Anatomical Morphology Analysis of Internal Jugular Veins and Factors Affecting Internal Jugular Vein Size


Abstract
:1. Introduction
2. Materials and Methods
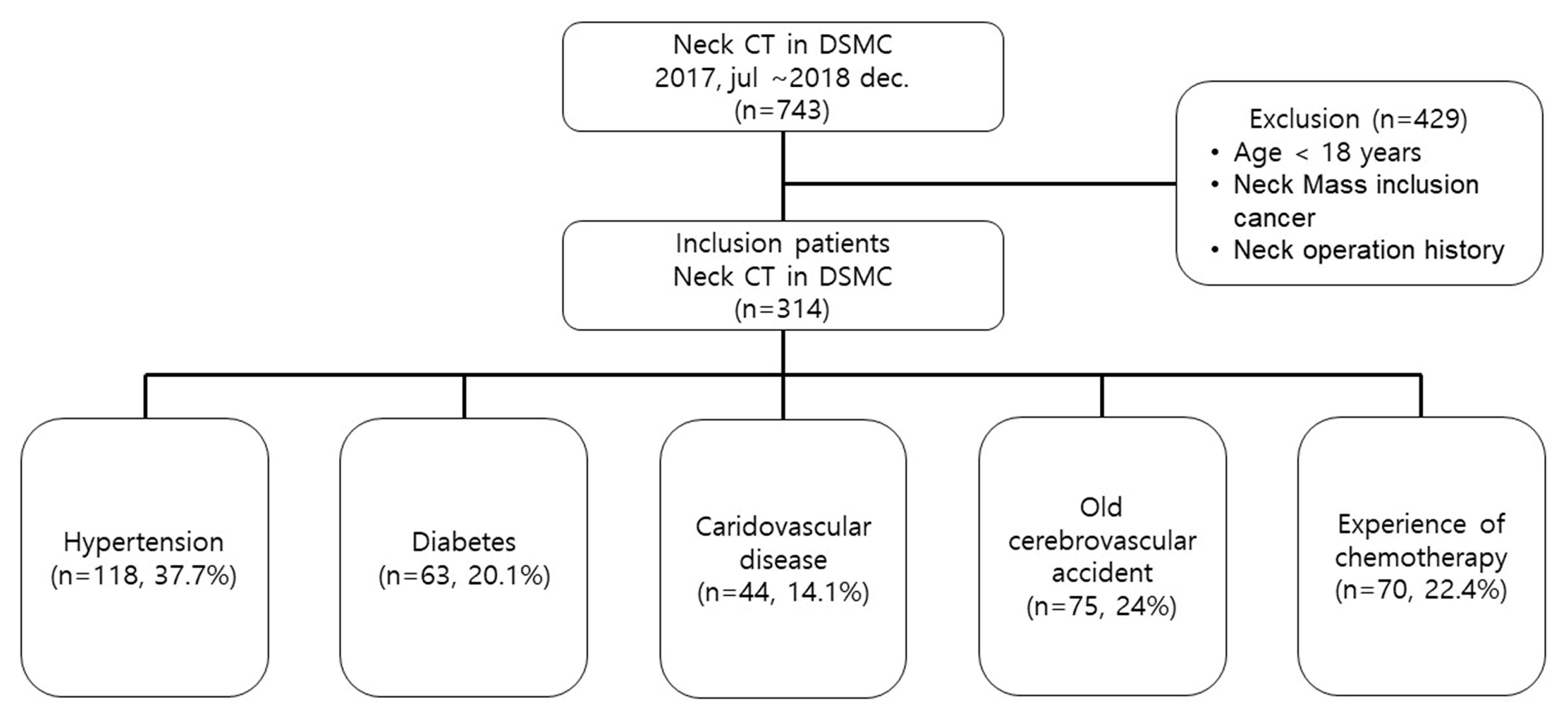
2.1. Study Design and Search Strategy
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Decker, K.; Ireland, S.; O’Sullivan, L.; Boucher, S.; Kite, L.; Rhodes, D.; Mitra, B. Peripheral intravenous catheter insertion in the Emergency Department. Australas Emerg. Nurs. J. 2016, 19, 138–142. [Google Scholar] [CrossRef]
- McGee, D.C.; Gould, M.K. Preventing complications of central venous catheterization. N. Engl. J. Med. 2003, 348, 1123–1133. [Google Scholar] [CrossRef]
- Parienti, J.J.; Mongardon, N.; Megarbane, B.; Mira, J.P.; Kalfon, P.; Gros, A.; Marque, S.; Thuong, M.; Pottier, V.; Ramakers, M.; et al. Intravascular Complications of Central Venous Catheterization by Insertion Site. N. Engl. J. Med. 2015, 373, 1220–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saugel, B.; Scheeren, T.W.L.; Teboul, J.L. Ultrasound-guided central venous catheter placement: A structured review and recommendations for clinical practice. Crit. Care 2017, 21, 225. [Google Scholar] [CrossRef] [Green Version]
- Giordano, C.R.; Murtagh, K.R.; Mills, J.; Deitte, L.A.; Rice, M.J.; Tighe, P.J. Locating the optimal internal jugular target site for central venous line placement. J. Clin. Anesth. 2016, 33, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Monti, L.; Menci, E.; Piu, P.; Leonini, S.; Arrigucci, U.; Bellini, M.; Zandonella, A.; Galluzzi, P.; Casasco, A. A sonographic quantitative cutoff value of cerebral venous outflow in neurologic diseases: A blinded study of 115 subjects. AJNR Am. J. Neuroradiol. 2014, 35, 1381–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Berardino, F.; Alpini, D.C.; Bavera, P.M.; Cecconi, P.; Farabola, M.; Mattei, V.; Ambrosetti, U.; Cesarani, A. Chronic cerebrospinal venous insufficiency in Meniere disease. Phlebology 2015, 30, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Beggs, C.; Chung, C.P.; Bergsland, N.; Wang, P.N.; Shepherd, S.; Cheng, C.Y.; Dwyer, M.G.; Hu, H.-H.; Zivadinov, R. Jugular venous reflux and brain parenchyma volumes in elderly patients with mild cognitive impairment and Alzheimer’s disease. BMC Neurol. 2013, 13, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; Xu, H.; Wang, Y.; Zhong, Y.; Xia, S.; Utriainen, D.; Wang, T.; Haacke, E.M. Patterns of chronic venous insufficiency in the dural sinuses and extracranial draining veins and their relationship with white matter hyperintensities for patients with Parkinson’s disease. J. Vasc. Surg. 2015, 61, 1511–1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, E.; Kappel, J.; MacRae, J.; Dipchand, C.; Hiremath, S.; Kiaii, M.; Lok, C.; Moist, L.; Oliver, M.; Miller, L.M.; et al. Practical Aspects of Nontunneled and Tunneled Hemodialysis Catheters. Can. J. Kidney Health Dis. 2016, 3, 2054358116669128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safety Committee of Japanese Society of Anesthesiologists. Practical guide for safe central venous catheterization and management 2017. J. Anesth. 2019, 1–20. [Google Scholar] [CrossRef]
- Moayedi, S.; Witting, M.; Pirotte, M. Safety and Efficacy of the “Easy Internal Jugular (IJ)”: An Approach to Difficult Intravenous Access. J. Emerg. Med. 2016, 51, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Frykholm, P.; Pikwer, A.; Hammarskjold, F.; Larsson, A.T.; Lindgren, S.; Lindwall, R.; Taxbro, K.; Oberg, F.; Acosta, S.; AAkeson, J. Clinical guidelines on central venous catheterisation. Swedish Society of Anaesthesiology and Intensive Care Medicine. Acta Anaesthesiol. Scand. 2014, 58, 508–524. [Google Scholar] [CrossRef] [PubMed]
- Magnano, C.; Belov, P.; Krawiecki, J.; Hagemeier, J.; Beggs, C.; Zivadinov, R. Internal Jugular Vein Cross-Sectional Area Enlargement Is Associated with Aging in Healthy Individuals. PLoS ONE 2016, 11, e0149532. [Google Scholar] [CrossRef] [PubMed]
- Benter, T.; Teichgraber, U.K.; Kluhs, L.; Papadopoulos, S.; Kohne, C.H.; Felix, R.; Dorken, B. Anatomical variations in the internal jugular veins of cancer patients affecting central venous access. Ultraschall Med. 2001, 22, 23–26. [Google Scholar] [PubMed]
- Lin, B.S.; Kong, C.W.; Tarng, D.C.; Huang, T.P.; Tang, G.J. Anatomical variation of the internal jugular vein and its impact on temporary haemodialysis vascular access: An ultrasonographic survey in uraemic patients. Nephrol. Dial. Transplant. 1998, 13, 134–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, C.P.; Lin, Y.J.; Chao, A.C.; Lin, S.J.; Chen, Y.Y.; Wang, Y.J.; Hu, H.-H. Jugular venous hemodynamic changes with aging. Ultrasound Med. Biol. 2010, 36, 1776–1782. [Google Scholar] [CrossRef]
- Magnano, C.B.P.; Krawiecki, J.; Hagemeier, J.; Zivadinov, R. Internal jugular vein narrowing and body mass index in healthy individuals and multiple sclerosis patients. Veins Lymphat. 2014, 3. [Google Scholar] [CrossRef] [Green Version]
- Henry, G. Gray’s Anatomy: The Classics Collectors, 28th ed.; Random House: New York, NY, USA, 1966. [Google Scholar]
- Frank, N. Netter’s Atlas of Human Anatomy; ICON Learning System: Yardley, PA, USA, 1989. [Google Scholar]
- Agur, A.L.M. Grant’s Atlas of Anatomy, 10th ed.; Lippincott, Wiliams, and Wilkins: Philadelphia, PA, USA, 1999. [Google Scholar]
- Urakov, A.L.; Shchegolev, A.V.; Kasatkin, A.A.; Nigmatullina, A.R. Changes in the Internal Size of the Jugular Vein in Adult Patients with Hypovolemia. Int. J. Appl Basic Med. Res. 2018, 8, 174–176. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Location | Unit of Measure | Total | Right | Left | p-Value | Hedges’ g |
|---|---|---|---|---|---|---|
| Upper | Diameter (mm) | 13.2 (10.9–15.7) | 14.3 (12.3–16.8) | 12.0 (10.2–14.6) | <0.001 | 0.69 |
| Area (mm2) | 109.4 (76.5–153.2) | 124.3 (98.7–176.2) | 89.1 (65.1–124.9) | <0.001 | 0.73 | |
| Middle | Diameter (mm) | 16.0 (13.0–19.9) | 17.6 (14.8–20.9) | 14.4 (11.8–17.5) | <0.001 | 0.73 |
| Area (mm2) | 158.5 (105.8–226.7) | 190.8 (137.2–258.0) | 127.0 (88.0–180.2) | <0.001 | 0.73 | |
| Lower | Diameter (mm) | 13.9 (11.4–17.3) | 16.5 (14.2–19.1) | 11.8 (10.2–13.8) | <0.001 | 0.77 |
| Area (mm2) | 127.4 (89.0–196.3) | 183.1 (127.6–241.6) | 94.5 (68.7–126.7) | <0.001 | 0.19 |
| Location | Unit of Measure | Upper | Middle | Lower | p-Value |
|---|---|---|---|---|---|
| Right | Diameter (mm) | 14.3 (12.3–16.8) | 17.6 (14.8–20.9) | 16.5 (14.2–19.1) | <0.001 |
| Area (mm2) | 124.3 (98.7–176.2) | 190.8 (137.2–258.0) | 183.1 (127.6–241.6) | <0.001 | |
| Left | Diameter (mm) | 12.0 (10.2–14.6) | 14.4 (11.8–17.5) | 11.8 (10.2–13.8) | <0.001 |
| Area (mm2) | 89.1 (65.1–124.9) | 127.0 (88.0–180.2) | 94.5 (68.7–126.7) | <0.001 |
| Total (n = 313) | Small (n = 157) | Large (n = 156) | p-Value | |
|---|---|---|---|---|
| Sex, male, n (%) | 160 (51.1) | 75 (47.8) | 85 (54.5) | 0.235 |
| Hypertension, n (%) | 118 (37.7) | 51 (32.5) | 67 (42.9) | 0.056 |
| Diabetes, n (%) | 63 (20.1) | 30 (19.1) | 33 (21.2) | 0.652 |
| CV disease, n (%) | 44 (14.1) | 13 (8.3) | 31 (19.9) | 0.003 |
| Old CVA, n (%) | 75 (24.0) | 33 (21.0) | 42 (26.9) | 0.221 |
| History of CTx, n (%) | 70 (22.4) | 35 (22.3) | 35 (22.4) | 0.976 |
| Age (years) | 65.0 (50.0-74.0) | 58 (45.5-69) | 69 (59–77) | <0.001 |
| Height (cm) | 161.0 (155.3–167.9) | 162.0 (156.4–168.3) | 160.1 (153.2–166.4) | 0.099 |
| Weight (kg) | 62.0 (53.0–69.6) | 61.9 (53.0–68.3) | 62 (52.6–71) | 0.358 |
| Body mass index (kg/m2) | 23.6 (21.2–26.3) | 23.1 (20.8–25.5) | 23.9 (21.6–27.1) | 0.024 |
| Odds Ratio | 95% Confidence Interval | p-Value | |
|---|---|---|---|
| Age | 1.040 | 1.022–1.058 | <0.001 * |
| Sex, Male | 1.301 | 0.812–2.086 | 0.274 |
| Cardiovascular disease | 1.983 | 0.960–4.095 | 0.064 |
| Hypertension | 0.769 | 0.446–1.328 | 0.347 |
| Body mass index | 1.080 | 1.011–1.154 | 0.023 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, J.C.; Choi, W.I.; Lee, J.H.; Lee, S.H. Anatomical Morphology Analysis of Internal Jugular Veins and Factors Affecting Internal Jugular Vein Size. Medicina 2020, 56, 135. https://doi.org/10.3390/medicina56030135
Jeon JC, Choi WI, Lee JH, Lee SH. Anatomical Morphology Analysis of Internal Jugular Veins and Factors Affecting Internal Jugular Vein Size. Medicina. 2020; 56(3):135. https://doi.org/10.3390/medicina56030135
Chicago/Turabian StyleJeon, Jae Cheon, Woo Ik Choi, Jae Ho Lee, and Sang Hun Lee. 2020. "Anatomical Morphology Analysis of Internal Jugular Veins and Factors Affecting Internal Jugular Vein Size" Medicina 56, no. 3: 135. https://doi.org/10.3390/medicina56030135
APA StyleJeon, J. C., Choi, W. I., Lee, J. H., & Lee, S. H. (2020). Anatomical Morphology Analysis of Internal Jugular Veins and Factors Affecting Internal Jugular Vein Size. Medicina, 56(3), 135. https://doi.org/10.3390/medicina56030135