
Anatomy, Biomechanics, and Loads of the Wrist Joint



 ,
, 
Abstract
:1. Introduction
2. Anatomy of the Wrist Joint
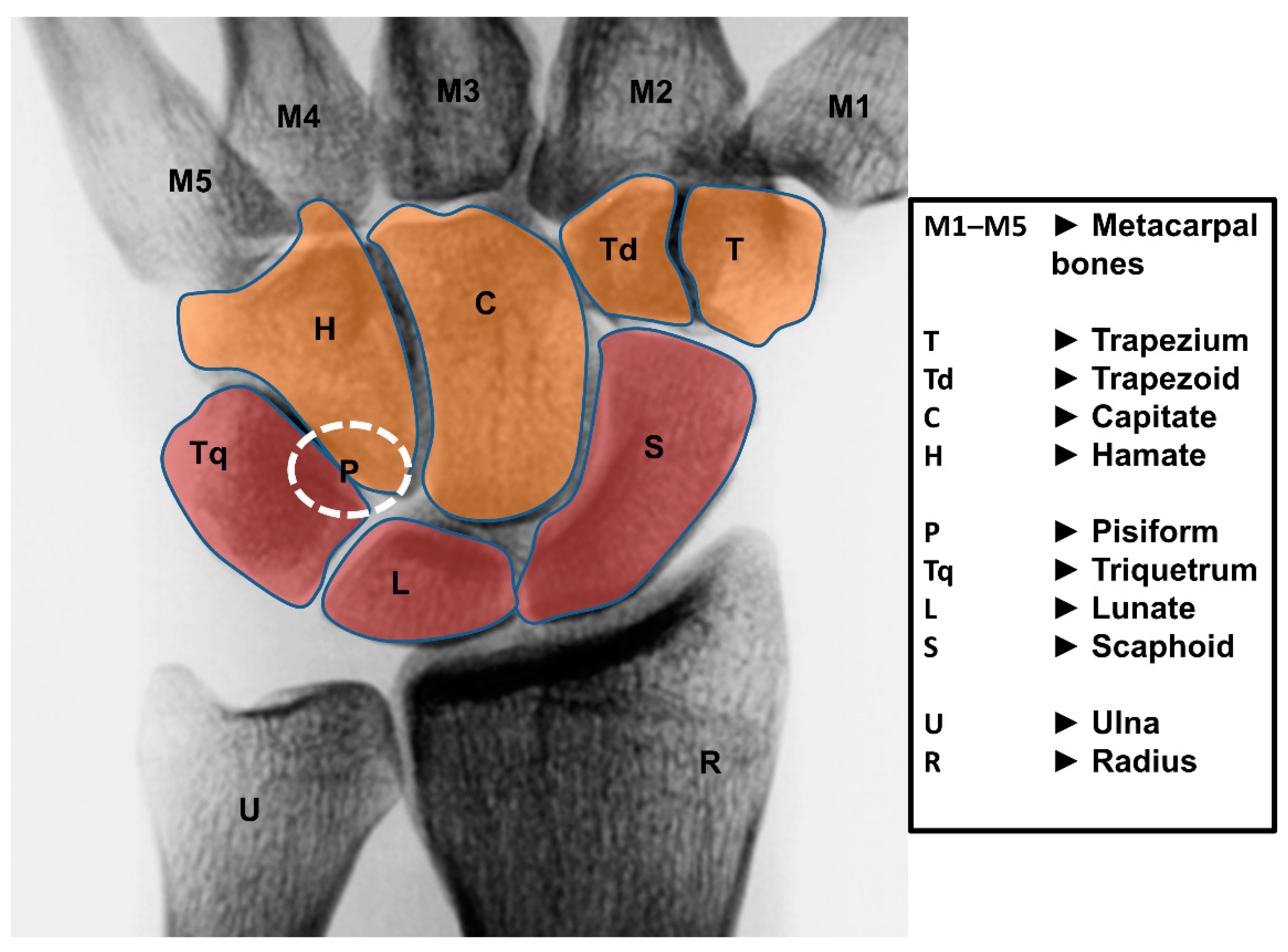
2.1. Bones
2.2. Ligaments
2.2.1. General
2.2.2. Extrinsic Carpal Ligaments
2.2.3. Intrinsic Carpal Ligaments
2.3. Muscles
3. Wrist Motion
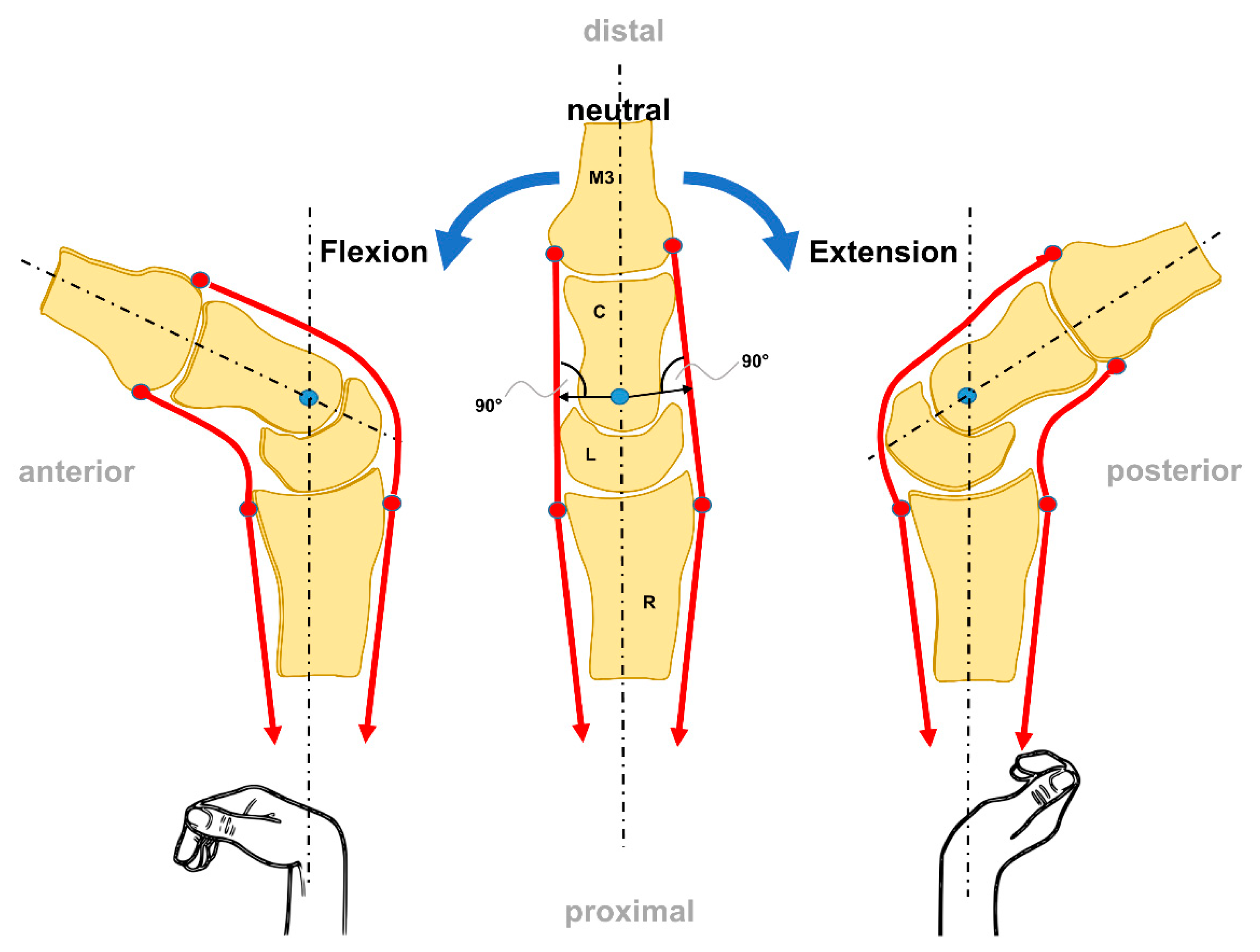
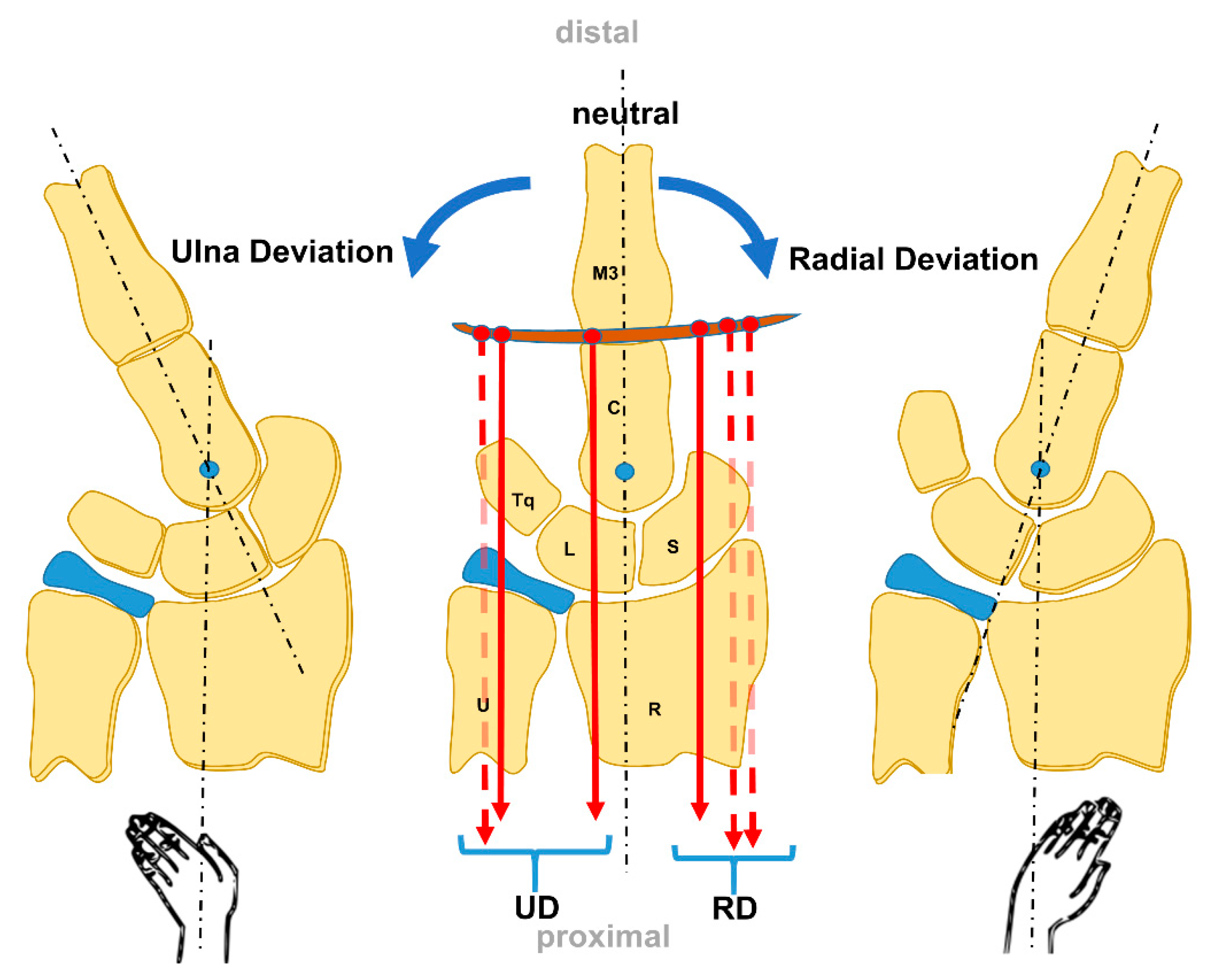
3.1. Overall Motion
3.2. Specific Wrist Bone Motion
4. Biomechanics of the Wrist Joint
4.1. Models and Theories of the Wrist Joint Biomechanics
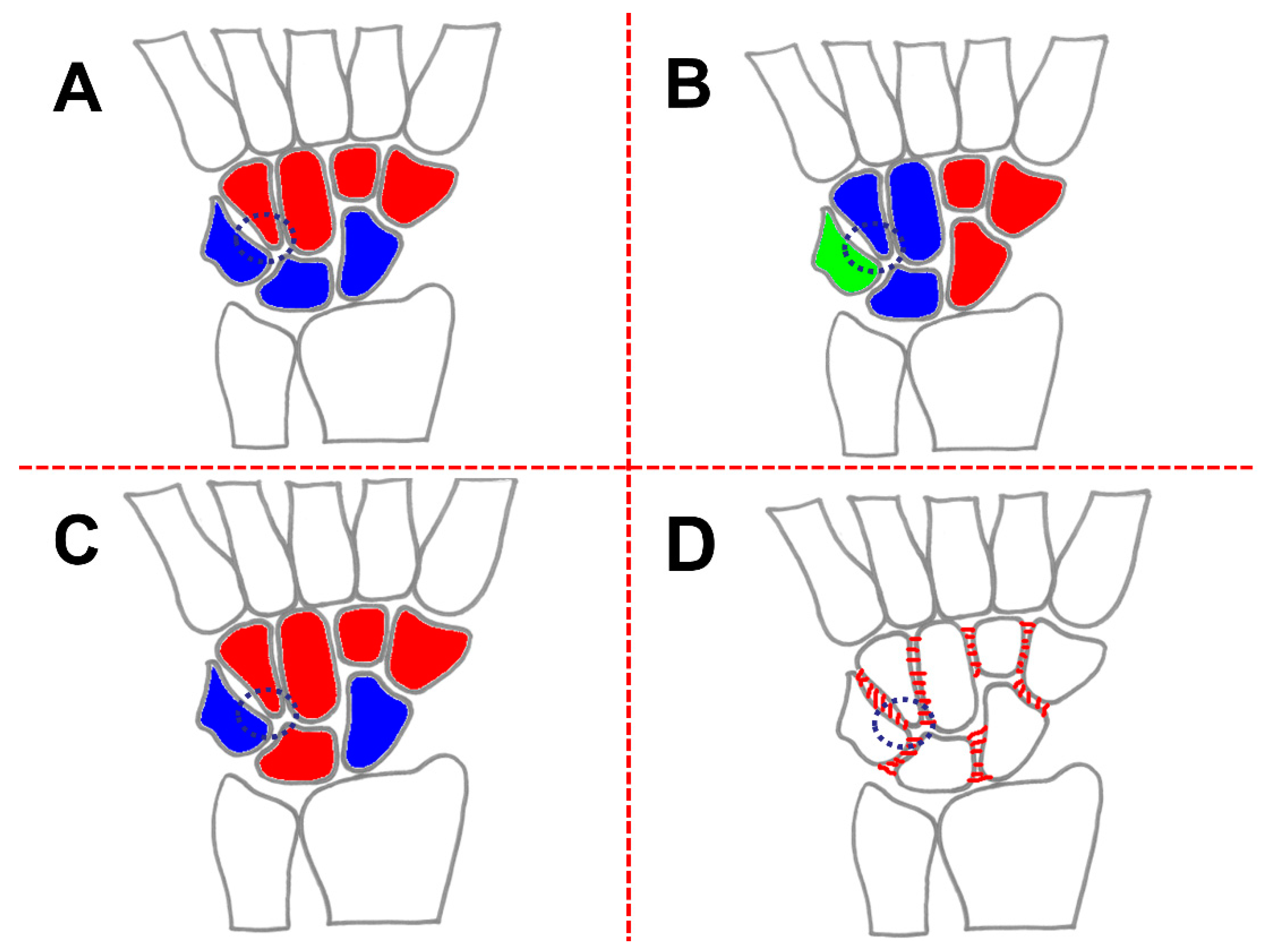
4.1.1. Row-Theory
4.1.2. Column-Theory
4.1.3. Row-Column-Theory
4.1.4. Ring-Model
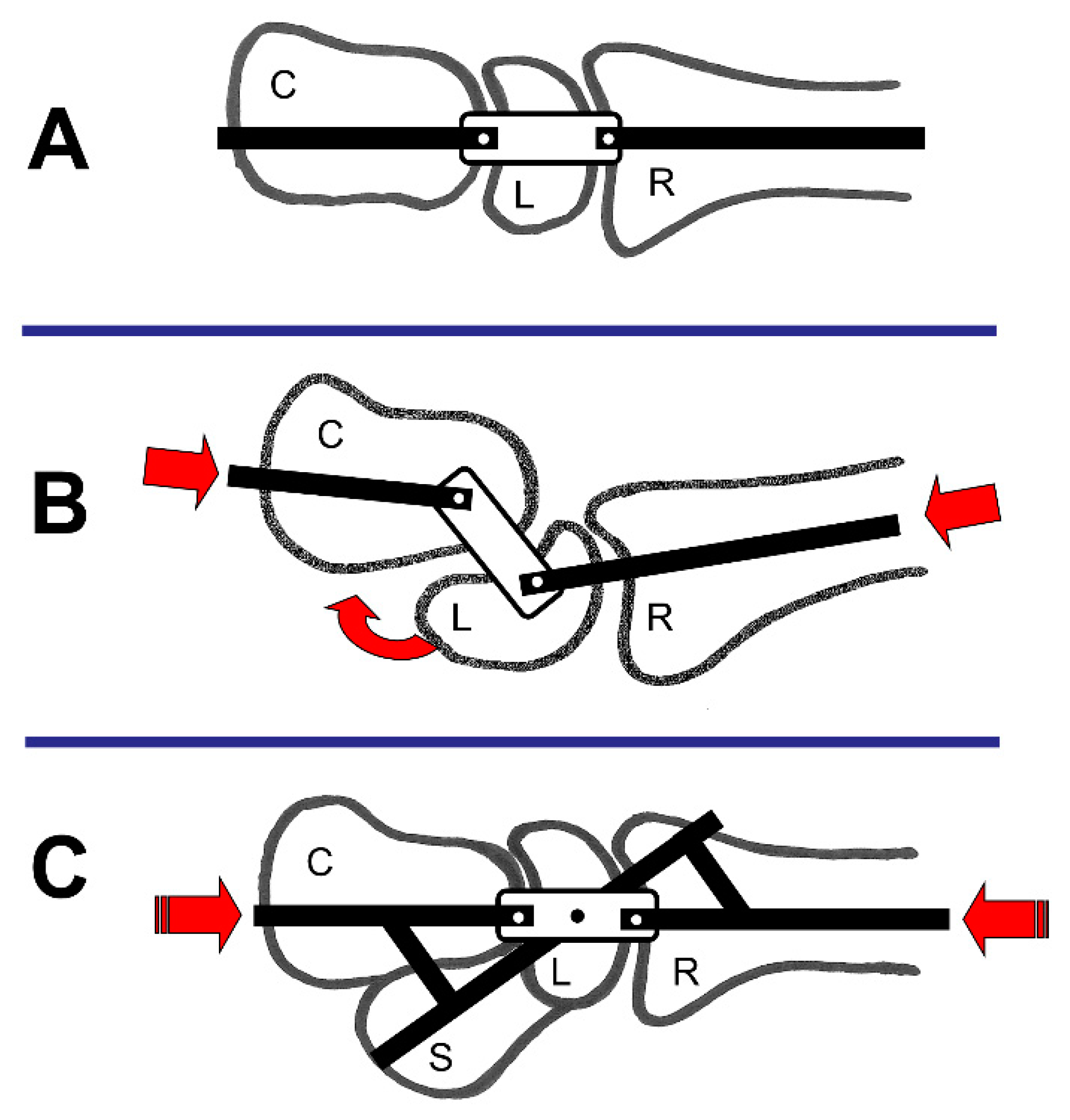
4.1.5. Link Joint-Theory
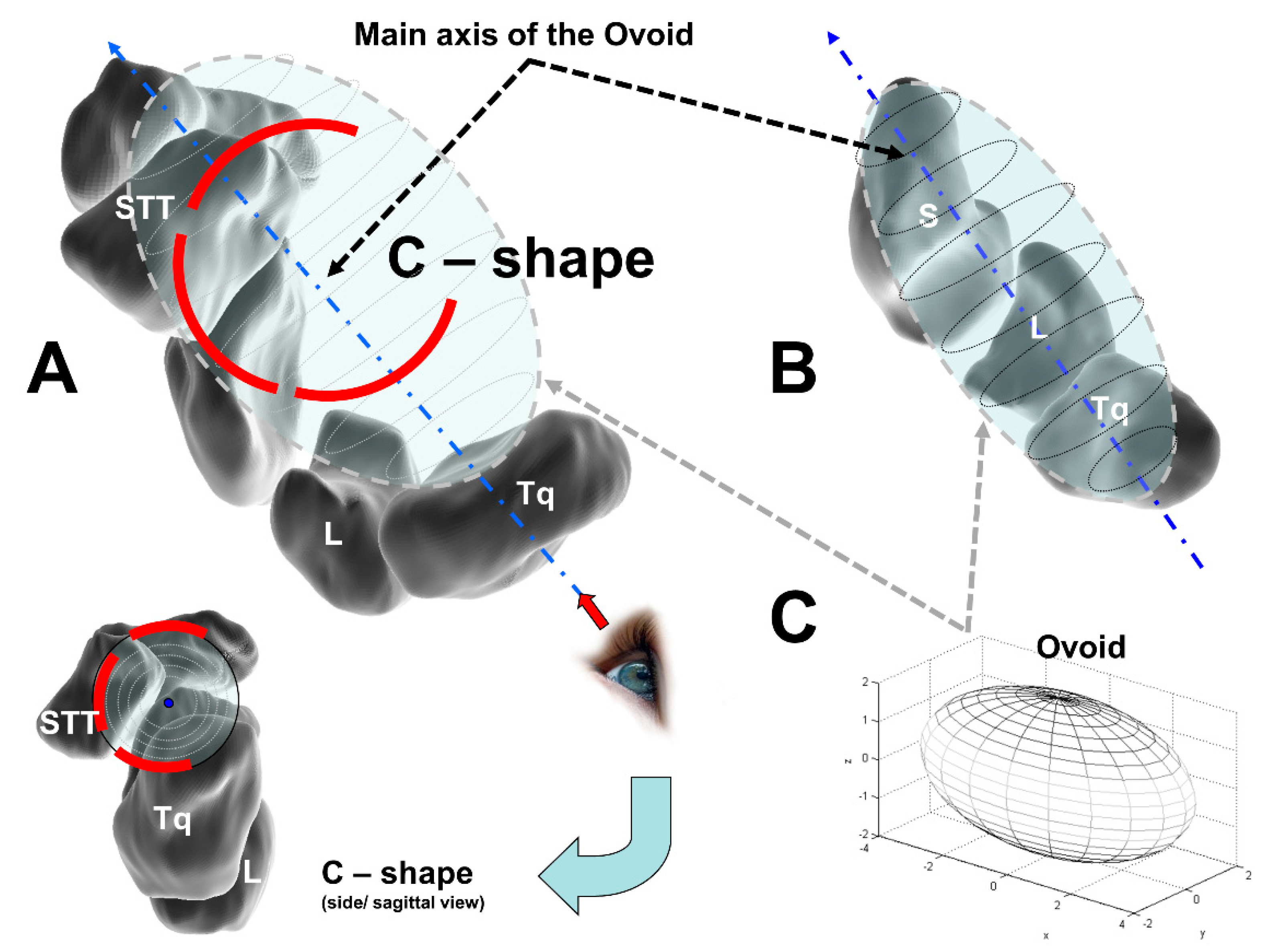
4.1.6. Ovoid-/C-Shape-Theory
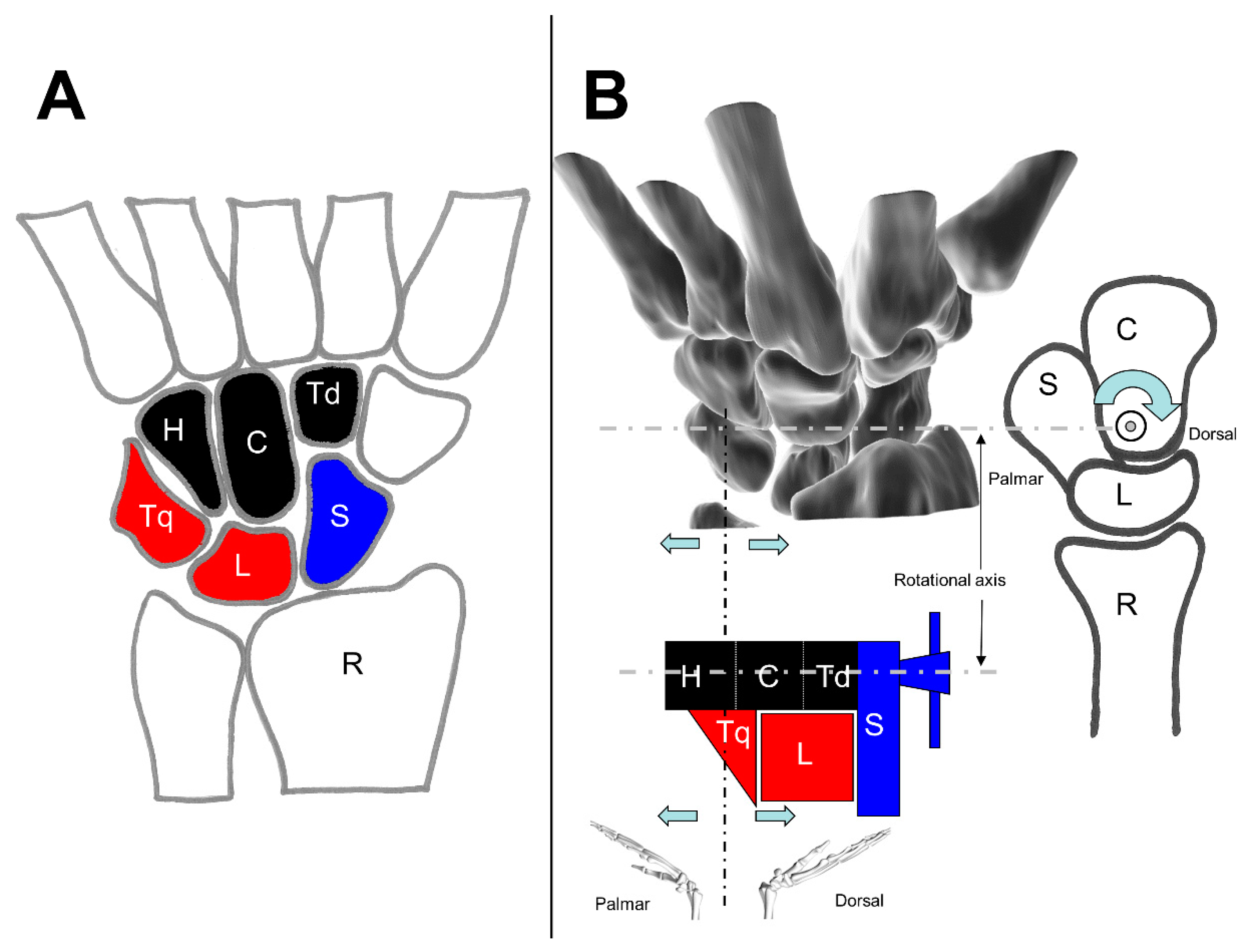
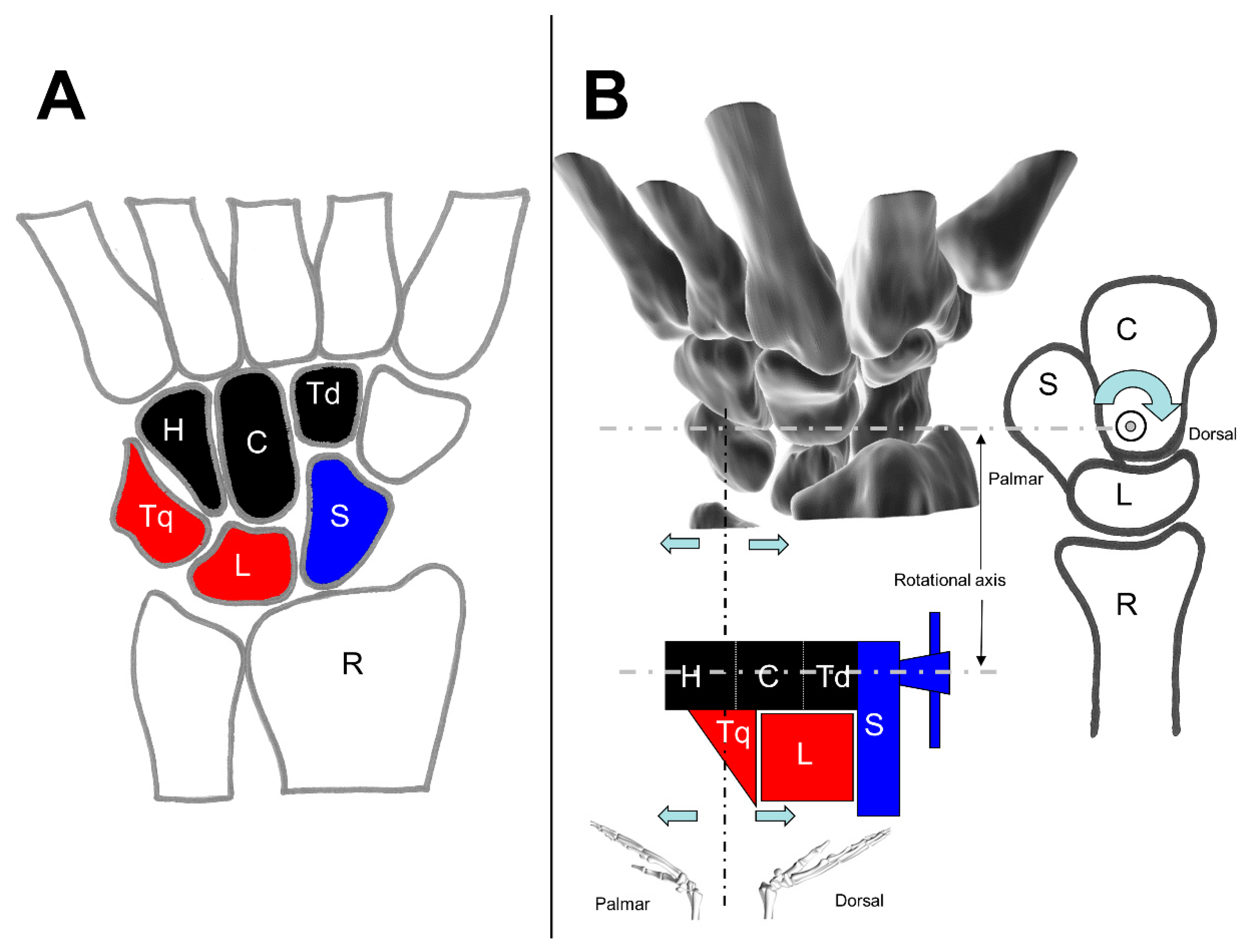
4.1.7. Screw Vice or Clamp-Theory
4.2. Loads of the Wrist Joint
5. Conclusions and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bajuri, M.; Abdul Kadir, M.R.; Amin, I.M.; Ochsner, A. Biomechanical analysis of rheumatoid arthritis of the wrist joint. Proc. Inst. Mech. Eng. Part H 2012, 226, 510–520. [Google Scholar] [CrossRef] [PubMed]
- Berger, R.A. The Anatomy and Basic Biomechanics of the Wrist joint. J. Hand Ther. 1996, 9, 84–93. [Google Scholar] [CrossRef]
- Kaufmann, R.A.; Pfaeffle, H.J.; Blankenhorn, B.D.; Stabile, K.; Robertson, D.; Goitz, R. Kinematics of the midcarpal and radiocarpal joint in flexion and extension: An in vitro study. J. Hand Surg. 2006, 31, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Kijima, Y.; Viegas, S.F. Wrist anatomy and biomechanics. J. Hand Surg. 2009, 34, 1555–1563. [Google Scholar] [CrossRef]
- Majors, B.J.; Wayne, J.S. Development and validation of a computational model for investigation of wrist biomechanics. Ann. Biomed. Eng. 2011, 39, 2807. [Google Scholar] [CrossRef]
- Rainbow, M.J.; Wolff, A.L.; Crisco, J.J.; Wolfe, S.W. Functional kinematics of the wrist. J. Hand Surg. 2016, 41, 7–21. [Google Scholar] [CrossRef]
- Eschweiler, J.; Stromps, J.-P.; Fischer, M.; Schick, F.; Rath, B.; Pallua, N.; Radermacher, K. A biomechanical model of the wrist joint for patient-specific model guided surgical therapy: Part 2. Proc. Inst. Mech. Eng. Part H 2016, 230, 326–334. [Google Scholar] [CrossRef]
- Eschweiler, J.; Stromps, J.-P.; Fischer, M.; Schick, F.; Rath, B.; Pallua, N.; Radermacher, K. Development of a biomechanical model of the wrist joint for patient-specific model guided surgical therapy planning: Part 1. Proc. Inst. Mech. Eng. Part H 2016, 230, 310–325. [Google Scholar] [CrossRef]
- Kuo, C.E.; Wolfe, S.W. Scapholunate instability: Current concepts in diagnosis and management. J. Hand Surg. 2008, 33, 998–1013. [Google Scholar] [CrossRef]
- Gelberman, R.H.; Cooney, W.P., 3rd; Szabo, R.M. Carpal instability. Instr. Course Lect. 2001, 50, 123–135. [Google Scholar] [CrossRef]
- Schmidt, H.-M.; Lanz, U. Chirurgische Anatomie der Hand, 2nd ed.; Thieme: Stuttgart, Germany, 2003; ISBN 3131306920. [Google Scholar]
- Sennwald, G. Das Handgelenk; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- An, K.-N.; Berger, R.A.; Cooney, W.P. (Eds.) Biomechanics of the Wrist Joint; Springer: New York, NY, USA, 1991; ISBN 9781461278337. [Google Scholar]
- Laulan, J.; Marteau, E.; Bacle, G. Wrist osteoarthritis. Orthop. Traumatol. 2015, 101, S1–S9. [Google Scholar] [CrossRef] [Green Version]
- Kamal, R.N.; Starr, A.; Akelman, E. Carpal Kinematics and Kinetics. J. Hand Surg. 2016, 41, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- Ayhan, Ç.; Ayhan, E. Kinesiology of the Wrist and the Hand. In Comparative Kinesiology of the Human Body; Elsevier: Amsterdam, The Netherlands, 2020; pp. 211–282. [Google Scholar]
- Feipel, V.; Rooze, M. The capsular ligaments of the wrist: Morphology, morphometry and clinical applications. Surg. Radiol. Anat. 1999, 21, 175–180. [Google Scholar] [CrossRef]
- Crisco, J.J.; Coburn, J.C.; Moore, D.C.; Upal, M.A. Carpal bone size and scaling in men versus in women. J. Hand Surg. 2005, 30, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Kapandji, A. Biomechanik des Carpus und des Handgelenkes. Orthopade 1986, 15, 60–73. [Google Scholar] [PubMed]
- Mayfield, J.K.; Johnson, R.P.; Kilcoyne, R.F. The ligaments of the human wrist and their functional significance. Anat. Rec. 1976, 186, 417–428. [Google Scholar] [CrossRef]
- Sennwald, G. Das Handgelenk; Springer: Berlin/Heidelberg, Germany; New York, NY, USA; London, UK; Paris, France; Tokyo, Japan, 1987; ISBN 0387180257. [Google Scholar]
- Taleisnik, J. The ligaments of the wrist. J. Hand Surg. 1976, 1, 110–118. [Google Scholar] [CrossRef]
- Taleisnik, J. The Wrist; Churchill Livingstone: New York, NY, USA, 1985; ISBN 9780443081347. [Google Scholar]
- Taleisnik, J. Current concepts review. Carpal instability. J. Bone Jt. Surg. Am. 1988, 70, 1262–1268. [Google Scholar] [CrossRef] [Green Version]
- Pulos, N.; Bozentka, D.J. Carpal Ligament Anatomy and Biomechanics. Hand Clin. 2015, 31, 381–387. [Google Scholar] [CrossRef]
- Rainbow, M.J.; Kamal, R.N.; Leventhal, E.; Akelman, E.; Moore, D.C.; Wolfe, S.W.; Crisco, J.J. In Vivo Kinematics of the Scaphoid, Lunate, Capitate, and Third Metacarpal in Extreme Wrist Flexion and Extension. J. Hand Surg. 2013, 38, 278–288. [Google Scholar] [CrossRef] [Green Version]
- Berger, R.A. The anatomy of the ligaments of the wrist and distal radioulnar joints. Clin. Orthop. Relat. Res. 2001, 383, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Schuind, F.; An, K.N.; Cooney, W.P., III; Garcia-Elias, M. (Eds.) Advances in the Biomechanics of the Hand and Wrist; Springer: New York, NY, USA, 1994; ISBN 9781475791099. [Google Scholar]
- Towfigh, H.; Hierner, R.; Langer, M.; Friedel, R. Handchirurgie; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Moritomo, H.; Murase, T.; Goto, A.; Oka, K.; Sugamoto, K.; Yoshikawa, H. In vivo three-dimensional kinematics of the midcarpal joint of the wrist. J. Bone Jt. Surg. Am. 2006, 88, 611–621. [Google Scholar] [CrossRef]
- Moore, D.C.; Crisco, J.J.; Trafton, T.G.; Leventhal, E.L. A digital database of wrist bone anatomy and carpal kinematics. J. Biomech. 2007, 40, 2537–2542. [Google Scholar] [CrossRef]
- Bawa, P.; Chalmers, G.R.; Jones, K.E.; Søgaard, K.; Walsh, M.L. Control of the wrist joint in humans. Eur. J. Appl. Physiol. 2000, 83, 116–127. [Google Scholar] [CrossRef]
- Shah, D.S.; Middleton, C.; Gurdezi, S.; Horwitz, M.D.; Kedgley, A.E. The importance of abductor pollicis longus in wrist motions: A physiological wrist simulator study. J. Biomech. 2018, 77, 218–222. [Google Scholar] [CrossRef]
- Moore, J.A.; Small, C.F.; Bryant, J.T.; Ellis, R.E.; Pichora, D.R.; Hollister, A.M. A kinematic technique for describing wrist joint motion: Analysis of configuration space plots. Proc. Inst. Mech. Eng. Part H 1993, 207, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, P.J.; Neumann, D.A. Essentials of Kinesiology for the Physical Therapist Assistant e-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Akhbari, B.; Morton, A.M.; Shah, K.N.; Molino, J.; Moore, D.C.; Weiss, A.-P.C.; Wolfe, S.W.; Crisco, J.J. Proximal-distal shift of the center of rotation in a total wrist arthroplasty is more than twice of the healthy wrist. J. Orthop. Res. 2020, 38, 1575–1586. [Google Scholar] [CrossRef]
- Kaufmann, R.; Pfaeffle, J.; Blankenhorn, B.; Stabile, K.; Robertson, D.; Goitz, R. Kinematics of the midcarpal and radiocarpal joints in radioulnar deviation: An in vitro study. J. Hand Surg. 2005, 30, 937–942. [Google Scholar] [CrossRef]
- Neu, C.P.; Crisco, J.J.; Wolfe, S.W. In vivo kinematic behavior of the radio-capitate joint during wrist flexion-extension and radio-ulnar deviation. J. Biomech. 2001, 34, 1429–1438. [Google Scholar] [CrossRef]
- Crisco, J.J. The Mechanical Axes of the Wrist Are Oriented Obliquely to the Anatomical Axes. J. Bone Jt. Surg. Am. 2011, 93, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Youm, Y.; McMurthy, R.Y.; Flatt, A.E.; Gillespie, T.E. Kinematics of the wrist. I. An experimental study of radial-ulnar deviation and flexion-extension. J. Bone Jt. Surg. Am. Vol. 1978, 60, 423–431. [Google Scholar] [CrossRef]
- Ruby, L.K.; Cooney, W.P.; An, K.N.; Linscheid, R.L.; Chao, E.Y. Relative motion of selected carpal bones: A kinematic analysis of the normal wrist. J. Hand Surg. 1988, 13, 1–10. [Google Scholar] [CrossRef]
- Garcia-Elias, M. Understanding Wrist Mechanics: A Long and Winding Road. J. Wrist Surg. 2013, 2, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Berger, R.A.; Crowninshield, R.D.; Flatt, A.E. The three-dimensional rotational behaviors of the carpal bones. Clin. Orthop. Relat. Res. 1982, 303–310. [Google Scholar] [CrossRef]
- Linscheid, R.L. Kinematic considerations of the wrist. Clin. Orthop. Relat. Res. 1986, 202, 27–39. [Google Scholar] [CrossRef]
- Patterson, R.M.; Williams, L.; Andersen, C.R.; Koh, S.; Viegas, S.F. Carpal kinematics during simulated active and passive motion of the wrist. J. Hand Surg. 2007, 32, 1013–1019. [Google Scholar] [CrossRef]
- Moojen, T.M.; Snel, J.G.; Ritt, M.J.P.F.; Venema, H.W.; Kauer, J.M.G.; Bos, K.E. In vivo analysis of carpal kinematics and comparative review of the literature. J. Hand Surg. 2003, 28, 81–87. [Google Scholar] [CrossRef]
- Moojen, T.M.; Snel, J.G.; Ritt, M.J.P.F.; Venema, H.W.; Kauer, J.M.G.; Bos, K.E. Scaphoid kinematics in vivo. J. Hand Surg. 2002, 27, 1003–1010. [Google Scholar] [CrossRef]
- Moojen, T.M.; Snel, J.G.; Ritt, M.J.P.F.; Kauer, J.M.G.; Venema, H.W.; Bos, K.E. Three-dimensional carpal kinematics in vivo. Clin. Biomech. 2002, 17, 506–514. [Google Scholar] [CrossRef]
- Rohde, R.S.; Crisco, J.J.; Wolfe, S.W. The advantage of throwing the first stone: How understanding the evolutionary demands of Homo sapiens is helping us understand carpal motion. J. Am. Acad. Orthop. Surg. 2010, 18, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Eschweiler, J.; Allmendinger, F.; Stromps, J.P.; Nick, H.E.; Pallua, N.; Radermacher, K. Biomechanische Modellierung der Handwurzel. Z. Orthopädie Unf. 2014, 152, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Navarro, A. Luxaciones del carpo. An. Fac. Med. 1921, 6, 113–141. [Google Scholar]
- Lichtman, D.M.; Schneider, J.R.; Swafford, A.R.; Mack, G.R. Ulnar midcarpal instability-clinical and laboratory analysis. J. Hand Surg. 1981, 6, 515–523. [Google Scholar] [CrossRef]
- Gilford, W.; Bolton, R.; Lambrinudi, C. The mechanism of the wrist joint with special reference to fractures of the scaphoid. Guy’s Hosp. Rep. 1943, 92, 52–59. [Google Scholar]
- Macconaill, M.A. The mechanical anatomy of the carpus and its bearings on some surgical problems. J. Anat. 1941, 75, 166–175. [Google Scholar]
- Bryce, T.H. Certain points in the anatomy and mechanism of the wrist-joint reviewed in the light of a series of Röntgen ray photographs of the living hand. J. Anat. Physiol. 1896, 31, 59–79. [Google Scholar]
- Destot, É. The Classic: Injuries of the Wrist: A Radiological Study. Clin. Orthop. Relat. Res. 2006, 445, 8–14. [Google Scholar] [CrossRef]
- Moritomo, H.; Murase, T.; Goto, A.; Oka, K.; Sugamoto, K.; Yoshikawa, H. Capitate-based kinematics of the midcarpal joint during wrist radioulnar deviation: An in vivo three-dimensional motion analysis. J. Hand Surg. 2004, 29, 668–675. [Google Scholar] [CrossRef]
- Genda, E.; Horii, E. Theoretical stress analysis in wrist joint--neutral position and functional position. J. Hand Surg. 2000, 25, 292–295. [Google Scholar] [CrossRef]
- Schuind, F.; Cooney, W.P.; Linscheid, R.L.; An, K.N.; Chao, E.Y. Force and pressure transmission through the normal wrist. A theoretical two-dimensional study in the posteroanterior plane. J. Biomech. 1995, 28, 587–601. [Google Scholar] [CrossRef]
- Tencer, A.F.; Viegas, S.F.; Cantrell, J.; Chang, M.; Clegg, P.; Hicks, C.; O´Meara, C.; Williamson, J.B. Pressure distribution in the wrist joint. J. Orthop. Res. 1988, 6, 509–517. [Google Scholar] [CrossRef]
- Horii, E.; Garcia-Elias, M.; Bishop, A.T.; Cooney, W.P.; Linscheid, R.L.; Chao, E.Y. Effect on force transmission across the carpus in procedures used to treat Kienböck’s disease. J. Hand Surg. 1990, 15, 393–400. [Google Scholar] [CrossRef]
- Iwasaki, N.; Genda, E.; Minami, A.; Kaneda, K.; Chao, E.Y. Force transmission through the wrist joint in Kienböck’s disease: A two-dimensional theoretical study. J. Hand Surg. 1998, 23, 415–424. [Google Scholar] [CrossRef]
- Jakubowitz, E.; Kaszap, B.; Zhang, H.; Mack, M.; Kiggen, K.; Jahnke, A.; Daecke, W. Kontaktkräfte im Radiokarpalgelenk in Abhängigkeit zur Handgelenksstellung; Deutsche Gesellschaft für Biomechaik: Ulm, Deutschland, 2013. [Google Scholar]
- Manal, K.; Lu, X.; Nieuwenhuis, M.K.; Helders, P.J.M.; Buchanan, T.S. Force transmission through the juvenile idiopathic arthritic wrist: A novel approach using a sliding rigid body spring model. J. Biomech. 2002, 35, 125–133. [Google Scholar] [CrossRef]
- Meier, R.; Busche, M.; Krettek, C.; Probst, C.; Schmitt, R.; Krimmer, H. Die Kraftübertragung am Handgelenk nach Skaphoid-, Trapezium- und Trapezoideumfusion. Unfallchirurg 2005, 108, 456–460. [Google Scholar] [CrossRef]
- Werner, F.W.; Palmer, A.K.; Fortino, M.D.; Short, W.H. Force transmission through the distal ulna: Effect of ulnar variance, lunate fossa angulation, and radial and palmar tilt of the distal radius. J. Hand Surg. 1992, 17, 423–428. [Google Scholar] [CrossRef]
- Tang, P.; Gauvin, J.; Muriuki, M.; Pfaeffle, J.H.; Imbriglia, J.E.; Goitz, R.J. Comparison of the “Contact Biomechanics” of the Intact and Proximal Row Carpectomy Wrist. J. Hand Surg. 2009, 34, 660–670. [Google Scholar] [CrossRef]
- Tang, P.; Wei, D.H.; Ueba, H.; Gardner, T.R.; Rosenwasser, M.P. Scaphoid Excision and 4-Bone Arthrodesis Versus Proximal Row Carpectomy: A Comparison of Contact Biomechanics. J. Hand Surg. 2012, 37, 1861–1867. [Google Scholar] [CrossRef]
- Lewis, O.J.; Hamshere, R.J.; Bucknill, T.M. The anatomy of the wrist joint. J. Anat. 1970, 106, 539–552. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Position | Ligament | Description and Characteristics |
|---|---|---|
| Volar radiocarpal ligaments | radial collateral ligament | |
| radioscaphocapitate ligament |
| |
| long radiolunate ligament |
| |
| radioscapho-lunate ligament |
| |
| short radiolunate ligament |
| |
| Volar ulnocarpal ligaments | ulnotriquetral ligament | |
| ulnolunate ligament | ||
| ulnocapitate ligament | ||
| Dorsal ligaments | radiotriquetral ligament |
|
| dorsal intercarpal (DIC) ligament | ||
| radiolunate ligament | ||
| radioscaphoid ligament |
| Position | Ligament | Description and Characteristics | |
|---|---|---|---|
| Proximal row | Scapholunate interosseous ligament | dorsal portion |
|
| volar portion |
| ||
| proximal portion | |||
| Lunotriquetral interosseous ligament | dorsal portion | ||
| volar portion |
| ||
| proximal portion | |||
| Distal row | trapeziotrapezoid ligament | ||
| trapeziocapitate ligament | |||
| capitohamate ligament | |||
| Palmar midcarpal | scaphotrapeziotrapezoid ligament | ||
| scaphocapitate ligament | |||
| triquetralcapitate ligament | |||
| triquetralhamate ligament | |||
| No. | Muscle | Origin | Insertion | Function on the Wrist | |
|---|---|---|---|---|---|
| 1 | Flexor carpi radialis | (FCR) | Epicondylus medialis humeri | Os metacarpale II | Flexion, Radial Deviation |
| 2 | Palmaris longus | (PL) | Epicondylus medialis humeri | Ligamentum carpi transversum (Retinaculum flexorum), palmar aponeurosis | Flexion |
| 3 | Flexor carpi ulnaris | (FCU) | Epicondylus medialis humeri, Olecranon | Os hamatum (sesamoid: Os pisiforme) | Flexion, Ulnar Deviation |
| 4 | Extensor carpi ulnaris | (ECU) | Epicondylus lateralis humeri | Os metacarpale V | Extension, Ulnar Deviation |
| 5 | Extensor carpi radialis brevis | (ECRB) | Epicondylus lateralis humeri | Os metacarpale III | Extension, Radial Deviation |
| 6 | Extensor carpi radialis longus | (ECRL) | Crista supracondylaris lateralis | Os metacarpale II | Extension, Radial Deviation |
| Model/Theory | Description | Author | Year | Development Basis |
|---|---|---|---|---|
| Row-theory | 2 horizontal rows | Bryce/Destot [55,56] | 1896 | Anatomical investigations |
| Column-theory | 3 vertical columns | Navarro [51] | 1921 | - |
| Screw vice or clamp theory | Mechanical behavior of the wrist | MacConaill [54] | 1941 | Cadaver and X-ray investigations |
| Link joint theory | Technical description of the wrist as a linkage system | Gilford [53] | 1943 | Cadaver and X-ray investigations |
| Row-Column-theory | Central T-structure in combination with 2 columns | Taleisnik [22] | 1976 | 17 cadaver investigations |
| Ring-model | The ring structure of the bones including the intrinsic ligamentous apparatus | Lichtman et al. [52] | 1981 | 23 cadaver investigations in combination with 10 clinical examinations |
| Ovoid/C-shape theory | Midcarpal joints are contained within a midcarpal ovoid, on an axial radiograph of the ovoid, the midcarpal joint displays a C-shaped outline | Moritomo et al. [30,57] | 2006 | MRI of 24 volunteers |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eschweiler, J.; Li, J.; Quack, V.; Rath, B.; Baroncini, A.; Hildebrand, F.; Migliorini, F. Anatomy, Biomechanics, and Loads of the Wrist Joint. Life 2022, 12, 188. https://doi.org/10.3390/life12020188
Eschweiler J, Li J, Quack V, Rath B, Baroncini A, Hildebrand F, Migliorini F. Anatomy, Biomechanics, and Loads of the Wrist Joint. Life. 2022; 12(2):188. https://doi.org/10.3390/life12020188
Chicago/Turabian StyleEschweiler, Jörg, Jianzhang Li, Valentin Quack, Björn Rath, Alice Baroncini, Frank Hildebrand, and Filippo Migliorini. 2022. "Anatomy, Biomechanics, and Loads of the Wrist Joint" Life 12, no. 2: 188. https://doi.org/10.3390/life12020188
APA StyleEschweiler, J., Li, J., Quack, V., Rath, B., Baroncini, A., Hildebrand, F., & Migliorini, F. (2022). Anatomy, Biomechanics, and Loads of the Wrist Joint. Life, 12(2), 188. https://doi.org/10.3390/life12020188