Pre-Discharge Predictors of 1-Year Rehospitalization in Adolescents and Young Adults with Severe Mental Disorders: A Retrospective Cohort Study

 ,
,  , , , , , , ,
, , , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection
2.3. Inclusion Criteria
2.4. Outcome and Predictor Variables
2.5. Data Analysis
3. Results
3.1. Study Participants and Sample Characteristics
3.2. Univariate and Multivariable Cox Regression Model
4. Discussion
4.1. Summary and Interpretation of Findings
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Donisi, V.; Tedeschi, F.; Wahlbeck, K.; Haaramo, P.; Amaddeo, F. Pre-discharge factors predicting readmissions of psychiatric patients: A systematic review of the literature. BMC Psychiatry 2016, 6, 449. [Google Scholar] [CrossRef] [PubMed]
- Kalseth, J.; Lassemo, E.; Wahlbeck, K.; Haaramo, P.; Magnussen, J. Psychiatric readmissions and their association with environmental and health system characteristics: A systematic review of the literature. BMC Psychiatry 2016, 16, 376. [Google Scholar] [CrossRef] [PubMed]
- Rumball-Smith, J.; Hider, P. The validity of readmission rate as a marker of the quality of hospital care, and a recommendation for its definition. N. Z. Med. J. 2009, 122, 63–70. [Google Scholar] [PubMed]
- Kessler, R.C.; Angermeyer, M.; Anthony, J.C.; De Graaf, R.; Demyttenaere, K.; Gasquet, I.; De Girolamo, G.; Gluzman, S.; Gureje, O.; Haro, J.M.; et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry 2007, 6, 168–176. [Google Scholar] [PubMed]
- Nakamura, M.M.; Toomey, S.L.; Zaslavsky, A.M.; Berry, J.G.; Lorch, S.A.; Jha, A.K.; Bryant, M.C.; Geanacopoulos, A.T.; Loren, S.S.; Pain, D.; et al. Measuring pediatric hospital readmission rates to drive quality improvement. Acad. Pediatr. 2014, 14, S39–S46. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.S.; Steelesmith, D.L.; Campo, J.V.; Pradhan, T.; Fontanella, C.A. Factors Associated With Multiple Psychiatric Readmissions for Youth with Mood Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 619–631. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, F.; Donisi, V.; Salazzari, D.; Cresswell-Smith, J.; Wahlbeck, K.; Amaddeo, F. Clinical and organizational factors predicting readmission for mental health patients across Italy. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 55, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Fontanella, C.A. The influence of clinical, treatment, and healthcare system characteristics on psychiatric readmission of adolescents. Am. J. Orthopsychiatry 2008, 78, 187–198. [Google Scholar] [CrossRef] [Green Version]
- Madden, A.; Vajda, J.; Llamocca, E.N.; Campo, J.V.; Gorham, T.J.; Lin, S.; Fontanella, C.A. Factors associated with psychiatric readmission of children and adolescents in the U.S.: A systematic review of the literature. Gen. Hosp. Psychiatry 2020, 65, 33–42. [Google Scholar] [CrossRef]
- Miller, D.A.A.; Ronis, S.T.; Slaunwhite, A.K.; Audas, R.; Richard, J.; Tilleczek, K.; Zhang, M. Longitudinal examination of youth readmission to mental health inpatient units. Child Adolesc. Ment. Health 2020, 25, 238–248. [Google Scholar] [CrossRef]
- van Alphen, N.R.; Stewart, J.G.; Esposito, E.C.; Pridgen, B.; Gold, J.; Auerbach, R.P. Predictors of Rehospitalization for Depressed Adolescents Admitted to Acute Psychiatric Treatment. J. Clin. Psychiatry 2017, 78, 592–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edgcomb, J.B.; Sorter, M.; Lorberg, B.; Zima, B.T. Psychiatric Readmission of Children and Adolescents: A Systematic Review and Meta-Analysis. Psychiatr. Serv. 2020, 71, 269–279. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrà, G.; Sciarini, P.; Segagni-Lusignani, G.; Clerici, M.; Montomoli, C.; Kessler, R.C. Do they actually work across borders? Evaluation of two measures of psychological distress as screening instruments in a non Anglo-Saxon country. Eur. Psychiatry 2011, 26, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Carrà, G.; Bartoli, F.; Carretta, D.; Crocamo, C.; Bozzetti, A.; Clerici, M.; Bebbington, P.E. The prevalence of metabolic syndrome in people with severe mental illness: A mediation analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1739–1746. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Bartoli, F.; Crocamo, C.; Dakanalis, A.; Riboldi, I.; Miotto, A.; Brosio, E.; Clerici, M.; Carrà, G. Association between total serum cholesterol and suicide attempts in subjects with major depressive disorder: Exploring the role of clinical and biochemical confounding factors. Clin. Biochem. 2017, 50, 274–278. [Google Scholar] [CrossRef]
- Chowdhury, M.Z.I.; Turin, T.C. Variable selection strategies and its importance in clinical prediction modelling. Fam. Med. Community Health 2020, 8, e000262. [Google Scholar] [CrossRef] [Green Version]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LP: College Station, TX, USA, 2019. [Google Scholar]
- Azuero, A. A note on the magnitude of hazard ratios. Cancer 2016, 122, 1298–1299. [Google Scholar] [CrossRef]
- Mounteney, J.; Griffiths, P.; Sedefov, R.; Noor, A.; Vicente, J.; Simon, R. The drug situation in Europe: An overview of data available on illicit drugs and new psychoactive substances from European monitoring in 2015. Addiction 2016, 111, 34–48. [Google Scholar] [CrossRef]
- Carrà, G.; Bartoli, F.; Brambilla, G.; Crocamo, C.; Clerici, M. Comorbid addiction and major mental illness in Europe: A narrative review. Subst. Abus. 2015, 36, 75–81. [Google Scholar] [CrossRef]
- Colizzi, M.; Burnett, N.; Costa, R.; De Agostini, M.; Griffin, J.; Bhattacharyya, S. Longitudinal assessment of the effect of cannabis use on hospital readmission rates in early psychosis: A 6-year follow-up in an inpatient cohort. Psychiatry Res. 2018, 268, 381–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rezai-Zadeh, K.P.; Engstrom, R.N.; Sharma, A.; Chen, Y.; Chu, J.; Cox, R.P.; Lee, M.T. Generational trends and patterns in readmission within a statewide cohort of clients receiving heroin use disorder treatment in Maryland, 2007–2013. J. Subst. Abus. Treat. 2019, 96, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Böckmann, V.; Lay, B.; Seifritz, E.; Kawohl, W.; Roser, P.; Habermeyer, B. Patient-Level Predictors of Psychiatric Readmission in Substance Use Disorders. Front. Psychiatry 2019, 10, 828. [Google Scholar] [CrossRef] [PubMed]
- Carrà, G.; Johnson, S.; Crocamo, C.; Angermeyer, M.C.; Brugha, T.; Azorin, J.; Toumi, M.; Bebbington, P.E. Psychosocial functioning, quality of life and clinical correlates of comorbid alcohol and drug dependence syndromes in people with schizophrenia across Europe. Psychiatry Res. 2016, 239, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Verdoux, H.; Liraud, F.; Gonzales, B.; Assens, F.; Abalan, F.; van Os, J. Predictors and outcome characteristics associated with suicidal behaviour in early psychosis: A two-year follow-up of first-admitted subjects. Acta Psychiatr. Scand. 2001, 103, 347–354. [Google Scholar] [CrossRef]
- Bartoli, F.; Lev-Ran, S.; Crocamo, C.; Carrà, G. The interplay between cannabis use and suicidal behaviours: Epidemiological overview, psychopathological and clinical models. J. Psychopathol. 2018, 24, 180–186. [Google Scholar]
- Pompili, M.; Serafini, G.; Innamorati, M.; Biondi, M.; Siracusano, A.; Di Giannantonio, M.; Giupponi, G.; Amore, M.; Lester, D.; Girardi, P.; et al. Substance abuse and suicide risk among adolescents. Eur. Arch. Psychiatry Clin. Neurosci. 2012, 262, 469–485. [Google Scholar] [CrossRef]
- Zhang, X.; Wu, L.T. Suicidal ideation and substance use among adolescents and young adults: A bidirectional relation? Drug Alcohol Depend. 2014, 142, 63–73. [Google Scholar] [CrossRef] [Green Version]
- Bartoli, F.; Crocamo, C.; Carrà, G. Cannabis use disorder and suicide attempts in bipolar disorder: A meta-analysis. Neurosci. Biobehav. Rev. 2019, 103, 14–20. [Google Scholar] [CrossRef]
- Hor, K.; Taylor, M. Suicide and schizophrenia: A systematic review of rates and risk factors. J. Psychopharmacol. 2010, 24, 81–90. [Google Scholar] [CrossRef] [Green Version]
- Carrà, G.; Scioli, R.; Monti, M.; Marinoni, A. Severity Profiles of Substance-Abusing Patients in Italian Community Addiction Facilities: Influence of Psychiatric Concurrent Disorders. Eur. Addict. Res. 2006, 12, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Carrà, G.; Bartoli, F.; Crocamo, C.; Brady, K.T.; Clerici, M. Attempted suicide in people with co-occurring bipolar and substance use disorders: Systematic review and meta-analysis. J. Affect. Disord. 2014, 167, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Ostuzzi, G.; Mazzi, M.A.; Terlizzi, S.; Bertolini, F.; Aguglia, A.; Bartoli, F.; Bortolaso, P.; Callegari, C.; Caroleo, M.; Carrà, G.; et al. STAR Network Investigators. Factors associated with first- versus second-generation long-acting antipsychotics prescribed under ordinary clinical practice in Italy. PLoS ONE 2018, 13, e0201371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, L.; Chapman, S.; Syrett, M.; Bowskill, R.; Horne, R. Improving medication adherence in bipolar disorder: A systematic review and meta-analysis of 30 years of intervention trials. J. Affect. Disord. 2016, 194, 202–221. [Google Scholar] [CrossRef]
- Dell’Osso, B.; Albert, U.; Carrà, G.; Pompili, M.; Nanni, M.G.; Pasquini, M.; Poloni, N.; Raballo, A.; Sambataro, F.; Serafini, G.; et al. How to improve adherence to antidepressant treatments in patients with major depression: A psychoeducational consensus checklist. Ann. Gen. Psychiatry 2020, 19, 61. [Google Scholar] [CrossRef]
- Landolt, K.; Rössler, W.; Ajdacic-Gross, V.; Derks, E.M.; Libiger, J.; Kahn, R.S.; Fleischhacker, W.W.; EUFEST Study Group. Predictors of discontinuation of antipsychotic medication and subsequent outcomes in the European First Episode Schizophrenia Trial (EUFEST). Schizophr. Res. 2016, 172, 145–151. [Google Scholar] [CrossRef]
- WHO Collaborating Centre for Drug Statistic Methodology. Guidelines for ATC Classification and DDD Assignment; WHO Collaborating Centre for Drug Statistic Methodology ed.: Oslo, Norway, 2003. [Google Scholar]
- Gavrielov-Yusim, N.; Friger, M. Use of administrative medical databases in population-based research. J. Epidemiol. Community Health 2014, 68, 283–287. [Google Scholar] [CrossRef]
- Ruggeri, M.; Lora, A.; Semisa, D.; SIEP-DIRECT’S Group. The SIEP-DIRECT’S Project on the discrepancy between routine practice and evidence. An outline of main findings and practical implications for the future of community based mental health services. Epidemiol. Psichiatr. Soc. 2008, 17, 358–368. [Google Scholar] [CrossRef]
- Carrà, G.; Crocamo, C.; Borrelli, P.; Tabacchi, T.I.; Bartoli, F.; Popa, I.; Montomoli, C.; Clerici, M. Area-Level Deprivation and Adverse Consequences in People With Substance Use Disorders: Findings From the Psychiatric and Addictive Dual Disorder in Italy (PADDI) Study. Subst. Use Misuse 2017, 52, 451–458. [Google Scholar] [CrossRef]
- Turecki, G.; Brent, D.A. Suicide and suicidal behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Carrà, G.; Crocamo, C.; Borrelli, P.; Popa, I.; Ornaghi, A.; Montomoli, C.; Clerici, M. Correlates of dependence and treatment for substance use among people with comorbid severe mental and substance use disorders: Findings from the “Psychiatric and Addictive Dual Disorder in Italy (PADDI)” Study. Compr. Psychiatry 2015, 58, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Calear, A.L.; Christensen, H.; Freeman, A.; Fenton, K.; Busby Grant, J.; van Spijker, B.; Donker, T. A systematic review of psychosocial suicide prevention interventions for youth. Eur. Child Adolesc. Psychiatry 2016, 25, 467–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, S.P.; Tuomainen, H. Transition from child to adult mental health services: Needs, barriers, experiences and new models of care. World Psychiatry 2015, 14, 358–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molfenter, T.; Connor, T.; Ford, J.H.; Hyatt, J.; Zimmerman, D. Reducing psychiatric inpatient readmissions using an organizational change model. WMJ 2016, 115, 122–128. [Google Scholar]

{kind=link}
| Characteristics | Total Sample (n = 125) | Readmitted Within 1 Year (n = 36) | Not Readmitted (n = 89) | p-Value * |
|---|---|---|---|---|
| Age at study entry, years | 0.727 | |||
| Mean (SD) | 20.6 (2.9) | 20.7 (3.3) | 20.6 (2.7) | |
| Median (IQR) | 20.3 (18.4 to 22.8) | 20.8 (17.9 to 23.6) | 20.3 (18.5 to 22.6) | |
| Male gender | 67 (53.6%) | 20 (55.6%) | 47 (52.8%) | 0.911 |
| Diagnosis | 0.684 | |||
| Schizophrenia spectrum or other psychotic disorder | 44 (35.2%) | 15 (41.7%) | 29 (32.6%) | |
| Bipolar disorder | 8 (6.4%) | 2 (5.6%) | 6 (6.7%) | |
| Major depressive disorder | 13 (10.4%) | 2 (5.6%) | 11 (12.4%) | |
| Personality disorder | 60 (48.0%) | 17 (47.2%) | 43 (48.3%) | |
| Alcohol use disorders | 17 (13.6%) | 7 (19.4%) | 10 (11.2%) | 0.170 |
| Substance use disorders | 45 (36.0%) | 17 (47.2%) | 28 (31.5%) | 0.081 |
| Admission for a suicide attempt | 20 (16.0%) | 9 (25.0%) | 11 (12.4%) | 0.078 |
| Previous contacts with mental health services | 86 (68.8%) | 28 (77.8%) | 58 (65.2%) | 0.201 |
| Previous hospitalizations | 0.130 | |||
| None | 95 (76.0%) | 24 (66.7%) | 71 (79.8%) | |
| At least one | 30 (24.0%) | 12 (33.3%) | 18 (20.2%) | |
| Compulsory hospitalization | 26 (20.8%) | 6 (16.7%) | 20 (22.5%) | 0.422 |
| Length of hospital stay, days | 0.504 | |||
| Mean (SD) | 16.7 (21.4) | 14.8 (9.7) | 17.5 (24.6) | |
| Median (IQR) | 11 (8–17) | 12.5 (9–17) | 10 (7–16) | |
| Psychopharmacological treatment | ||||
| Antipsychotics | 91 (72.8%) | 29 (80.6%) | 62 (69.7%) | 0.311 |
| LAIs § | 17 (13.6%) | 8 (22.2%) | 9 (10.1%) | 0.152 § |
| Mood stabilizers | 27 (21.6%) | 8 (22.2%) | 19 (21.3%) | 0.920 |
| Antidepressants | 32 (25.6%) | 10 (27.8%) | 22 (24.7%) | 0.687 |
| Type of discharge planning and referrals | 0.626 | |||
| Home | 112 (89.6%) | 33 (91.7%) | 79 (88.8%) | |
| Residential facilities | 13 (10.6%) | 3 (8.3%) | 10 (11.2%) |
| Characteristics | HR | 95% CI | p-Value |
|---|---|---|---|
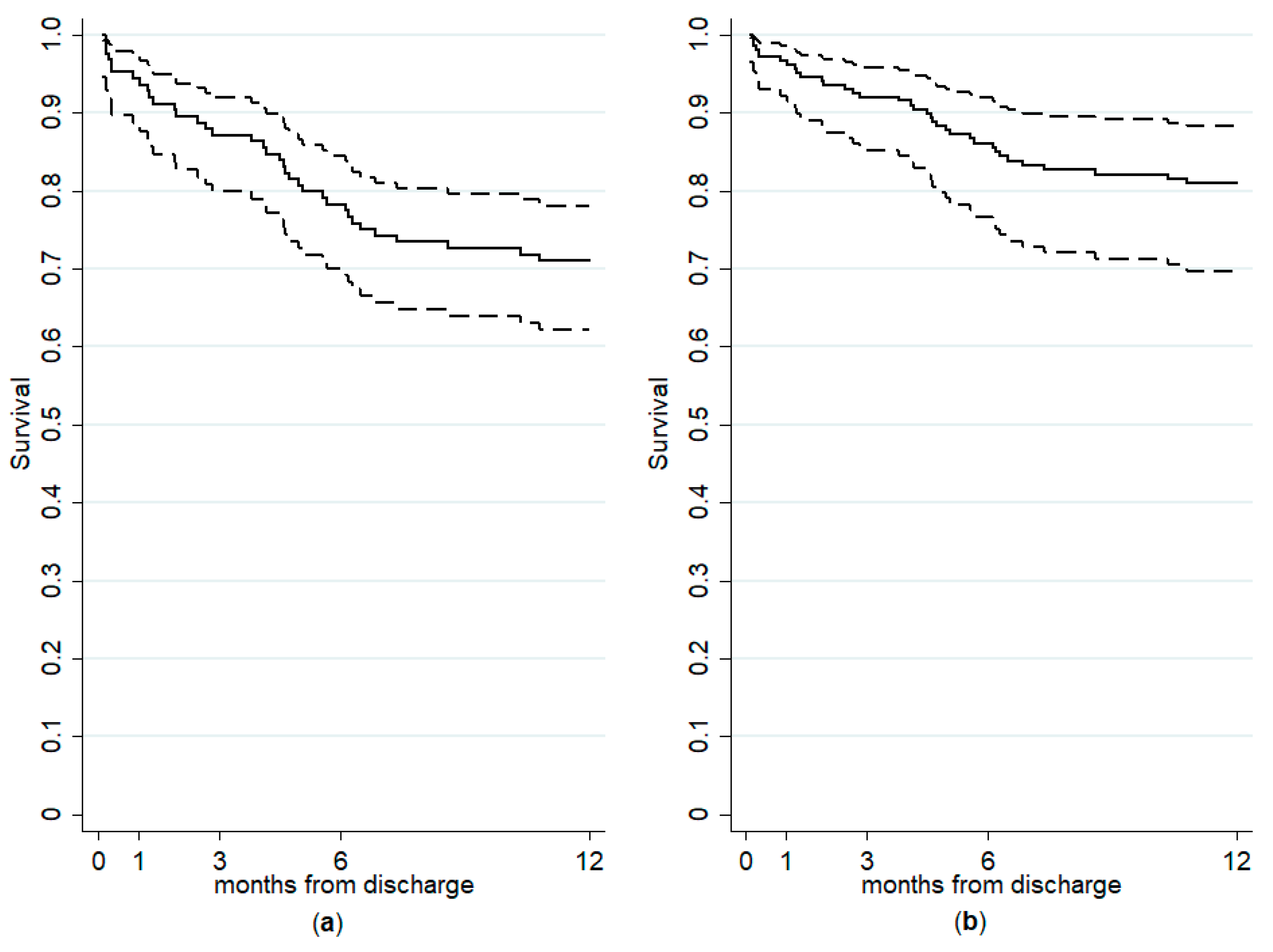
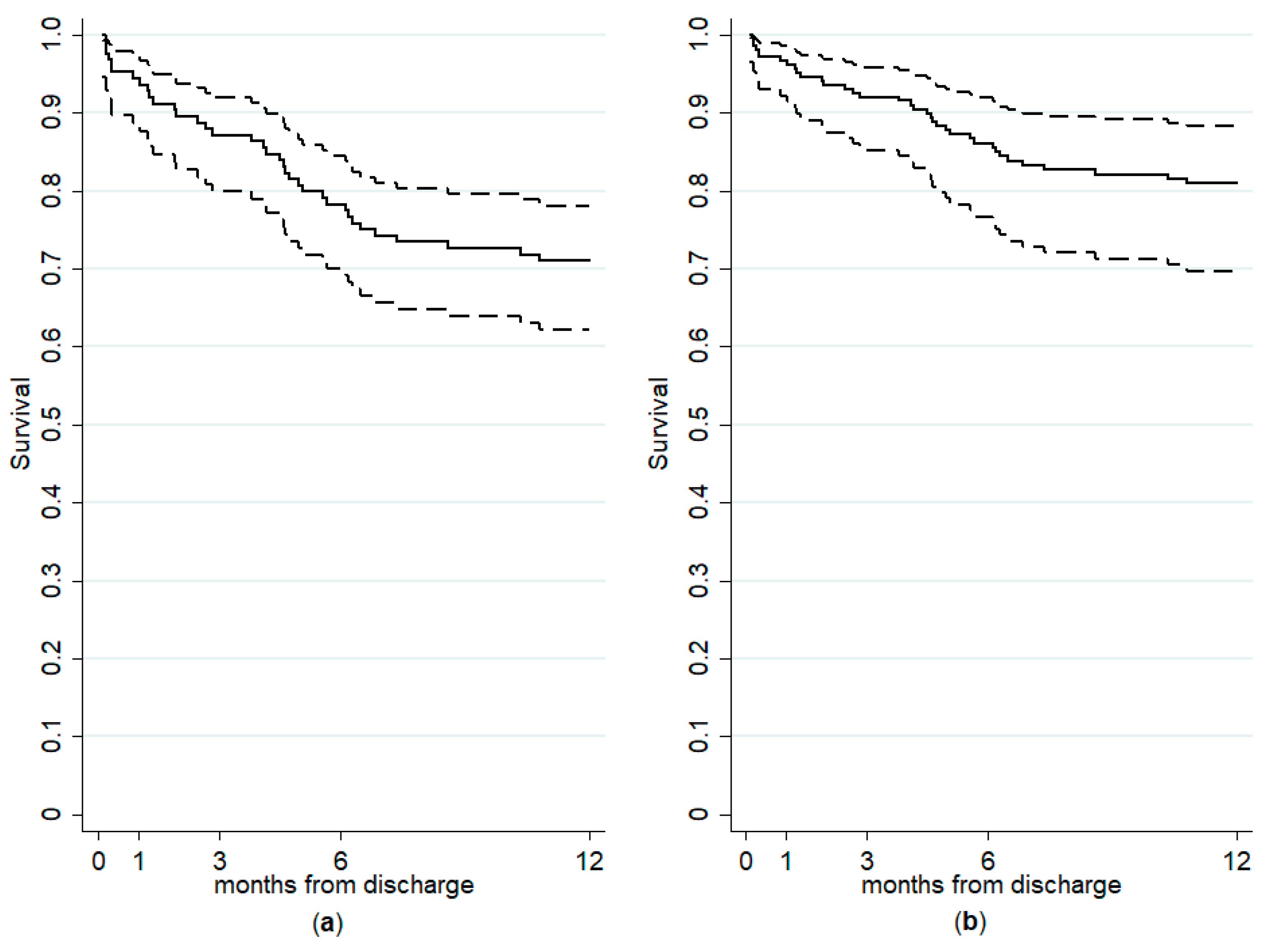
| Admission for a suicide attempt | 2.49 | 1.13 to 5.49 | 0.024 |
| Substance use disorders | 2.14 | 1.08 to 4.26 | 0.029 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartoli, F.; Cavaleri, D.; Moretti, F.; Bachi, B.; Calabrese, A.; Callovini, T.; Cioni, R.M.; Riboldi, I.; Nacinovich, R.; Crocamo, C.; et al. Pre-Discharge Predictors of 1-Year Rehospitalization in Adolescents and Young Adults with Severe Mental Disorders: A Retrospective Cohort Study. Medicina 2020, 56, 613. https://doi.org/10.3390/medicina56110613
Bartoli F, Cavaleri D, Moretti F, Bachi B, Calabrese A, Callovini T, Cioni RM, Riboldi I, Nacinovich R, Crocamo C, et al. Pre-Discharge Predictors of 1-Year Rehospitalization in Adolescents and Young Adults with Severe Mental Disorders: A Retrospective Cohort Study. Medicina. 2020; 56(11):613. https://doi.org/10.3390/medicina56110613
Chicago/Turabian StyleBartoli, Francesco, Daniele Cavaleri, Federico Moretti, Bianca Bachi, Angela Calabrese, Tommaso Callovini, Riccardo M. Cioni, Ilaria Riboldi, Renata Nacinovich, Cristina Crocamo, and et al. 2020. "Pre-Discharge Predictors of 1-Year Rehospitalization in Adolescents and Young Adults with Severe Mental Disorders: A Retrospective Cohort Study" Medicina 56, no. 11: 613. https://doi.org/10.3390/medicina56110613
APA StyleBartoli, F., Cavaleri, D., Moretti, F., Bachi, B., Calabrese, A., Callovini, T., Cioni, R. M., Riboldi, I., Nacinovich, R., Crocamo, C., & Carrà, G. (2020). Pre-Discharge Predictors of 1-Year Rehospitalization in Adolescents and Young Adults with Severe Mental Disorders: A Retrospective Cohort Study. Medicina, 56(11), 613. https://doi.org/10.3390/medicina56110613