

The Potential Role of sPD-L1 as a Predictive Biomarker in EGFR-Positive Non-Small-Cell Lung Cancer
 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Sample Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jia, Y.; Li, X.; Zhao, C.; Ren, S.; Su, C.; Gao, G.; Li, W.; Zhou, F.; Li, J.; Zhou, C. Soluble PD-L1 as a Predictor of the Response to EGFR-TKIs in Non-small Cell Lung Cancer Patients With EGFR Mutations. Front. Oncol. 2020, 10, 1455. [Google Scholar] [CrossRef] [PubMed]
- Okuma, Y.; Hosomi, Y.; Nakahara, Y.; Watanabe, K.; Sagawa, Y.; Homma, S. High plasma levels of soluble programmed cell death ligand 1 are prognostic for reduced survival in advanced lung cancer. Lung Cancer 2017, 104, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Costantini, A.; Takam Kamga, P.; Dumenil, C.; Chinet, T.; Emile, J.F.; Giroux Leprieur, E. Plasma Biomarkers and Immune Checkpoint Inhibitors in Non-Small Cell Lung Cancer: New Tools for Better Patient Selection? Cancers 2019, 11, 1269. [Google Scholar] [CrossRef] [PubMed]
- Han, J.J.; Kim, D.W.; Koh, J.; Keam, B.; Kim, T.M.; Jeon, Y.K.; Lee, S.H.; Chung, D.H.; Heo, D.S. Change in PD-L1 Expression After Acquiring Resistance to Gefitinib in EGFR-Mutant Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2016, 17, 263–270.e2. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.H.; Huang, Y.H.; Tseng, J.S.; Chen, K.C.; Ku, W.H.; Su, K.Y.; Chen, J.J.W.; Chen, H.W.; Yu, S.L.; Yang, T.Y.; et al. High PD-L1 expression correlates with primary resistance to EGFR-TKIs in treatment naïve advanced EGFR-mutant lung adenocarcinoma patients. Lung Cancer 2019, 127, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Su, S.; Dong, Z.Y.; Xie, Z.; Yan, L.X.; Li, Y.F.; Su, J.; Liu, S.Y.; Yin, K.; Chen, R.L.; Huang, S.M.; et al. Strong Programmed Death Ligand 1 Expression Predicts Poor Response and De Novo Resistance to EGFR Tyrosine Kinase Inhibitors Among NSCLC Patients With EGFR Mutation. J. Thorac. Oncol. 2018, 13, 1668–1675. [Google Scholar] [CrossRef] [PubMed]
- Abu Hejleh, T.; Furqan, M.; Ballas, Z.; Clamon, G. The clinical significance of soluble PD-1 and PD-L1 in lung cancer. Crit. Rev. Oncol. Hematol. 2019, 143, 148–152. [Google Scholar] [CrossRef]
- Li, C.; Li, C.; Zhi, C.; Liang, W.; Wang, X.; Chen, X.; Lv, T.; Shen, Q.; Song, Y.; Lin, D.; et al. Clinical significance of PD-L1 expression in serum-derived exosomes in NSCLC patients. J. Transl. Med. 2019, 17, 355. [Google Scholar] [CrossRef]
- Zhu, X.; Lang, J. Soluble PD-1 and PD-L1: Predictive and prognostic significance in cancer. Oncotarget 2017, 8, 97671–97682. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Xu, B.; Wang, Y.; Wu, C.; Jiang, J.; Wu, C. Prognostic significance of circulating soluble programmed death ligand-1 in patients with solid tumors: A meta-analysis. Medicine 2018, 97, e9617. [Google Scholar] [CrossRef] [PubMed]
- Larsen, T.V.; Maansson, C.T.; Daugaard, T.F.; Andresen, B.S.; Sorensen, B.S.; Nielsen, A.L. Trans-Regulation of Alternative PD-L1 mRNA Processing by CDK12 in Non-Small-Cell Lung Cancer Cells. Cells 2023, 12, 2844. [Google Scholar] [CrossRef] [PubMed]
- Bailly, C.; Thuru, X.; Quesnel, B. Soluble Programmed Death Ligand-1 (sPD-L1): A Pool of Circulating Proteins Implicated in Health and Diseases. Cancers 2021, 13, 3034. [Google Scholar] [CrossRef]
- Sagawa, R.; Sakata, S.; Gong, B.; Seto, Y.; Takemoto, A.; Takagi, S.; Ninomiya, H.; Yanagitani, N.; Nakao, M.; Mun, M.; et al. Solubile PD-L1 works as a decoy in lung cancer immunotherapy via alternative polyadenylation. JCI Insight 2022, 7, e153323. [Google Scholar] [CrossRef]
- Zhang, N.; Zeng, Y.; Du, W.; Zhu, J.; Shen, D.; Liu, Z.; Huang, J.A. The EGFR pathway is involved in the regulation of PD-L1 expression via the IL-6/JAK/STAT3 signaling pathway in EGFR-mutated non-small cell lung cancer. Int. J. Oncol. 2016, 49, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, J.V.; Greulich, H.; Sellers, W.R.; Meyerson, M.; Frank, D.A. Signal transducer and activator of transcription 3 is required for the oncogenic effects of non-small-cell lung cancer-associated mutations of the epidermal growth factor receptor. Cancer Res. 2006, 66, 3162–3168. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Fang, W.; Zhan, J.; Hong, S.; Tang, Y.; Kang, S.; Zhang, Y.; He, X.; Zhou, T.; Qin, T.; et al. Upregulation of PD-L1 by EGFR Activation Mediates the Immune Escape in EGFR-Driven NSCLC: Implication for Optional Immune Targeted Therapy for NSCLC Patients with EGFR Mutation. J. Thorac. Oncol. 2015, 10, 910–923. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Gao, J.; Li, Y.; Nie, J.; Dai, L.; Hu, W.; Chen, X.; Han, J.; Ma, X.; Tian, G.; et al. Circulating PD-L1 in NSCLC patients and the correlation between the level of PD-L1 expression and the clinical characteristics. Thorac. Cancer 2015, 6, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Choi, H.; Lee, S.M. Parametric and non-parametric estimation of reference intervals for routine laboratory tests: An analysis of health check-up data for 260 889 young men in the South Korean military. BMJ Open 2022, 12, e062617. [Google Scholar] [CrossRef] [PubMed]
- Skoulidis, F.; Heymach, J.V. Co-occurring genomic alterations in non-small-cell lung cancer biology and therapy. Nat. Rev. Cancer 2019, 19, 495–509. [Google Scholar] [CrossRef] [PubMed]
- Jiao, X.D.; Qin, B.D.; You, P.; Cai, J.; Zang, Y.S. The prognostic value of TP53 and its correlation with EGFR mutation in advanced non-small cell lung cancer, an analysis based on cBioPortal data base. Lung Cancer 2018, 123, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Sun, C.; Li, J.; Hu, L.; Li, M.; Liu, J.; Pu, L.; Xiong, S. The Prognostic Significance of Soluble Programmed Death Ligand 1 Expression in Cancers: A Systematic Review and Meta-analysis. Scand. J. Immunol. 2017, 86, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Si, J.; Liu, Y.; Wang, H.; Ni, R.; Wang, J. Elevated serum soluble programmed cell death ligand 1 concentration as a potential marker for poor prognosis in small cell lung cancer patients with chemotherapy. Respir. Res. 2018, 19, 197. [Google Scholar] [CrossRef]
- Jovanović, D.; Roksandić-Milenković, M.; Kotur-Stevuljević, J.; Ćeriman, V.; Vukanić, I.; Samardžić, N.; Popević, S.; Ilić, B.; Gajić, M.; Simon, M.; et al. Soluble sPD-L1 and Serum Amyloid A1 as Potential Biomarkers for Lung Cancer. J. Med. Biochem. 2019, 38, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.Q.; Chen, Y.; Pan, X.; Xing, Y.F.; Shi, M.H.; Chen, Y.J. Level of soluble programmed death-1 ligand 1 in peripheral blood of patients with advanced epidermal growth factor receptor mutated lung adenocarcinoma and its clinical implications. Zhonghua Yi Xue Za Zhi 2016, 96, 3870–3874. [Google Scholar] [PubMed]
- Zhao, J.; Zhang, P.; Wang, J.; Xi, Q.; Zhao, X.; Ji, M.; Hu, G. Plasma levels of soluble programmed death ligand-1 may be associated with overall survival in nonsmall cell lung cancer patients receiving thoracic radiotherapy. Medicine 2017, 96, e6102. [Google Scholar] [CrossRef]
- Okuma, Y.; Wakui, H.; Utsumi, H.; Sagawa, Y.; Hosomi, Y.; Kuwano, K.; Homma, S. Soluble Programmed Cell Death Ligand 1 as a Novel Biomarker for Nivolumab Therapy for Non-Small-cell Lung Cancer. Clin. Lung Cancer 2018, 19, 410–417.e1. [Google Scholar] [CrossRef] [PubMed]
- Costantini, A.; Julie, C.; Dumenil, C.; Hélias-Rodzewicz, Z.; Tisserand, J.; Dumoulin, J.; Giraud, V.; Labrune, S.; Chinet, T.; Emile, J.F.; et al. Predictive role of plasmatic biomarkers in advanced non-small cell lung cancer treated by nivolumab. Oncoimmunology 2018, 7, e1452581. [Google Scholar] [CrossRef] [PubMed]
- Bonomi, M.; Ahmed, T.; Addo, S.; Kooshki, M.; Palmieri, D.; Levine, B.J.; Ruiz, J.; Grant, S.; Petty, W.J.; Triozzi, P.L. Circulating immune biomarkers as predictors of the response to pembrolizumab and weekly low dose carboplatin and paclitaxel in NSCLC and poor PS: An interim analysis. Oncol. Lett. 2019, 17, 1349–1356. [Google Scholar] [CrossRef]
- Dronca, R.S.; Liu, X.; Harrington, S.M.; Enninga, E.A.L.; Kottschade, L.A.; Koo, C.W.; McWilliams, R.R.; Block, M.S.; Nevala, W.K.; Markovic, S.; et al. Bim and soluble PD-L1 (sPD-L1) as predictive biomarkers of response to anti-PD-1 therapy in patients with melanoma and lung carcinoma. J. Clin. Oncol. 2017, 35, S11534. [Google Scholar] [CrossRef]
- Wang, Y.; He, H. Prognostic value of soluble programmed cell death ligand-1 in patients with non-small-cell lung cancer: A meta-analysis. Immunotherapy 2022, 14, 945–956. [Google Scholar] [CrossRef]
- Zhu, H.B.; Song, X. Analysis of soluble programmed death-1 ligand-1 of lung cancer patients with different characteristics. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 8690–8696. [Google Scholar]
- Tiako Meyo, M.; Jouinot, A.; Giroux-Leprieur, E.; Fabre, E.; Wislez, M.; Alifano, M.; Leroy, K.; Boudou-Rouquette, P.; Tlemsani, C.; Khoudour, N.; et al. Predictive Value of Soluble PD-1, PD-L1, VEGFA, CD40 Ligand and CD44 for Nivolumab Therapy in Advanced Non-Small Cell Lung Cancer: A Case-Control Study. Cancers 2020, 12, 473. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Bu, Z.; Liu, X.; Zhang, L.; Li, Z.; Wu, A.; Wu, X.; Cheng, X.; Xing, X.; Du, H.; et al. Level of circulating PD-L1 expression in patients with advanced gastric cancer and its clinical implications. Chin. J. Cancer Res. 2014, 26, 104–111. [Google Scholar] [PubMed]
- Vecchiarelli, S.; Passiglia, F.; D’Incecco, A.; Gallo, M.; De Luca, A.; Rossi, E.; D’Incà, F.; Minuti, G.; Landi, L.; Bennati, C.; et al. Circulating programmed death ligand-1 (cPD-L1) in non-small-cell lung cancer (NSCLC). Oncotarget 2018, 9, 17554–17563. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, S.F.; Demuth, C.; Weber, B.; Sorensen, B.S.; Meldgaard, P. Increase in soluble PD-1 is associated with prolonged survival in patients with advanced EGFR-mutated non-small cell lung cancer treated with erlotinib. Lung Cancer 2016, 100, 77–84. [Google Scholar] [CrossRef]
- Khan, M.; Zhao, Z.; Arooj, S.; Fu, Y.; Liao, G. Soluble PD-1: Predictive, Prognostic, and Therapeutic Value for Cancer Immunotherapy. Front. Immunol. 2020, 11, 587460. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Demographic Characteristics |
sPD-L1 ≤ 182.5 ng/L n = 25 |
sPD-L1 ˃ 182.5 ng/L n = 10 | p -Value |
|---|---|---|---|
| Age, mean ± sd | 63.5 | 63.4 | 0.976 |
| Female sex, n (%) | 17 (68%) | 7 (70%) | |
| Male sex, n (%) | 8 (32%) | 3 (30%) | |
| Smoking, n (%) | 0.354 | ||
| Never smokers | 14 (56%) | 5 (50%) | |
| Former smokers | 6 (24%) | 3 (30%) | |
| Current smokers | 5 (20%) | 2 (20%) | |
| EGFR mutation | 0.749 | ||
| Del 19 | 13 (52%) | 7 (70%) | |
| L858R point mutation exon 21 | 9 (36%) | 2 (20%) | |
| Rare mutations | 3 (12%) | 1 (10%) | |
| Del 20 | 1 | ||
| G719X exon 18 | 1 | 1 | |
| G719X exon 18 and S768I exon 20 | 1 |
| Variable |
sPD-L1 ≤ 182.5 ng/L N = 25 |
sPD-L1 ˃ 182.5 ng/L N = 10 |
|---|---|---|
| Complete response | 0/25 | 1/10 (10%) |
| Partial response | 12/25 (48%) | 2/10 (20%) |
| Response | 12/25 (48%) | 3/10 (30%) |
| Stable disease | 13/25 (52%) | 7/10 (70%) |
| Disease control | 25/25 (100%) | 10/10 (100%) |
| Study | Patient Population | sPD-L1 Cut-Off Value | Findings |
|---|---|---|---|
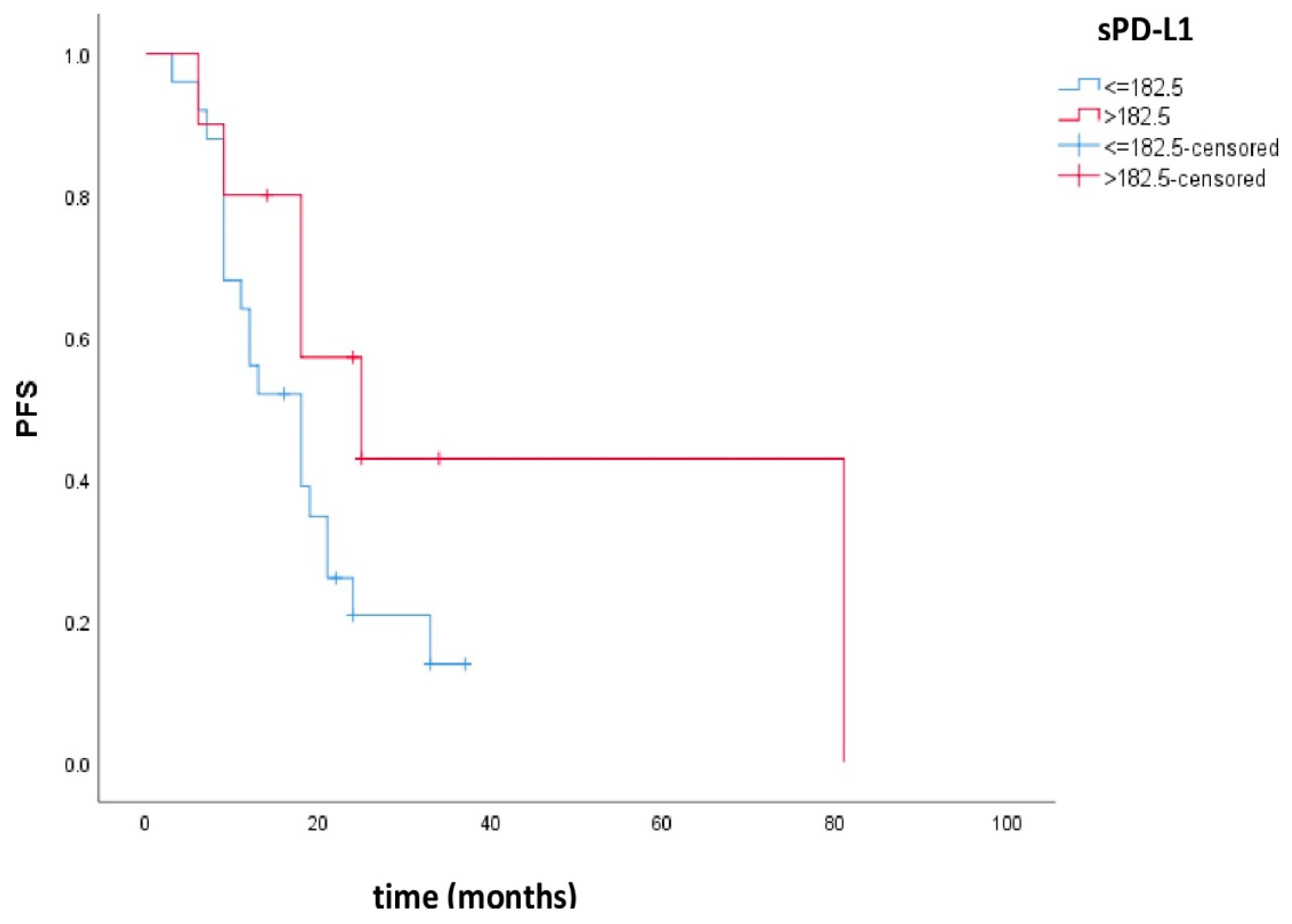
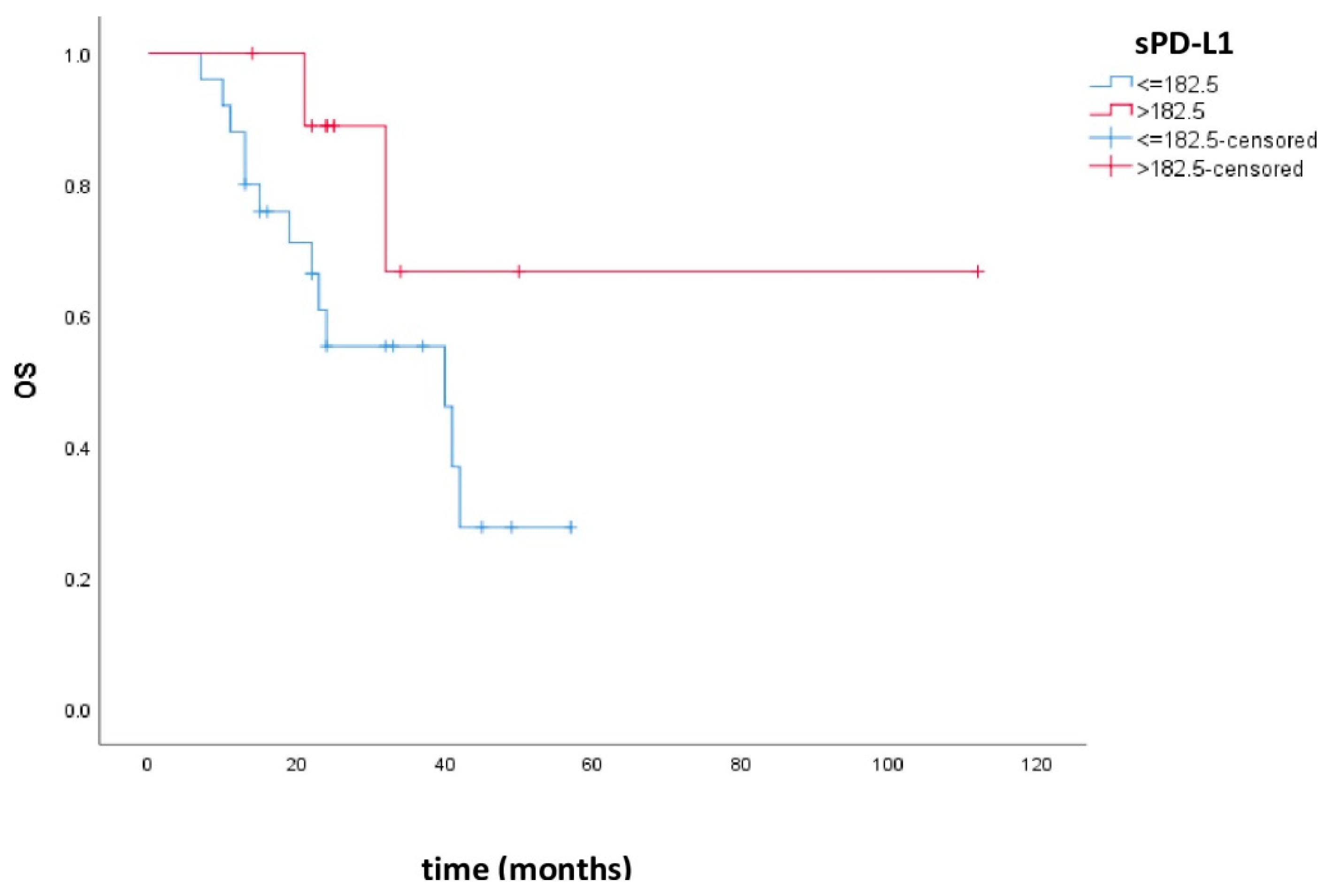
| Ceriman Krstic et al. | EGFRmut NSCLC patients who achieved disease control | 182.5 ng/L | Pts with higher levels had better outcomes, but there was no statistical significance. |
| Jin et al. [22] | SCLC | 7.0 ng/mL | Pts with higher levels had no response to CT. |
| Okuma et al. [2] | Advanced lung cancer | 7.32 ng/mL | Pts with high levels had worse prognoses. |
| Jia et al. [1] | EGFRmut lung adenocarcinoma | 568.19 pg/mL | Pts with high baseline sPD-L1 levels and patients with high on-treatment sPD-L1 levels had shortened PFS, but there was no statistical significance. |
| Zhang et al. [17] | NSCLC, healthy controls | 0.636 ng/mL | Pts with high levels had worse prognoses; the same results were observed for the EGFRmut group, but there was no statistical significance. |
| Zhao et al. [25] | Advanced NSCLC | 0.0965 ng/mL | Lower levels of baseline sPD-L1 correlated with longer OS; sPD-L1 levels were significantly lower at week 2 and week 4 compared to baseline, but afterward, RT levels were similar to baseline. |
| Okuma et al. [26] | NSCLC | 3.357 ng/mL | Pts with high levels had worse prognoses. |
| Costantini et al. [27] | Advanced NSCLC (EGFRwt, ALK negat) | 0.0337 ng/mL | Pts with high levels had worse prognoses. |
| Tiako Meyo et al. [32] | EGFRwt vs. EGFRmut | 0.156 ng/mL | Positive levels of sPD-L1 in pts treated with nivolumab correlated with shorter PFS. Such correlation was not found in the EGFRmut group of patients. After two cycles of nivolumab, pts with increased or stable levels of sPD-1 had longer PFS and OS. |
| Zheng et al. [33] | Advanced gastric cancer | 0.5993 ng/mL | Pts with higher levels of sPD-L1 had better prognoses. |
| Vecchiarelli et al. [34] | Advanced NSCLC, healthy controls | 37.81 pg/mL | Pts treated with CT had significant increases in median sPD-L1 after 3 months of treatment. Pts treated with TKIs and immunotherapy did not have significant changes in their median sPD-L1 levels. No significant differences in ORR, PFS, and OS were found between patients with high and low sPD-L1 levels. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ćeriman Krstić, V.; Jovanović, D.; Samardžić, N.; Gajić, M.; Kotur Stevuljević, J.; Klisic, A.; Soldatović, I.; Radončić, D.; Roksandić Milenković, M.; Šeha, B.; et al. The Potential Role of sPD-L1 as a Predictive Biomarker in EGFR-Positive Non-Small-Cell Lung Cancer. Curr. Issues Mol. Biol. 2025, 47, 45. https://doi.org/10.3390/cimb47010045
Ćeriman Krstić V, Jovanović D, Samardžić N, Gajić M, Kotur Stevuljević J, Klisic A, Soldatović I, Radončić D, Roksandić Milenković M, Šeha B, et al. The Potential Role of sPD-L1 as a Predictive Biomarker in EGFR-Positive Non-Small-Cell Lung Cancer. Current Issues in Molecular Biology. 2025; 47(1):45. https://doi.org/10.3390/cimb47010045
Chicago/Turabian StyleĆeriman Krstić, Vesna, Dragana Jovanović, Natalija Samardžić, Milija Gajić, Jelena Kotur Stevuljević, Aleksandra Klisic, Ivan Soldatović, Damir Radončić, Marina Roksandić Milenković, Biljana Šeha, and et al. 2025. "The Potential Role of sPD-L1 as a Predictive Biomarker in EGFR-Positive Non-Small-Cell Lung Cancer" Current Issues in Molecular Biology 47, no. 1: 45. https://doi.org/10.3390/cimb47010045
APA StyleĆeriman Krstić, V., Jovanović, D., Samardžić, N., Gajić, M., Kotur Stevuljević, J., Klisic, A., Soldatović, I., Radončić, D., Roksandić Milenković, M., Šeha, B., Čolić, N., Lukić, K., & Savić, M. (2025). The Potential Role of sPD-L1 as a Predictive Biomarker in EGFR-Positive Non-Small-Cell Lung Cancer. Current Issues in Molecular Biology, 47(1), 45. https://doi.org/10.3390/cimb47010045