Influence of Different Repair Acrylic Resin and Thermocycling on the Flexural Strength of Denture Base Resin


Abstract
:1. Introduction
2. Materials and Methods
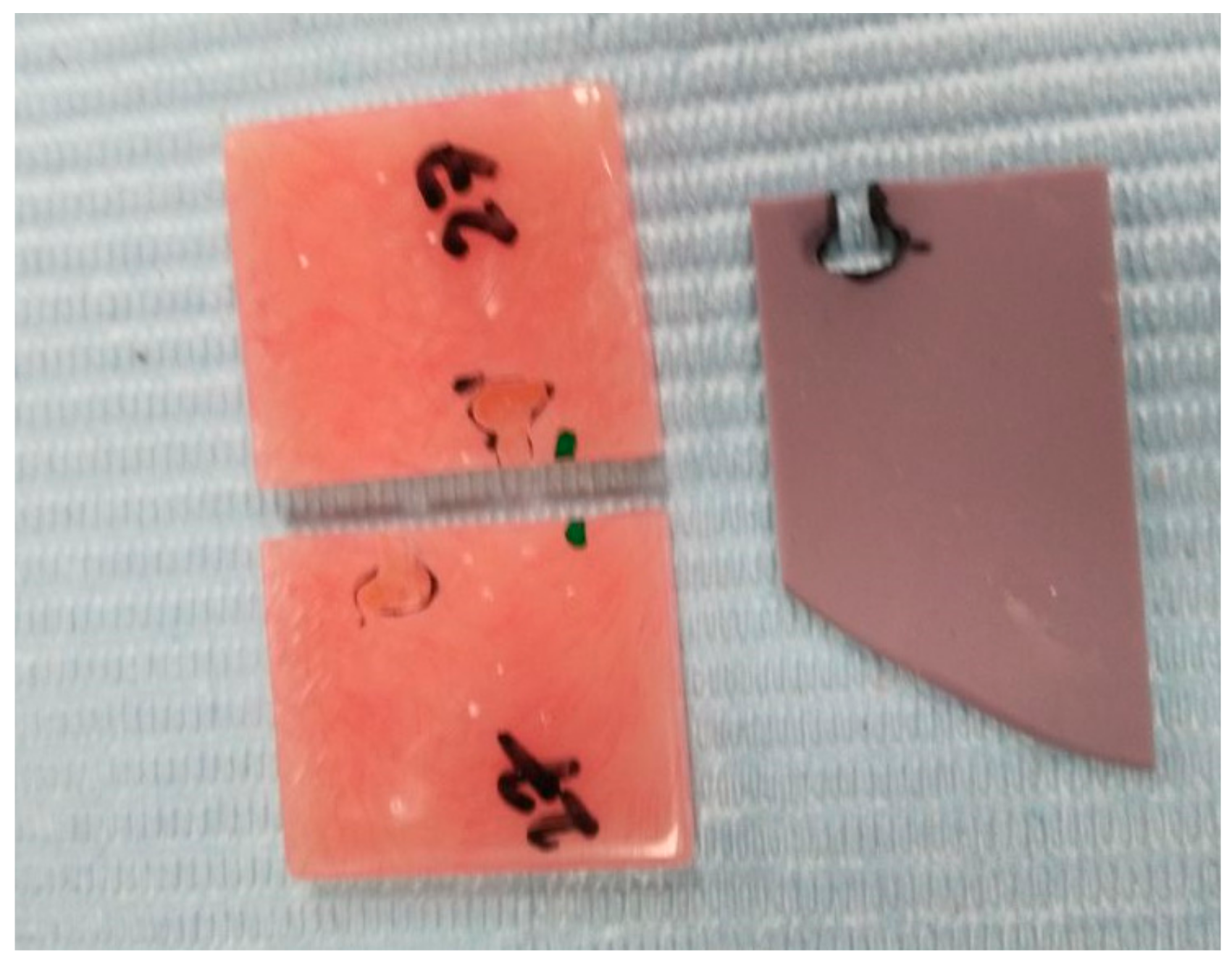
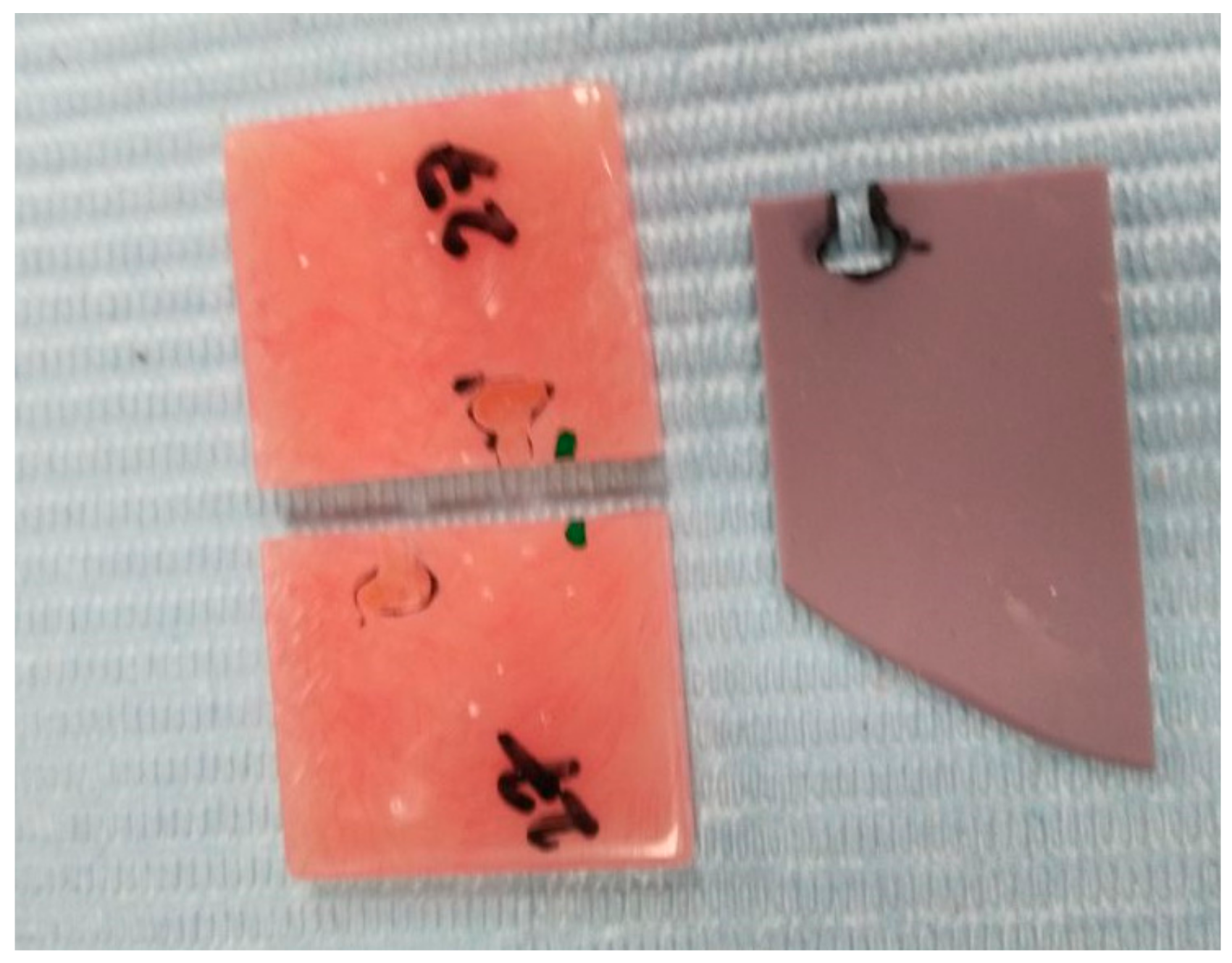
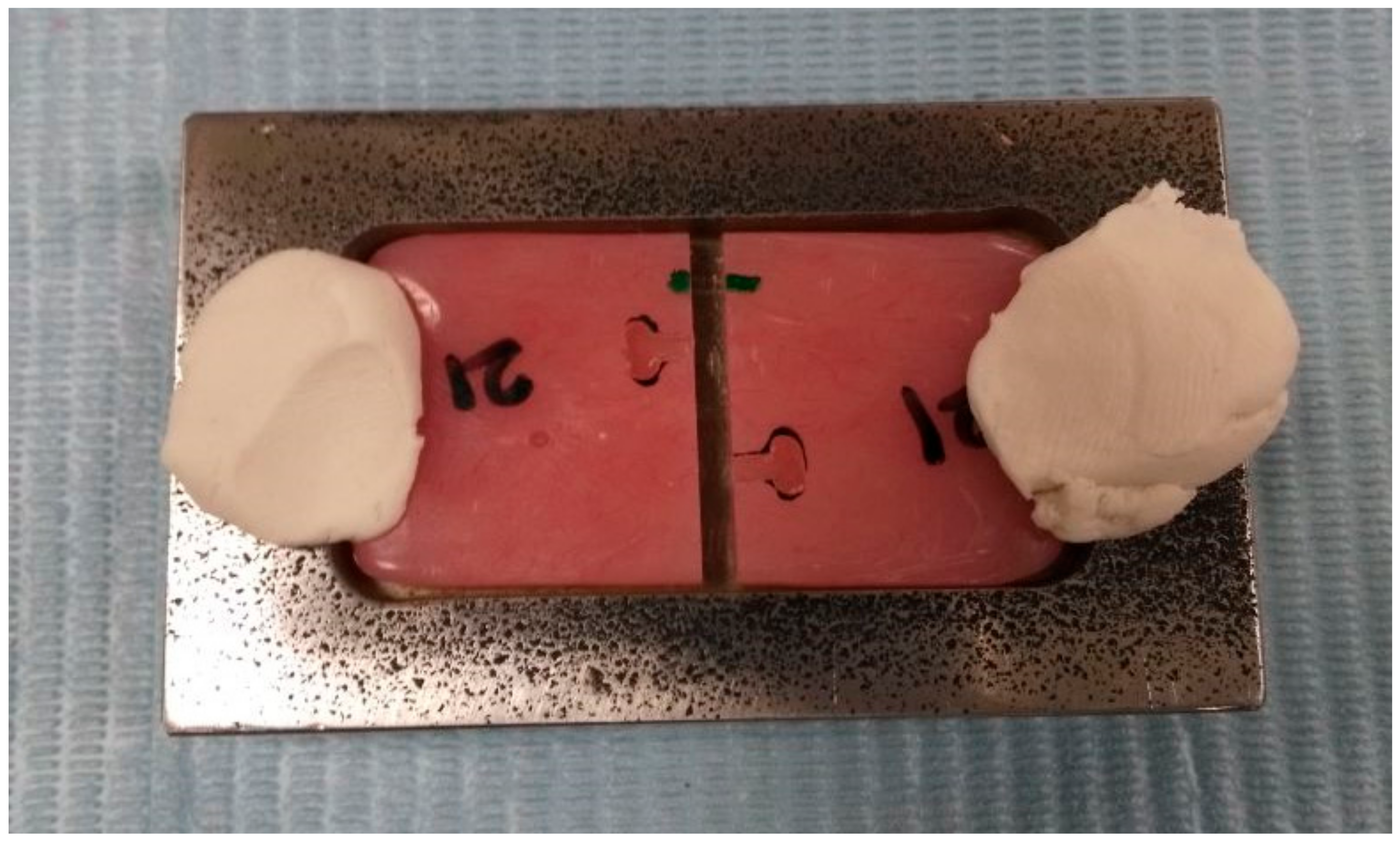
2.1. Preparation of the Samples
2.2. Repair Procedures
2.3. Three-Point Flexural Test
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- The Heat cured PMMA denture base repair with heat polymerized acrylic resin provided the highest fracture resistance and flexural strength.
- Light polymerized acrylic resin used for repairing PMMA denture base performed inferior to heat and auto polymerized acrylic resins both in maximum load and flexural strength.
- Auto-polymerized repair acrylic resins showed a moderately higher flexural strength than light polymerized acrylic resin but showed significantly lesser performance than the heat cure resins.
- Though heat cure repair acrylic resins, recorded the maximum flexural strength, the denture repair procedures are time-consuming, higher cost and require dental laboratory support. Hence, further researches to simplify the repair process is required.
Author Contributions
Funding
Conflicts of Interest
References
- Carlsson, G.E.; Omar, R. The future of complete dentures in oral rehabilitation. A critical review. J. Oral. Rehabil. 2010, 37, 143–156. [Google Scholar] [CrossRef]
- Alla, R.; Raghavendra, K.; Vyas, R.; Konakanchi, A. Conventional and contemporary polymers for the fabrication of denture prosthesis: part I–overview, composition and properties. Int. J. Appl. Dent. Sci. 2015, 1, 82. [Google Scholar]
- Takamiya, A.S.; Monteiro, D.R.; Marra, J.; Compagnoni, M.A.; Barbosa, D.B. Complete denture wearing and fractures among edentulous patients treated in university clinics. Gerodontology 2012, 29, e728–e734. [Google Scholar] [CrossRef]
- Chand, P.; Patel, C.B.S.; Singh, B.P.; Singh, R.D.; Singh, K. Mechanical properties of denture base resins: An evaluation. Indian J. Dent. Res. 2011, 22, 180. [Google Scholar] [PubMed]
- Faot, F.; Garcia, R.C.M.R.; Del Bel Cury, A.A. Fractographic analysis, accuracy of fit and impact strength of acrylic resin. Braz. Oral Res. 2008, 22, 334–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prombonas, A.E.; Vlissidis, D.S. Comparison of the midline stress fields in maxillary and mandibular complete dentures: A pilot study. J. Prosthet. Dent. 2006, 95, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Frascaria, M.; Pietropaoli, D.; Casinelli, M.; Cattaneo, R.; Ortu, E.; Monaco, A. Neutral zone recording in computer-guided implant prosthesis: A new digital neuromuscular approach. Clin. Exp. Dent. Res. 2019, 5, 670–676. [Google Scholar] [CrossRef] [Green Version]
- Falisi, G.; Bernardi, S.; Rastelli, C.; Pietropaoli, D.; De Angelis, F.; Frascaria, M.; C, D.I.P. “All on short” prosthetic-implant supported rehabilitations. ORAL Implantol. 2017, 10, 477–487. [Google Scholar] [CrossRef]
- Eklund, S.A.; Burt, B.A. Risk factors for total tooth loss in the United States; longitudinal analysis of national data. J. Public Health Dent. 1994, 54, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Caplan, D.J.; Weintraub, J.A. The oral health burden in the United States: A summary of recent epidemiologic studies. J. Dent. Educ. 1993, 57, 853–862. [Google Scholar]
- Jeyapalan, V.; Krishnan, C.S. Partial Edentulism and its Correlation to Age, Gender, Socio-economic Status and Incidence of Various Kennedy’s Classes- A Literature Review. J. Clin. Diagn. Res. 2015, 9, Ze14–Ze17. [Google Scholar] [CrossRef] [PubMed]
- Kostoulas, I.; Kavoura, V.T.; Frangou, M.J.; Polyzois, G.L. Fracture force, deflection, and toughness of acrylic denture repairs involving glass fiber reinforcement. J. Prosthodont. 2008, 17, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Meng, T.R., Jr.; Latta, M.A. Physical properties of four acrylic denture base resins. J. Contemp. Dent. Pract. 2005, 6, 93–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, E.; Tan, L.; Chew, B.; Thean, H. Shear bond strength of microwaveable acrylic resin for denture repair. J. Oral Rehabil. 2004, 31, 798–802. [Google Scholar] [CrossRef] [PubMed]
- Lewinstein, I.; Zeltser, C.; Mayer, C.M.; Tal, Y. Transverse bond strength of repaired acrylic resin strips and temperature rise of dentures relined with VLC reline resin. J. Prosthet. Dent. 1995, 74, 392–399. [Google Scholar] [CrossRef]
- John, J.; Gangadhar, S.A.; Shah, I. Flexural strength of heat-polymerized polymethyl methacrylate denture resin reinforced with glass, aramid, or nylon fibers. J. Prosthet. Dent. 2001, 86, 424–427. [Google Scholar] [CrossRef]
- DeBoer, J.; Vermilyea, S.; Brady, R. The effect of carbon fiber orientation on the fatigue resistance and bending properties of two denture resins. J. Prosthet. Dent. 1984, 51, 119–121. [Google Scholar] [CrossRef]
- Murthy, H.M.; Shaik, S.; Sachdeva, H.; Khare, S.; Haralur, S.B.; Roopa, K. Effect of Reinforcement Using Stainless Steel Mesh, Glass Fibers, and Polyethylene on the Impact Strength of Heat Cure Denture Base Resin-An In Vitro Study. J. Int. Oral Health JIOH 2015, 7, 71. [Google Scholar]
- Kanie, T.; Fujii, K.; Arikawa, H.; Inoue, K. Flexural properties and impact strength of denture base polymer reinforced with woven glass fibers. Dent. Mater. 2000, 16, 150–158. [Google Scholar] [CrossRef]
- Nagai, E.; Otani, K.; Satoh, Y.; Suzuki, S. Repair of denture base resin using woven metal and glass fiber: effect of methylene chloride pretreatment. J. Prosthet. Dent. 2001, 85, 496–500. [Google Scholar] [CrossRef]
- Pereira Rde, R.; Delfino, C.S.; Butignon, L.E.; Vaz, M.A.; Arioli-Filho, J.N. Influence of surface treatments on the flexural strength of denture base repair. Gerodontology 2012, 29, e234–e238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasthare, A.; Shetty, S.; Shenoy, K.K.; Shetty, M.S.; Parveen, K.A.; Shetty, R. Effect of different edge profile, surface treatment, and glass fiber reinforcement on the transverse strength of denture base resin repaired with autopolymerizing acrylic resin: An In vitro study. J. Interdis. Dent. 2017, 7, 31. [Google Scholar] [CrossRef]
- Harrison, W.M.; Stansbury, B.E. The effect of joint surface contours on the transverse strength of repaired acrylic resin. J. Prosthet. Dent. 1970, 23, 464–472. [Google Scholar] [CrossRef]
- Seó, R.S.; Neppelenbroek, K.H.; Filho, J.N. Factors affecting the strength of denture repairs. J. Prosthodont. 2007, 16, 302–310. [Google Scholar] [CrossRef]
- Ayaz, E.A.; Bağış, B.; Turgut, S. Effects of thermal cycling on surface roughness, hardness and flexural strength of polymethylmethacrylate and polyamide denture base resins. J. Appl. Biomater. Func. 2015, 13, 280–286. [Google Scholar] [CrossRef]
- Ferracane, J.L. Hygroscopic and hydrolytic effects in dental polymer networks. Dent. Mater 2006, 22, 211–222. [Google Scholar] [CrossRef]
- Mumcu, E.; Cilingir, A.; Gencel, B.; Sülün, T. Flexural properties of a light-cure and a self-cure denture base materials compared to conventional alternatives. J. Adv. Prosthodont. 2011, 3, 136–139. [Google Scholar] [CrossRef]
- Heidari, B.; Firouz, F.; Izadi, A.; Ahmadvand, S.; Radan, P. Flexural strength of cold and heat cure acrylic resins reinforced with different materials. J. Dent. 2015, 12, 316. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Vallittu, P.K.; Ruyter, I. Swelling of poly (methyl methacrylate) resin at the repair joint. Int. J. Prosthodont. 1997, 10, 254–258. [Google Scholar]
- Stipho, H.; Stipho, A. Effectiveness and durability of repaired acrylic resin joints. J. Prosthet. Dent. 1987, 58, 249–253. [Google Scholar] [CrossRef]
- Beyli, M.; Von Fraunhofer, J. Repair of fractured acrylic resin. J. Prosthet. Dent. 1980, 44, 497–503. [Google Scholar] [CrossRef]
- Sarac, Y.S.; Sarac, D.; Kulunk, T.; Kulunk, S. The effect of chemical surface treatments of different denture base resins on the shear bond strength of denture repair. J. Prosthet. Dent. 2005, 94, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Vallittu, P.K. The effect of surface treatment of denture acrylic resin on the residual monomer content and its release into water. Acta Odontol. Scand. 1996, 54, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Leong, A.; Grant, A. The transverse strength of repairs in polymethyl methacrylate. Aust. Dent. J. 1971, 16, 232–234. [Google Scholar] [CrossRef]
- Tan, H.-K.; Brudvik, J.S.; Nicholls, J.I.; Smith, D.E. Adaptation of a visible light-cured denture base material. J. Prosthet. Dent. 1989, 61, 326–331. [Google Scholar] [CrossRef]
- Faot, F.; Da Silva, W.J.; Da Rosa, R.S.; Del Bel Cury, A.A.; Garcia, R.C.M.R. Strength of denture base resins repaired with auto-and visible light-polymerized materials. J. Prosthodont. 2009, 18, 496–502. [Google Scholar] [CrossRef]
- Berge, M. Bending strength of intact and repaired denture base resins. Acta Odontol. Scand. 1983, 41, 187–191. [Google Scholar] [CrossRef]
- Siddesh, C.S.; Aras, M.A. In vitro evaluation of transverse strength of repaired heat cured denture base resins with and without surface chemical treatment. J. Indian Prosthodont. Soc. 2008, 8, 87–93. [Google Scholar]
- Agarwal, M.; Nayak, A.; Hallikerimath, R. A study to evaluate the transverse strength of repaired acrylic denture resins with conventional heat-cured, autopolymerizing and microwave-cured resins: an in vitro study. J. Indian Prosthodont. Soc. 2008, 8, 36. [Google Scholar] [CrossRef]
- Rached, R.N.; Powers, J.M.; Cury, A.A.D.B. Repair strength of autopolymerizing, microwave, and conventional heat-polymerized acrylic resins. J. Prosthet. Dent. 2004, 92, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Stanford, J.W.; Burns, C.L.; Paffenbarger, G.C. Self-curing resins for repairing dentures: Some physical properties. J. Am. Dent. Assoc. 1955, 51, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Al-Mulla, M.; Murphy, W.; Huggett, R.; Brooks, S. Effect of water and artificial saliva on mechanical properties of some denture-base materials. Dent. Mater. 1989, 5, 399–402. [Google Scholar] [CrossRef]
- Heath, J.; Boru, T.; Grant, A. The stability of temporary prosthetic base materials I: Introduction, angular changes and dimensional stability. J. Oral Rehabil. 1993, 20, 363–372. [Google Scholar] [CrossRef]
- Minami, H.; Suzuki, S.; Kurashige, H.; Minesaki, Y.; Tanaka, T. Flexural strengths of denture base resin repaired with autopolymerizing resin and reinforcements after thermocycle stressing. J. Prosthodont. 2005, 14, 12–18. [Google Scholar] [CrossRef]
- Hayakawa, I.; Nagao, M.; Matsumoto, T.; Masuhara, E. Properties of a new light-polymerized relining material. Int. J. Prosthodont. 1990, 3, 278–284. [Google Scholar]
- Ogle, R.; Sorensen, S.; Lewis, E. A new visible light-cured resin system applied to removable prosthodontics. J. Prosthet. Dent. 1986, 56, 497–506. [Google Scholar] [CrossRef]
- Cunningham, J. Shear bond strength of resin teeth to heat-cured and light-cured denture base resin. J. Oral Rehabil. 2000, 27, 312–316. [Google Scholar] [CrossRef]
- Dar-Odeh, N.; Harrison, A.; Abu-Hammad, O. An evaluation of self-cured and visible light-cured denture base materials when used as a denture base repair material. J. Oral Rehabil. 1997, 24, 755–760. [Google Scholar] [CrossRef]
- Polyzois, G.L.; Tarantili, P.A.; Frangou, M.J.; Andreopoulos, A.G. Fracture force, deflection at fracture, and toughness of repaired denture resin subjected to microwave polymerization or reinforced with wire or glass fiber. J. Prosthet. Dent. 2001, 86, 613–619. [Google Scholar] [CrossRef]
- Andreopoulos, A.G.; Polyzois, G.L. Repair of denture base resins using visible light-cured materials. J. Prosthet. Dent. 1994, 72, 462–468. [Google Scholar] [CrossRef]
- Jagger, D.; Alshumailin, Y.; Harrison, A.; Rees, J. The effect of the addition of poly (methyl methacrylate) fibres on the transverse strength of repaired heat-cured acrylic resin. J. Oral Rehabil. 2003, 30, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Vojdani, M.; Rezaei, S.; Zareeian, L. Effect of chemical surface treatments and repair material on transverse strength of repaired acrylic denture resin. Indian J. Dent. Res. 2008, 19, 2. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, H.; Kakigi, M.; Fujii, J.; Tsue, F.; Takahashi, Y. Effect of surface preparation using ethyl acetate on the shear bond strength of repair resin to denture base resin. J. Prosthodont. 2008, 17, 451–455. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Group | N | Maximum Load | Flexure Strength |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| Control | 10 | 173.60 (18.48) | 13.02 (1.29) |
| Heat PMMA | 10 | 87.36 (4.82) | 6.55 (0.45) |
| APMMA | 10 | 62.94 (1.83) | 4.72 (0.13) |
| UDMA | 10 | 57.51 (2.23) | 4.06 (0.21) |
| Test | Source | df | SS | MS | F | p |
|---|---|---|---|---|---|---|
| Maximum load | Between Groups | 3 | 86,700.453 | 28,900.15 | 309.48 | 0.000 * |
| Within Groups | 36 | 3361.689 | 93.38 | |||
| Total | 39 | 90,062.141 | ||||
| Flexural strength | Between Groups | 3 | 501.932 | 167.31 | 343.74 | 0.000 * |
| Within Groups | 36 | 17.522 | 0.48 | |||
| Total | 39 | 519.454 |
| Test | Group | Control | HPMMA | APMMA | UDMA |
|---|---|---|---|---|---|
| Maximum load | Control | - | 0.000 * | 0.000 * | 0.000 * |
| HPMMA | 0.000 * | - | 0.000 * | 0.000 * | |
| APMMA | 0.000 * | 0.000 * | - | 0.000 * | |
| UDMA | 0.000 * | 0.000 * | 0.000 * | - | |
| Flexural strength | Control | - | 0.000 * | 0.000 * | 0.000 * |
| HPMMA | 0.000 * | - | 0.000 * | 0.000 * | |
| APMMA | 0.000 * | 0.000 * | - | 0.000 * | |
| UDMA | 0.000 * | 0.000 * | 0.000 * | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlQahtani, M.; Haralur, S.B. Influence of Different Repair Acrylic Resin and Thermocycling on the Flexural Strength of Denture Base Resin. Medicina 2020, 56, 50. https://doi.org/10.3390/medicina56020050
AlQahtani M, Haralur SB. Influence of Different Repair Acrylic Resin and Thermocycling on the Flexural Strength of Denture Base Resin. Medicina. 2020; 56(2):50. https://doi.org/10.3390/medicina56020050
Chicago/Turabian StyleAlQahtani, Mohammed, and Satheesh B. Haralur. 2020. "Influence of Different Repair Acrylic Resin and Thermocycling on the Flexural Strength of Denture Base Resin" Medicina 56, no. 2: 50. https://doi.org/10.3390/medicina56020050