Normative Data for Handgrip Strength in Saudi Older Adults Visiting Primary Health Care Centers

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measures
2.4. Statistical Analyses
3. Results
3.1. Participant’s Characteristics
3.2. Results Related to Normative Data
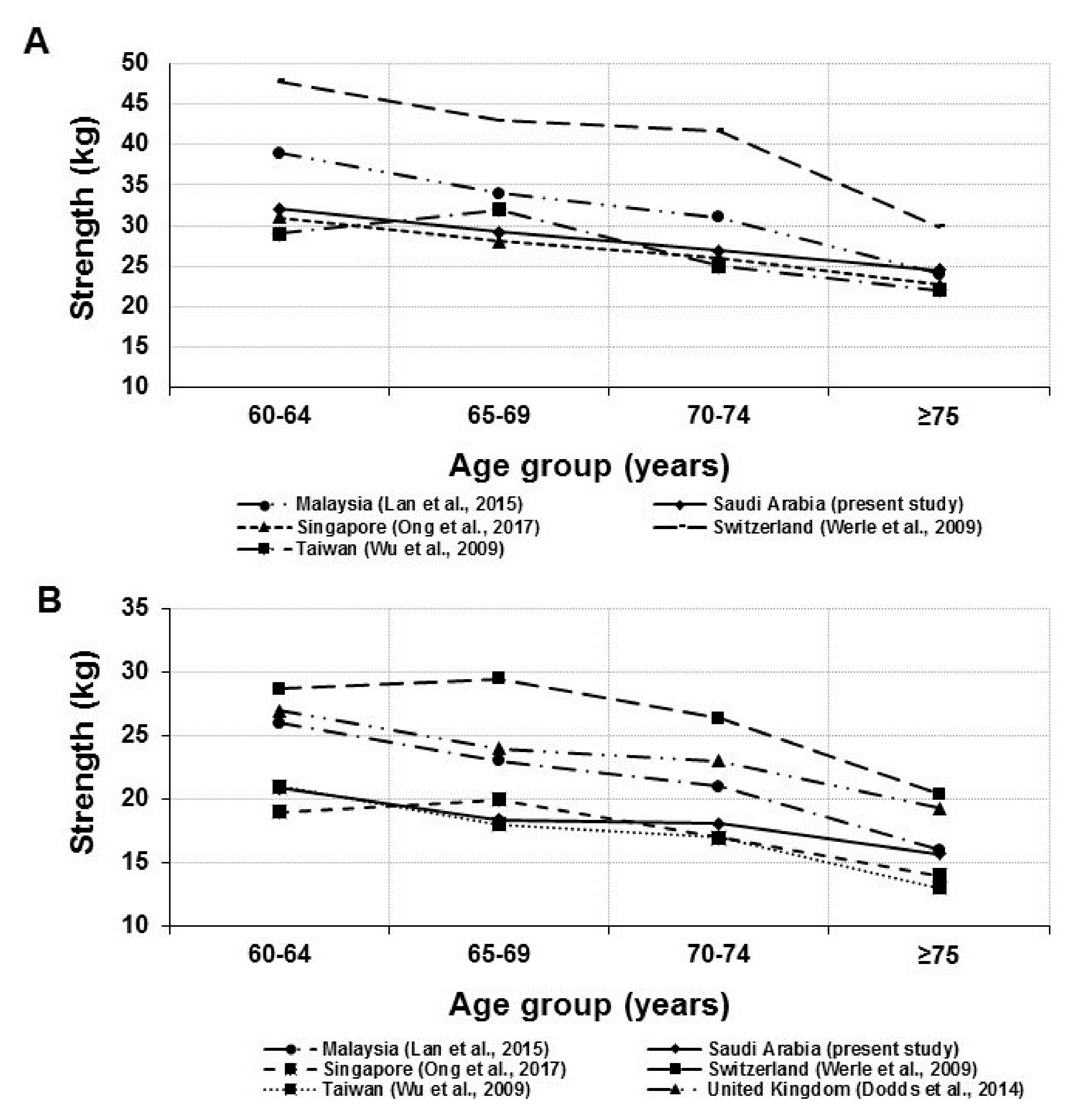
3.3. Comparison between the Present Study and Other Countries Norms
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McGrath, R.P.; Kraemer, W.J.; Al Snih, S.; Peterson, M.D. Handgrip Strength and Health in Aging Adults. Sports Med. 2018, 48, 1993–2000. [Google Scholar] [CrossRef] [PubMed]
- Giampaoli, S.; Ferrucci, L.; Cecchi, F.; Lo Noce, C.; Poce, A.; Dima, F.; Santaquilani, A.; Vescio, M.F.; Menotti, A. Hand-grip strength predicts incident disability in non-disabled older men. Age Ageing 1999, 28, 283–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, H.; Kasagi, F.; Yamada, M.; Fujita, S. Grip strength predicts cause-specific mortality in middle-aged and elderly persons. Am. J. Med. 2007, 120, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Carson, R.G. Get a grip: Individual variations in grip strength are a marker of brain health. Neurobiol. Aging 2018, 71, 189–222. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.C.; Ribeiro, S.M.; Luna, N.M.S.; Peterson, M.D.; Bocalini, D.S.; Serra, M.M.; Brech, G.C.; Greve, J.M.D.; Garcez-Leme, L.E. Association between handgrip strength, balance, and knee flexion/extension strength in older adults. PLoS ONE 2018, 13, e0198185. [Google Scholar] [CrossRef]
- Gale, C.R.; Martyn, C.N.; Cooper, C.; Sayer, A.A. Grip strength, body composition, and mortality. Int. J. Epidemiol. 2006, 36, 228–235. [Google Scholar] [CrossRef] [Green Version]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Benzeval, M.; Deary, I.J.; Dennison, E.M.; Der, G.; Gale, C.R.; Inskip, H.M.; Jagger, C.; et al. Grip strength across the life course: Normative data from twelve British studies. PLoS ONE 2014, 9, e113637. [Google Scholar] [CrossRef]
- Oksuzyan, A.; Singh, P.K.; Christensen, K.; Jasilionis, D. A Cross-National Study of the Gender Gap in Health Among Older Adults in India and China: Similarities and Disparities. Gerontologist 2018, 58, 1156–1165. [Google Scholar] [CrossRef]
- Hossain, M.G.; Zyroul, R.; Pereira, B.P.; Kamarul, T. Multiple regression analysis of factors influencing dominant hand grip strength in an adult Malaysian population. J. Hand Surg. Eur. Vol. 2012, 37, 65–70. [Google Scholar] [CrossRef]
- Bunout, D.; Barrera, G.; De La Maza, T.; Avendano, M.; Gattas, V.; Petermann, M.; Hirsch, S. Lean and fat mass as determinants of muscle strength and insulin sensitivity in Chilean elderly subjects. J. Nutr. Health Aging 2004, 8, 374–378. [Google Scholar] [PubMed]
- Rantanen, T.; Guralnik, J.M.; Leveille, S.; Izmirlian, G.; Hirsch, R.; Simonsick, E.; Ling, S.; Fried, L.P. Racial differences in muscle strength in disabled older women. J. Gerontol. A Biol. Sci. Med. Sci. 1998, 53, B355–B361. [Google Scholar] [CrossRef] [PubMed]
- Haas, S.A.; Krueger, P.M.; Rohlfsen, L. Race/ethnic and nativity disparities in later life physical performance: The role of health and socioeconomic status over the life course. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2012, 67, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Günther, C.M.; Bürger, A.; Rickert, M.; Crispin, A.; Schulz, C.U. Grip strength in healthy caucasian adults: reference values. J. Hand Surg. Am. 2008, 33, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Kuh, D.; Cooper, C.; Sayer, A.A. Global variation in grip strength: A systematic review and meta-analysis of normative data. Age Ageing 2016, 45, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Peolsson, A.; Massy-Westropp, N.; Desrosiers, J.; Bear-Lehman, J. Reference values for adult grip strength measured with a Jamar dynamometer: A descriptive meta-analysis. Physiotherapy 2006, 92, 11–15. [Google Scholar] [CrossRef]
- Bohannon, R.W. Hand-grip dynamometry predicts future outcomes in aging adults. J. Geriatr. Phys. Ther. 2008, 31, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Kutty, V.R.; Lanas, F.; Hui, C.; Quanyong, X.; Zhenzhen, Q.; Jinhua, T.; Noorhassim, I.; et al. Reference ranges of handgrip strength from 125,462 healthy adults in 21 countries: A prospective urban rural epidemiologic (PURE) study. J. Cachexia Sarcopenia Muscle 2016, 7, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Lam, N.W.; Goh, H.T.; Kamaruzzaman, S.B.; Chin, A.-V.; Poi, P.J.H.; Tan, M.P. Normative data for hand grip strength and key pinch strength, stratified by age and gender for a multiethnic Asian population. Singap. Med. J. 2016, 57, 578. [Google Scholar] [CrossRef]
- Wong, S.L. Grip strength reference values for Canadians aged 6 to 79: Canadian Health Measures Survey, 2007 to 2013. Health Rep. 2016, 27, 3. [Google Scholar]
- Bindawas, S.M.; Vennu, V. The National and Regional Prevalence Rates of Disability, Type, of Disability and Severity in Saudi Arabia—Analysis of 2016 Demographic Survey Data. Int. J. Environ. Res. Public Health 2018, 15, 419. [Google Scholar] [CrossRef] [PubMed]
- Karlin, N.J.; Weil, J.; Felmban, W. Aging in Saudi Arabia: An exploratory study of contemporary older persons’ views about daily life, health, and the experience of aging. Gerontol. Geriatr. Med. 2016, 2, 2333721415623911. [Google Scholar] [CrossRef] [PubMed]
- Alahmari, K.A.; Silvian, S.P.; Reddy, R.S.; Kakaraparthi, V.N.; Ahmad, I.; Alam, M.M. Hand grip strength determination for healthy males in Saudi Arabia: A study of the relationship with age, body mass index, hand length and forearm circumference using a hand-held dynamometer. J. Int. Med. Res. 2017, 45, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Omar, M.T.A.; Alghadir, A.; Al Baker, S. Norms for hand grip strength in children aged 6–12 years in Saudi Arabia. Dev. Neurorehabilit. 2015, 18, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Fiebert, I.M.; Roach, K.E.; Armstrong, T.; Mandel, D.W.; Donohue, M. Dynamometric grip strength assessment of subjects sixty years and older. Phys. Occup. Ther. Geriatr. 1996, 13, 27–40. [Google Scholar] [CrossRef]
- Wang, C.-Y.; Chen, L.-Y. Grip strength in older adults: Test-retest reliability and cutoff for subjective weakness of using the hands in heavy tasks. Arch. Phys. Med. Rehabil. 2010, 91, 1747–1751. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.; Shelkey, M. Katz index of independence in activities of daily living (ADL). Urol. Nurs. 2007, 27, 93–94. [Google Scholar]
- Schoene, D.; Wu, S.M.S.; Mikolaizak, A.S.; Menant, J.C.; Smith, S.T.; Delbaere, K.; Lord, S.R. Discriminative ability and predictive validity of the timed Up and Go test in identifying older people who fall: Systematic review and meta-analysis. J. Am. Geriatr. Soc. 2013, 61, 202–208. [Google Scholar] [CrossRef]
- Ong, H.L.; Abdin, E.; Chua, B.Y.; Zhang, Y.; Seow, E.; Vaingankar, J.A.; Chong, S.A.; Subramaniam, M. Hand-grip strength among older adults in Singapore: a comparison with international norms and associative factors. BMC Geriatr. 2017, 17, 176. [Google Scholar] [CrossRef]
- Wu, S.W.; Wu, S.F.; Liang, H.W.; Wu, Z.T.; Huang, S. Measuring factors affecting grip strength in a Taiwan Chinese population and a comparison with consolidated norms. Appl. Ergon. 2009, 40, 811–815. [Google Scholar] [CrossRef]
- Werle, S.; Goldhahn, J.; Drerup, S.; Simmen, B.R.; Sprott, H.; Herren, D. Age-and gender-specific normative data of grip and pinch strength in a healthy adult Swiss population. J. Hand Surg. Eur. Vol. 2009, 34, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Kamarul, T.; Ahmad, T.S.; Loh, W. Hand grip strength in the adult Malaysian population. J. Orthop. Surg. 2006, 14, 172–177. [Google Scholar] [CrossRef] [PubMed]
- McQuiddy, V.A.; Scheerer, C.R.; Lavalley, R.; McGrath, T.; Lin, L. Normative values for grip and pinch strength for 6-to 19-year-olds. Arch. Phys. Med. Rehabil. 2015, 96, 1627–1633. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.H.; Roh, S.Y.; Kim, J.S.; Lee, D.C.; Ki, S.H.; Yang, J.W.; Jeon, M.K.; Lee, S.M. Normative measurements of grip and pinch strengths of 21st century Korean population. Arch. Plast. Surg. 2013, 40, 52. [Google Scholar] [CrossRef] [PubMed]
- Luna-Heredia, E.; Martin-Pena, G.; Ruiz-Galiana, J. Handgrip dynamometry in healthy adults. Clin. Nutr. 2005, 24, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Beumer, A.; Lindau, T.R. Grip strength ratio: A grip strength measurement that correlates well with DASH score in different hand/wrist conditions. BMC Musculoskelet. Disord. 2014, 15, 336. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, R.; Ang, S.; Allen, J.C.; Tan, N.C.; Østbye, T.; Saito, Y.; Chan, A. Normative values of hand grip strength for elderly singaporeans aged 60 to 89 years: A cross-sectional study. J. Am. Med. Dir. Assoc. 2016, 17, e864. [Google Scholar] [CrossRef]
- Fink, B.; Hamdaoui, A.; Wenig, F.; Neave, N. Hand-grip strength and sensation seeking. Pers. Individ. Differ. 2010, 49, 789–793. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Schaubert, K.L. Test–retest reliability of grip-strength measures obtained over a 12-week interval from community-dwelling elders. J. Hand Ther. 2005, 18, 426–428. [Google Scholar] [CrossRef]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar]

{kind=link}
| Characteristics | Men | Women | p-Value |
|---|---|---|---|
| (N = 1138) | (N = 907) | ||
| Age in years | 67.0 ± 6.8 | 65.0 ± 6.5 | p < 0.001 |
| Age group, (%) | |||
| 60–64 years | 529 (46.5) | 559 (61.6) | p < 0.001 |
| 65–69 years | 238 (20.9) | 149 (16.4) | |
| 70–74 years | 201 (17.7) | 114 (12.6) | |
| 75–79 years | 97 (8.5) | 44 (4.9) | |
| 80-84 years | 52 (4.6) | 26 (2.9) | |
| >=85 years | 21 (1.8) | 15 (1.7) | |
| Marital status, (%) | |||
| Married | 1084 (95.3) | 540 (59.5) | p < 0.001 |
| Single | 6 (0.5) | 9 (1.0) | |
| Widow | 45 (4.0) | 304 (33.5) | |
| Divorced | 3 (0.3) | 54 (6.0) | |
| Education levels, (%) | |||
| Illiterate | 224 (19.7) | 522 (57.6) | p < 0.001 |
| Reads and write + Primary | 337 (29.6) | 214 (23.6) | |
| Intermediate + Secondary | 416 (36.6) | 137 (15.1) | |
| University or above | 161 (14.1) | 34 (3.7) | |
| Occupation, (%) | |||
| Employed | 259 (22.8) | 74 (8.2) | p < 0.001 |
| Not Employed | 879 (77.2) | 833 (91.8) | |
| BMI, kg/m2 | 28.5 ± 5.3 | 30.9 ± 5.7 | p < 0.001 |
| Underweight, (%) | 18 (1.6) | 7 (0.8) | |
| Normal, (%) | 251 (22.8) | 102 (12.0) | p < 0.001 |
| Overweight, (%) | 450 (40.9) | 280 (32.8) | |
| Obese, (%) | 380 (34.6) | 464 (54.4) | |
| ADL, (%) | 0.076 | ||
| 0–2 | 19 (1.7) | 16 (1.8) | |
| 3–5 | 115 (10.2) | 121 (13.4) | |
| 6 | 992 (88.1) | 763 (84.8) |
| Characteristics | Men (N = 1138) | Women (N = 907) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Right Hand | Left Hand | Right Hand | Left Hand | ||||||
| Mean ± SD | 95% CI | Mean ± SD | 95% CI | Mean ± SD | 95% CI | Mean ± SD | 95% CI | ||
| 60–64 | N = 1088 | 32.1 ± 7.2 | 31.5–32.6 | 30.5 ± 7.9 | 29.9–31.1 | 20.9 ± 7.4 | 20.2–21.5 | 19.3 ± 7.1 | 18.7–19.9 |
| 65–69 | N = 387 | 29.2 ± 8.4 | 28.0–30.3 | 27.4 ± 7.5 | 26.4–28.4 | 18.4 ± 6.7 | 17.4–19.4 | 16.9 ± 6.6 | 15.9–17.9 |
| 70–74 | N = 315 | 26.9 ± 7.2 | 25.8–27.9 | 25.1 ± 7.1 | 24.0–26.1 | 18.1 ± 7.0 | 16.9–19.2 | 17.0 ± 6.5 | 15.9–18.0 |
| 75–79 | N = 141 | 25.8 ± 6.3 | 24.4–27.2 | 24.8 ± 6.1 | 23.4–26.1 | 17.0 ± 6.9 | 15.2–18.7 | 16.2 ± 6.6 | 14.5–17.8 |
| 80–84 | N = 78 | 22.2 ± 7.4 | 20.0–24.4 | 20.2 ± 6.6 | 18.2–22.1 | 15.7 ± 6.4 | 13.6–17.7 | 15.0 ± 6.6 | 12.9–17.0 |
| >=85 | N = 36 | 25.4 ± 6.5 | 22.5–28.2 | 21.3 ± 5.8 | 18.7–23.8 | 14.4 ± 6.9 | 11.0–17.8 | 12.1 ± 5.4 | 9.4–14.7 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bindawas, S.M.; Vennu, V.; Al-Orf, S.M.; Alshammari, S.A.; Al-Amoud, M.M.; Calder, P.C.; Al-Muammar, M.N.; Alhamdan, A.A. Normative Data for Handgrip Strength in Saudi Older Adults Visiting Primary Health Care Centers. Medicina 2019, 55, 251. https://doi.org/10.3390/medicina55060251
Bindawas SM, Vennu V, Al-Orf SM, Alshammari SA, Al-Amoud MM, Calder PC, Al-Muammar MN, Alhamdan AA. Normative Data for Handgrip Strength in Saudi Older Adults Visiting Primary Health Care Centers. Medicina. 2019; 55(6):251. https://doi.org/10.3390/medicina55060251
Chicago/Turabian StyleBindawas, Saad M., Vishal Vennu, Saada M. Al-Orf, Sulaiman A. Alshammari, Maysoon M. Al-Amoud, Philip C. Calder, May N. Al-Muammar, and Adel A. Alhamdan. 2019. "Normative Data for Handgrip Strength in Saudi Older Adults Visiting Primary Health Care Centers" Medicina 55, no. 6: 251. https://doi.org/10.3390/medicina55060251