Timing of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Single-Center Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
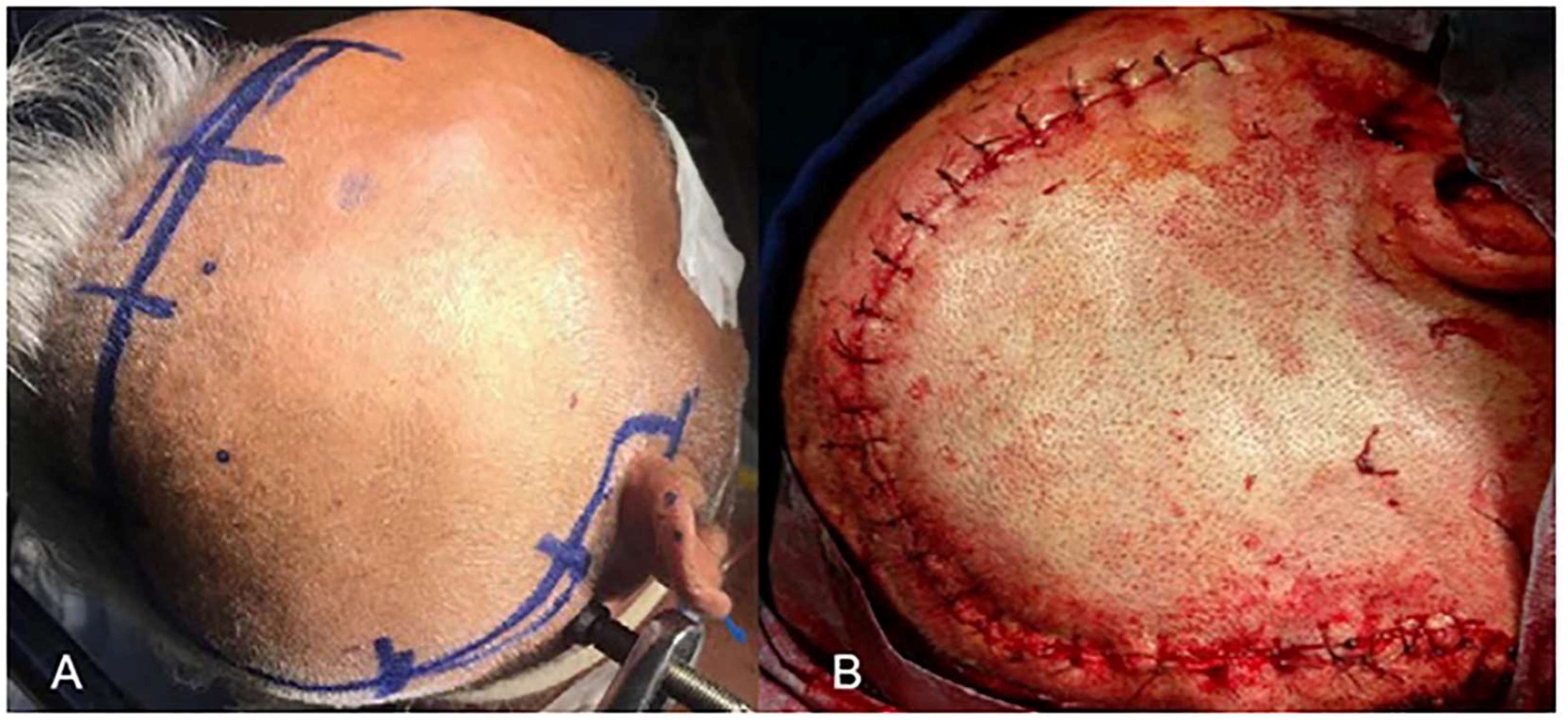
2.2. Surgical Procedure
2.3. Statistical Analysis
3. Results
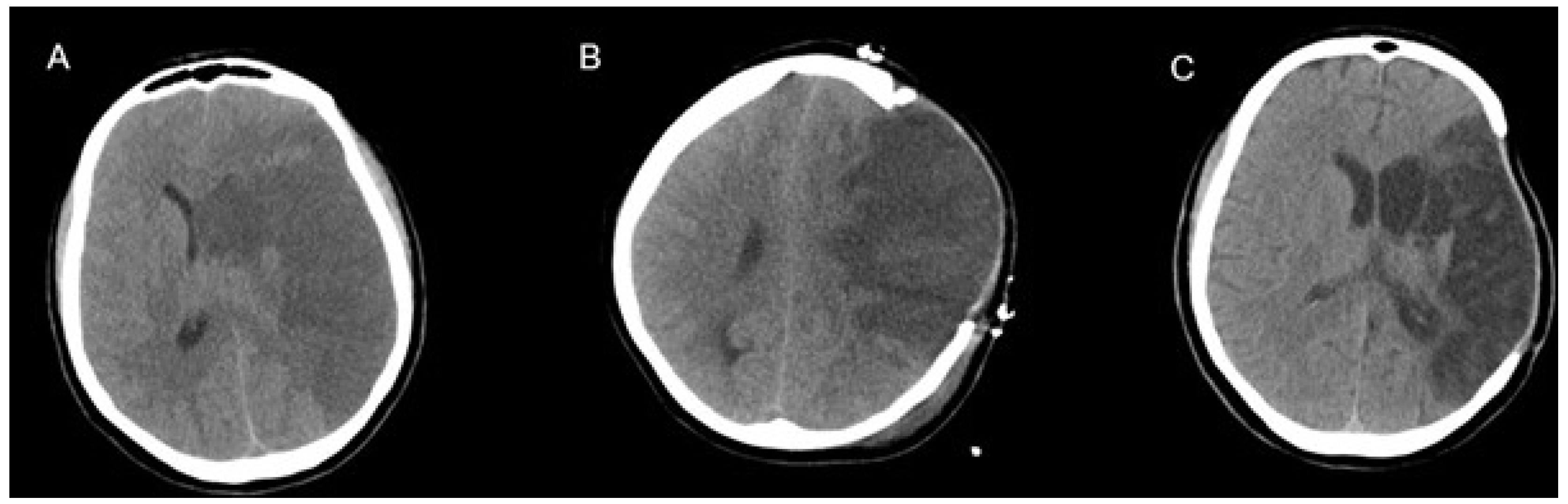
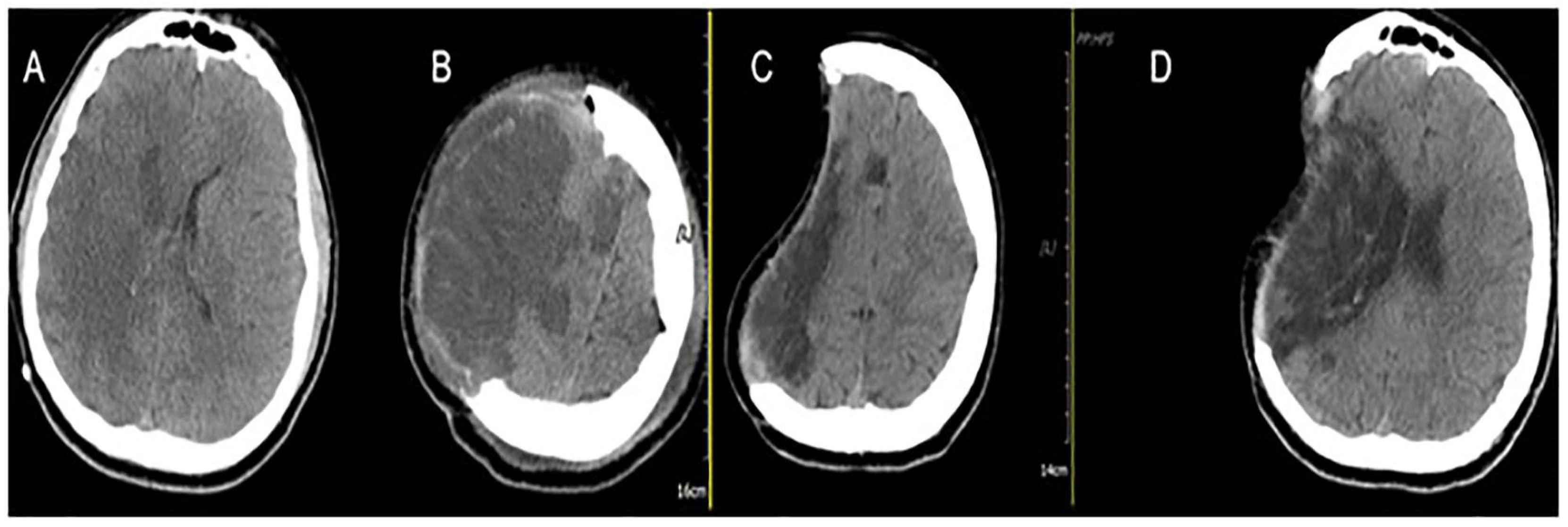
Illustrative Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Treadwell, S.D.; Thanvi, B. Malignant middle cerebral artery (MCA) infarction: Pathophysiology, diagnosis and management. Postgrad. Med. J. 2010, 86, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Hacke, W.; Schwab, S.; Horn, M.; Spranger, M.; De Georgia, M.; Von Kummer, R. ‘Malignant’ middle cerebral artery territory infarction: Clinical course and prognostic signs. Arch. Neurol. 1996, 53, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Vahedi, K.; Hofmeijer, J.; Juettler, E.; Vicaut, E.; George, B.; Algra, A.; Amelink, G.J.; Schmiedeck, P.; Schwab, S.; Rothwell, P.M.; et al. Early decompressive surgery in malignant infarction of the middle cerebral artery: A pooledanalysis of three randomised controlled trials. Lancet Neurol. 2007, 6, 215–222. [Google Scholar] [CrossRef]
- Balan, C.; Alliez, B. Decompressive craniectomy: From option to standard—Part I. Rom Neurosurg. 2009, 16, 20–26. [Google Scholar]
- Chen, C.C.; Cho, D.Y.; Tsai, S.C. Outcome of and prognostic factors for decompressive hemicraniectomy in malignant middle cerebral artery infarction. J. Clin. Neurosci. 2007, 14, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Dasenbrock, H.H.; Robertson, F.C.; Vaitkevicius, H.; Aziz-Sultan, M.A.; Guttieres, D.; Dunn, I.F.; Du, R.; Gormley, W.B. Timing of decompressive hemicraniectomy for stroke: A nationwide inpatient sample analysis. Stroke 2017, 48, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Wartenberg, K.E. Malignant middle cerebral artery infarction. Curr. Opin. Crit. Care 2012, 18, 152–163. [Google Scholar] [CrossRef] [PubMed]
- Heiss, W.D. Malignant MCA Infarction: Pathophysiology and Imaging for Early Diagnosis and Management Decisions. Cerebrovasc. Dis. 2016, 41, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bansal, H.; Chaudhary, A.; Singh, A.; Paul, B.; Garg, R. Decompressive craniectomy in malignant middle cerebral artery infarct: An institutional experience. Asian J. Neurosurg. 2015, 10, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Yoo, B.R.; Yoo, C.J.; Kim, M.J.; Kim, W.K.; Choi, D.H. Analysis of the outcome and prognostic factors of decompressive craniectomy between young and elderly patients for acute middle cerebral artery infarction. J. Cerebrovasc. Endovasc. Neurosurg. 2016, 18, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Hofmeijer, J.; Kappelle, L.J.; Algra, A.; Amelink, G.J.; van Gijn, J.; van der Worp, H.B. Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial (HAMLET)): A multicentre, open, randomised trial. Lancet Neurol. 2009, 8, 326–333. [Google Scholar] [CrossRef]
- Vahedi, K.; Vicaut, E.; Mateo, J.; Kurtz, A.; Orabi, M.; Guichard, J.P.; Boutron, C.; Couvreur, G.; Rouanet, F.; Touzé, E.; et al. Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery infarction (DECIMAL Trial). Stroke 2007, 38, 2506–2517. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Connolly, E.S.; Mayer, S.; Elkind, M.S. Hemicraniectomy for massive middle cerebral artery territory infarction: A systematic review. Stroke 2004, 35, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Juttler, E.; Schwab, S.; Schmiedek, P.; Unterberg, A.; Hennerici, M.; Woitzik, J.; Witte, S.; Jenetzky, E.; Hacke, W. Decompressive surgery for the treatment of malignant infarction of the middle cerebral artery (DESTINY): A randomized, controlled trial. Stroke 2007, 38, 2518–2525. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.W.; Choi, J.H.; Kim, D.H.; Cha, J.K.; Huh, J.T. Outcome following decompressive craniectomy for malignant middle cerebral artery infarction in patients older than 70 years old. J. Cerebrovasc. Endovasc. 2012, 14, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Frank, J.I.; Schumm, L.P.; Wroblewski, K.; Chyatte, D.; Rosengart, A.J.; Kordeck, C.; Thisted, R.A.; HeADDFIRST, T.; Bernardini, G.; Andrefsky, J. Hemicraniectomy and durotomy upon deterioration from infarction-related swelling trial: Randomized pilot clinical trial. Stroke 2014, 45, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Montano, N.; Bianchi, F.; D’Alessandris, Q.G.; D’Ercole, M.; Lauretti, L. Decompressive hemicraniectomy: Dissociation between clinical and radiological findings. Acta Neurol. Belg. 2012, 112, 225–227. [Google Scholar] [CrossRef] [PubMed]
- Chang, V.; Hartzfeld, P.; Langlois, M.; Mahmood, A.; Seyfried, D. Outcomes of cranial repair after craniectomy. J. Neurosurg. 2010, 112, 1120–1124. [Google Scholar] [CrossRef] [PubMed]
- Waziri, A.; Fusco, D.; Mayer, S.A.; McKhann, G.M.I.I.; Connolly, E.S., Jr. Postoperative hydrocephalus in patients undergoing decompressive hemicraniectomy for ischemic or hemorrhagic stroke. Neurosurgery 2007, 61, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Brondani, R.; Garcia de Almeida, A.; Cherubini, P.; Mota, S.M.; de Alencastro, L.C.; Antunes, A.C.M.; Muxfeldt, M.B. High Risk of Seizures and Epilepsy after Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery Stroke. Cerebrovasc. Dis. Extra 2017, 7, 51–61. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| n | Timing of Surgery | Number of Deaths | Mean GCS Scores | p Value | Mean mRS Scores | p Value | |||
|---|---|---|---|---|---|---|---|---|---|
| Preop. | Postop. | Preop. | Postop. | ||||||
| Group 1 | 16 | <24 h | 2 | 8.7 | 14.5 | 0.000 | 4.2 | 2.3 | 0.000 |
| Group 2 | 5 | 24–48 h | 1 | 7.02 | 9 | 0.015 | 4.8 | 4.5 | 0.823 |
| Group 3 | 6 | >48 h | 2 | 11.38 | 12.75 | 0.330 | 5.6 | 5.5 | 0.970 |
| n | GCS Scores | mRS | Deaths | |||||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | p Value | Mean ± SD | p Value | n | p Value | |||
| Age | <60 | 15 | 13.42 ± 1.89 | 0.027 | 2.87 ± 1.88 | 0.033 | 2 | 0.861 |
| ≥60 | 12 | 11.09 ± 1.26 | 3.67 ± 2.27 | 3 | ||||
| Gender | F | 9 | 12.03 ± 2.20 | 0.792 | 2.78 ± 1.86 | 0.421 | 1 | 0.476 |
| M | 18 | 12.96 ± 1.73 | 3.44 ± 1.98 | 4 | ||||
| Hemispheric dominance | Dominant | 13 | 11.79 ± 2.33 | 0.693 | 2.26 ± 1.73 | 0.706 | 3 | 0.538 |
| Nondominant | 14 | 12.36 ± 1.58 | 2.04 ± 2.05 | 2 | ||||
| Infarction side | Left | 10 | 10.49 ± 2.50 | 0.326 | 3.6 ± 2.07 | 0.581 | 3 | 0.675 |
| Right | 17 | 12.18 ± 1.07 | 3 ± 1.87 | 2 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kilic, M.; Ertem, D.H.; Ozdemir, B. Timing of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Single-Center Analysis. Medicina 2019, 55, 31. https://doi.org/10.3390/medicina55020031
Kilic M, Ertem DH, Ozdemir B. Timing of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Single-Center Analysis. Medicina. 2019; 55(2):31. https://doi.org/10.3390/medicina55020031
Chicago/Turabian StyleKilic, Mustafa, Devrimsel Harika Ertem, and Burak Ozdemir. 2019. "Timing of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Single-Center Analysis" Medicina 55, no. 2: 31. https://doi.org/10.3390/medicina55020031
APA StyleKilic, M., Ertem, D. H., & Ozdemir, B. (2019). Timing of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Single-Center Analysis. Medicina, 55(2), 31. https://doi.org/10.3390/medicina55020031