Use of interferon-gamma release assay and tuberculin skin test in diagnosing tuberculosis in Lithuanian adults: A comparative analysis

Abstract
:1. Introduction
2. Material and methods
2.1. Study sample
2.2. Tuberculin skin test
2.3. T SPOT TB
2.4. Statistical analysis
3. Results
4. Discussion
5. Conclusions
Conflict of Interest
Contributions
Acknowledgments
R E F E R E N C E S
- Dheda, K; Barry, CE, 3rd; Maartens, G. Tuberculosis. Lancet 2015. [Google Scholar] [CrossRef]
- World Health Organization. Tuberculosis. Tuberculosis country profiles. https://extranet.who.int/sree/Reports?op=Replet&name=%2FWHO_HQ_Reports%2FG2%2FPROD%2FEXT%2FTBCountryProfile&ISO2=LT&LAN=EN&outtype=html [accessed 29.09.15].
- de Vries, G; Aldridge, RW; Cayla, JA; Haas, WH; Sandgren, A; van Hest, NA; et al. Epidemiology of tuberculosis in big cities of the European Union and European Economic Area countries. Euro Surveill 2014, 19(9). [Google Scholar] [CrossRef]
- Ignatyeva, O; Balabanova, Y; Nikolayevskyy, V; Koshkarova, E; Radiulyte, B; Davidaviciene, E; et al. Resistance profile and risk factors of drug resistant tuberculosis in the Baltic countries. Tuberculosis (Edinb) 2015, 95(5), 581–8. [Google Scholar] [CrossRef] [PubMed]
- Getahun, H; Matteelli, A; Abubakar, I; Aziz, MA; Baddeley, A; Barreira, D; et al. Management of latent Mycobacterium tuberculosis infection: WHO guidelines for low tuberculosis burden countries. Eur Respir J 2015. [Google Scholar] [CrossRef] [PubMed]
- Moreno, S; Blázquez, R; Novoa, A; Carpena, I; Menasalvas, A; Ramírez, C; et al. The effect of BCG vaccination on tuberculin reactivity and the booster effect among hospital employees. Arch Intern Med 2001, 161(14), 1760–5. [Google Scholar] [CrossRef] [PubMed]
- Nayak, S; Acharjya, B. Mantoux test and its interpretation. Indian Dermatol Online J 2012, 3(1), 2–6. [Google Scholar] [CrossRef] [PubMed]
- Singh, D; Sutton, C; Woodcock, A. Repeat tuberculin testing in BCG-vaccinated subjects in the United Kingdom. The booster effect varies with the time of reading. Am J Respir Crit Care Med 2001, 164(6), 962–4. [Google Scholar] [CrossRef] [PubMed]
- Tissot, F; Zanetti, G; Francioli, P; Zellweger, JP; Zysset, F. Influence of bacille Calmette-Guérin vaccination on size of tuberculin skin test reaction: to what size? Clin Infect Dis 2005, 40(2), 211–7. [Google Scholar] [CrossRef] [PubMed]
- The BCG world atlas. A database of global BCG vaccination policies and practices. http://www.bcgatlas.org/ [accessed 21.11.15].
- Infuso, A; Falzon, D. EuroTB network. European survey of BCG vaccination policies and surveillance in children, 2005. Euro Surveill 2006, 11(3), 6–11. [Google Scholar] [CrossRef] [PubMed]
- Zellweger, JP; Zellweger, A; Ansermet, S; de Senarclens, B; Wrighton-Smith, P. Contact tracing using a new T-cell-based test: better correlation with tuberculosis exposure than the tuberculin skin test. Int J Tuberc Lung Dis 2005, 9(11), 1242–7. [Google Scholar] [PubMed]
- King, TC; Upfal, M; Gottlieb, A; Adamo, P; Bernacki, E; Kadlecek, CP; et al. T-SPOT.TB interferon-γ release assay performance in healthcare worker screening at nineteen U.S. Hospitals. Am J Respir Crit Care Med 2015, 192(3), 367–73. [Google Scholar] [CrossRef] [PubMed]
- De Keyser, E; De Keyser, F; De Baets, F. Tuberculin skin test versus interferon-gamma release assays for the diagnosis of tuberculosis infection. Acta Clin Belg 2014, 69(5), 358–66. [Google Scholar] [CrossRef] [PubMed]
- Borkowska, D; Zwolska, Z; Michałowska-Mitczuk, D; Korzeniewska-Koseła, M; Zabost, A; Napiórkowska, A; et al. Interferon-gamma assays T-SPOT.TB for the diagnosis of latent tuberculosis infection. Pneumonol Alergol Pol 2011, 79(4), 264–71. [Google Scholar] [PubMed]
- Yan, L; Xiao, H; Han, M; Zhang, Q. Diagnostic value of T-SPOT.TB interferon-γ release assays for active tuberculosis. Exp Ther Med 2015, 10(1), 345–51. [Google Scholar] [CrossRef] [PubMed]
- Arenas Miras Mdel, M; Hidalgo-Tenorio, C; Jimenez-Gamiz, P; Jiménez-Alonso, J. Diagnosis of latent tuberculosis in patients with systemic lupus erythematosus: T.SPOT.TB versus tuberculin skin test. Biomed Res Int 2014, 291031. [Google Scholar]
- Meier, T; Eulenbruch, HP; Wrighton-Smith, P; Enders, G; Regnath, T. Sensitivity of a new commercial enzyme-linked immunospot assay (T SPOT-TB) for diagnosis of tuberculosis in clinical practice. Eur J Clin Microbiol Infect Dis 2005, 24(8), 529–36. [Google Scholar] [CrossRef] [PubMed]
- Landizabal, AA; Reichman, LB. Diagnosis of latent tuberculosis infection. Tuberculosis and nontuberculous mycobacterial infections, 5th ed.; McGraw-Hill Medical Publishing Division: New York, USA, 2006; pp. 61–70. [Google Scholar]
- Mazurek, GH; Jereb, J; Vernon, A; LoBue, P; Goldberg, S; Castro, K; et al. Updated guidelines for using interferon gamma release assays to detect Mycobacterium tuberculosis infection United States, 2010. MMWR Recomm Rep 2010, 59(RR-5), 1–25. [Google Scholar] [PubMed]
- Hansted, E; Andriuskeviciene, A; Sakalauskas, R; Kevalas, R; Sitkauskiene, B. T-cell-based diagnosis of tuberculosis infection in children in Lithuania: a country of high incidence despite a high coverage with bacille Calmette-Guerin vaccination. BMC Pulm Med 2009, 9, 41. [Google Scholar] [CrossRef] [PubMed]
- Pan, L; Jia, H; Liu, F; Sun, H; Gao, M; Du, F; et al. Risk factors for false-negative T-SPOT.TB assay results in patients with pulmonary and extra-pulmonary TB. J Infect 2015, 70(4), 367–80. [Google Scholar] [CrossRef] [PubMed]
- Encinales, L; Zuñiga, J; Granados-Montiel, J; Yunis, M; Granados, J; Almeciga, I; et al. Humoral immunity in tuberculin skin test anergy and its role in high-risk persons exposed to active tuberculosis. Mol Immunol 2010, 47(5), 1066–73. [Google Scholar] [CrossRef] [PubMed]
- Storla, DG; Kristiansen, I; Oftung, F; Korsvold, GE; Gaupset, M; Gran, G; et al. Use of interferon gamma-based assay to diagnose tuberculosis infection in health care workers after short term exposure. BMC Infect Dis 2009, 9, 60. [Google Scholar] [CrossRef] [PubMed]
- Leung, CC; Yam, WC; Ho, PL; Yew, WW; Chan, CK; Law, WS; et al. T-Spot.TB outperforms tuberculin skin test in predicting development of active tuberculosis among household contacts. Respirology 2015, 20(3), 496–503. [Google Scholar] [CrossRef] [PubMed]
- Dilektasli, AG; Erdem, E; Durukan, E; Eyüboğlu, FÖ. Is the T-cell-based interferon-gamma releasing assay feasible for diagnosis of latent tuberculosis infection in an intermediate tuberculosis-burden country? Jpn J Infect Dis 2010, 63(6), 433–6. [Google Scholar] [PubMed]
- Feng, Y; Diao, N; Shao, L; Wu, J; Zhang, S; Jin, J; et al. Interferon gamma release assay performance in pulmonary and extrapulmonary tuberculosis. PLoS ONE 2012, 7(3), e32652. [Google Scholar] [CrossRef] [PubMed]
- Balmelli, C; Zysset, F; Pagnamenta, A; Francioli, P; Lazor-Blanchet, C; Zanetti, G; et al. Contact tracing investigation after professional exposure to tuberculosis in a Swiss hospital using both tuberculin skin test and IGRA. Swiss Med Wkly 2014, 144, w13988. [Google Scholar] [CrossRef] [PubMed]
- Katsenos, S; Nikolopoulou, M; Konstantinidis, AK; Gartzonika, C; Gogali, A; Margelis, I; et al. Interferon-gamma release assay clarifies the effect of bacille Calmette-Guérin vaccination in Greek army recruits. Int J Tuberc Lung Dis 2010, 14(5), 545–50. [Google Scholar] [PubMed]
- Hizel, K; Maral, I; Karakus, R; Aktas, F. The influence of BCG immunisation on tuberculin reactivity and booster effect in adults in a country with a high prevalence of tuberculosis. Clin Microbiol Infect 2004, 10(11), 980–3. [Google Scholar] [CrossRef] [PubMed]
- Farhat, M; Greenaway, C; Pai, M; Menzies, D. False-positive tuberculin skin tests: what is the absolute effect of BCG and non-tuberculous mycobacteria? Int J Tuberc Lung Dis 2006, 10(11), 1192–204. [Google Scholar] [PubMed]
- Araujo, Z; de Waard, JH; de Larrea, CF; Borges, R; Convit, J. The effect of Bacille Calmette-Guérin vaccine on tuberculin reactivity in indigenous children from communities with high prevalence of tuberculosis. Vaccine 2008, 26(44), 5575–81. [Google Scholar] [CrossRef] [PubMed]
- Belknap, R; Daley, CL. Interferon-gamma release assays. Clin Lab Med 2014, 34(2), 337–49. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S; Shao, L; Mo, L; Chen, J; Wang, F; Meng, C; et al. Evaluation of gamma interferon release assays using Mycobacterium tuberculosis antigens for diagnosis of latent and active tuberculosis in Mycobacterium bovis BCG-vaccinated populations. Clin Vaccine Immunol 2010, 17(12), 1985–90. [Google Scholar] [CrossRef] [PubMed]
- Pavić, I; Hojsak, I; Žmak, L; Tješić-Drinković, D; Bogović, JČ; Katalinić-Janković, V. Choosing a tuberculin skin test for the child with hyperreactive tuberculin skin test results. Lijec Vjesn 2015, 137(7–8), 241–5. [Google Scholar]
- Nienhaus, A; Schablon, A; Costa, JT; Diel, R. Systematic review of cost and cost-effectiveness of different TB-screening strategies. BMC Health Serv Res 2011, 11, 247. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic | Diagnosed TB (N = 40) | Healthcare workers (N = 22) | Low risk of TB (N = 21) |
|---|---|---|---|
| Men, N (% of studied subjects) | 27 (32.5) | 0 (0.0) | 7 (8.4) |
| Women, N (% of studied subjects) | 13 (15.7) | 22 (26.5) | 14 (16.9) |
| Age, years | 42.7 ± 2.4 | 47.4 ± 2.7 | 40.9 ± 3.1 |
| T SPOT TB positive, N (%) | 39 (97.5)* | 8 (36.4)‡ | 0 (0) |
| T SPOT A spots number | 15.3 ± 1.9* | 6.5 ± 2.5 | 1.5 ± 0.5 |
| T SPOT B spots number | 22.4 ± 2.5* | 6.0 ± 1.5† | 2.0 ± 0.4 |
| TST positive, N (%) | 37 (92.5)† | 21 (95.5)† | 15 (71.4) |
| Mean TST diameter, mm | 14.0 ± 0.7 | 16.2 ± 1.3 | 10.4 ± 1.4 |
| Values are mean ± SEM unless otherwise indicated. | |||
| * P < 0.01 compared to healthcare workers and low risk of TB groups. | |||
| † P < 0.05 compared to low risk of TB group. | |||
| ‡ P < 0.01 compared to low risk of TB group. | |||
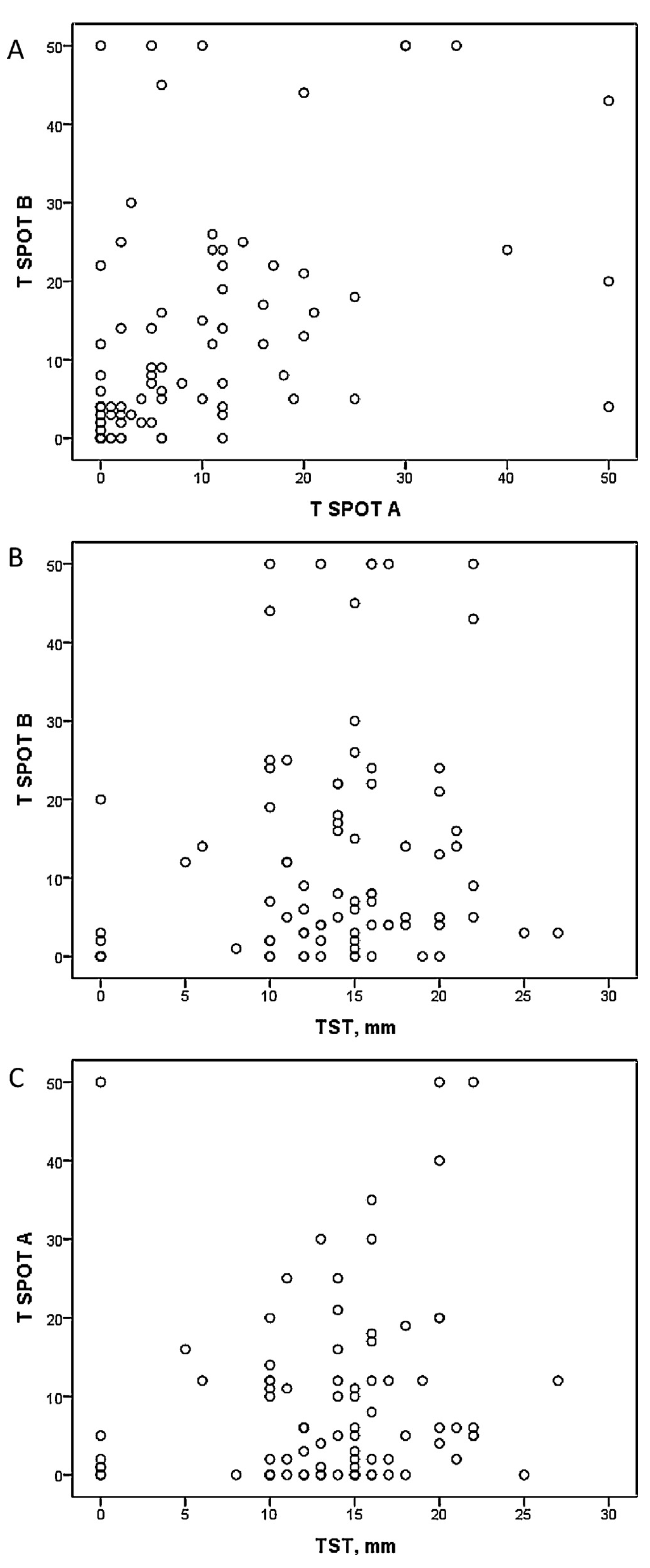
| T SPOT A | T SPOT B | TST | ||
|---|---|---|---|---|
| Diagnosed TB | T SPOT A | – | 0.08 | −0.01 |
| T SPOT B | 0.08 | – | 0.10 | |
| TST | −0.01 | 0.10 | – | |
| Healthcare workers | T SPOT A | – | 0.27 | 0.33* |
| T SPOT B | 0.27 | – | 0.21 | |
| TST | 0.33* | 0.21 | – | |
| Low risk of TB | T SPOT A | – | 0.06 | −0.01 |
| T SPOT B | 0.06 | – | 0.32 | |
| TST | −0.01 | 0.32 | – | |
| * P < 0.05. | ||||
| T SPOT TB positive | T SPOT TB negative | Total | |
|---|---|---|---|
| TST 0–4 mm | 1 (14.3) | 6 (85.7) | 7 (100.0) |
| TST 5–9 mm | 2 (66.7) | 1 (33.3) | 3 (100.0) |
| TST 10–14 mm | 19 (59.4) | 13 (40.6) | 32 (100.0) |
| TST ≥15 mm | 25 (61.0) | 16 (39.0) | 41 (100.0) |
| Values are N (%). | |||
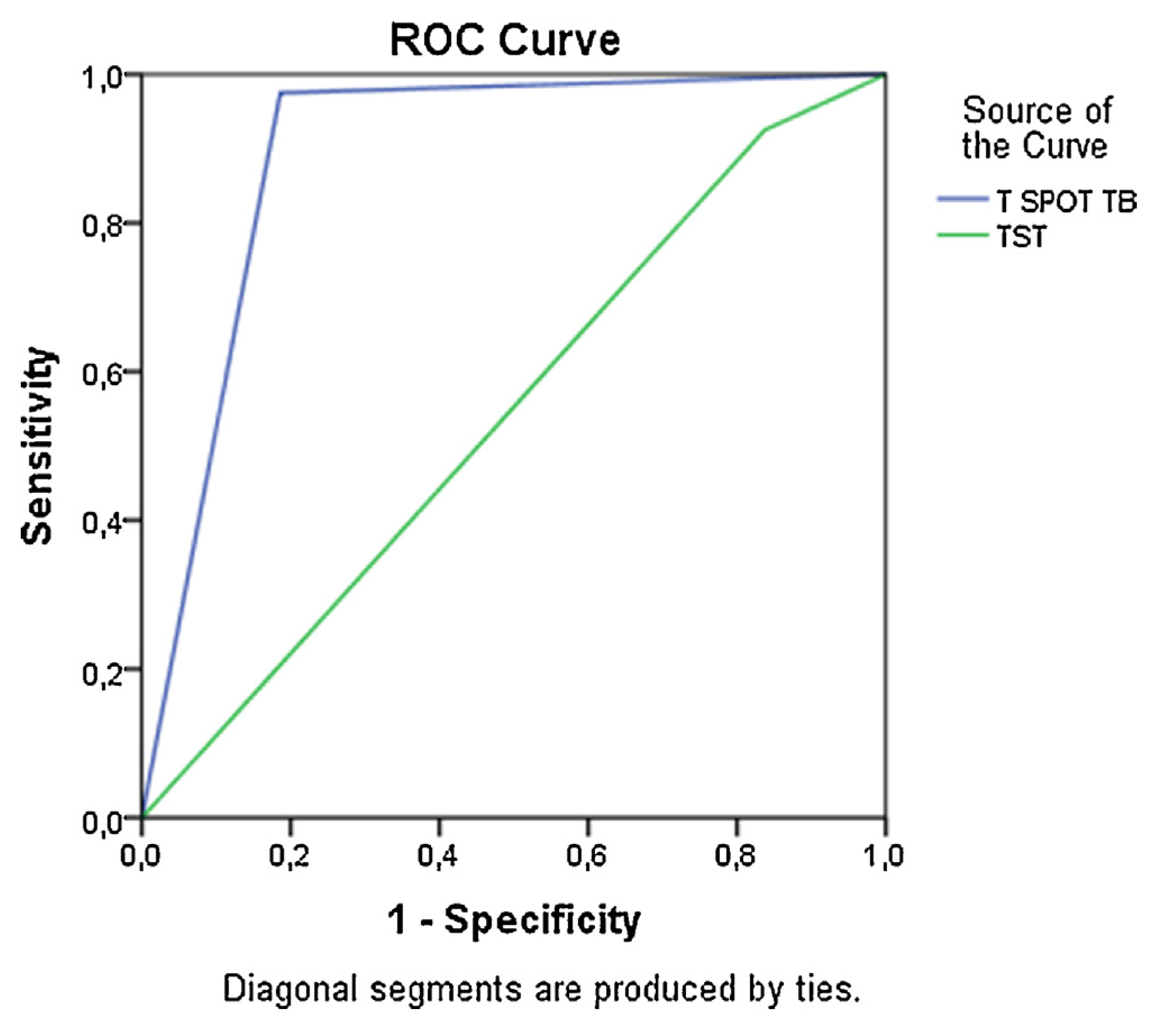
| Test | Specificity, % | Sensitivity, % | NPV, % | PPV, % |
|---|---|---|---|---|
| TST | 28.6 | 92.5 | 66.7 | 70.6 |
| T SPOT TB | 100.0 | 97.5 | 94.6 | 100.0 |
© 2017 The Lithuanian University of Health Sciences. Production and hosting by Elsevier Sp. z o.o. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Share and Cite
Tamašauskienė, L.; Hansted, E.; Vitkauskienė, A.; Miliauskas, S.; Naudžiūnas, A.; Šitkauskienė, B. Use of interferon-gamma release assay and tuberculin skin test in diagnosing tuberculosis in Lithuanian adults: A comparative analysis. Medicina 2017, 53, 159-165. https://doi.org/10.1016/j.medici.2017.05.003
Tamašauskienė L, Hansted E, Vitkauskienė A, Miliauskas S, Naudžiūnas A, Šitkauskienė B. Use of interferon-gamma release assay and tuberculin skin test in diagnosing tuberculosis in Lithuanian adults: A comparative analysis. Medicina. 2017; 53(3):159-165. https://doi.org/10.1016/j.medici.2017.05.003
Chicago/Turabian StyleTamašauskienė, Laura, Edita Hansted, Astra Vitkauskienė, Skaidrius Miliauskas, Albinas Naudžiūnas, and Brigita Šitkauskienė. 2017. "Use of interferon-gamma release assay and tuberculin skin test in diagnosing tuberculosis in Lithuanian adults: A comparative analysis" Medicina 53, no. 3: 159-165. https://doi.org/10.1016/j.medici.2017.05.003