Relationship between Maximum Tongue Pressure Value and Age, Occlusal Status, or Body Mass Index among the Community-Dwelling Elderly

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Ethical Approval
2.2. Examination Measures
2.3. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. The MTP Value in Each Age Group
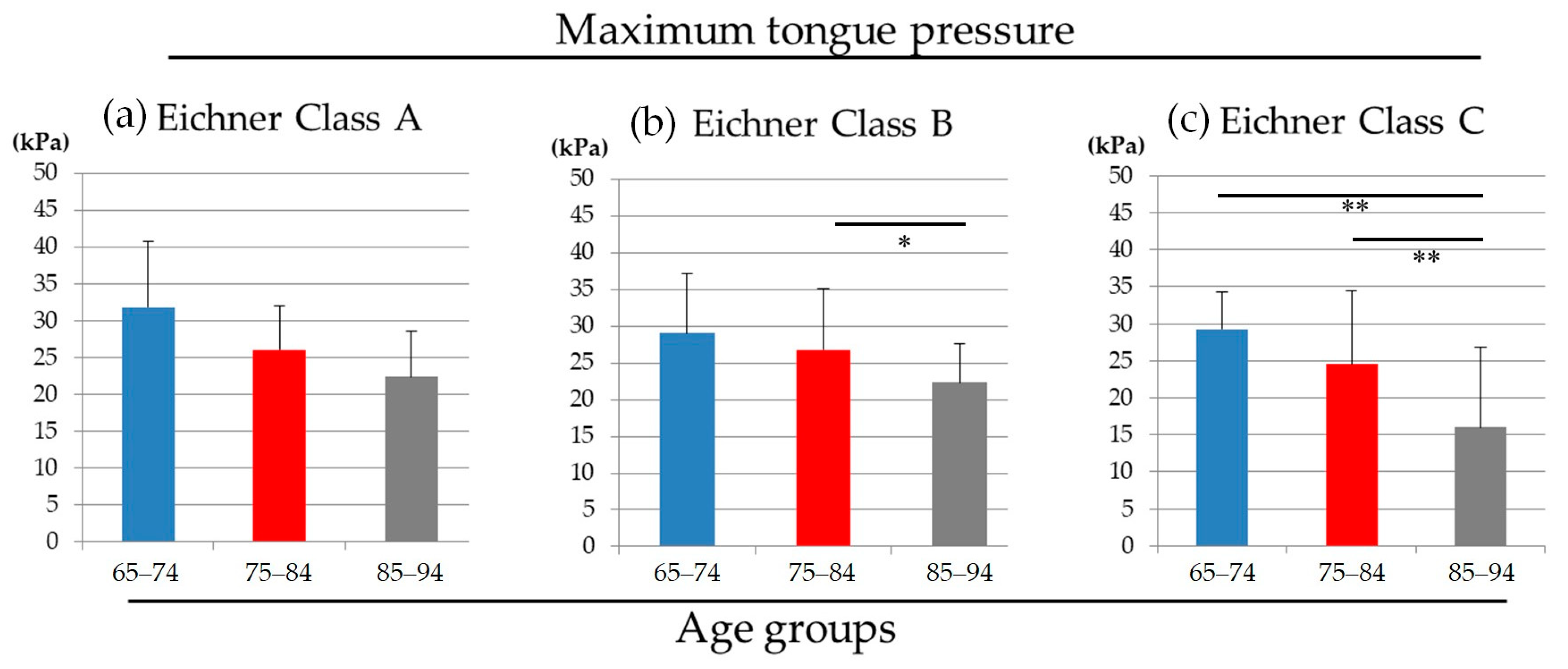
3.3. The Difference of MTP Value among Age Groups within Each Occlusal Status (Eichner Classification)
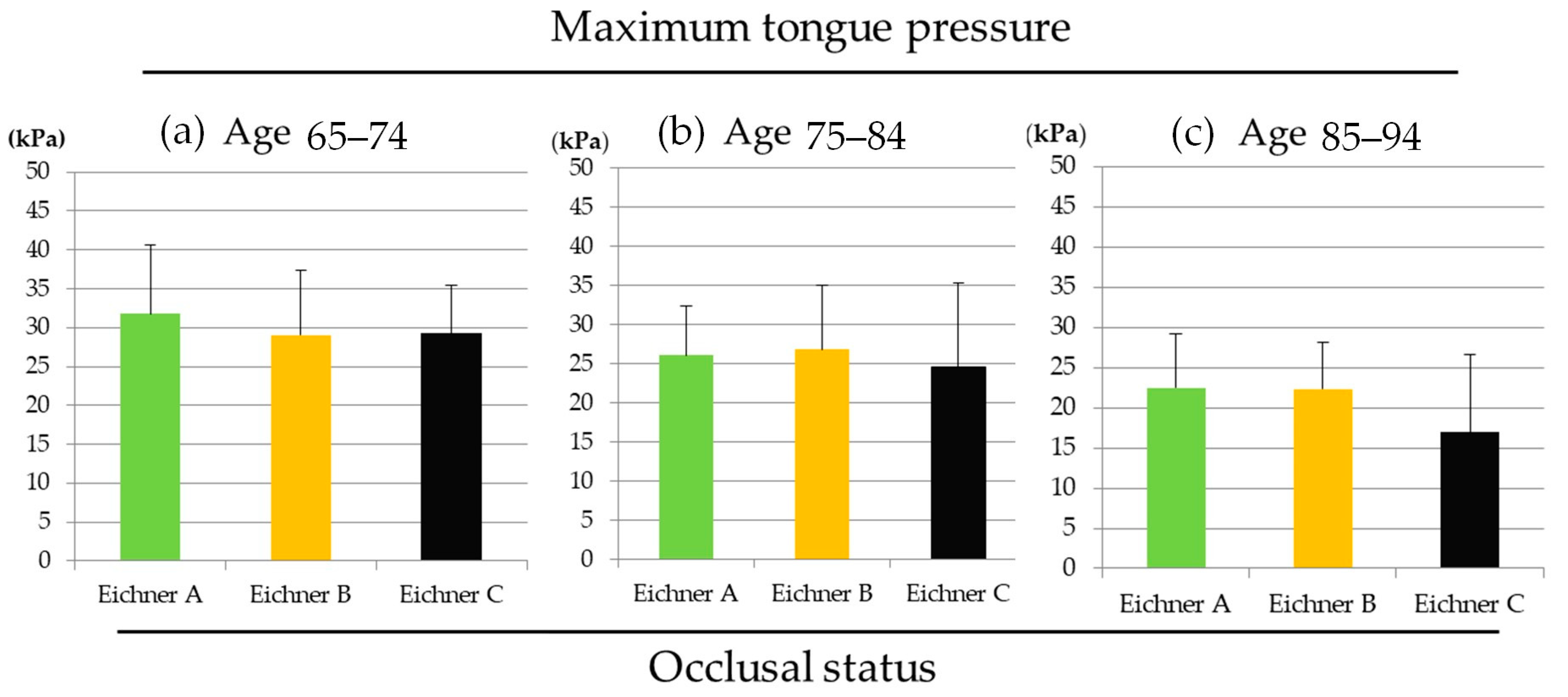
3.4. The Difference of MTP Value among Occlusal Status within Each Age Group
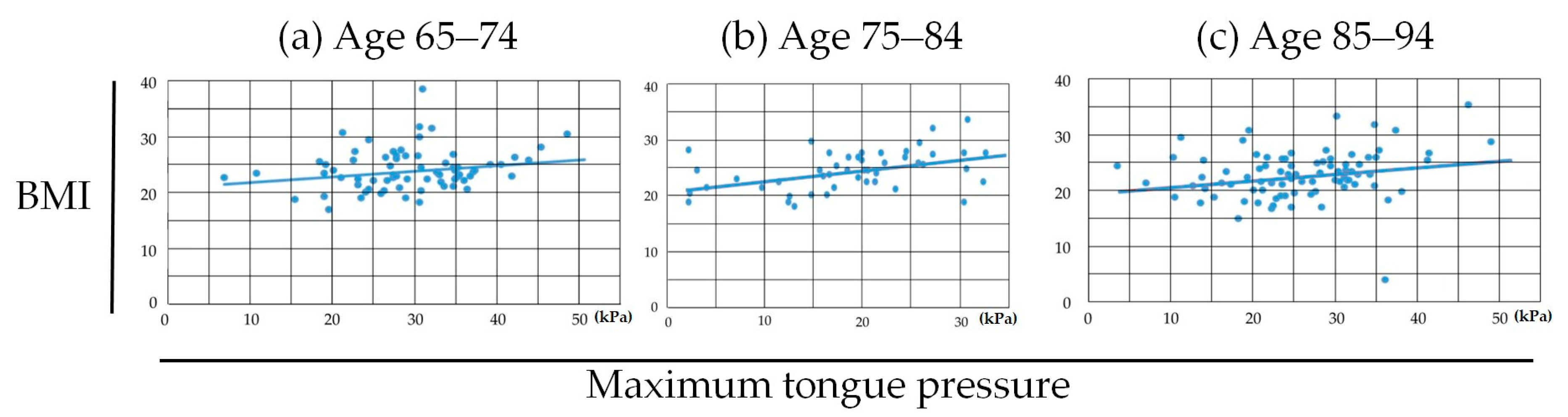
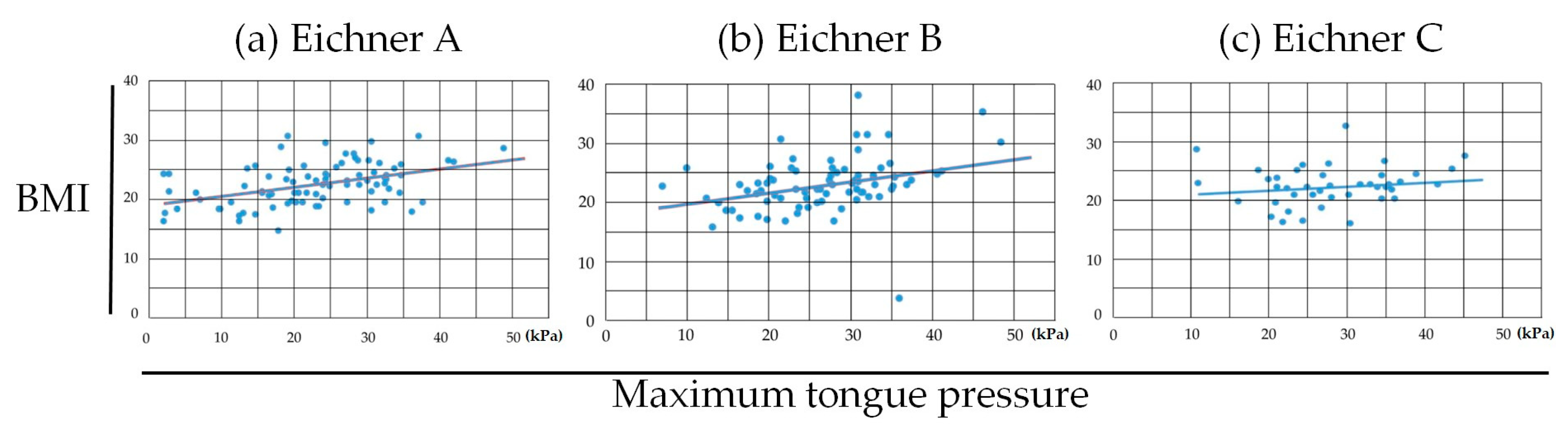
3.5. Correlation Coefficients between MTP and BMI within Each Age Group and MTP and BMI within Each Occlusal Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Iwasa, H.; Masui, Y.; Gondo, Y.; Yoshida, Y.; Inagaki, H.; Kawaai, C.; Kim, H.; Yoshida, H.; Suzuki, T. Personality and participation in mass health checkups among Japanese community-dwelling elderly. J. Psychosom. Res. 2009, 66, 155–159. [Google Scholar] [CrossRef]
- Fukutomi, E.; Kimura, Y.; Wada, T.; Okumiya, K.; Matsubayashi, K. Long-term care prevention project in Japan. Lancet 2013, 381, 116. [Google Scholar] [CrossRef]
- Yoshida, M.; Kikutani, T.; Tsuga, K.; Utanohara, Y.; Hayashi, R.; Akagawa, Y. Decreased tongue pressure reflects symptom of dysphagia. Dysphagia 2006, 21, 61–65. [Google Scholar] [CrossRef]
- Maeda, K.; Akagi, J. Decreased tongue pressure is associated with sarcopenia and sarcopenic dysphagia in the elderly. Dysphagia 2015, 30, 80–87. [Google Scholar] [CrossRef]
- Tsuga, K.; Yoshikawa, M.; Oue, H.; Okazaki, Y.; Tsuchioka, H.; Maruyama, M.; Yoshida, M.; Akagawa, Y. Maximal voluntary tongue pressure is decreased in Japanese frail elderly persons. Gerodontology 2012, 29, e1078–e1085. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tetsuo, T.; Akishita, M.; Iijima, K. Oral Frailty as a Risk Factor for Physical Frailty and Mortality in Community-Dwelling Elderly. J. Gerontol. Ser. A 2018, 73, 1661–1667. [Google Scholar] [CrossRef] [PubMed]
- Hirai, T.; Tanaka, O.; Koshino, H.; Yajima, T. Ultrasound observations of tongue motor behavior. J. Prosthet. Dent. 1991, 65, 840–844. [Google Scholar] [CrossRef]
- Shawker, T.H.; Sonies, B.C.; Stone, M. Soft tissue anatomy of the tongue and floor of the mouth: An ultrasound demonstration. Brain Lang. 1984, 21, 335–350. [Google Scholar] [CrossRef]
- Sonies, B.C.; Baum, B.J.; Shawker, T.H. Tongue motion in elderly adults: Initial in situ observations. J. Gerontol. 1984, 39, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Sonies, B.C.; Parent, L.J.; Morrish, K.; Baum, B.J. Durational aspects of the oral-pharyngeal phase of swallow in normal adults. Dysphagia 1988, 3, 1–10. [Google Scholar] [CrossRef]
- Tracy, J.F.; Logemann, J.A.; Kahrilas, P.J.; Jacob, P.; Kobara, M.; Krugler, C. Preliminary observations on the effects of age on oropharyngeal deglutition. Dysphagia 1989, 4, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, R.; Tsuga, K.; Hosokawa, R.; Yoshida, M.; Sato, Y.; Akagawa, Y. A novel handy probe for tongue pressure measurement. Int. J. Prosthodont. 2002, 15, 385–388. [Google Scholar] [PubMed]
- Utanohara, Y.; Hayashi, R.; Yoshikawa, M.; Yoshida, M.; Tsuga, K.; Akagawa, Y. Standard values of maximum tongue pressure taken using newly developed disposable tongue pressure measurement device. Dysphagia 2008, 23, 286–290. [Google Scholar] [CrossRef]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Morita, K.; Tsuka, H.; Kato, K.; Mori, T.; Nishimura, R.; Yoshida, M.; Tsuga, K. Factors related to masticatory performance in healthy elderly individuals. J. Prosthodont. Res. 2018, 62, 432–435. [Google Scholar] [CrossRef]
- Hori, K.; Ono, T.; Nokubi, T. Coordination of Tongue Pressure and Jaw Movement in Mastication. J. Dent. Res. 2016, 85, 187–191. [Google Scholar] [CrossRef]
- Eichner, K. Über eine gruppeneinteilung der lückengebisse für die prothetik. Dtsch. Zahnärztliche Z. 1955, 10, 1331–1834. [Google Scholar]
- Hiraoka, A.; Yoshikawa, M.; Nakamori, M.; Hosomi, N.; Nagasaki, T.; Mori, T.; Oda, M.; Maruyama, H.; Yoshida, M.; Izumi, Y.; et al. Maximum Tongue Pressure is Associated with Swallowing Dysfunction in ALS Patients. Dysphagia 2017, 32, 542–547. [Google Scholar] [CrossRef]
- Crow, H.C.; Ship, J.A. Tongue strength and endurance in different aged individuals. J. Gerontol. A Biol. Sci. Med. Sci. 1996, 51, M247–M250. [Google Scholar] [CrossRef]
- Todd, J.T.; Lintzenich, C.R.; Butler, S.G. Isometric and swallowing tongue strength in healthy adults. Laryngoscope 2013, 123, 2469–2473. [Google Scholar] [CrossRef]
- Yoshikawa, M.; Yoshida, M.; Tsuga, K.; Akagawa, Y.; Groher, M.E. Comparison of three types of tongue pressure measurement devices. Dysphagia 2011, 26, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Yamanashi, H.; Shimizu, Y.; Higashi, M.; Koyamatsu, J.; Sato, S.; Nagayoshi, M.; Kadota, K.; Kawashiri, S.; Tamai, M.; Takamura, N.; et al. Validity of maximum isometric tongue pressure as a screening test for physical frailty: Cross-sectional study of Japanese community-dwelling older adults. Geriatr. Gerontol. Int. 2018, 18, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Ohno, K.; Fujita, Y.; Ohno, Y.; Takeshima, T.; Maki, K. The factors related to decreases in masticatory performance and masticatory function until swallowing using gummy jelly in subjects aged 20–79 years. J. Oral Rehabil. 2020, 47, 851–886. [Google Scholar] [CrossRef] [PubMed]
- Hara, K.; Tohara, H.; Kenichiro, K.; Yamaguchi, K.; Ariya, C.; Yoshimi, K.; Nakane, A.; Minakuchi, S. Association between tongue muscle strength and masticatory muscle strength. J. Oral Rehabil. 2019, 46, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, K.; Ikeuchi, T.; Shinkai, S.; Hirano, H.; Ryu, M.; Tamaki, K.; Yatani, H.; Kuboki, T.; Kusatsu ISLE Study Working Group Collaborators; Kimura-Ono, A.; et al. Number of functional teeth more strongly predicts all-cause mortality than number of present teeth in Japanese older adults. Geriatr. Gerontol. Int. 2020, 20, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, Y.; Aida, J.; Takeuchi, K.; Tsakos, G.; Watt, R.G.; Kondo, K.; Osaka, K. Inequalities of dental prosthesis use under universal healthcare insurance. Community Dent. Oral Epidemiol. 2014, 42, 122–128. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years Old) | n | Eichner Classification | n |
|---|---|---|---|
| 65–74 | 74 | A | 42 |
| 75–84 | 84 | B | 78 |
| 85–94 | 47 | C | 85 |
| Total | 205 | Total | 205 |
| Average ± SD | |
|---|---|
| Age | 78.00 ± 7.64 |
| BMI | 22.42 ± 4.00 |
| The number of remaining teeth | 16.11 ± 9.31 |
| MTP (kPa) | 25.67 ± 9.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, H.; Ayukawa, Y.; Ueno, Y.; Atsuta, I.; Jinnouchi, A.; Koyano, K. Relationship between Maximum Tongue Pressure Value and Age, Occlusal Status, or Body Mass Index among the Community-Dwelling Elderly. Medicina 2020, 56, 623. https://doi.org/10.3390/medicina56110623
Suzuki H, Ayukawa Y, Ueno Y, Atsuta I, Jinnouchi A, Koyano K. Relationship between Maximum Tongue Pressure Value and Age, Occlusal Status, or Body Mass Index among the Community-Dwelling Elderly. Medicina. 2020; 56(11):623. https://doi.org/10.3390/medicina56110623
Chicago/Turabian StyleSuzuki, Hiroki, Yasunori Ayukawa, Yoko Ueno, Ikiru Atsuta, Akio Jinnouchi, and Kiyoshi Koyano. 2020. "Relationship between Maximum Tongue Pressure Value and Age, Occlusal Status, or Body Mass Index among the Community-Dwelling Elderly" Medicina 56, no. 11: 623. https://doi.org/10.3390/medicina56110623
APA StyleSuzuki, H., Ayukawa, Y., Ueno, Y., Atsuta, I., Jinnouchi, A., & Koyano, K. (2020). Relationship between Maximum Tongue Pressure Value and Age, Occlusal Status, or Body Mass Index among the Community-Dwelling Elderly. Medicina, 56(11), 623. https://doi.org/10.3390/medicina56110623