda, Kohtaro Abe, Takumi Inami, Koshin Horimoto, Shiro Adachi, Satoshi Yasuda, Fusako Sera, and et al. 2024. "Switching from Beraprost to Selexipag in the Treatment of Pulmonary Arterial Hypertension: Insights from a Phase IV Study of the Japanese Registry (The EXCEL Study: EXChange from bEraprost to seLexipag Study)" Pharmaceuticals 17, no. 5: 555. https://doi.org/10.3390/ph17050555
APA StyleTamura, Y., Kumamaru, H., Tsujino, I., Suda, R., Abe, K., Inami, T., Horimoto, K., Adachi, S., Yasuda, S., Sera, F., Taniguchi, Y., Kuwana, M., & Tatsumi, K., on behalf of the Japan Pulmonary Hypertension Registry Network. (2024). Switching from Beraprost to Selexipag in the Treatment of Pulmonary Arterial Hypertension: Insights from a Phase IV Study of the Japanese Registry (The EXCEL Study: EXChange from bEraprost to seLexipag Study). Pharmaceuticals, 17(5), 555. https://doi.org/10.3390/ph17050555