
Objectivation of an Educational Model in Cranial Osteopathy Based on Experience



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
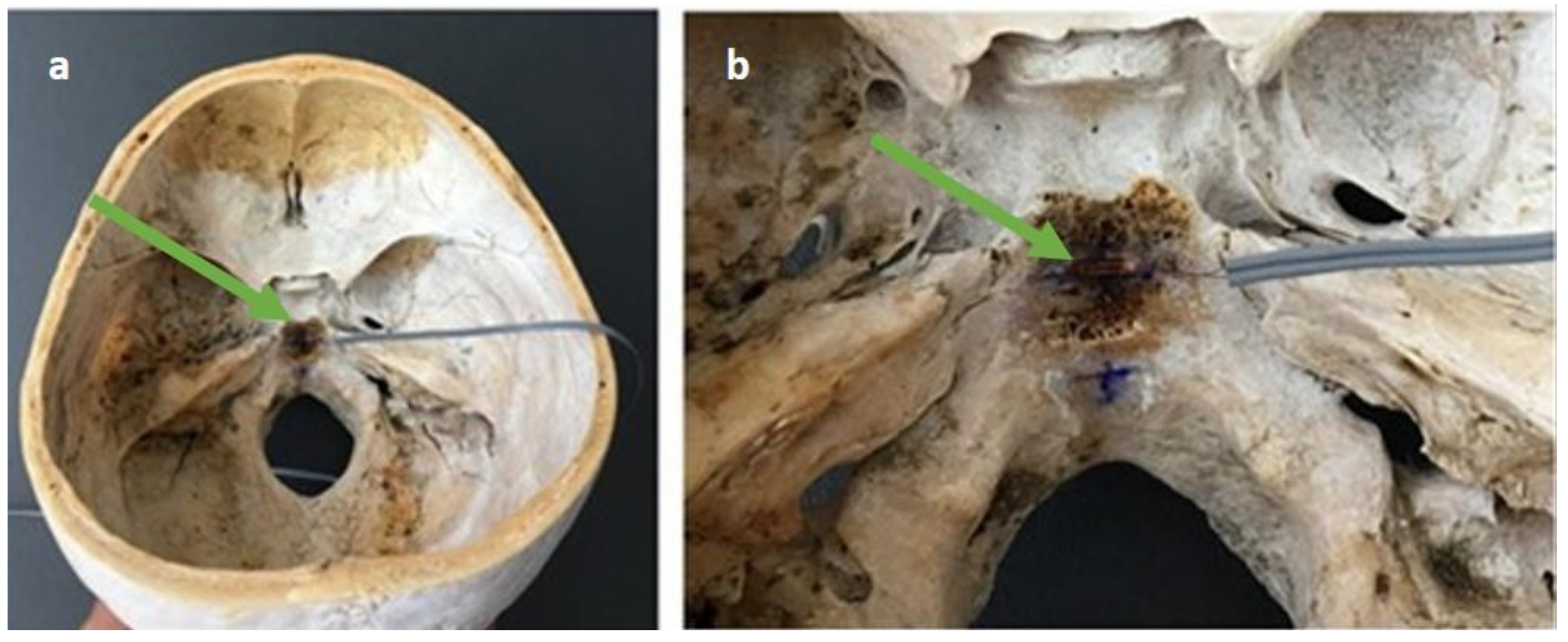
2.2. Material of Assays
2.3. Measurements
- Lateral compression (technique 1): The osteopath places one hand on the occipital and the other on the main wings of the sphenoid. The anterior hand makes an internal pressure through the major wings of the sphenoid, the posterior hand makes an internal pressure through the occipital squama.
- Anteroposterior compression (technique 2): Osteopath’s hands are placed on the occipital and on the frontal bone. The maneuver consists of performing an integer-posterior pressure producing compression of the SBS.
- Compression of mastoids (technique 3): The osteopath places both thumbs and thenar eminences on the mastoid processes. The action consists of pressing both mastoids in the direction of the SBS.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hamonet, C. Andrew Taylor Still and the birth of osteopathy (Baldwin, Kansas, USA, 1855). Jt. Bone Spine 2003, 70, 80–84. [Google Scholar] [CrossRef]
- Jonas, C. Musculoskeletal Therapies: Osteopathic Manipulative Treatment. FP Essent. 2018, 470, 11–15. [Google Scholar] [PubMed]
- American Osteopathic Association Guidelines for Osteopathic Manipulative Treatment (OMT) for Patients With Low Back Pain. J. Am. Osteopath. Assoc. 2016, 116, 536–549. [CrossRef] [Green Version]
- Licciardone, J.C.; Brimhall, A.K.; King, L.N. Osteopathic manipulative treatment for low back pain: A systematic review and meta-analysis of randomized controlled trials. BMC Musculoskelet. Disord. 2005, 6, 43. [Google Scholar] [CrossRef] [PubMed]
- Luciani, E.; Consorti, G.; van Dun, P.L.S.; Merdy, O.; Lunghi, C.; Petracca, M.; Esteves, J.E.; Cerritelli, F. An overview of osteopathy graduates’ perceived preparedness at transition from educational environment to clinic environment one year after graduation: A cross sectional study. BMC Med. Educ. 2018, 18, 319. [Google Scholar] [CrossRef] [Green Version]
- Guillaud, A.; Darbois, N.; Monvoisin, R.; Pinsault, N. Reliability of Diagnosis and Clinical Efficacy of Cranial Osteopathy: A Systematic Review. PLoS ONE 2016, 11, e0167823. [Google Scholar] [CrossRef] [PubMed]
- Dossett, M.L.; Cohen, E.M.; Cohen, J. Integrative Medicine for Gastrointestinal Disease. Prim. Care 2017, 44, 265–280. [Google Scholar] [CrossRef]
- Martins, W.R.; Diniz, L.R.; Blasczyk, J.C.; Lagoa, K.F.; Thomaz, S.; Rodrigues, M.E.; de Oliveira, R.J.; Bonini-Rocha, A.C. Immediate changes in electroencephalography activity in individuals with nonspecific chronic low back pain after cranial osteopathic manipulative treatment: Study protocol of a randomized, controlled crossover trial. BMC Complement Altern. Med. 2015, 15, 223. [Google Scholar] [CrossRef] [Green Version]
- Hall, H.; Cramer, H.; Sundberg, T.; Ward, L.; Adams, J.; Moore, C.; Sibbritt, D.; Lauche, R. The effectiveness of complementary manual therapies for pregnancy-related back and pelvic pain: A systematic review with meta-analysis. Medicine 2016, 95, e4723. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.C.; Thomas, J.S.; Walkowski, S.A.; Howell, J.N. The biology of manual therapies. J. Am. Osteopath. Assoc. 2012, 112, 617–629. [Google Scholar] [PubMed]
- Hastings, V.; McCallister, A.M.; Curtis, S.A.; Valant, R.J.; Yao, S. Efficacy of Osteopathic Manipulative Treatment for Management of Postpartum Pain. J. Am. Osteopath. Assoc. 2016, 116, 502–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutherland, W.G. The cranial bowl. 1944. J. Am. Osteopath. Assoc. 2000, 100, 568–573. [Google Scholar] [PubMed]
- Sommerfeld, P.; Kaider, A.; Klein, P. Inter- and intraexaminer reliability in palpation of the “primary respiratory mechanism” within the “cranial concept”. Man. Ther. 2004, 9, 22–29. [Google Scholar] [CrossRef]
- Hartman, S.E. Cranial osteopathy: Its fate seems clear. Chiropr. Osteopat. 2006, 14, 10. [Google Scholar] [CrossRef] [Green Version]
- Sabini, R.C.; Elkowitz, D.E. Significance of differences in patency among cranial sutures. J. Am. Osteopath. Assoc. 2006, 106, 600–604. [Google Scholar] [PubMed]
- Kiviniemi, V.; Wang, X.; Korhonen, V.; Keinänen, T.; Tuovinen, T.; Autio, J.; LeVan, P.; Keilholz, S.; Zang, Y.F.; Hennig, J.; et al. Ultra-fast magnetic resonance encephalography of physiological brain activity—Glymphatic pulsation mechanisms? J. Cereb. Blood Flow Metab. 2016, 36, 1033–1045. [Google Scholar] [CrossRef] [PubMed]
- Strik, C.; Klose, U.; Erb, M.; Strik, H.; Grodd, W. Intracranial oscillations of cerebrospinal fluid and blood flows: Analysis with magnetic resonance imaging. J. Magn. Reson. Imaging 2002, 15, 251–258. [Google Scholar] [CrossRef]
- Crow, W.T.; King, H.H.; Patterson, R.M.; Giuliano, V. Assessment of calvarial structure motion by MRI. Osteopath. Med. Prim. Care 2009, 3, 8. [Google Scholar] [CrossRef] [Green Version]
- Bordoni, B.; Zanier, E. Sutherland’s legacy in the new millennium: The osteopathic cranial model and modern osteopathy. Adv. Mind Body Med. 2015, 29, 15–21. [Google Scholar] [PubMed]
- Whalen, J.; Yao, S.; Leder, A. A Short Review of the Treatment of Headaches Using Osteopathic Manipulative Treatment. Curr. Pain Headache Rep. 2018, 22, 82. [Google Scholar] [CrossRef] [PubMed]
- Haller, H.; Lauche, R.; Cramer, H.; Rampp, T.; Saha, F.J.; Ostermann, T.; Dobos, G. Craniosacral Therapy for the Treatment of Chronic Neck Pain: A Randomized Sham-controlled Trial. Clin. J. Pain 2016, 32, 441–449. [Google Scholar] [CrossRef] [Green Version]
- Jakel, A.; von Hauenschild, P. Therapeutic effects of cranial osteopathic manipulative medicine: A systematic review. J. Am. Osteopath. Assoc. 2011, 111, 685–693. [Google Scholar] [PubMed]
- Ingber, D.E. Tensegrity: The architectural basis of cellular mechanotransduction. Annu. Rev. Physiol. 1997, 59, 575–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langevin, H.M.; Storch, K.N.; Snapp, R.R.; Bouffard, N.A.; Badger, G.J.; Howe, A.K.; Taatjes, D.J. Tissue stretch induces nuclear remodeling in connective tissue fibroblasts. Histochem. Cell Biol. 2010, 133, 405–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kostopoulos, D.C.; Keramidas, G. Changes in elongation of falx cerebri during craniosacral therapy techniques applied on the skull of an embalmed cadaver. Cranio 1992, 10, 9–12. [Google Scholar] [CrossRef]
- Oleski, S.L.; Smith, G.H.; Crow, W.T. Radiographic evidence of cranial bone mobility. Cranio 2002, 20, 34–38. [Google Scholar] [CrossRef]
- Green, C.; Martin, C.W.; Bassett, K.; Kazanjian, A. A systematic review of craniosacral therapy: Biological plausibility, assessment reliability and clinical effectiveness. Complement Ther. Med. 1999, 7, 201–207. [Google Scholar] [CrossRef]
- Moran, R.W.; Gibbons, P. Intraexaminer and interexaminer reliability for palpation of the cranial rhythmic impulse at the head and sacrum. J. Manip. Physiol. Ther. 2001, 24, 183–190. [Google Scholar] [CrossRef]
- Fechoz, F.; Delecrin, J.; Passuti, N.; Royer, J. Mechanical behavior of the human acetabulum. Study by electric extensiometry before and after implantations of prosthetic units. Chirurgie 1993, 119, 278–281. [Google Scholar] [PubMed]
- Downey, P.A.; Barbano, T.; Kapur-Wadhwa, R.; Sciote, J.J.; Siegel, M.I.; Mooney, M.P. Craniosacral therapy: The effects of cranial manipulation on intracranial pressure and cranial bone movement. J. Orthop. Sports Phys. Ther. 2006, 36, 845–853. [Google Scholar] [CrossRef]
- Seimetz, C.N.; Kemper, A.R.; Duma, S.M. An investigation of cranial motion through a review of biomechanically based skull deformation literature. Int. J. Osteopath. Med. 2012, 15, 152–165. [Google Scholar] [CrossRef]
- Nascimento, L.P.; Oliva-Pascual-Vaca, A.; Renan-Ordine, R.; Riquelme, I.; Ricard, F.; Rodriguez-Blanco, C. Comparative assessment of tactile sensitivity between undergraduate and postgraduate health sciences students. Int. J. Osteopath. Med. 2016, 19, 13–19. [Google Scholar] [CrossRef]
- Zegarra-Parodi, R.; de Chauvigny de Blot, P.; Rickards, L.D.; Renard, E.O. Cranial palpation pressures used by osteopathy students: Effects of standardized protocol training. J. Am. Osteopath. Assoc. 2009, 109, 79–85. [Google Scholar] [PubMed]
- Scarr, G. A model of the cranial vault as a tensegrity structure, and its significance to normal and abnormal cranial development. Int. J. Osteopath. Med. 2008, 11, 80–89. [Google Scholar] [CrossRef]
- Kasparian, H.; Signoret, G.; Kasparian, J. Quantification of Motion Palpation. J. Am. Osteopath. Assoc. 2015, 115, 604–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basic-Kes, V.; Basic-Jukic, N.; Kes, P.; Demarin, V.; Labar, B. Neurologic sequelae of bone changes in multiple myeloma and its therapy. Acta Med. Croat. 2002, 56, 103–107. [Google Scholar]


{kind=link}
{kind=link}
| Technique 1 | Technique 2 | Technique 3 | |||||
|---|---|---|---|---|---|---|---|
| Mean (SD) | [95%CI] | Mean (SD) | [95%CI] | Mean (SD) | [95%CI] | ||
| >15 years | −63.92 (12.721) | [−69.17 to −58.67] | 44.48 (7.880) | [41.43 to 47.73] | −56.28 (10.872) | [−60.77 to −51.79] | |
| 5–10 years | Observer 1 | −56.68 (17.509) | [−63.91 to −49.45] | 41.16 (10.896) | [36.66 to 45.66] | −53.36 (11.090) | [−57.94 to −48.78] |
| Observer 2 | −53.92 (18.307) | [−61.48 to −46.36] | 40.00 (8.869) | [36.34 to 43.66] | −51.48 (10.621) | [−56.22 to −47.46] | |
| 1–5 years | Observer 1 | −6.88 (2.068) | [−7.73 to −6.03] | 20.06 (3.697) | [19.07 to 22.13] | −59.08 (18.632) | [−66.77 to −51.39] |
| Observer 2 | −19.56 (3.731) | [−21.10 to −18.02] | 22.92 (2.886) | [21.73 to 24.11] | −37.28 (8.142) | [−40.67 to −33.92] | |
| <1 year | Observer 1 | −6.80 (3.488) | [−8.24 to −5.36] | 16.16 (4.972) | [14.11 to 18.21] | −39.40 (9.954) | [−43.51 to −35.29] |
| Observer 2 | −10.08 (4.890) | [−12.10 to −8.06] | 26.72 (6.202) | [24.16 to 29.28] | −36.28 (9.374) | [−40.15 to −32.41] | |
| Technique 1 | ||||||
|---|---|---|---|---|---|---|
| Measures | Mean Differences (SD) | 95% Limits of Agreement | ICC | [95%CI] | ||
| 5–10 years | Observer 1—>15 years | 25 | −7.240 (10.868) | −11.726 to −2.754 | 0.809 | [0.444 to 0.924] |
| Observer 2—>15 years | 25 | −10.000 (13.491) | −15.569 to −4.431 | 0.696 | [0.173 to 0.877] | |
| 1–5 years | Observer 1—>15 years | 25 | −57.040 (13.843) | −62.754 to −51.326 | 0.015 | [−0.051 to 0.067] |
| Observer 2—>15 years | 25 | −44.360 (11.676) | −49.180 to −39.540 | 0.036 | [−0.042 to 0.184] | |
| <1 year | Observer 1—>15 years | 25 | −57.120 (10.635) | −61.510 to −52.730 | 0.035 | [−0.027 to 0.170] |
| Observer 2—>15 years | 25 | −53.840 (10.656)) | −58.239 to −49.441 | 0.046 | [−0.031 to 0.213] | |
| Technique 2 | ||||||
| Measures | Mean Differences (SD) | 95% Limits of Agreement | ICC | [95%CI] | ||
| 5–10 years | Observer 1—>15 years | 25 | 3.320 (6.310) | 0.716 to 5.924 | 0.851 | [0.620 to 0.938] |
| Observer 2—>15 years | 25 | 4.480 (6.404) | 1.837 to 7.123 | 0.770 | [0.339 to 0.909] | |
| 1–5 years | Observer 1—>15 years | 25 | 23.880 (7.965) | 20.592 to 27.168 | 0.038 | [−0.059 to 0.205] |
| Observer 2—>15 years | 25 | 21.560 (7.969) | 18.271 to 24.849 | 0.026 | [−0.066 to 0.184] | |
| <1 year | Observer 1—>15 years | 25 | 28.320 (9.371) | 24.452 to 32.188 | 0.002 | [−0.061 to 0.109] |
| Observer 2—>15 years | 25 | 17.760 (7.102) | 14.828 to 20.692 | 0.216 | [−0.124 to 0.586] | |
| Technique 3 | ||||||
| Measures | Mean Differences (SD) | 95% Limits of Agreement | ICC | [95%CI] | ||
| 5–10 years | Observer 1—>15 years | 25 | −2.920 (7.354) | −5.955 to 0.115 | 0.861 | [0.678 to 0.939] |
| Observer 2—>15 years | 25 | −4.440 (7.534) | −7.550 to −1.330 | 0.824 | [0.529 to 0.928] | |
| 1–5 years | Observer 1—>15 years | 25 | 2.800 (12.261) | −2.261 to 7.861 | 0.806 | [0.565 to 0.914] |
| Observer 2—>15 years | 25 | −19.000 (7.269) | −22.000 to −16.000 | 0.390 | [−0.127 to 0.766] | |
| <1 year | Observer 1—>15 years | 25 | −16.880 (9.293) | −20.716 to −13.044 | 0.416 | [−0.209 to 0.769] |
| Observer 2—>15 years | 25 | −20.000 (7.522) | −23.105 to −16.895 | 0.397 | [−0.124 to 0.772] | |
| Technique 1 | Technique 2 | Technique 3 | |||||
|---|---|---|---|---|---|---|---|
| ICC | [95%CI] | ICC | [95%CI] | ICC | [95%CI] | ||
| 5–10 years | Observers—>15 years | 0.760 | [0.288 to 0.906] | 0.856 | [0.499 to 0.946] | 0.856 | [0.627 to 0.940] |
| 1–5 years | Observers—>15 years | 0.003 | [−0.032 to 0.075] | 0.032 | [−0.058 to 0.191] | 0.480 | [−0.086 to 0.762] |
| <1 year | Observers—>15 years | 0.040 | [−0.028 to 0.191] | 0.077 | [−0.072 to 0.318] | 0.413 | [−0.142 to 0.781] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Requena-García, J.; García-Nieto, E.; Varillas-Delgado, D. Objectivation of an Educational Model in Cranial Osteopathy Based on Experience. Medicina 2021, 57, 246. https://doi.org/10.3390/medicina57030246
Requena-García J, García-Nieto E, Varillas-Delgado D. Objectivation of an Educational Model in Cranial Osteopathy Based on Experience. Medicina. 2021; 57(3):246. https://doi.org/10.3390/medicina57030246
Chicago/Turabian StyleRequena-García, Jesús, Evelyn García-Nieto, and David Varillas-Delgado. 2021. "Objectivation of an Educational Model in Cranial Osteopathy Based on Experience" Medicina 57, no. 3: 246. https://doi.org/10.3390/medicina57030246
APA StyleRequena-García, J., García-Nieto, E., & Varillas-Delgado, D. (2021). Objectivation of an Educational Model in Cranial Osteopathy Based on Experience. Medicina, 57(3), 246. https://doi.org/10.3390/medicina57030246