Hereditary Deficiency of the Second Component of Complement: Early Diagnosis and 21-Year Follow-Up of a Family

 ,
,  and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Laboratory Studies
2.2.1. Hemolytic Assay for Functional Activity of the Classical Complement Pathway
2.2.2. C2 Specific Activity
2.2.3. Functional Immuno-Enzymatic Assay for the Classical Complement Pathway
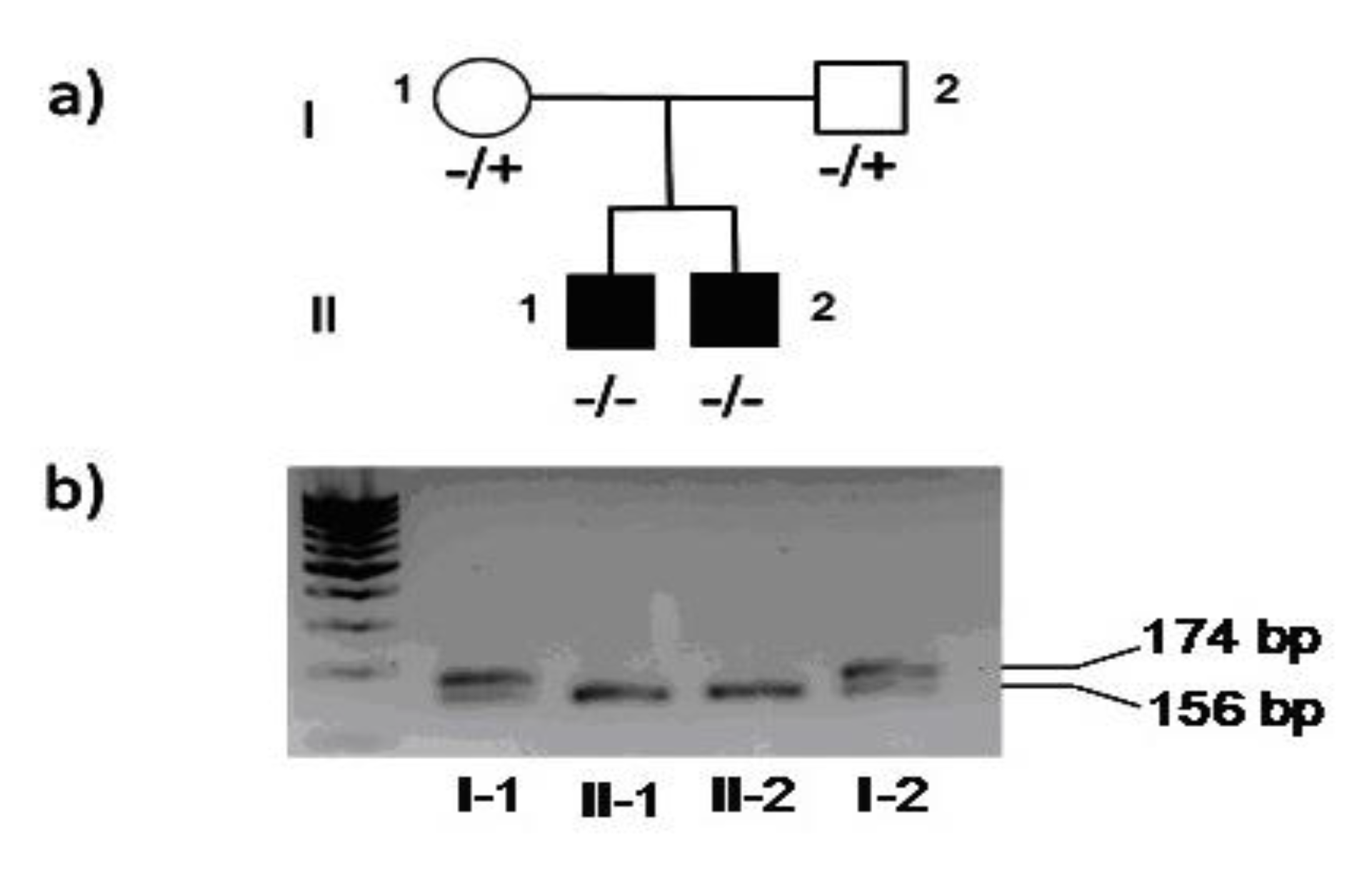
2.2.4. Genetic Analysis
3. Results
3.1. Clinical Features
3.2. Laboratory Studies
3.3. Follow-Up
3.3.1. Patient 1
3.3.2. Patient 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Carroll, M.V.; Sim, R.B. Complement in health and disease. Adv. Drug Deliv. Rev. 2011, 63, 965–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botto, M.; Kirschfink, M.; Macor, P.; Pickering, M.C.; Wurzner, R.; Tedesco, F. Complement in human diseases: Lessons from complement deficiencies. Mol. Immunol. 2009, 46, 2774–2783. [Google Scholar] [CrossRef] [PubMed]
- Tedesco, F. Inherited complement deficiencies and bacterial infections. Vaccine 2008, 26 (Suppl. 8), I3–I8. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.C.; Atkinson, J.P. Overcoming C2 deficiency. Clin. Immunol. 2012, 144, 269–271. [Google Scholar] [CrossRef]
- Pickering, M.C.; Botto, M.; Taylor, P.R.; Lachmann, P.J.; Walport, M.J. Systemic lupus erythematosus, complement deficiency, and apoptosis. Adv. Immunol. 2000, 76, 227–324. [Google Scholar] [CrossRef]
- Barilla-LaBarca, M.L.; Atkinson, J.P. Rheumatic syndromes associated with complement deficiency. Curr. Opin. Rheumatol. 2003, 15, 55–60. [Google Scholar] [CrossRef]
- Sullivan, K.E. Complement deficiency and autoimmunity. Curr. Opin. Pediatrics 1998, 10, 600–606. [Google Scholar] [CrossRef]
- Jonsson, G.; Truedsson, L.; Sturfelt, G.; Oxelius, V.A.; Braconier, J.H.; Sjoholm, A.G. Hereditary C2 deficiency in Sweden: Frequent occurrence of invasive infection, atherosclerosis, and rheumatic disease. Medicine 2005, 84, 23–34. [Google Scholar] [CrossRef]
- Jonsson, G.; Lood, C.; Gullstrand, B.; Holmstrom, E.; Selander, B.; Braconier, J.H.; Sturfelt, G.; Bengtsson, A.A.; Truedsson, L. Vaccination against encapsulated bacteria in hereditary C2 deficiency results in antibody response and opsonization due to antibody-dependent complement activation. Clin. Immunol. 2012, 144, 214–227. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.W.; Rich, E.; Saint-Cyr, C.; Bourre-Tessier, J. Hereditary Heterozygous C2 Deficiency: Variable Clinical and Serological Manifestations Among Three Sisters. Curr. Rheumatol. Rev. 2017, 13, 158–160. [Google Scholar] [CrossRef]
- Sullivan, K.E.; Petri, M.A.; Schmeckpeper, B.J.; McLean, R.H.; Winkelstein, J.A. Prevalence of a mutation causing C2 deficiency in systemic lupus erythematosus. J. Rheumatol. 1994, 21, 1128–1133. [Google Scholar] [PubMed]
- Grumach, A.S.; Kirschfink, M. Are complement deficiencies really rare? Overview on prevalence, clinical importance and modern diagnostic approach. Mol. Immunol. 2014, 61, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Pontoglio, M.; Pausa, M.; Doyen, A.; Viollet, B.; Yaniv, M.; Tedesco, F. Hepatocyte nuclear factor 1alpha controls the expression of terminal complement genes. J. Exp. Med. 2001, 194, 1683–1689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dellepiane, R.M.; Dell’Era, L.; Pavesi, P.; Macor, P.; Giordano, M.; De Maso, L.; Pietrogrande, M.C.; Cugno, M. Invasive meningococcal disease in three siblings with hereditary deficiency of the 8(th) component of complement: Evidence for the importance of an early diagnosis. Orphanet J. Rare Dis. 2016, 11, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jorge, E.G.; Macor, P.; Paixao-Cavalcante, D.; Rose, K.L.; Tedesco, F.; Cook, H.T.; Botto, M.; Pickering, M.C. The development of atypical hemolytic uremic syndrome depends on complement C5. J. Am. Soc. Nephrol. JASN 2011, 22, 137–145. [Google Scholar] [CrossRef] [Green Version]
- Cugno, M.; Gualtierotti, R.; Possenti, I.; Testa, S.; Tel, F.; Griffini, S.; Grovetti, E.; Tedeschi, S.; Salardi, S.; Cresseri, D.; et al. Complement functional tests for monitoring eculizumab treatment in patients with atypical hemolytic uremic syndrome. J. Thromb. Haemost. JTH 2014, 12, 1440–1448. [Google Scholar] [CrossRef]
- Modell, V.; Gee, B.; Lewis, D.B.; Orange, J.S.; Roifman, C.M.; Routes, J.M.; Sorensen, R.U.; Notarangelo, L.D.; Modell, F. Global study of primary immunodeficiency diseases (PI)–diagnosis, treatment, and economic impact: An updated report from the Jeffrey Modell Foundation. Immunol. Res. 2011, 51, 61–70. [Google Scholar] [CrossRef]
- Naidoo, R.; Ungerer, L.; Cooper, M.; Pienaar, S.; Eley, B.S. Primary immunodeficiencies: A 27-year review at a tertiary paediatric hospital in Cape Town, South Africa. J. Clin. Immunol. 2011, 31, 99–105. [Google Scholar] [CrossRef]
- Turley, A.J.; Gathmann, B.; Bangs, C.; Bradbury, M.; Seneviratne, S.; Gonzalez-Granado, L.I.; Hackett, S.; Kutukculer, N.; Alachkar, H.; Hambleton, S.; et al. Spectrum and management of complement immunodeficiencies (excluding hereditary angioedema) across Europe. J. Clin. Immunol. 2015, 35, 199–205. [Google Scholar] [CrossRef]
- Orren, A.; Owen, E.P.; Henderson, H.E.; van der Merwe, L.; Leisegang, F.; Stassen, C.; Potter, P.C. Complete deficiency of the sixth complement component (C6Q0), susceptibility to Neisseria meningitidis infections and analysis of the frequencies of C6Q0 gene defects in South Africans. Clin. Exp. Immunol. 2012, 167, 459–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahl, M.; Tybjaerg-Hansen, A.; Schnohr, P.; Nordestgaard, B.G. A population-based study of morbidity and mortality in mannose-binding lectin deficiency. J. Exp. Med. 2004, 199, 1391–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Circolo, A.; Lokki, M.L.; Shackelford, P.G.; Wetsel, R.A.; Colten, H.R. Molecular heterogeneity in deficiency of complement protein C2 type I. Immunology 1998, 93, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Gaschignard, J.; Levy, C.; Chrabieh, M.; Boisson, B.; Bost-Bru, C.; Dauger, S.; Dubos, F.; Durand, P.; Gaudelus, J.; Gendrel, D.; et al. Invasive pneumococcal disease in children can reveal a primary immunodeficiency. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2014, 59, 244–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidel, M.G.; Kindle, G.; Gathmann, B.; Quinti, I.; Buckland, M.; van Montfrans, J.; Scheible, R.; Rusch, S.; Gasteiger, L.M.; Grimbacher, B.; et al. The European Society for Immunodeficiencies (ESID) Registry Working Definitions for the Clinical Diagnosis of Inborn Errors of Immunity. J. Allergy Clin. Immunol. Pract. 2019, 7, 1763–1770. [Google Scholar] [CrossRef]
- Picard, C.; Bobby Gaspar, H.; Al-Herz, W.; Bousfiha, A.; Casanova, J.L.; Chatila, T.; Crow, Y.J.; Cunningham-Rundles, C.; Etzioni, A.; Franco, J.L.; et al. International Union of Immunological Societies: 2017 Primary Immunodeficiency Diseases Committee Report on Inborn Errors of Immunity. J. Clin. Immunol. 2018, 38, 96–128. [Google Scholar] [CrossRef] [Green Version]
- Bousfiha, A.; Jeddane, L.; Picard, C.; Ailal, F.; Bobby Gaspar, H.; Al-Herz, W.; Chatila, T.; Crow, Y.J.; Cunningham-Rundles, C.; Etzioni, A.; et al. The 2017 IUIS Phenotypic Classification for Primary Immunodeficiencies. J. Clin. Immunol. 2018, 38, 129–143. [Google Scholar] [CrossRef] [Green Version]
- Seligmann, M.; Brouet, J.C.; Sasportes, M. Hereditary C2 deficiency associated with common variable immunodeficiency. Ann. Intern. Med. 1979, 91, 216–217. [Google Scholar] [CrossRef]
- Agnello, V. Complement deficiency states. Medicine 1978, 57, 1–23. [Google Scholar] [CrossRef]
- Alper, C.A.; Xu, J.; Cosmopoulos, K.; Dolinski, B.; Stein, R.; Uko, G.; Larsen, C.E.; Dubey, D.P.; Densen, P.; Truedsson, L.; et al. Immunoglobulin deficiencies and susceptibility to infection among homozygotes and heterozygotes for C2 deficiency. J. Clin. Immunol. 2003, 23, 297–305. [Google Scholar] [CrossRef]
- Sjoholm, A.G.; Jonsson, G.; Braconier, J.H.; Sturfelt, G.; Truedsson, L. Complement deficiency and disease: An update. Mol. Immunol. 2006, 43, 78–85. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| CH50 (U/mL) | Classical Pathway Activity (% of Normal) | C2 (μg/mL) | |
|---|---|---|---|
| Father | 876 | 100 | 8 |
| Mother | 684 | 84 | 12 |
| Patient 1 | 0 | 3 | 0 |
| Patient 2 | 0 | 3 | 0 |
| Normal values * | 900–1300 | 69–129 | 10–30 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dellepiane, R.M.; Baselli, L.A.; Cazzaniga, M.; Lougaris, V.; Macor, P.; Giordano, M.; Gualtierotti, R.; Cugno, M. Hereditary Deficiency of the Second Component of Complement: Early Diagnosis and 21-Year Follow-Up of a Family. Medicina 2020, 56, 120. https://doi.org/10.3390/medicina56030120
Dellepiane RM, Baselli LA, Cazzaniga M, Lougaris V, Macor P, Giordano M, Gualtierotti R, Cugno M. Hereditary Deficiency of the Second Component of Complement: Early Diagnosis and 21-Year Follow-Up of a Family. Medicina. 2020; 56(3):120. https://doi.org/10.3390/medicina56030120
Chicago/Turabian StyleDellepiane, Rosa Maria, Lucia Augusta Baselli, Marco Cazzaniga, Vassilios Lougaris, Paolo Macor, Mara Giordano, Roberta Gualtierotti, and Massimo Cugno. 2020. "Hereditary Deficiency of the Second Component of Complement: Early Diagnosis and 21-Year Follow-Up of a Family" Medicina 56, no. 3: 120. https://doi.org/10.3390/medicina56030120