Lower Limb Maneuver Investigation of Chasse Steps Among Male Elite Table Tennis Players




Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Experimental Setup and Data Processing
2.3. Date Recording and Statistics Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zhang, Z. Biomechanical Analysis and Model Development Applied to Table Tennis Forehand Strokes. Ph.D. Thesis, Loughborough University, Loughborough, UK, 2017. [Google Scholar]
- Nikolić, I.; Furjan–Mandić, G.; Kondrič, M. The relationship of morphology and motor abilities to specific table tennis tasks in youngsters. Coll. Antropol. 2014, 38, 241–245. [Google Scholar]
- Yin, Y.; Qu, F. The analysis of plantar biomechanics at the three footwork in table tennis. J. Beijing Sport Univ. 2013, 5, 49–53. [Google Scholar]
- Malagoli Lanzoni, I.; Di Michele, R.; Merni, F. A notational analysis of shot characteristics in top-level table tennis players. Eur. J. Sport Sci. 2014, 14, 309–317. [Google Scholar] [CrossRef]
- Malagoli Lanzoni, I.; Lobietti, R.; Merni, F. Footwork techniques used in table tennis: A qualitative analysis. In Proceedings of the 10th ITTF Sports Science Congress, Zagreb, Croatia, 18–20 May 2007; pp. 401–408. [Google Scholar]
- Fang, Q. Comparisons of foot pressure between teenager girls and young female adults. Phys. Act. Health 2018, 2, 24–28. [Google Scholar] [CrossRef]
- Elliott, B. Biomechanics and tennis. Br. J. Sports Med. 2006, 40, 392–396. [Google Scholar] [CrossRef]
- Qian, J.; Zhang, Y.; Baker, J.S.; Gu, Y. Effects of performance level on lower limb kinematics during table tennis forehand loop. Acta Bioeng. Biomech. 2016, 18, 149. [Google Scholar]
- Girard, O.; Millet, G.P. Neuromuscular fatigue in racquet sports. Phys. Med. Rehabil. Clin. N. Am. 2009, 20, 161–173. [Google Scholar] [CrossRef]
- Elliott, B.K.R. The Art and Science of Tennis; Saunders College Publications: New York, NJ, USA, 1983. [Google Scholar]
- Landlinger, J.; Lindinger, S.; Stoggl, T.; Wagner, H.; Muller, E. Key factors and timing patterns in the tennis forehand of different skill levels. J. Sports Sci Med. 2010, 9, 643–651. [Google Scholar]
- Girard, O.; Micallef, J.P.; Millet, G.P. Lower-limb activity during the power serve in tennis: Effects of performance level. Med. Sci. Sports Exerc. 2005, 37, 1021–1029. [Google Scholar]
- Malagoli Lanzoni, I.; Bartolomei, S.; Di Michele, R.; Fantozzi, S. A kinematic comparison between long-line and cross-court top spin forehand in competitive table tennis players. J. Sports Sci. 2018, 36, 2637–2643. [Google Scholar] [CrossRef]
- Iino, Y.; Kojima, T. Kinematics of table tennis topspin forehands: Effects of performance level and ball spin. J. Sports Sci. 2009, 27, 1311–1321. [Google Scholar] [CrossRef] [PubMed]
- Seeley, M.K.; Funk, M.D.; Denning, W.M.; Hager, R.L.; Hopkins, J.T. Tennis forehand kinematics change as post-impact ball speed is altered. Sports Biomech. 2011, 10, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Iino, Y.; Kojima, T. Torque acting on the pelvis about its superior-inferior axis through the hip joints during a tennis forehand stroke. J. Human Mov. Stud. 2001, 40, 269–290. [Google Scholar]
- Elliott, B.C.; Marshall, R.N.; Noffal, G.J. Contributions of upper limb segment rotations during the power serve in tennis. J. Appl. Biomech. 1995, 11, 433–442. [Google Scholar] [CrossRef]
- Van Gheluwe, B.; Hebbelinck, M. Muscle actions and ground reaction forces in tennis. Int. J. Sport Biomech. 1986, 2, 88–99. [Google Scholar] [CrossRef]
- Hutchinson, M.R.; Laprade, R.F.; Burnett, Q.M.; Moss, R.; Terpstra, J. Injury surveillance at the USTA Boys’ Tennis Championships: A 6-yr study. Med. Sci. Sports Exerc. 1995, 27, 826–831. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B.; Safran, M. Tennis injuries. In Epidemiology of Pediatric Sports Injuries; Karger Publishers: Basel, Switzerland, 2005; Volume 48, pp. 120–137. [Google Scholar]
- Kibler, W.B. Biomechanical analysis of the shoulder during tennis activities. Clin. Sports Med. 1995, 14, 79–85. [Google Scholar] [PubMed]
- Kibler, W.B. Current concepts of shoulder biomechanics for tennis. Tennis Sports Med. Sci. 1995, 14, 59–72. [Google Scholar]
- Lam, W.K.; Fan, J.X.; Zheng, Y.; Lee, W.C.C. Joint and plantar loading in table tennis topspin forehand with different footwork. Eur. J. Sport Sci. 2018, 19, 1–9. [Google Scholar] [CrossRef]
- Shehab, R.; Mirabelli, M.; Gorenflo, D.; Fetters, M.D. Pre-exercise stretching and sports related injuries: Knowledge, attitudes and practices. Clin. J. Sport Med. 2006, 16, 228–231. [Google Scholar] [CrossRef]
- Herman, K.; Barton, C.; Malliaras, P.; Morrissey, D. The effectiveness of neuromuscular warm-up strategies, that require no additional equipment, for preventing lower limb injuries during sports participation: A systematic review. BMC Med. 2012, 10, 75. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.B. Comparison of muscle patterning in the overarm throw and tennis serve. Res. Quart. Am. Alliance Health Phys. Educ. Recreat. Dance 1979, 50, 541–553. [Google Scholar] [CrossRef]
- Miyashita, M.; Tsunoda, T.; Sakurai, S.; Nishizono, H.; Mizuno, T. Muscular activities in the tennis serve and overhand throwing. Scand. J. Sports Sci. 1980, 2, 52–58. [Google Scholar]
- Chow, J.W.; Shim, J.H.; Lim, Y.T. Lower trunk muscle activity during the tennis serve. J. Sci. Med. Sport 2003, 6, 512–518. [Google Scholar] [CrossRef]
- Brody, L.R. On understanding gender differences in the expression of emotion. In Human Feelings: Explorations in Affect Development and Meaning; Ablon, S.L., Brown, D., Khantzian, E.J., Mack, J.E., Eds.; Analytic Press: Hillsdale, NJ, USA, 1993; pp. 87–121. [Google Scholar]
- Zakas, A. Bilateral isokinetic peak torque of quadriceps and hamstring muscles in professional soccer players with dominance on one or both two sides. J. Sports Med. Phys. Fitness 2006, 46, 28. [Google Scholar]
- Peters, M.; Murphy, K. Cluster analysis reveals at least three, and possibly five distinct handedness groups. Neuropsychologia 1992, 30, 373. [Google Scholar] [CrossRef]
- Li, L.; Caldwell, G.E. Muscle coordination in cycling: Effect of surface incline and posture. J. Appl. Physiol. 1998, 85, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Hilsdale NJ, Lawrence Earlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Gentili, R.; Papaxanthis, C.; Pozzo, T. Improvement and generalization of arm motor performance through motor imagery practice. Neuroscience 2006, 137, 761–772. [Google Scholar] [CrossRef]
- Fleisig, G.; Nicholls, R.; Elliott, B.; Escamilla, R. Kinematics used by world class tennis players to produce high-velocity serves. Sports Biomech. 2003, 2, 51–64. [Google Scholar] [CrossRef]
- Komi, P.V.; Bosco, C. Utilization of stored elastic energy in leg extensor muscles by men and women. Med. Sci. Sports 1978, 10, 261–265. [Google Scholar] [PubMed]
- Walshe, A.D.; Wilson, G.J.; Ettema, G.J. Stretch-shorten cycle compared with isometric preload: Contributions to enhanced muscular performance. J. Appl. Physiol. 1998, 84, 97–106. [Google Scholar] [CrossRef]
- Elliott, B.; Fleisig, G.; Nicholls, R.; Escamilia, R. Technique effects on upper limb loading in the tennis serve. J. Sci. Med. Sport 2003, 6, 76–87. [Google Scholar] [CrossRef]
- Fong, D.T.; Ha, S.C.; Mok, K.M.; Chan, C.W.; Chan, K.M. Kinematics analysis of ankle inversion ligamentous sprain injuries in sports: Five cases from televised tennis competitions. Am. J. Sports Med. 2012, 40, 2627–2632. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, K.R.; Brodine, S.K.; Shaffer, R.A.; Johnson, C.W.; Cullison, T.R. The effect of foot structure and range of motion on musculoskeletal overuse injuries. Am. J. Sports Med. 1999, 27, 585–593. [Google Scholar] [CrossRef]
- Beynnon, B.D.; Renström, P.A.; Alosa, D.M.; Baumhauer, J.F.; Vacek, P.M. Ankle ligament injury risk factors: A prospective study of college athletes. J. Orthop. Res. 2001, 19, 213–220. [Google Scholar] [CrossRef]
- Ball, K.A.; Best, R.J. Different centre of pressure patterns within the golf stroke II: Group-based analysis. J. Sports Sci. 2007, 25, 771–779. [Google Scholar] [CrossRef] [PubMed]
- Krivickas, L.S.; Feinberg, J.H. Lower extremity injuries in college athletes: Relation between ligamentous laxity and lower extremity muscle tightness. Arch. Phys. Med. Rehabil. 1996, 77, 1139–1143. [Google Scholar] [CrossRef]
- Zazulak, B.T.; Hewett, T.E.; Reeves, N.P.; Goldberg, B.; Cholewicki, J. The effects of core proprioception on knee injury. Am. J. Sports Med. 2007, 35, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Song, Y. The categories of AFO and its effect on patients with foot impair: A systemic review. Phys. Act. Health 2017, 1, 8–16. [Google Scholar] [CrossRef]
- Kondrič, M.; Matković, B.; Furjan-Mandić, G.; Hadžić, V.; Dervišević, E. Injuries in racket sports among Slovenian players. Coll. Antropol. 2011, 35, 413–417. [Google Scholar] [PubMed]
- Murray, K.J. Hypermobility disorders in children and adolescents. Best Pract. Res. Clin. Rheumatol. 2006, 20, 329–351. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, R.; Von Arx, O.; Azzopardi, T.; Schranz, P.J. The risk of anterior cruciate ligament rupture with generalised joint laxity. Bone Jt. J. 2005, 87, 800–803. [Google Scholar] [CrossRef] [PubMed]
 ,
,  represent the footwork orders for chasse steps.
, represent the footwork orders for chasse steps.
represent the footwork orders for chasse steps.
, represent the footwork orders for chasse steps.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Short or Long Chasse Steps | Mean ± SD | SEM | CI | ES | |
|---|---|---|---|---|---|
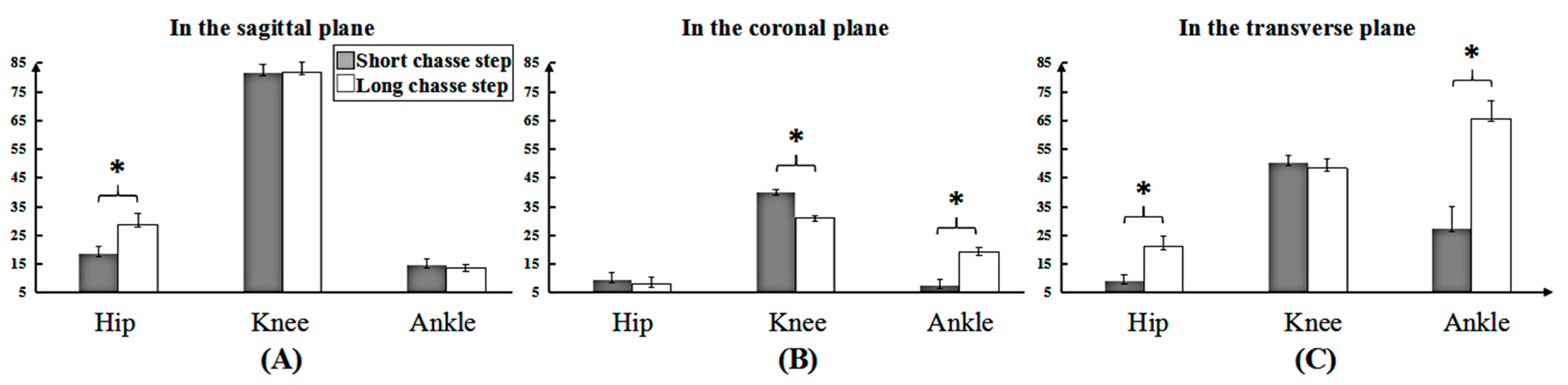
| Hip | |||||
| X | Short | 9.57 ± 1.30 | 0.38 | (8.74, 10.40) | 0.83 |
| Long | 15.11 ± 2.34 * | 0.68 | (13.62, 16.60) | ||
| Y | Short | 4.91± 1.26 | 0.36 | (4.11, 5.71) | 0.31 |
| Long | 4.12 ± 1.17 | 0.34 | (3.38, 4.86) | ||
| Z | Short | 4.70 ± 1.06 | 0.31 | (4.03, 5.38) | 0.91 |
| Long | 11.08 ± 1.82 * | 0.52 | (9.92, 12.23) | ||
| Knee | |||||
| X | Short | 42.23 ± 1.60 | 0.46 | (41.21, 43.24) | 0.20 |
| Long | 42.87 ± 1.60 | 0.46 | (41.85, 43.88) | ||
| Y | Short | 20.70 ± 1.67 | 0.48 | (19.64, 21.77) | 0.83 |
| Long | 16.22 ± 1.27 * | 0.37 | (15.41, 17.03) | ||
| Z | Short | 26.00 ± 1.37 | 0.40 | (25.13, 26.87) | 0.22 |
| Long | 25.39 ± 1.39 | 0.40 | (24.51, 26.27) | ||
| Ankle | |||||
| X | Short | 7.66 ± 1.11 | 0.32 | (6.95, 8.36) | 0.06 |
| Long | 7.10 ± 0.71 | 0.21 | (6.64, 7.55) | ||
| Y | Short | 3.82 ± 1.16 | 0.34 | (3.08, 4.56) | 0.95 |
| Long | 10.00 ± 0.80 * | 0.23 | (9.49, 10.51) | ||
| Z | Short | 14.11 ± 3.83 | 1.12 | (11.68, 16.55) | 0.94 |
| Long | 34.37 ± 3.22 * | 0.93 | (32.32, 36.42) | ||
| Short Chasse Step | Long Chasse Step | ES | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | SEM | CI | Mean ± SD | SEM | CI | ||||
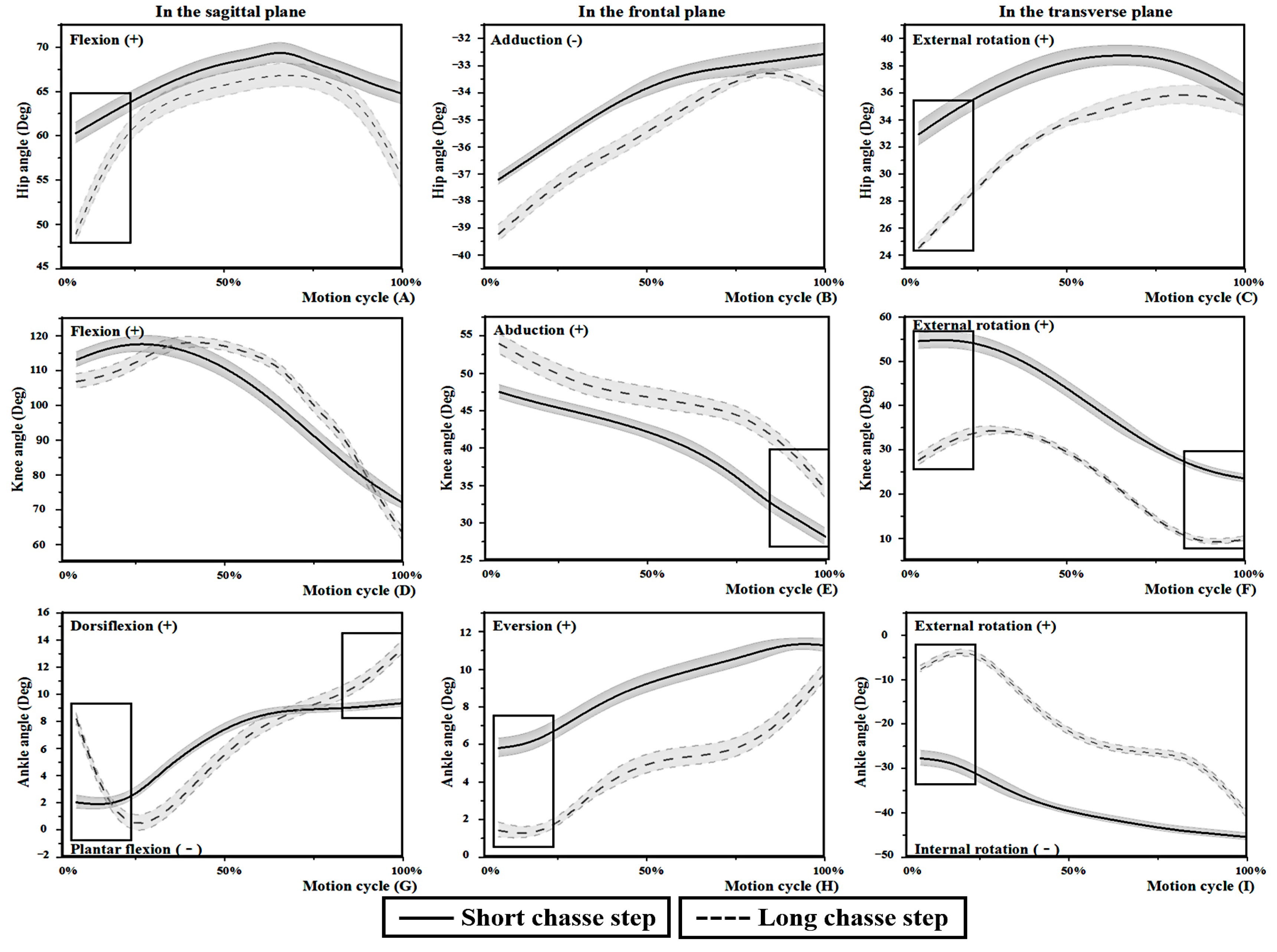
| TI | Hip | X | 60.16 ± 2.42 | 0.70 | (58.62, 61.70) | 48.85 ± 3.22 * | 0.93 | (46.80, 50.89) | 0.89 |
| Y | −37.78 ± 0.94 | 0.27 | (−38.38, −37.18) | −38.30 ± 1.39 | 0.40 | (−39.18, −37.41) | 0.21 | ||
| Z | 33.01 ± 1.57 | 0.45 | (32.02, 34.01) | 24.53 ± 0.36 * | 0.10 | (24.30, 24.76) | 0.97 | ||
| Knee | X | 109.79 ± 3.38 | 0.97 | (107.65, 111.94) | 107.95 ± 1.42 | 0.41 | (107.05, 108.86) | 0.33 | |
| Y | 49.96 ± 2.00 | 0.58 | (48.69, 51.23) | 51.08 ± 2.04 | 0.59 | (49.78, 52.38) | 0.27 | ||
| Z | 54.15 ± 1.75 | 0.51 | (53.04, 55.27) | 29.26 ± 1.77 * | 0.51 | (28.13, 30.39) | 0.99 | ||
| Ankle | X | 2.06 ± 1.31 | 0.38 | (1.23, 2.89) | 8.21 ± 1.07 * | 0.31 | (7.53, 8.89) | 0.93 | |
| Y | 5.81 ± 1.02 | 0.29 | (5.16, 6.46) | 1.48 ± 0.75 * | 0.22 | (1.00, 1.96) | 0.92 | ||
| Z | −27.10 ± 2.43 | 0.70 | (−28.64, −25.56) | −11.72 ± 1.90 * | 0.55 | (−12.92, −10.51) | 0.96 | ||
| BE | Hip | X | 64.45 ± 2.82 | 0.81 | (62.66, 66.24) | 55.14 ± 3.26 * | 0.94 | (53.07, 57.20) | 0.84 |
| Y | −32.86 ± 1.49 | 0.43 | (−33.81, −31.92) | −33.72 ± 2.03 | 0.59 | (−35.01, −32.43) | 0.23 | ||
| Z | 35.33 ± 1.59 | 0.46 | (34.32, 36.34) | 35.60 ± 2.02 | 0.58 | (34.32, 36.88) | 0.07 | ||
| Knee | X | 69.24 ± 1.85 | 0.53 | (68.06, 70.41) | 69.08 ± 2.13 | 0.61 | (67.73, 70.44) | 0.04 | |
| Y | 29.25 ± 1.88 | 0.54 | (28.06, 30.45) | 34.86 ± 1.45 * | 0.42 | (33.94, 35.78) | 0.86 | ||
| Z | 28.77 ± 1.95 | 0.56 | (27.54, 30.00) | 9.86 ± 0.65 * | 0.19 | (9.45, 10.27) | 0.99 | ||
| Ankle | X | 9.72 ± 0.68 | 0.20 | (9.29, 10.15) | 10.39 ± 0.54 * | 0.15 | (10.05, 10.73) | 0.48 | |
| Y | 9.63 ± 0.90 | 0.26 | (9.06, 10.20) | 9.99 ± 0.88 | 0.26 | (9.42, 10.55) | 0.20 | ||
| Z | −41.21 ± 2.42 | 0.70 | (−42.75, −39.67) | −40.59 ± 3.23 | 0.93 | (−42.64, −38.54) | 0.11 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, C.; Shao, S.; Awrejcewicz, J.; Baker, J.S.; Gu, Y. Lower Limb Maneuver Investigation of Chasse Steps Among Male Elite Table Tennis Players. Medicina 2019, 55, 97. https://doi.org/10.3390/medicina55040097
Yu C, Shao S, Awrejcewicz J, Baker JS, Gu Y. Lower Limb Maneuver Investigation of Chasse Steps Among Male Elite Table Tennis Players. Medicina. 2019; 55(4):97. https://doi.org/10.3390/medicina55040097
Chicago/Turabian StyleYu, Changxiao, Shirui Shao, Jan Awrejcewicz, Julien S. Baker, and Yaodong Gu. 2019. "Lower Limb Maneuver Investigation of Chasse Steps Among Male Elite Table Tennis Players" Medicina 55, no. 4: 97. https://doi.org/10.3390/medicina55040097
APA StyleYu, C., Shao, S., Awrejcewicz, J., Baker, J. S., & Gu, Y. (2019). Lower Limb Maneuver Investigation of Chasse Steps Among Male Elite Table Tennis Players. Medicina, 55(4), 97. https://doi.org/10.3390/medicina55040097