Drinking Water Intake Is Associated with Higher Diet Quality among French Adults

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Demographic, Socio-Economic and Behavioural Variables
2.3. Dietary Assessment
2.4. Foods and Fluids Categorization
2.5. Nutritional Quality of Diet
2.6. Diet Cost
2.7. Statistical Analysis
3. Results
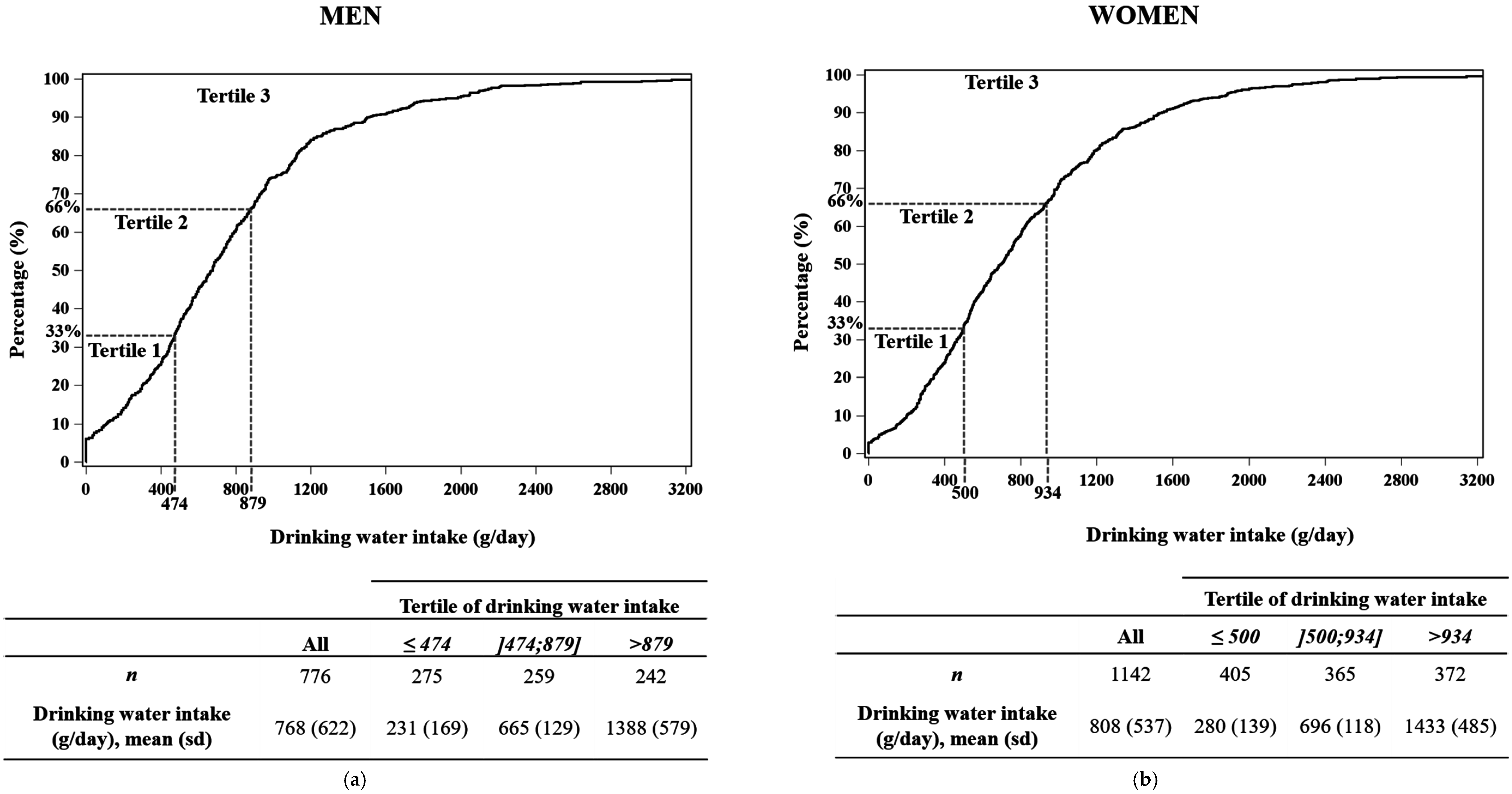
3.1. Drinking Water Intake
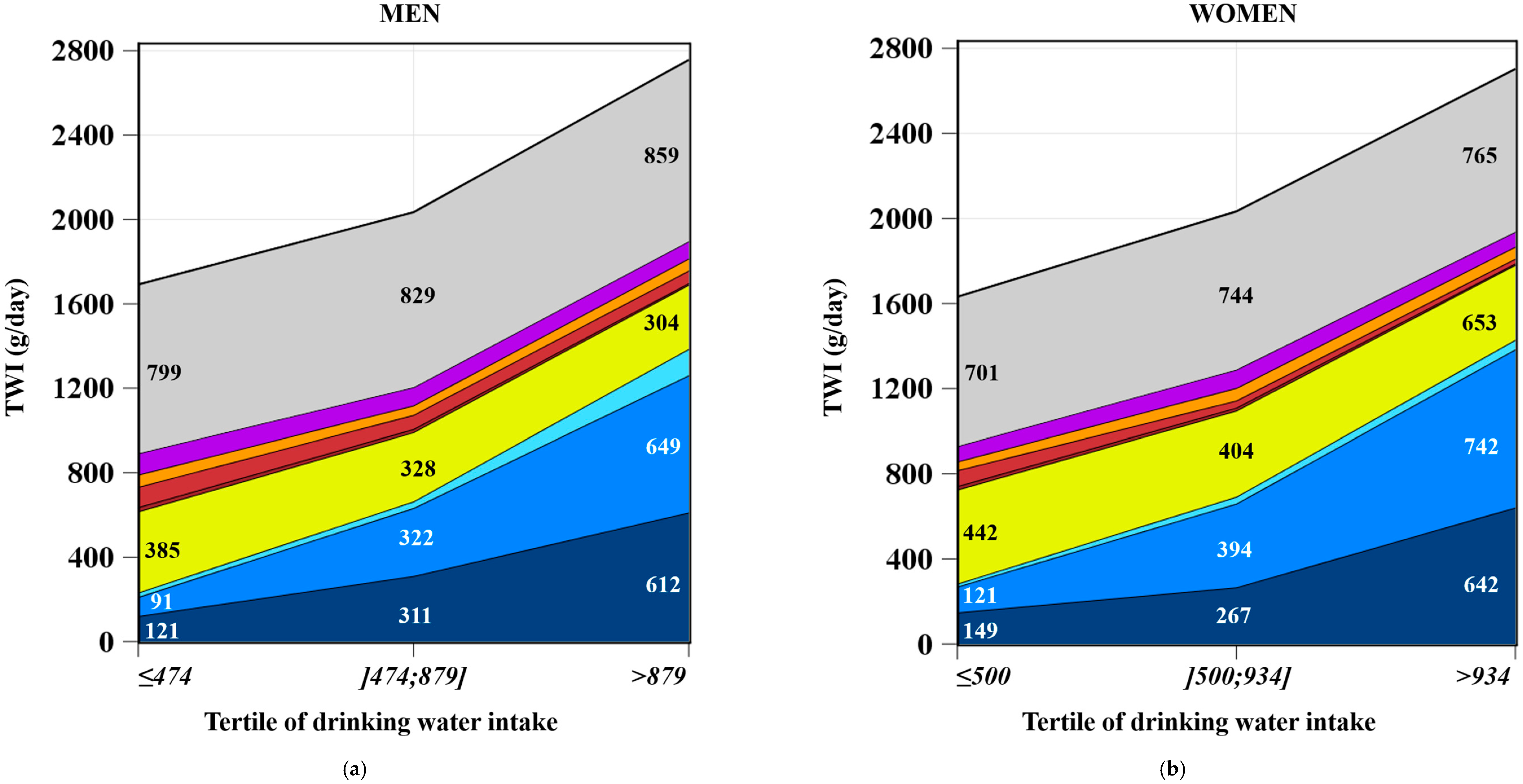
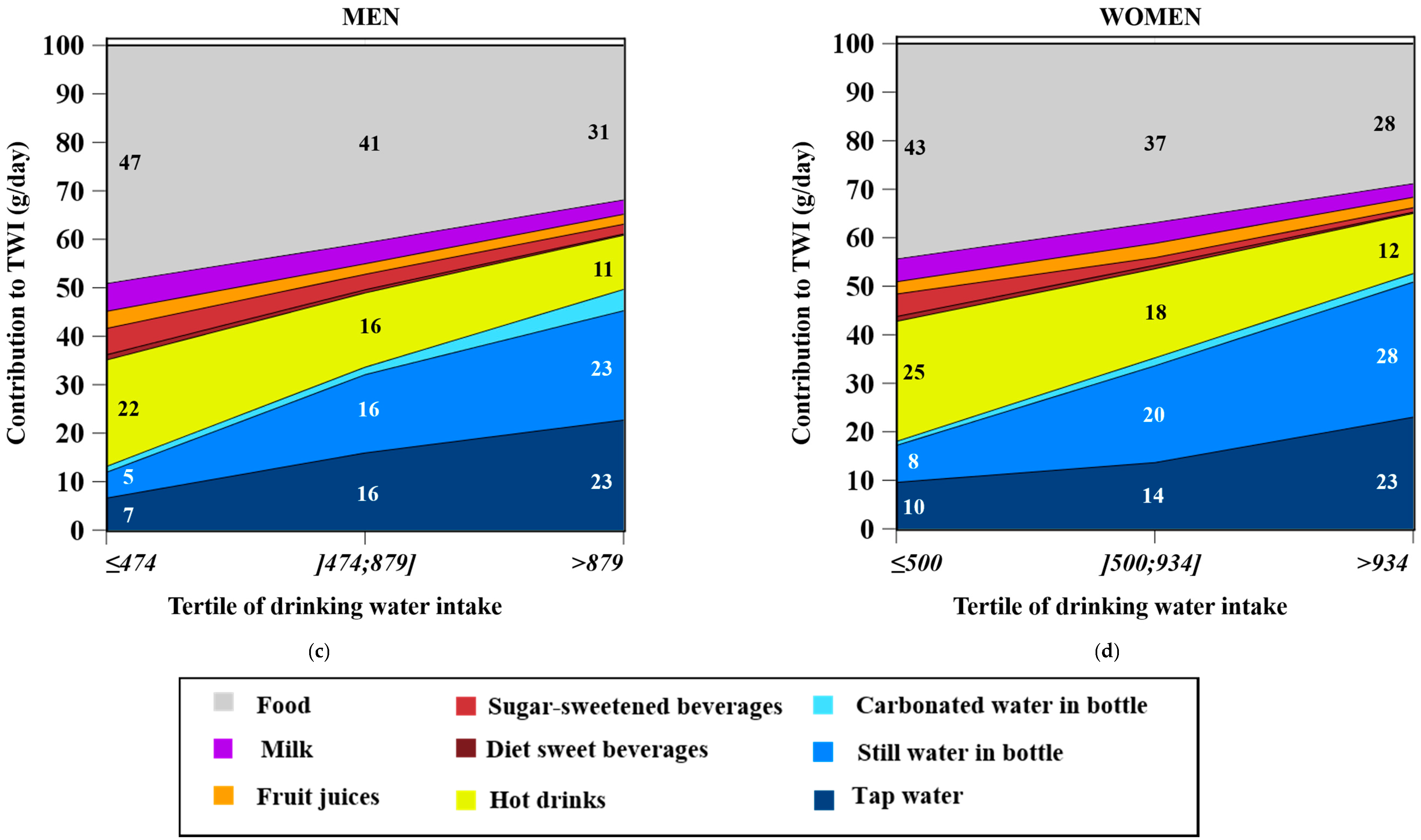
3.2. Water Intakes from Fluids and Food Moisture
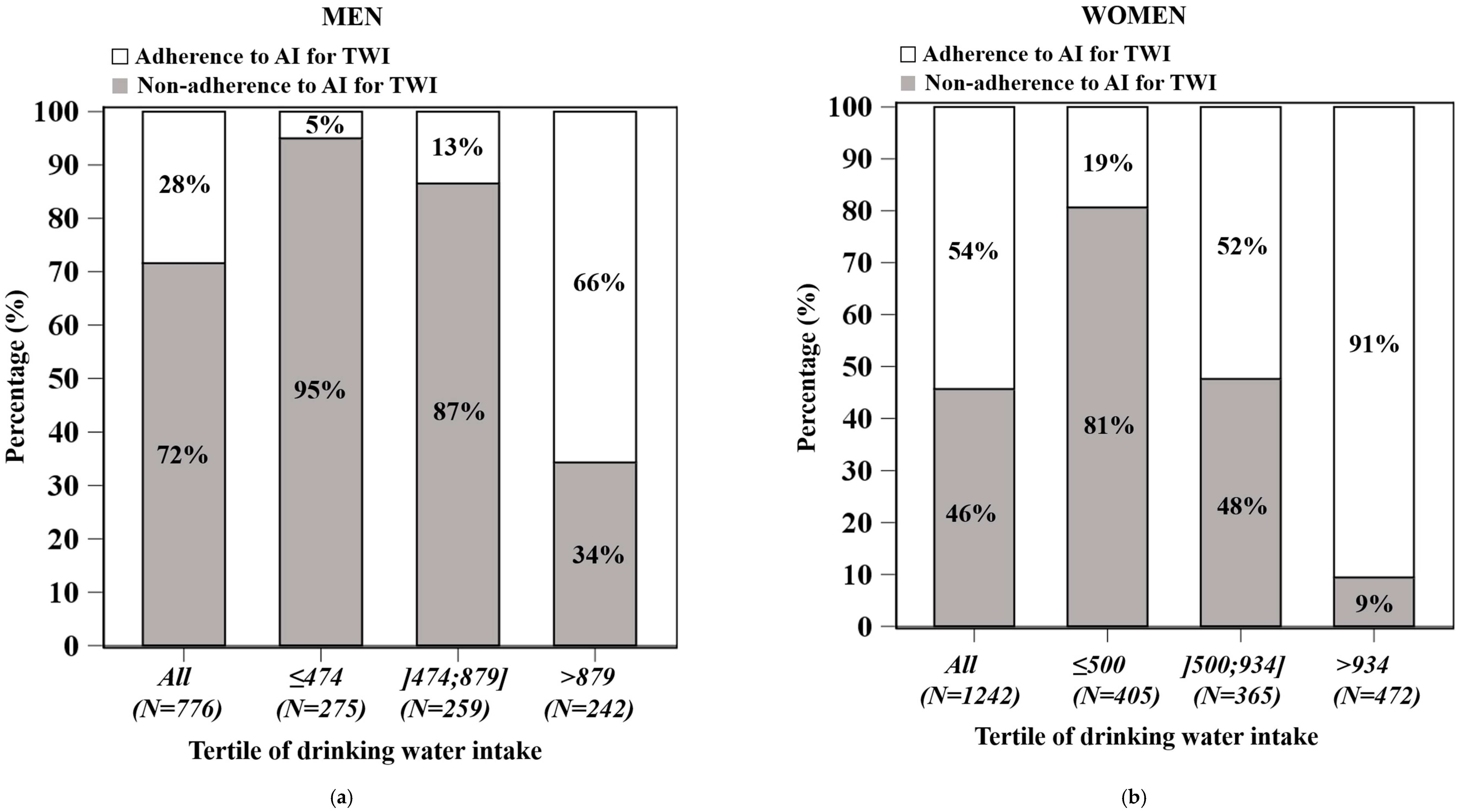
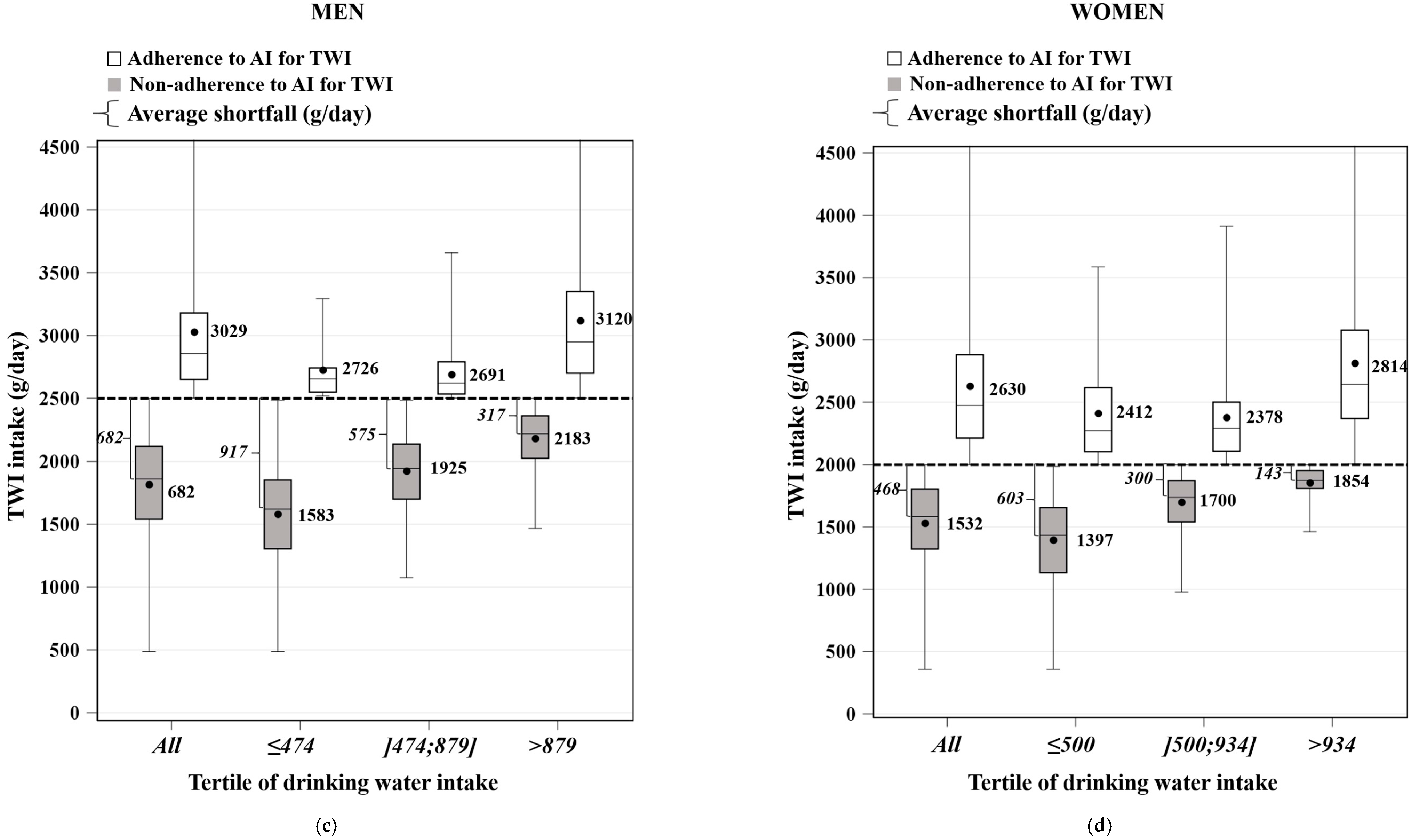
3.3. TWI and Adherence to EFSA AI
3.4. Drinking Water Intake and Nutritional Quality of Diet
3.5. Food Intake Compared to Levels of Drinking Water Intake
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Popkin, B.M.; D’Anci, K.E.; Rosenberg, I.H. Water, hydration, and health. Nutr. Rev. 2010, 68, 439–458. [Google Scholar] [CrossRef] [PubMed]
- Pross, N.; Demazières, A.; Girard, N.; Barnouin, R.; Santoro, F.; Chevillotte, E.; Klein, A.; Le Bellego, L. Influence of progressive fluid restriction on mood and physiological markers of dehydration in women. Br. J. Nutr. 2013, 109, 313–321. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of health claims related to water and maintenance of normal physical and cognitive functions (ID 1102, 1209, 1294, 1331), maintenance of normal thermoregulation (ID 1208) and “basic requirement of all living things. EFSA J. 2011, 9, 2075. [Google Scholar]
- Sontrop, J.M.; Dixon, S.N.; Garg, A.X.; Buendia-Jimenez, I.; Dohein, O.; Huang, S.-H.S.; Clark, W.F. Association between water intake, chronic kidney disease, and cardiovascular disease: A cross-sectional analysis of NHANES data. Am. J. Nephrol. 2013, 37, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Muckelbauer, R.; Sarganas, G.; Grüneis, A.; Müller-Nordhorn, J. Association between water consumption and body weight outcomes: A systematic review. Am. J. Clin. Nutr. 2013, 98, 282–299. [Google Scholar] [CrossRef] [PubMed]
- Roussel, R.; Fezeu, L.; Bouby, N.; Balkau, B.; Lantieri, O.; Alhenc-Gelas, F.; Marre, M.; Bankir, L. Low water intake and risk for new-onset hyperglycemia. Diabetes Care 2011, 34, 2551–2554. [Google Scholar] [CrossRef] [PubMed]
- Clark, W.F.; Sontrop, J.M.; Macnab, J.J.; Suri, R.S.; Moist, L.; Salvadori, M.; Garg, A.X. Urine volume and change in estimated GFR in a community-based cohort study. Clin. J. Am. Soc. Nephrol. 2011, 6, 2634–2641. [Google Scholar] [CrossRef] [PubMed]
- Strippoli, G.F.; Craig, J.C.; Rochtchina, E.; Flood, V.M.; Wang, J.J.; Mitchell, P. Fluid and nutrient intake and risk of chronic kidney disease. Nephrology 2011, 16, 326–334. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for water/European Food Safety Authority. EFSA J. 2010, 8, 48. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate; National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- O’Connor, L.; Walton, J.; Flynn, A. Water intakes and dietary sources of a nationally representative sample of Irish adults. J. Hum. Nutr. Diet. 2014, 27, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Nissensohn, M.; Sánchez-Villegas, A.; Ortega, R.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Varela-Moreiras, G.; Serra-Majem, L. Beverage Consumption Habits and Association with Total Water and Energy Intakes in the Spanish Population: Findings of the ANIBES Study. Nutrients 2016, 8, 232. [Google Scholar] [CrossRef] [PubMed]
- Cartier, T.; Dubuisson, C.; Panetier, P.; Volatier, J.-L. Human water consumption in France: Results from the INCA2 diet study. Environ. Risques Santé 2012, 11, 479–491. [Google Scholar]
- Gibson, S.; Shirreffs, S.M. Beverage consumption habits “24/7” among British adults: Association with total water intake and energy intake. Nutr. J. 2013, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Bellisle, F.; Thornton, S.N.; Hébel, P.; Denizeau, M.; Tahiri, M. A study of fluid intake from beverages in a sample of healthy French children, adolescents and adults. Eur. J. Clin. Nutr. 2010, 64, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Guelinckx, I.; Ferreira-Pêgo, C.; Moreno, L.A.; Kavouras, S.A.; Gandy, J.; Martinez, H.; Bardosono, S.; Abdollahi, M.; Nasseri, E.; Jarosz, A.; Ma, G.; et al. Intake of water and different beverages in adults across 13 Countries. Eur. J. Nutr. 2015, 54, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Vieux, F.; Maillot, M.; Constant, F.; Drewnowski, A. Water and beverage consumption among children aged 4–13 years in France: Analyses of INCA 2 (Étude Individuelle Nationale des Consommations Alimentaires 2006–2007) data. Public Health Nutr. 2016, 19, 2305–2314. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Armstrong, L.E.; Bray, G.M.; Caballero, B.; Frei, B.; Willett, W.C. A new proposed guidance system for beverage consumption in the United States. Am. J. Clin. Nutr. 2006, 83, 529–542. [Google Scholar] [PubMed]
- Duffey, K.J.; Popkin, B.M. Adults with healthier dietary patterns have healthier beverage patterns. J. Nutr. 2006, 136, 2901–2907. [Google Scholar] [PubMed]
- Kant, A.K.; Graubard, B.I.; Atchison, E.A. Intakes of plain water, moisture in foods and beverages, and total water in the adult US population—Nutritional, meal pattern, and body weight correlates: National Health and Nutrition Examination Surveys 1999–2006. Am. J. Clin. Nutr. 2009, 90, 655–663. [Google Scholar] [CrossRef] [PubMed]
- An, R.; McCaffrey, J. Plain water consumption in relation to energy intake and diet quality among US adults, 2005–2012. J. Hum. Nutr. Diet. 2016, 29, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Chun, O.K. Consumptions of plain water, moisture in foods and beverages, and total water in relation to dietary micronutrient intakes and serum nutrient profiles among US adults. Public Health Nutr. 2015, 18, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A.B.; Blanck, H.M.; Sherry, B.; Park, S.; Nebeling, L.; Yaroch, A.L. Behaviors and attitudes associated with low drinking water intake among US adults, Food Attitudes and Behaviors Survey, 2007. Prev. Chronic Dis. 2013, 10, E51. [Google Scholar] [CrossRef] [PubMed]
- Dubuisson, C.; Lioret, S.; Touvier, M.; Dufour, A.; Calamassi-Tran, G.; Volatier, J.-L.; Lafay, L. Trends in food and nutritional intakes of French adults from 1999 to 2007: Results from the INCA surveys. Br. J. Nutr. 2010, 103, 1035–1048. [Google Scholar] [CrossRef] [PubMed]
- Bocquier, A.; Vieux, F.; Lioret, S.; Dubuisson, C.; Caillavet, F.; Darmon, N. Socio-economic characteristics, living conditions and diet quality are associated with food insecurity in France. Public Health Nutr. 2015, 18, 2952–2961. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; Touvier, M.; Lafay, L.; Volatier, J.-L.; Maire, B. Are eating occasions and their energy content related to child overweight and socioeconomic status? Obesity (Silver Spring). 2008, 16, 2518–2523. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Statistics and Economic Studies (INSEE). Definitions and Methods. Definitions. Consumption Unit. Available online: http://www.insee.fr/en/methodes/default.asp?page=definitions/unite-consommation.htm (accessed on 15 June 2016).
- Kendrick, T.; King, F.; Albertella, L.; Smith, P.W. GP treatment decisions for patients with depression: An observational study. Br. J. Gen. Pract. 2005, 55, 280–286. [Google Scholar] [PubMed]
- International Physical Activity Questionnaire (IPAQ). Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)—Short and Long Forms. Available online: https://www.researchgate.net/file.PostFileLoader.html?id=56f92d66615e27d49a658031&assetKey=AS%3A344600888791041%401459170662924 (accessed on 17 April 2016).
- Le Moullec, N.; Deheeger, M.; Preziosi, P.; Montero, P.; Valeix, P.; Rolland-Cachera, M.; Potier de Courcy, G.; Christides, J.; Galan, P.; Hercberg, S. Validation du manuel-photos utilisé pour l’enquête alimentaire de l’étude SUVIMAX. Cah. Nutr. Diet 1996, 31, 158–164. [Google Scholar]
- Agence Nationale de Sécurité Sanitaire de L’alimentation, de L’environnement et du Travail (ANSES). French Food Composition Table Ciqual 2013. Available online: https://pro.anses.fr/TableCIQUAL/index.htm (accessed on 23 March 2016).
- Verger, E.O.; Mariotti, F.; Holmes, B.A.; Paineau, D.; Huneau, J.-F. Evaluation of a diet quality index based on the probability of adequate nutrient intake (PANDiet) using national French and US dietary surveys. PLoS ONE 2012, 7, e42155. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, H.A.; Scheer, J.C. Validity of a dietary score for assessing nutrient adequacy. J. Am. Diet Assoc. 1981, 78, 240–245. [Google Scholar] [PubMed]
- Vieux, F.; Soler, L.-G.; Touazi, D.; Darmon, N. High nutritional quality is not associated with low greenhouse gas emissions in self-selected diets of French adults. Am. J. Clin. Nutr. 2013, 97, 569–583. [Google Scholar] [CrossRef] [PubMed]
- Ledikwe, J.H.; Blanck, H.M.; Khan, L.K.; Serdula, M.K.; Seymour, J.D.; Tohill, B.C.; Rolls, B.J. Low-energy-density diets are associated with high diet quality in adults in the United States. J. Am. Diet. Assoc. 2006, 106, 1172–1180. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, J.; Ferres, S.; Horgan, G. Energy density of foods: Effects on energy intake. Crit. Rev. Food Sci. Nutr. 2000, 40, 481–515. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Caillavet, F.; Joly, C.; Maillot, M.; Drewnowski, A. Low-cost foods: How do they compare with their brand name equivalents? A French study. Public Health Nutr. 2009, 12, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Verger, E.O.; Holmes, B.A.; Huneau, J.F.; Mariotti, F. Simple changes within dietary subgroups can rapidly improve the nutrient adequacy of the diet of French adults. J. Nutr. 2014, 144, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Masset, G.; Vieux, F.; Verger, E.O.; Soler, L.G.; Touazi, D.; Darmon, N. Reducing energy intake and energy density for a sustainable diet: A study based on self-selected diets in French adults. Am. J. Clin. Nutr. 2014, 99, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Kantar Worldpanel. French Household Consumer Panel—Kantar Worldpanel. Available online: http://www.kantarworldpanel.com/global/Sectors (accessed on 5 May 2013).
- Kim, J.; Yang, Y.J. Plain water intake of Korean adults according to life style, anthropometric and dietary characteristic: The Korea National Health and Nutrition Examination Surveys 2008–2010. Nutr. Res. Pract. 2014, 8, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Illescas-Zarate, D.; Espinosa-Montero, J.; Flores, M.; Barquera, S. Plain water consumption is associated with lower intake of caloric beverage: Cross-sectional study in Mexican adults with low socioeconomic status. BMC Public Health 2015, 15, 405. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, V.E.; Davy, B.M.; Duffey, K.J. Is Beverage Consumption Related to Specific Dietary Pattern Intakes? Curr. Nutr. Rep. 2014, 4, 72–81. [Google Scholar] [CrossRef]
- Özen, A.E.; Bibiloni, M.D.M.; Pons, A.; Tur, J.A. Fluid intake from beverages across age groups: A systematic review. J. Hum. Nutr. Diet. 2015, 28, 417–442. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among adults in the United States: Cross-sectional study using data from NHANES 2005–2010. BMC Public Health 2013, 13, 1068. [Google Scholar] [CrossRef] [PubMed]
- Beardsworth, A.; Bryman, A.; Keil, T.; Goode, J.; Haslam, C.; Lancashire, E. Women, men and food: The significance of gender for nutritional attitudes and choices. Brit. Food J. 2002, 104, 470–491. [Google Scholar] [CrossRef]
- Hattersley, L.; Irwin, M.; King, L.; Allman-Farinelli, M. Determinants and patterns of soft drink consumption in young adults: A qualitative analysis. Public Health Nutr. 2009, 12, 1816–1822. [Google Scholar] [CrossRef] [PubMed]
- Martinez, H. Fluid intake in Mexican adults; a cross-sectional study. Nutr. Hosp. 2014, 29, 1179–1187. [Google Scholar] [PubMed]
- Ferreira-Pêgo, C.; Babio, N.; Fenández-Alvira, J.M.; Iglesia, I.; Moreno, L.A.; Salas-Salvadó, J. Fluid intake from beverages in Spanish adults; cross-sectional study. Nutr. Hosp. 2014, 29, 1171–1178. [Google Scholar] [PubMed]
- Manz, F.; Johner, S. A.; Wentz, A.; Boeing, H.; Remer, T. Water balance throughout the adult life span in a German population. Br. J. Nutr. 2012, 107, 1673–1681. [Google Scholar] [CrossRef] [PubMed]
- Agence française de sécurité sanitaire des aliments (AFSSA). Étude Individuelle Nationale des Consommations Alimentaires 2 (INCA 2) 2006–2007; AFSSA: Paris, France, 2009.
- Gandy, J. Water intake: Validity of population assessment and recommendations. Eur. J. Nutr. 2015, 54, 11–16. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Men | Women | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Tertile of Drinking Water Intake | Tertile of Drinking Water Intake | |||||||||
| All | ≤474 mL/Day | 474–879 mL/Day | >879 mL/Day | p | All | ≤500 mL/Day | 500–932 mL/Day | >934 mL/Day | p | |
| n | 776 | 275 | 259 | 242 | 1142 | 405 | 365 | |||
| Mean ± SD | Mean ± SD | |||||||||
| Age (years) | 49.0 ± 17.8 | 50.5 ± 16.9 | 48.7 ± 19.1 | 47.9 ± 17.2 | 0.333 | 45.2 ± 15.0 | 45.4 ± 15.1 | 45.1 ± 15.4 | 45.0 ± 14.6 | 0.977 |
| (%) | (%) | |||||||||
| Socio-occupational status | 0.001 | 0.009 | ||||||||
| Low | 20.4 | 19.1 | 18.1 | 23.9 | 10.1 | 6.9 | 10.1 | 13.4 | ||
| Intermediate | 26.2 | 25.2 | 21.2 | 32.0 | 40.4 | 41.7 | 38.4 | 41.0 | ||
| High | 10.7 | 8.6 | 11.1 | 12.2 | 7.3 | 5.7 | 5.5 | 10.6 | ||
| Economically inactive | 42.7 | 47.1 | 49.6 | 31.9 | 42.2 | 45.7 | 46.1 | 34.9 | ||
| Familial status | 0.182 | 0.204 | ||||||||
| Couple with children | 26.5 | 25.7 | 22.7 | 30.8 | 33.0 | 33.3 | 31.5 | 34.2 | ||
| Couple without child | 47.9 | 52.2 | 47.2 | 44.4 | 34.4 | 29.6 | 35.8 | 37.8 | ||
| Single parent household | 6.3 | 4.9 | 8.8 | 5.2 | 7.0 | 9.1 | 5.9 | 6.0 | ||
| Single without children | 19.3 | 17.2 | 21.3 | 19.5 | 25.4 | 27.9 | 26.4 | 22.1 | ||
| No answer | 0.0 | 0.0 | 0.0 | 0.0 | 0.1 | 0.0 | 0.4 | 0.0 | ||
| Quintile of ICU † | 0.009 | 0.154 | ||||||||
| 1 | 20.2 | 25.2 | 18.2 | 17.3 | 20.6 | 23.5 | 20.9 | 17.5 | ||
| 2 | 19.3 | 21.3 | 22.3 | 14.3 | 19.9 | 19.1 | 19.2 | 21.2 | ||
| 3 | 23.1 | 14.9 | 27.3 | 26.9 | 19.6 | 21.5 | 18.9 | 18.6 | ||
| 4 | 19.6 | 19.2 | 17.8 | 21.8 | 23.2 | 20.7 | 24.9 | 24.0 | ||
| 5 | 17.8 | 19.4 | 14.3 | 19.8 | 16.7 | 15.1 | 16.1 | 18.7 | ||
| Food insecurity | 0.339 | 0.303 | ||||||||
| Yes | 9.9 | 9.3 | 11.9 | 8.3 | 11.9 | 14.0 | 10.2 | 11.5 | ||
| No | 85.9 | 84.2 | 83.7 | 89.6 | 83.2 | 81.7 | 86.0 | 81.9 | ||
| No answer | 4.3 | 6.4 | 4.3 | 2.1 | 4.9 | 4.4 | 3.8 | 6.6 | ||
| Perception of household financial situation | 0.242 | 0.174 | ||||||||
| High | 6.4 | 8.7 | 5.3 | 5.3 | 94.7 | 92.8 | 94.8 | 96.6 | ||
| Low | 93.0 | 90.5 | 93.9 | 94.6 | 5.0 | 7.0 | 4.7 | 3.4 | ||
| No answer | 0.5 | 0.7 | 0.8 | 0.1 | 0.3 | 0.2 | 0.6 | 0.0 | ||
| Level of education | 0.010 | 0.599 | ||||||||
| Low | 15.4 | 21.0 | 17.0 | 8.4 | 20.1 | 22.1 | 20.2 | 18.1 | ||
| Intermediate | 55.5 | 53.4 | 53.8 | 59.2 | 48.6 | 49.1 | 49.5 | 47.2 | ||
| High | 29.0 | 25.7 | 29 | 32.2 | 31.2 | 28.8 | 30.0 | 34.7 | ||
| No answer | 0.1 | 0.0 | 0.2 | 0.2 | 0.1 | 0.0 | 0.3 | 0.0 | ||
| Region of residence | 0.128 | 0.008 | ||||||||
| Northwest | 13.8 | 12.8 | 13.3 | 15.2 | 15 | 11.2 | 19 | 15 | ||
| East | 8.9 | 10.0 | 11.2 | 5.6 | 9.7 | 8.5 | 8.7 | 11.8 | ||
| Ile De France | 17.7 | 19.7 | 14.7 | 18.8 | 17.3 | 22.5 | 15.0 | 14.3 | ||
| West | 14.1 | 15.2 | 13.8 | 13.3 | 14.4 | 12.5 | 18.1 | 12.6 | ||
| Centre | 10.4 | 10.4 | 13.6 | 7.4 | 9.6 | 10.3 | 9.5 | 9.1 | ||
| Centre-east | 11.6 | 10.1 | 7.9 | 16.5 | 12.6 | 14.8 | 12.2 | 10.8 | ||
| South-west | 11.2 | 10.4 | 12.8 | 10.3 | 10.0 | 9.2 | 6.2 | 14.4 | ||
| South-east | 12.4 | 11.5 | 12.6 | 13.0 | 11.5 | 11.1 | 11.4 | 12.0 | ||
| Season of protocol completion | 0.004 | <0.001 | ||||||||
| Winter | 23.8 | 27.4 | 25.0 | 19.0 | 26.9 | 33.1 | 25.3 | 22.5 | ||
| Spring | 26.4 | 22.4 | 25.4 | 31.4 | 23.5 | 23.6 | 22.1 | 24.7 | ||
| Summer | 24.0 | 21.2 | 20.3 | 30.3 | 26.9 | 16.8 | 28.9 | 35.0 | ||
| Autumn | 25.9 | 29.0 | 29.3 | 19.4 | 22.6 | 26.5 | 23.7 | 17.8 | ||
| Level of physical activity (IPAQ score) | 0.017 | 0.808 | ||||||||
| Low | 20.7 | 24.6 | 20.6 | 17.0 | 24.0 | 23.3 | 24.3 | 24.5 | ||
| Middle | 29.6 | 31.8 | 33.9 | 23.2 | 32.4 | 34.2 | 33.4 | 29.7 | ||
| High | 48.6 | 43.3 | 45.3 | 56.9 | 42.4 | 41.6 | 41.1 | 44.5 | ||
| No answer | 1.1 | 0.2 | 0.2 | 2.8 | 1.1 | 0.9 | 1.2 | 1.2 | ||
| Smoker | 0.004 | 0.164 | ||||||||
| Smoker | 28.1 | 36.5 | 22.3 | 25.7 | 23.3 | 26.9 | 19.9 | 23.0 | ||
| Not smoker | 71.9 | 63.5 | 77.7 | 74.3 | 76.7 | 73.1 | 80.1 | 77.0 | ||
| Men | |||||||
|---|---|---|---|---|---|---|---|
| Tertile of Drinking Water Intake | |||||||
| All | ≤474 mL/Day | 474–879 mL/Day | >879 mL/Day | ||||
| Variables | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | p † | p ‡ | p for Trend § |
| Energy (kcal/day) | 2403.8 ± 592.0 | 2289.7 ± 529.3 | 2400.1 ± 551.3 | 2518.0 ± 671.2 | <0.001 | 0.003 | 0.001 |
| Total water (TWI 2, g/day) | 2160.8 ± 28.8 | 1691.6 ± 25.2 | 2034.1 ± 19.9 | 2756.7 ± 41.2 | <0.001 | <0.001 | <0.001 |
| Water from foods (g/day) | 829.1 ± 16.9 | 798.9 ± 15.7 | 829.2 ± 18.0 | 859.3 ± 17.2 | 0.041 | 0.032 | 0.009 |
| Water from fluids (g/day) | 1331.7 ± 27.3 | 892.7 ± 24.1 | 1204.9 ± 17.9 | 1897.3 ± 40.0 | <0.001 | <0.001 | <0.001 |
| Total weight (g/day) | 2668.3 ± 29.1 | 2199.9 ± 25.3 | 2540.4 ± 20.4 | 3264.7 ± 41.7 | <0.001 | <.0001 | <0.001 |
| Weight of solid foods (g/day) | 1304.6 ± 18.1 | 1270.4 ± 17.4 | 1306.0 ± 18.8 | 1337.3 ± 18.3 | 0.036 | 0.022 | 0.006 |
| Weight of fluids (g/day) | 1363.8 ± 28.3 | 929.5 ± 25.6 | 1234.3 ± 18.6 | 1927.5 ± 40.6 | <0.001 | <0.001 | <0.001 |
| Food variety | 56.1 ± 1.1 | 53.2 ± 1.0 | 57.6 ± 1.2 | 57.5 ± 1.1 | 0.003 | 0.121 | |
| Energy from alcohol | 180.4 ± 194.4 | 216.2 ± 211.9 | 154 ± 171.4 | 171.5 ± 191.1 | 0.008 | 0.007 | 0.030 |
| Alcoholic drinks | 255.4 ± 21.2 | 294.7 ± 20.9 | 222.8 ± 22.4 | 248.7 ± 20.4 | 0.053 | 0.077 | |
| SED (kcal/100 g) | 179.9 ± 2.1 | 183.0 ± 2.2 | 180.0 ± 2.3 | 176.8 ± 2.0 | 0.119 | 0.084 | |
| PANDiet | 62.5 ± 0.5 | 61.4 ± 0.4 | 62.6 ± 0.5 | 63.7 ± 0.5 | 0.001 | 0.084 | |
| Adequacy subscore | 69.6 ± 0.7 | 68.1 ± 0.7 | 69.7 ± 0.7 | 71.0 ± 0.6 | 0.005 | 0.274 | |
| Moderate subscore | 55.5 ± 0.7 | 54.7 ± 0.7 | 55.4 ± 0.7 | 56.3 ± 0.7 | 0.235 | 0.299 | |
| MAR (% adequacy) | 83.3 ± 0.4 | 82.3 ± 0.5 | 83.4 ± 0.4 | 84.2 ± 0.4 | 0.006 | 0.093 | |
| MER (% excess) | 44.4 ± 1.2 | 47.2 ± 1.2 | 43.9 ± 1.2 | 42.1 ± 1.2 | 0.004 | 0.065 | |
| Cost (€/day) | 7.3 ± 0.1 | 7.0 ± 0.1 | 7.3 ± 0.1 | 7.7 ± 0.1 | <0.001 | <0.001 | <0.001 |
| Cost (€/2000 kcal) | 6.2 ± 0.2 | 5.8 ± 0.2 | 6.1 ± 0.2 | 6.5 ± 0.2 | <0.001 | 0.084 | |
| Proteins (% energy) | 16.9 ± 2.9 | 17.0 ± 3.3 | 17.0 ± 2.8 | 16.6 ± 2.7 | 0.326 | 0.369 | |
| Carbohydrates (% energy) | 43.0 ± 6.9 | 43.0 ± 7.2 | 42.6 ± 6.6 | 43.4 ± 7.0 | 0.459 | 0.751 | |
| Total fat (% energy) | 37.9 ± 6.2 | 37.8 ± 6.0 | 38.2 ± 5.9 | 37.7 ± 6.7 | 0.681 | 0.885 | |
| Saturated fat (% energy) | 14.6 ± 3.3 | 14.9 ± 3.1 | 14.7 ± 3.2 | 14.3 ± 3.6 | 0.141 | 0.306 | |
| Free sugar (% energy) | 9.0 ± 5.6 | 9.4 ± 5.9 | 8.7 ± 5.3 | 8.9 ± 5.5 | 0.372 | 0.243 | |
| Fiber (g) † | 20.6 ± 0.3 | 20.1 ± 0.3 | 20.5 ± 0.3 | 21.1 ± 0.4 | 0.099 | 0.038 | 0.015 |
| Saturated fat (g/day) | 39.3 ± 0.6 | 39.9 ± 0.5 | 39.4 ± 0.5 | 38.5 ± 0.7 | 0.229 | 0.421 | |
| Free sugar (g/day) | 56.0 ± 2.2 | 59.7 ± 2.3 | 54.6 ± 2.3 | 53.7 ± 2.1 | 0.119 | 0.105 | |
| Sodium (mg/day) | 3664.1 ± 49.9 | 3652.5 ± 45.4 | 3684.0 ± 58.4 | 3655.8 ± 45.7 | 0.895 | 0.769 | |
| Women | |||||||
| Tertile of Drinking Water Intake | |||||||
| All | ≤500 mL/Day | 500–934 mL/Day | >934 mL/Day | ||||
| Variables | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | p † | p ‡ | p for Trend § |
| Energy (kcal/day) | 1866.1 ± 427.1 | 1779.4 ± 421.9 | 1910.9 ± 407.7 | 1908.6 ± 440.5 | 0.001 | 0.003 | 0.004 |
| Total water (TWI 2, g/day) | 2122.3 ± 34.2 | 1631.4 ±33.5 | 2033.0± 34.8 | 2702.6 ± 34.4 | <0.001 | <0.001 | <0.001 |
| Water from foods (g/day) | 736.3 ± 13.7 | 700.9 ± 14.9 | 743.5 ± 13.0 | 764.5 ± 13.1 | 0.004 | 0.006 | 0.002 |
| Water from fluids (g/day) | 1386.1 ± 30.2 | 930.6 ± 25.2 | 1289.5 ± 35.5 | 1938.1 ± 29.9 | <0.001 | <0.001 | <0.001 |
| Total weight (g/day) | 2512.2 ± 34.7 | 2021.0 ± 33.8 | 2422.3 ± 35.6 | 3093.4 ± 34.8 | <0.001 | <0.001 | <0.001 |
| Weight of solid foods (g/day) | 1100.2 ± 14.6 | 1063.0 ± 15.8 | 1105.9 ± 14.0 | 1131.7 ± 14.0 | 0.004 | 0.005 | 0.001 |
| Weight of fluids (g/day) | 1412.1 ± 30.7 | 958.0 ± 25.9 | 1316.4 ± 36.3 | 1961.8 ± 29.9 | <0.001 | <0.001 | <0.001 |
| Food variety | 59.8 ± 0.8 | 55.5 ± 0.6 | 62.9 ± 1.0 | 61.1 ± 0.8 | <0.001 | <0.001 | <0.001 |
| Energy from alcohol | 49.5 ± 70.5 | 45.1 ± 65.4 | 53.4± 67.1 | 50.2 ± 78.5 | 0.397 | 0.257 | |
| Alcoholic drinks | 63.2 ± 6.0 | 57.9 ± 5.7 | 66.2 ± 5.8 | 65.4 ± 6.5 | 0.547 | 0.438 | |
| SED (kcal/100 g) | 165.5 ± 2.0 | 171.7 ± 2.5 | 164.3 ± 1.9 | 160.5 ± 1.7 | 0.001 | <0.001 | <0.001 |
| PANDiet | 62.3 ± 0.5 | 60.6 ± 0.5 | 62.6 ± 0.4 | 63.6 ± 0.5 | <0.001 | 0.001 | <0.001 |
| Adequacy subscore | 64.3 ± 0.6 | 60.7 ± 0.6 | 65.8 ± 0.5 | 66.5 ± 0.6 | <0.001 | <0.001 | <0.001 |
| Moderate subscore | 60.2 ± 0.7 | 60.5 ± 0.6 | 59.3 ± 0.7 | 60.7±0.7 | 0.295 | 0.188 | |
| MAR (% adequacy) | 79.1 ± 0.4 | 76.4 ± 0.5 | 79.9 ± 0.4 | 80.8 ± 0.4 | <0.001 | <0.001 | <0.001 |
| MER (% excess) | 21.7 ± 0.9 | 23.3 ± 1.1 | 21.7 ± 1.0 | 20.2 ± 0.7 | 0.089 | 0.199 | |
| Cost (€/day) | 6.2 ± 0.2 | 5.8 ± 0.2 | 6.3 ± 0.2 | 6.5 ± 0.2 | <0.001 | <0.001 | <0.001 |
| Cost (€/2000 kcal) | 6.8 ± 0.1 | 6.3 ± 0.1 | 6.9 ±0.1 | 7.2 ± 0.1 | <0.001 | <0.001 | <0.001 |
| Proteins (% energy) | 16.2 ± 2.7 | 16.2 ± 2.8 | 16.1 ± 2.7 | 16.3 ± 2.7 | 0.608 | 0.810 | |
| Carbohydrates (% energy) | 42.5 ± 5.7 | 42.8 ± 6.1 | 42.3 ± 5.9 | 42.4 ± 5.2 | 0.507 | 0.427 | |
| Total fat (% energy) | 38.8 ± 5.3 | 38.6 ± 5.3 | 39.2 ± 5.5 | 38.8 ± 5.1 | 0.552 | 0.388 | |
| Saturated fat (% energy) | 14.6 ± 2.8 | 14.6 ± 2.9 | 14.8 ± 2.7 | 14.6 ± 2.9 | 0.592 | 0.508 | |
| Free sugar (% energy) | 9.9 ± 4.8 | 10.2 ± 5.7 | 10.2 ± 4.4 | 9.4 ± 4.0 | 0.066 | 0.028 | 0.028 |
| Fibre (g) † | 16.9 ± 0.3 | 16.3 ± 0.2 | 16.7 ± 0.3 | 17.5 ± 0.2 | 0.003 | <0.001 | <0.001 |
| Saturated fat (g/day) | 30.4 ± 0.4 | 30.3 ± 0.3 | 30.6 ± 0.4 | 30.3 ± 0.4 | 0.769 | 0.662 | |
| Free sugar (g/day) | 47.4 ± 1.5 | 49.8 ± 1.7 | 48.1 ± 1.5 | 44.2 ± 1.2 | 0.015 | 0.006 | 0.003 |
| Sodium (mg/day) | 2687.1 ± 40.6 | 2577.2 ± 30.8 | 2712.3 ± 54.8 | 2771.9 ± 36.4 | <0.001 | <0.001 | <0.001 |
| Men | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tertile of Drinking Water Intake | |||||||||||
| All | ≤474 mL/Day | 474–879 mL/Day | >879 mL/Day | ||||||||
| Food Groups and Subgroups (g/Day) | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | p † | p ‡ | p for Trend § | ||||
| Fruits and vegetables | 368.1 ± 19.1 | 336.6 ± 16.3 | 370.4 ± 21.3 | 397.4 ± 19.7 | 0.069 | 0.076 | |||||
| Vegetables, soup and crudités | 210.0 ± 11.6 | 201.2 ± 12.1 | 215.1 ± 11.8 | 213.6 ± 10.8 | 0.602 | 0.449 | |||||
| Fresh and processed fruits | 155.9 ± 11.1 | 132.4 ± 7.6 | 153.3 ± 12.3 | 181.9 ± 13.4 | 0.008 * | 0.048 * | 0.015 | ||||
| Nuts | 2.3 ± 0.4 | 3.0 ± 0.5 | 2.0 ± 0.4 | 1.9 ± 0.3 | 0.139 | 0.209 | |||||
| Starches | 306.3 ± 7.5 | 303.1 ± 8.1 | 304.6 ± 6.2 | 311.3 ± 8.0 | 0.742 | 0.355 | |||||
| Refined starches | 212.0 ± 6.3 | 206.0 ± 7.5 | 210.7 ± 5.9 | 219.4 ± 5.4 | 0.316 | 0.093 | |||||
| Unrefined starches | 89.8 ± 4.0 | 91.3 ±3.7 | 89.6±3.4 | 88.5 ± 4.9 | 0.907 | 0.869 | |||||
| Cereals for breakfast | 4.5 ± 1.3 | 5.8 ± 1.8 | 4.4 ± 1.1 | 3.4 ± 1.0 | 0.504 | 0.200 | |||||
| Meats/fishes/eggs | 190.9±4.7 | 181.1 ± 4.6 | 194.5 ± 4.4 | 197.3 ± 5.1 | 0.026 * | 0.034 * | 0.027 | ||||
| Eggs | 16.2 ± 1.2 | 15.2 ± 1.1 | 17.1 ± 1.3 | 16.2 ± 1.3 | 0.530 | 0.503 | |||||
| Fishes | 30.2 ± 2.1 | 27.6 ± 2.1 | 31.9 ± 2.1 | 31.2 ± 2.1 | 0.271 | 0.514 | |||||
| Meat | 144.6 ± 4.6 | 138.3 ± 4.6 | 145.5 ± 4.1 | 149.9 ± 5.2 | 0.270 | 0.253 | |||||
| Mixed dishes and sandwiches | 153.6 ± 7.6 | 175.1 ± 7.3 | 148.3 ± 8.6 | 137.4 ± 6.9 | <0.001 * | 0.001 * | 0.001 | ||||
| Ready-made dishes and stocks | 90.9 ± 5.6 | 101.4 ± 5.1 | 90.6 ± 5.5 | 80.7 ± 6.2 | 0.018 * | 0.063 | |||||
| Sandwiches and savoury puff pastries | 62.7 ± 5.3 | 73.7 ± 6.1 | 57.6 ± 5.0 | 56.7 ± 4.8 | 0.018 * | 0.002 * | 0.001 | ||||
| Dairy products | 214.1 ± 14.3 | 219.3 ± 20.9 | 211.1 ± 11.9 | 211.7 ± 10.0 | 0.924 | 0.603 | |||||
| Milk | 101.9 ± 13.1 | 114.7 ± 20.2 | 98.0 ± 10.5 | 93.1 ± 8.5 | 0.563 | 0.247 | |||||
| Fresh dairy products | 70.9 ± 5.8 | 61.4 ± 5.1 | 71.2 ± 5.1 | 80.1 ± 7.4 | 0.075 | 0.167 | |||||
| Cheese | 41.2 ± 2.8 | 43.2 ± 2.8 | 42.0 ± 2.7 | 38.5 ± 2.8 | 0.332 | 0.502 | |||||
| Sweet products | 123.6 ± 4.7 | 126.4 ± 4.6 | 125.9 ± 4.9 | 118.5 ± 4.6 | 0.367 | 0.601 | |||||
| Dairy dessert | 18.6 ± 2.2 | 20.6 ± 2.2 | 17.5 ± 2.2 | 17.8 ± 2.2 | 0.550 | 0.532 | |||||
| Cakes, tarts, sweet pastries | 67.5 ± 3.8 | 67.8 ± 4.2 | 70.0 ± 4.1 | 64.6 ± 3.1 | 0.585 | 0.564 | |||||
| Biscuits and sweets | 37.5 ± 2.4 | 38.0 ± 2.1 | 38.4 ± 3.1 | 36.0 ± 2.0 | 0.791 | 0.774 | |||||
| Drinking water | 761.5 ± 18.5 | 232.4 ± 11.1 | 664.8 ± 8.5 | 1387.3 ± 35.8 | <0.001 * | <0.001 * | <0.001 | ||||
| Tap water | 348.2 ± 24.2 | 120.9 ± 11.3 | 311.2 ± 22.2 | 612.6 ± 38.9 | <0.001 * | <0.001 * | <0.001 | ||||
| Still water in a bottle | 354.1 ± 28.1 | 90.7 ± 10.9 | 322.3 ± 24.1 | 649.2±49.3 | <0.001 * | <0.001 * | <0.001 | ||||
| Carbonated water in a bottle | 59.2 ± 14.0 | 20.8 ± 4.7 | 31.3 ± 5.5 | 125.5±31.8 | 0.005 * | 0.025 * | 0.007 | ||||
| Beverages | 500.3 ± 21.1 | 582.4 ± 21.9 | 471.5 ± 21.3 | 447.0 ± 20.2 | <0.001 * | <0.001 * | <0.001 | ||||
| Hot drinks (Tea. Coffee) | 343.6 ± 18.5 | 389.8 ± 20.4 | 332.4 ± 17.4 | 308.7 ± 17.7 | 0.011 * | 0.010 * | 0.003 | ||||
| Diet sweet beverages | 14.4 ± 4.8 | 20.3 ± 5.8 | 14.8 ± 5.7 | 8.1 ± 3.0 | 0.086 | 0.351 | |||||
| Sugar-sweetened beverages | 82.2 ± 12.4 | 106.8 ± 14.7 | 74.0 ± 10.9 | 65.9 ± 11.5 | 0.035 * | 0.055 | |||||
| Fruit juices | 60.1 ± 6.7 | 65.6 ± 8.4 | 50.3 ± 4.9 | 64.4 ± 6.9 | 0.092 | 0.064 | |||||
| Fat products | 47.0 ± 1.9 | 42.5 ± 1.5 | 47.8 ± 2.1 | 50.6 ± 2.0 | 0.003 * | 0.003 * | 0.001 | ||||
| Animal fat | 14.7 ± 0.9 | 14.7 ± 0.8 | 14.6 ± 1.2 | 14.7 ± 0.8 | 0.993 | 0.844 | |||||
| Vegetable fat | 23.2 ± 1.4 | 19.7 ± 1.3 | 23.6 ± 1.6 | 26.3 ± 1.2 | 0.001 * | 0.001 * | <0.001 | ||||
| Spices and sauces | 9.1 ± 0.9 | 8.2 ± 0.7 | 9.6 ± 0.7 | 9.6 ± 1.3 | 0.183 | 0.286 | |||||
| Women | |||||||||||
| Tertile of Drinking Water Intake | |||||||||||
| All | ≤500 mL/Day | 500–934 mL/Day | >934 mL/Day | ||||||||
| Food Groups and Subgroups (g/Day) | Mean | SD | Mean | SD | Mean | SD | Mean | SD | p † | p ‡ | p for Trend § |
| Fruits and vegetables | 374.7 | 13.4 | 345.8 | 16.9 | 378.7 | 12.5 | 399.5 | 10.7 | 0.047 | 0.008 | 0.003 |
| Vegetables, soup and crudités | 213.7 | 8.6 | 203.0 | 10.3 | 216.4 | 7.9 | 221.6 | 7.7 | 0.333 | 0.105 | |
| Fresh and processed fruits | 159.3 | 8.3 | 141.2 | 8.5 | 160.5 | 7.5 | 176.0 | 8.8 | 0.025 | 0.037 | 0.011 |
| Nuts | 1.8 | 0.3 | 1.6 | 0.2 | 1.8 | 0.3 | 1.9 | 0.3 | 0.777 | 0.712 | |
| Starches | 202.4 | 4.8 | 207.7 | 5.4 | 192.8 | 4.1 | 206.7 | 5.1 | 0.019 | 0.005 | 0.551 |
| Refined starches | 126.8 | 3.5 | 130.4 | 3.2 | 120.7 | 3.4 | 129.1 | 3.9 | 0.084 | 0.084 | |
| Unrefined starches | 70.3 | 3.5 | 73.5 | 3.7 | 66.6 | 2.8 | 70.9 | 3.9 | 0.342 | 0.223 | |
| Cereals for breakfast | 5.4 | 1.0 | 3.8 | 0.8 | 5.5 | 1.0 | 6.7 | 1.1 | 0.056 | 0.299 | |
| Meats/fishes/eggs | 138.1 | 3.0 | 134.7 | 2.7 | 137.8 | 3.3 | 141.8 | 3.0 | 0.165 | 0.579 | |
| Eggs | 14.4 | 1.3 | 15.0 | 1.6 | 12.9 | 1.0 | 15.4 | 1.4 | 0.285 | 0.194 | |
| Fishes | 29.8 | 1.6 | 27.9 | 1.4 | 31.3 | 1.9 | 30.3 | 1.5 | 0.229 | 0.345 | |
| Meat | 93.9 | 2.7 | 91.9 | 2.5 | 93.7 | 2.9 | 96.2 | 2.6 | 0.495 | 0.793 | |
| Mixed dishes and sandwiches | 106.5 | 4.5 | 107.7 | 5.8 | 113.1 | 4.0 | 98.8 | 3.8 | 0.035 | 0.003 | 0.214 |
| Ready-made dishes and stocks | 64.8 | 3.3 | 61.7 | 2.9 | 70.8 | 3.7 | 61.8 | 3.2 | 0.122 | 0.043 | |
| Sandwiches and savoury puff pastries | 41.7 | 2.9 | 46.0 | 4.2 | 42.3 | 2.4 | 36.9 | 2.1 | 0.159 | 0.008 | 0.023 |
| Dairy products | 199.4 | 9.6 | 185.5 | 8.8 | 213.1 | 11.2 | 199.5 | 8.7 | 0.182 | 0.353 | |
| Milk | 86.3 | 7.6 | 82.0 | 6.3 | 97.3 | 8.3 | 79.5 | 8.2 | 0.217 | 0.240 | |
| Fresh dairy products | 86.6 | 4.6 | 78.5 | 4.1 | 89.2 | 5.0 | 92.0 | 4.6 | 0.080 | 0.603 | |
| Cheese | 26.5 | 1.4 | 25.0 | 1.3 | 26.7 | 1.3 | 27.9 | 1.6 | 0.309 | 0.114 | |
| Sweet products | 111.9 | 4.2 | 114.9 | 3.5 | 116.1 | 5.7 | 104.7 | 3.5 | 0.047 | 0.004 | 0.002 |
| Dairy dessert | 18.1 | 2.3 | 16.9 | 1.4 | 19.7 | 3.2 | 17.8 | 2.4 | 0.734 | 0.711 | |
| Cakes, tarts, sweet pastries | 61.1 | 3.4 | 62.8 | 3.6 | 65.2 | 3.9 | 55.2 | 2.6 | 0.057 | 0.013 | |
| Biscuits and sweets | 32.7 | 1.8 | 35.2 | 2.0 | 31.2 | 1.6 | 31.7 | 1.9 | 0.238 | 0.419 | |
| Drinking water | 802.5 | 14.9 | 284.0 | 8.3 | 693.2 | 8.1 | 1430.3 | 28.2 | <0.001 | <0.001 | <0.001 |
| Tap water | 352.8 | 23.6 | 148.8 | 8.3 | 266.7 | 18.0 | 642.9 | 44.6 | <0.001 | <0.001 | <0.001 |
| Still water in a bottle | 419.2 | 21.6 | 121.2 | 8.5 | 394.1 | 20.1 | 742.4 | 36.3 | <0.001 | <0.001 | <0.001 |
| Carbonated water in a bottle | 30.5 | 5.2 | 14.0 | 3.6 | 32.3 | 5.2 | 45.1 | 6.7 | <0.001 | <0.001 | <0.001 |
| Beverages | 523.3 | 29.5 | 592.0 | 27.5 | 526.0 | 35.7 | 451.9 | 25.4 | <0.001 | <0.001 | <0.001 |
| Hot drinks (Tea. Coffee) | 404.1 | 27.8 | 447.0 | 23.8 | 408.4 | 34.6 | 356.8 | 25.1 | 0.011 | 0.018 | 0.005 |
| Diet sweet beverages | 12.2 | 3.5 | 16.2 | 4.9 | 13.7 | 3.9 | 6.8 | 1.6 | 0.016 | 0.014 | 0.100 |
| Sugar-sweetened beverages | 48.4 | 10.4 | 82.9 | 17.6 | 37.5 | 9.5 | 24.8 | 4.2 | 0.006 | 0.007 | 0.002 |
| Fruit juices | 58.6 | 6.4 | 45.9 | 8.7 | 66.3 | 5.2 | 63.5 | 5.2 | 0.069 | 0.049 | 0.150 |
| Fat products | 45.1 | 1.2 | 43.0 | 0.9 | 45.1 | 1.1 | 47.1 | 1.4 | 0.033 | 0.029 | 0.008 |
| Animal fat | 13.3 | 0.8 | 13.5 | 0.7 | 12.9 | 0.7 | 13.6 | 0.8 | 0.786 | 0.489 | |
| Vegetable fat | 23.4 | 0.9 | 22.2 | 0.8 | 23.6 | 0.8 | 24.5 | 1.1 | 0.117 | 0.189 | |
| Spices and sauces | 8.3 | 0.7 | 7.3 | 0.6 | 8.6 | 0.5 | 9.0 | 0.9 | 0.198 | 0.300 | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gazan, R.; Sondey, J.; Maillot, M.; Guelinckx, I.; Lluch, A. Drinking Water Intake Is Associated with Higher Diet Quality among French Adults. Nutrients 2016, 8, 689. https://doi.org/10.3390/nu8110689
Gazan R, Sondey J, Maillot M, Guelinckx I, Lluch A. Drinking Water Intake Is Associated with Higher Diet Quality among French Adults. Nutrients. 2016; 8(11):689. https://doi.org/10.3390/nu8110689
Chicago/Turabian StyleGazan, Rozenn, Juliette Sondey, Matthieu Maillot, Isabelle Guelinckx, and Anne Lluch. 2016. "Drinking Water Intake Is Associated with Higher Diet Quality among French Adults" Nutrients 8, no. 11: 689. https://doi.org/10.3390/nu8110689
APA StyleGazan, R., Sondey, J., Maillot, M., Guelinckx, I., & Lluch, A. (2016). Drinking Water Intake Is Associated with Higher Diet Quality among French Adults. Nutrients, 8(11), 689. https://doi.org/10.3390/nu8110689