
Cryobiopsy in Lung Cancer Diagnosis—A Literature Review

Abstract
:1. Introduction
- Biopsy of malignant endobronchial growth tumors,
- Tangential biopsy of malignant infiltrating tumors that are hard to sample using conventional forceps biopsy,
- Biopsy of benign tumors,
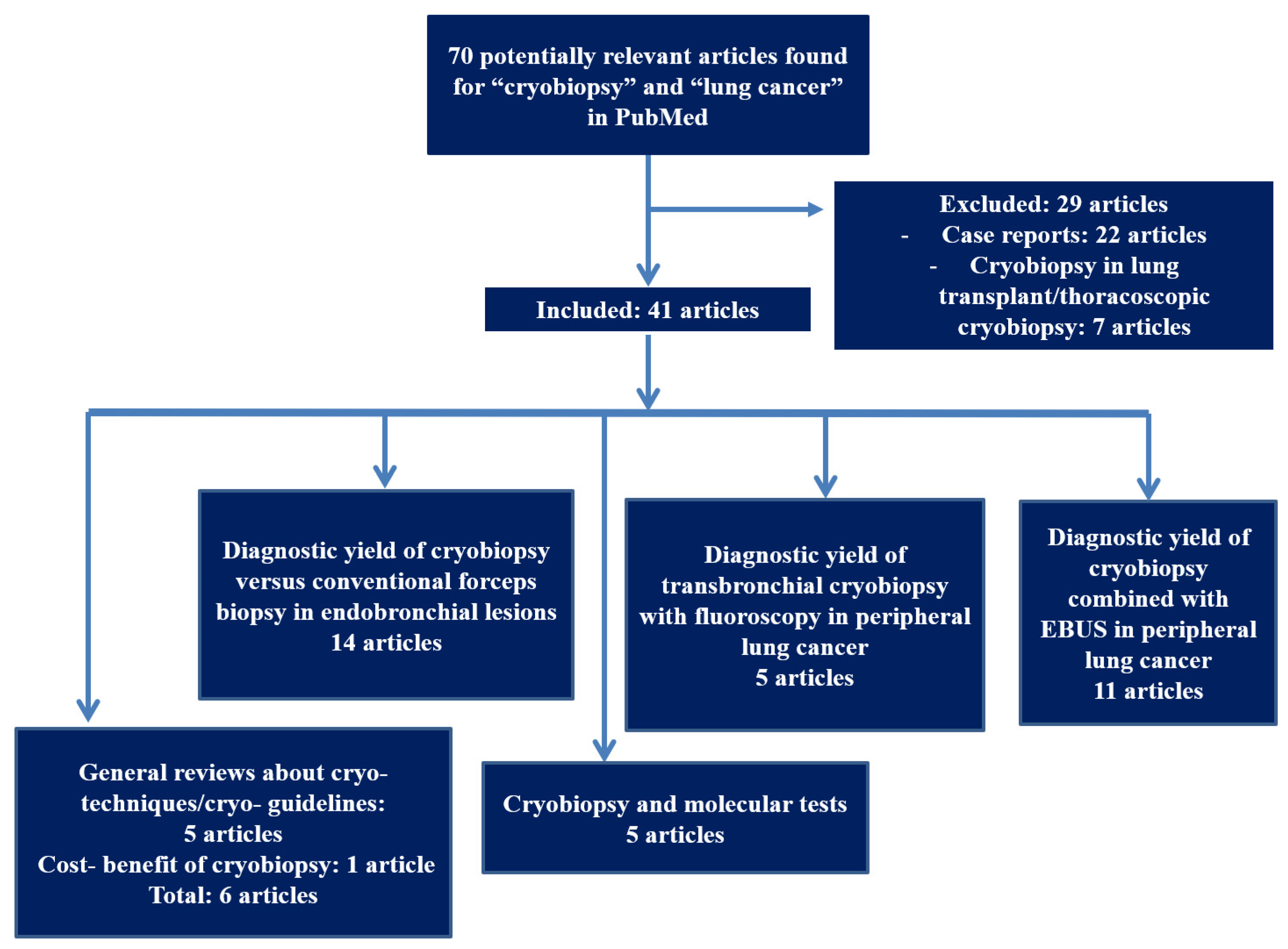
2. Study Selection
3. Diagnostic Yield of Cryobiopsy versus Conventional Forceps Biopsy in Endobronchial Lesions
4. Diagnostic Yield of Transbronchial Cryobiopsy in Peripheral Lung Cancer
5. Cryobiopsy and Molecular Tests
6. Advantages of Cryobiopsy
- -
- the larger size and volume of the collected sample,
- -
- the well-preserved tissue samples for histopathologic, molecular and genetic analysis,
- -
- less crush artifacts.
7. Limitations and Complications of Cryobiopsy
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tomic, R.; Podgaetz, E.; Andrade, R.S.; Dincer, H.E. Cryotechnology in Diagnosing and Treating Lung Diseases. J. Bronchol. Interv. Pulmonol. 2015, 22, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Hetzel, J.; Linzenbold, W.; Boesmueller, H.; Enderle, M.; Poletti, V. Evaluation of Efficacy of a New Cryoprobe for Transbronchial Cryobiopsy: A Randomized, Controlled in vivo Animal Study. Respiration 2020, 99, 1–9. [Google Scholar] [CrossRef]
- Hetzel, J.; Hetzel, M.; Hasel, C.; Moeller, P.; Babiak, A. Old Meets Modern: The Use of Traditional Cryoprobes in the Age of Molecular Biology. Respiration 2008, 76, 193–197. [Google Scholar] [CrossRef]
- Schumann, C.; Hetzel, J.; Babiak, A.J.; Merk, T.; Wibmer, T.; Möller, P.; Lepper, P.M.; Hetzel, M. Cryoprobe biopsy increases the diagnostic yield in endobronchial tumor lesions. J. Thorac. Cardiovasc. Surg. 2010, 140, 417–421. [Google Scholar] [CrossRef] [Green Version]
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global Epidemiology of Lung Cancer. Ann. Glob. Health 2019, 85, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travis, W.D. Pathology of Lung Cancer. Clin. Chest Med. 2011, 32, 669–692. [Google Scholar] [CrossRef] [PubMed]
- Santini, F.C.; Hellmann, M.D. PD-1/PD-L1 Axis in Lung Cancer. Cancer J. 2018, 24, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.S.; Sharshar, R.S.; Wasfy, R.E. The diagnostic yield of cryobiopsy versus forceps biopsy of malignant endobronchial lesions. Egypt. J. Chest Dis. Tuberc. 2016, 65, 267–270. [Google Scholar] [CrossRef] [Green Version]
- Hetzel, J.R.; Eberhardt, R.; Herth, F.J.F.; Petermann, C.; Reichle, G.; Freitag, L.; Dobbertin, I.; Franke, K.J.; Stanzel, F.; Beyer, T.; et al. Cryobiopsy increases the diagnostic yield of endobronchial biopsy: A multicentre trial. Eur. Respir. J. 2012, 39, 685–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivera, M.P.; Mehta, A.C. Initial Diagnosis of Lung Cancer. Chest 2007, 132 (Suppl. 3), 131S–148S. [Google Scholar] [CrossRef] [Green Version]
- Popp, W.; Rauscher, H.; Ritschka, L.; Redtenbacher, S.; Zwick, H.; Dutz, W. Diagnostic sensitivity of different techniques in the diagnosis of lung tumors with the flexible fiberoptic bronchoscope. Comparison of brush biopsy, imprint cytology of forceps biopsy, and histology of forceps biopsy. Cancer 1991, 67, 72–75. [Google Scholar] [CrossRef]
- Ehab, A.; El-Badrawy, M.K.; Moawad, A.A.; Abo-Shehata, M.E.-D. Cryobiopsy versus forceps biopsy in endobronchial lesions, diagnostic yield and safety. Adv. Respir. Med. 2017, 85, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Rubio, E.R.; Le, S.R.; Whatley, R.E.; Boyd, M.B. Cryobiopsy: Should This Be Used in Place of Endobronchial Forceps Biopsies? BioMed Res. Int. 2013, 2013, 730574. [Google Scholar] [CrossRef] [PubMed]
- Kvale, P.A. Collection and preparation of bronchoscopic specimens. Chest 1978, 73 (Suppl. 5), 707–712. [Google Scholar] [CrossRef] [PubMed]
- Gunay, E.; Hoca, N.T.; Yilmaz, A.; Demirag, F.; Gunay, S.; Sipit, T.; Kurt, E.B.; Aktas, Z. Endobronchial cryobiopsy or forceps biopsy for lung cancer diagnosis. Ann. Thorac. Med. 2010, 5, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Segmen, F.; Aktaş, Z.; Öztürk, A.; Kızılgöz, D.; Yılmaz, A.; Alıcı, I.O.; Demirağ, F.; Pehlivanoğlu, P. How many samples would be optimal for endobronchial cryobiopsy? Surg. Endosc. 2017, 31, 1219–1224. [Google Scholar] [CrossRef] [PubMed]
- Joyner, L.R.; Scheinhorn, D.J. Transbronchial Forceps Lung Biopsy through the Fiberoptic Bronchoscope. Chest 1975, 67, 532–535. [Google Scholar] [CrossRef] [Green Version]
- Cazzato, S.; Zompatori, M.; Burzi, M.; Baruzzi, G.; Falcone, F.; Poletti, V. Bronchoalveolar lavage and transbronchial lung biopsy in alveolar and/or ground-glass opacification. Monaldi Arch. Chest Dis. 1999, 54, 115–119. [Google Scholar]
- Verhoeven, R.L.; Fütterer, J.J.; Hoefsloot, W.; Van Der Heijden, E.H. Cone-Beam CT Image Guidance With and Without Electromagnetic Navigation Bronchoscopy for Biopsy of Peripheral Pulmonary Lesions. J. Bronchol. Interv. Pulmonol. 2021, 28, 60–69. [Google Scholar] [CrossRef]
- Poletti, V.; Casoni, G.L.; Gurioli, C.; Ryu, J.H.; Tomassetti, S. Lung cryobiopsies: A paradigm shift in diagnostic bronchoscopy? Respirol. 2014, 19, 645–654. [Google Scholar] [CrossRef]
- Nasu, S.; Okamoto, N.; Suzuki, H.; Shiroyama, T.; Tanaka, A.; Samejima, Y.; Kanai, T.; Noda, Y.; Morita, S.; Morishita, N.; et al. Comparison of the Utilities of Cryobiopsy and Forceps Biopsy for Peripheral Lung Cancer. Anticancer. Res. 2019, 39, 5683–5688. [Google Scholar] [CrossRef]
- Imabayashi, T.; Uchino, J.; Yoshimura, A.; Chihara, Y.; Tamiya, N.; Kaneko, Y.; Yamada, T.; Takayama, K. Safety and Usefulness of Cryobiopsy and Stamp Cytology for the Diagnosis of Peripheral Pulmonary Lesions. Cancers 2019, 11, 410. [Google Scholar] [CrossRef] [Green Version]
- Şimon, M.; Pop, B.; Toma, I.L.; Vallasek, A.K.; Şimon, I. The use of EBUS-TBNA and ROSE in the diagnosis of lung cancer. Rom. J. Morphol. Embryol. Rev. Roum. Morphol. Embryol. 2017, 58, 79–87. [Google Scholar]
- Rivera, M.P.; Mehta, A.C.; Wahidi, M.M. Establishing the diagnosis of lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e142S–e165S. [Google Scholar] [CrossRef]
- Shirakawa, T.; Imamura, F.; Hamamoto, J.; Honda, I.; Fukushima, K.; Sugimoto, M.; Shirkakusa, T. Usefulness of endobronchial ultra-sonography for transbronchial lung biopsies of peripheral lung lesions. Respiration 2004, 71, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Asahina, H.; Yamazaki, K.; Onodera, Y.; Kikuchi, E.; Shinagawa, N.; Asano, F.; Nishimura, M. Transbronchial Biopsy Using Endobronchial Ultrasonography With a Guide Sheath and Virtual Bronchoscopic Navigation. Chest 2005, 128, 1761–1765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herth, F.J.; Eberhardt, R.; Becker, H.D.; Ernst, A. Endobronchial ultrasound-guided transbronchial lung biopsy in fluoroscop-ically invisible solitary pulmonary nodules: A prospective trial. Chest 2006, 129, 147–150. [Google Scholar] [CrossRef]
- Takai, M.; Izumo, T.; Chavez, C.; Tsuchida, T.; Sasada, S. Transbronchial needle aspiration through a guide sheath with en-dobronchial ultrasonography (GS-TBNA) for peripheral pulmonary lesions. Ann. Thorac. Cardiovasc. Surg. 2014, 20, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Arimura, K.; Sekine, Y.; Hiroshima, K.; Sato, A.; Hasegawa, M.; Katsura, H.; Tagaya, E.; Kondo, M.; Tamaoki, J. The efficacy of transbronchial needle aspi-ration with endobronchial ultrasonography using a guide sheath for peripheral pulmonary lesions suspected to be lung cancer. Respir. Investig. 2017, 55, 365–371. [Google Scholar] [CrossRef]
- Schuhmann, M.; Bostanci, K.; Bugalho, A.; Warth, A.; Schnabel, P.A.; Herth, F.J.; Eberhardt, R. Endobronchial ultrasound-guided cryobiopsies in peripheral pulmonary lesions: A feasibility study. Eur. Respir. J. 2013, 43, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Arimura, K.; Tagaya, E.; Akagawa, H.; Nagashima, Y.; Shimizu, S.; Atsumi, Y.; Sato, A.; Kanzaki, M.; Kondo, M.; Takeyama, K.; et al. Cryobiopsy with endobronchial ultrasonography using a guide sheath for peripheral pulmonary lesions and DNA analysis by next generation sequencing and rapid on-site evaluation. Respir. Investig. 2019, 57, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Taton, O.; Bondue, B.; Gevenois, P.A.; Remmelink, M.; Leduc, D. Diagnostic Yield of Combined Pulmonary Cryobiopsies and Electromagnetic Navigation in Small Pulmonary Nodules. Pulm. Med. 2018, 2018, 6032974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pannu, J.K.; Roller, L.J.; Lentz, R.J.; Rickman, O.B.; Aboudara, M.C.; Chen, H.; Maldonado, F. Cryobiopsy With Radial UltraSound Guidance (CYRUS). J. Bronchol. Interv. Pulmonol. 2021, 28, 21–28. [Google Scholar] [CrossRef]
- Hibare, K.R.; Goyal, R.; Nemani, C.; Avinash, R.; Bajpai, R.; Ullas, B. Radial endobronchial ultrasound for the diagnosis of bronchoscopically invisible lesions: First case series from India. Lung India 2017, 34, 43–46. [Google Scholar] [CrossRef]
- Kho, S.S.; Chan, S.K.; Yong, M.C.; Tie, S.T. Performance of transbronchial cryobiopsy in eccentrically and adjacently orientated radial endobronchial ultrasound lesions. ERJ Open Res. 2019, 5, 00135–02019. [Google Scholar] [CrossRef]
- Herath, S.; Yap, E. Novel hybrid cryo-radial method: An emerging alternative to CT-guided biopsy in suspected lung cancer. A prospective case series and description of technique. Respirol. Case Rep. 2018, 6, e00287. [Google Scholar] [CrossRef] [Green Version]
- Arimura, K.; Kondo, M.; Nagashima, Y.; Kanzaki, M.; Kobayashi, F.; Takeyama, K.; Tamaoki, J.; Tagaya, E. Comparison of tumor cell numbers and 22C3 PD-L1 expression between cryobiopsy and transbronchial biopsy with endobronchial ultrasonography-guide sheath for lung cancer. Respir. Res. 2019, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Udagawa, H.; Kirita, K.; Naito, T.; Nomura, S.; Ishibashi, M.; Matsuzawa, R.; Hisakane, K.; Usui, Y.; Matsumoto, S.; Yoh, K.; et al. Feasibility and utility of transbronchial cryobiopsy in precision medicine for lung cancer: Prospective single-arm study. Cancer Sci. 2020, 111, 2488–2498. [Google Scholar] [CrossRef]
- Lim, W.; Ridge, C.A.; Nicholson, A.G.; Mirsadraee, S. The 8th lung cancer TNM classification and clinical staging system: Review of the changes and clinical implications. Quant. Imaging Med. Surg. 2018, 8, 709–718. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.; Yatabe, Y.; Ishikawa, Y.; Wistuba, I.; Flieder, D.B.; Franklin, W.; et al. Diagnosis of Lung Cancer in Small Biopsies and Cytology: Implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society Classification. Arch. Pathol. Lab. Med. 2013, 137, 668–684. [Google Scholar] [CrossRef] [Green Version]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Haranguș, A.; Berindan-Neagoe, I.; Todea, D.A.; Șimon, I.; Șimon, M. Noncoding RNAs and Liquid Biopsy in Lung Cancer: A Literature Review. Diagnostics 2019, 9, 216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haentschel, M.; Boeckeler, M.; Ehab, A.; Wagner, R.; Spengler, W.; Steger, V.; Boesmueller, H.; Horger, M.; Lewis, R.A.; Fend, F.; et al. Cryobiopsy increases the EGFR detection rate in non-small cell lung cancer. Lung Cancer 2020, 141, 56–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindeman, N.I.; Cagle, P.T.; Beasley, M.B.; Chitale, D.A.; Dacic, S.; Giaccone, G.; Jenkins, R.B.; Kwiatkowski, D.J.; Saldivar, J.-S.; Squire, J.A.; et al. Molecular Testing Guideline for Selection of Lung Cancer Patients for EGFR and ALK Tyrosine Kinase Inhibitors: Guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J. Thorac. Oncol. 2013, 8, 823–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massarelli, E.; Papadimitrakopoulou, V.; Welsh, J.; Tang, C.; Tsao, A.S. Immunotherapy in lung cancer. Transl. Lung Cancer Res. 2014, 3, 53–63. [Google Scholar]
- Ravaglia, C.; Bonifazi, M.; Wells, A.U.; Tomassetti, S.; Gurioli, C.; Piciucchi, S.; Dubini, A.; Tantalocco, P.; Sanna, S.; Negri, E.; et al. Safety and Diagnostic Yield of Transbronchial Lung Cryobiopsy in Diffuse Parenchymal Lung Diseases: A Comparative Study versus Video-Assisted Thoracoscopic Lung Biopsy and a Systematic Review of the Literature. Respiration 2016, 91, 215–227. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Author | Study Design | Number of Patients | Median Size of Biopsy Sample TBB vs. TBLC | Use of EBUS or Fluoroscopy | Comments |
|---|---|---|---|---|---|
| Nasu et al. [21] | Retrospective | 53 | 2.62/14.1 mm2 | r-EBUS + GS | Cryobiopsy with GS in PPLs with positive bronchus sign significantly increases diagnostic yield (OR = 11.6, p = 0.044) |
| Imabayashi et al. [22] | Retrospective | 38 | NA/12.2 mm2 | r-EBUS | Diagnostic yield of CB increased from 86.1% to 91.6% when adding stamp cytology. |
| Schuhmann et al. [30] | Randomized controlled study | 38 | 4.69/11.17 mm2 | r-EBUS +GS | Time of TBLC was significantly longer when compared to TBB. Diagnostic yield was of 61.3% (19/31) for TBB and 74.2% (23/31) for TBLC (p = 0.42) |
| Arimura et al. [31] | Prospective | 23 | 0.003 ± 0.0003/0.078 ± 0.008 (mean ± SEM) cm3 | r-EBUS + GS + Fluoroscopy | Higher diagnostic accuracy for TBLB in comparison to TBB (87% versus 82.6%). Sufficient quantity and quality for DNA analysis by NGS. |
| Taton et. al. [32] | Prospective | 32 | 1.1 ± 0.6/5.3 ± 0.7 mm | r-EBUS + GS | No statistically significant impact on the diagnostic yield for the location or size of nodule or the technique use (visualization with EBUS mini probe) |
| Hibare et al. [34] | Retrospective | 55 | NA | Radial EBUS ± GS ± Fluoroscopy | No significant difference was found in diagnostic yield between TBB or TBLC. 14% of lesions could not be located by r-EBUS |
| Kho et al. [35] | Retrospectve | 114 | NA | Radial EBUS ± GS ± Fluoroscopy | The addition of rapid on-site cytology (ROSE) increased the sensitivity, specificity, PPV and diagnostic accuracy |
| Herath et al. [36] | Prospective | 6 | 3.4/6.4 mm | Radial EBUS + GS | The GS was trimmed by 3 cm from the distal end of the scope for a better contact. |
| Udagawa et al. [38] | Prospective | 121 | 2/15 mm2 | Radial EBUS ± GS + Fluoroscopy | Larger amounts of DNA and RNA with TBLC (a median of 1.60 µg DNA and 0.62 µg RNA with cryoprobe vs. 0.58 µg DNA and 0.17 µg RNA with forceps). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simon, M.; Simon, I.; Tent, P.A.; Todea, D.A.; Haranguș, A. Cryobiopsy in Lung Cancer Diagnosis—A Literature Review. Medicina 2021, 57, 393. https://doi.org/10.3390/medicina57040393
Simon M, Simon I, Tent PA, Todea DA, Haranguș A. Cryobiopsy in Lung Cancer Diagnosis—A Literature Review. Medicina. 2021; 57(4):393. https://doi.org/10.3390/medicina57040393
Chicago/Turabian StyleSimon, Mărioara, Ioan Simon, Paul Andrei Tent, Doina Adina Todea, and Antonia Haranguș. 2021. "Cryobiopsy in Lung Cancer Diagnosis—A Literature Review" Medicina 57, no. 4: 393. https://doi.org/10.3390/medicina57040393