
The Impact of Monitoring Depth of Anesthesia and Nociception on Postoperative Cognitive Function in Adult Multiple Trauma Patients


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
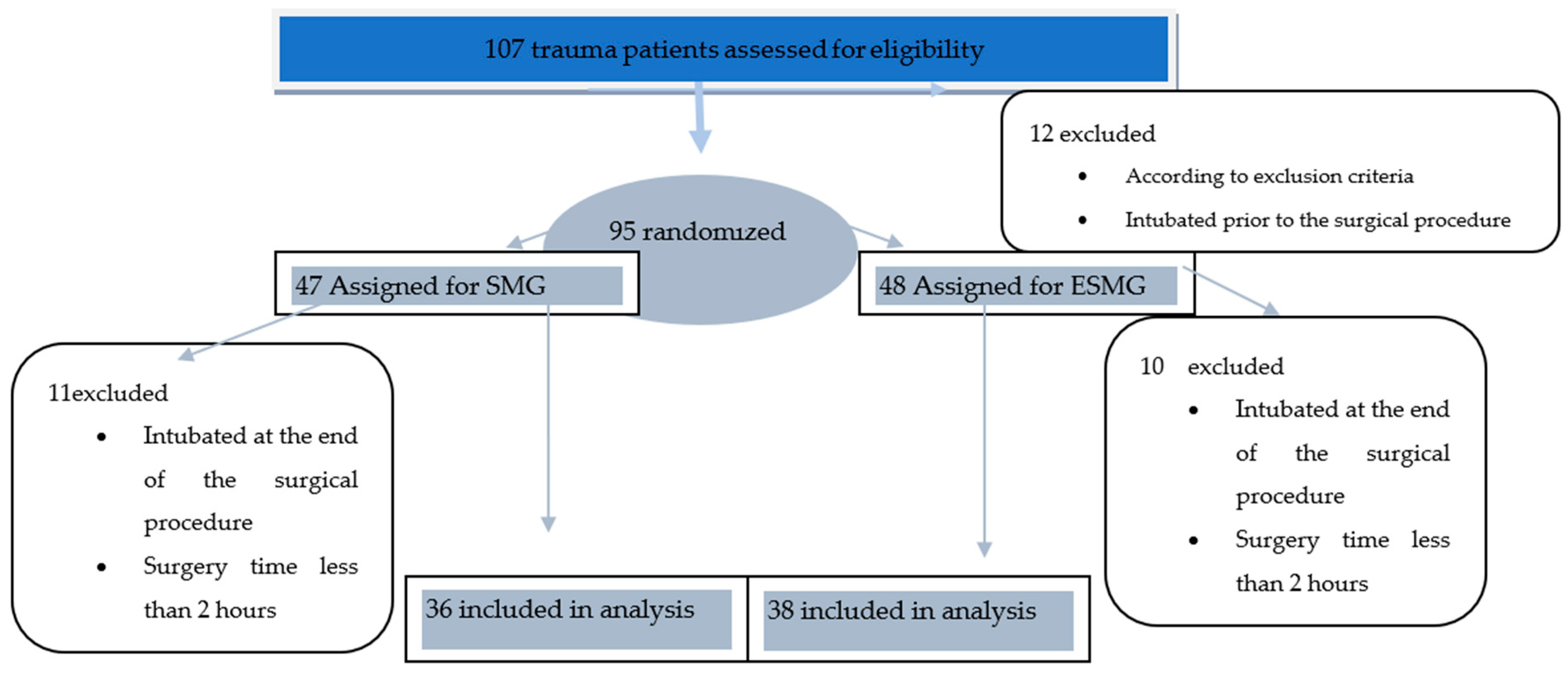
2.1. Study Design
2.2. Anesthesia
2.3. Data Collection, Assesment of Postoperative of POCD, and Delirium
2.4. Statistical Analysis
3. Results
Postoperative Delirium and Cognitive Dysfunction
4. Discussion
5. Limits
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bedford, P.D. Adverse cerebral effects of anaesthesia on old people. Lancet 1955, 266, 259–263. [Google Scholar] [CrossRef]
- Ramaiah, R. What’s new in emergencies, trauma and shock? Anesthesia, surgery and postoperative cognition. J. Emergencies Trauma Shock 2011, 4, 1–2. [Google Scholar] [CrossRef]
- Kotekar, N.; Shenkar, A.; Nagaraj, R. Postoperative cognitive dysfunction—Current preventive strategies. Clin. Interv. Aging 2018, 13, 2267–2273. [Google Scholar] [CrossRef] [Green Version]
- Rundshagen, I. Postoperative cognitive dysfunction. Dtsch. Arztebl. Int. 2014, 111, 119–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, S.D.; Stygall, J.; Hirani, S.; Shaefi, S.; Maze, M. Postoperative cognitive dysfunction after noncardiac surgery: A systematic review. Anesthesiology 2007, 106, 572–590. [Google Scholar] [CrossRef]
- Monk, T.G.; Weldon, B.C.; Garvan, C.W.; Dede, D.E.; Van Der Aa, M.T.; Heilman, K.M.; Gravenstein, J.S. Predictors of cognitive dysfunction after major noncardiac surgery. Anesthesiology 2008, 108, 18–30. [Google Scholar] [CrossRef] [Green Version]
- Culley, D.J.; Monk, T.G.; Cosby, G. Post-Operative Central Nervous System Dysfunction, Geriatric Anaesthesiology, 2nd ed.; Springer: New York, NY, USA, 2018; Volume 9, pp. 123–136. [Google Scholar]
- Steinmetz, J.; Christensen, K.B.; Lund, T.; Lohse, N.; Rasmussen, L.S.; ISPOCD Group. Long-term consequences of postoperative cognitive dysfunction. Anesthesiology 2009, 110, 548–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neelon, V.J.; Champagne, M.T.; Carlson, J.R.; Funk, S.G. The NEECHAM Confusion Scale: Construction, validation, and clinical testing. Nurs. Res. 1996, 45, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Polderman, K.H. Screening methods for delirium: Don’t get confused! Intensive Care Med. 2007, 33, 3–5. [Google Scholar] [CrossRef]
- Van Rompaey, B.; Schuurmans, M.J.; Shortridge-Baggett, L.M.; Truijen, S.; Elseviers, M.; Bossaert, L. A comparison of the CAM-ICU and the NEECHAM Confusion Scale in intensive care delirium assessment: An observational study in non-intubated patients. Crit Care 2008, 12, R16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, D.; Ballard, C.; Kunst, G. Depth of anaesthesiaoptimisation and postoperative cognitive dysfunction. BJA Br. J. 2015, 114, 343–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viertio-Oja, H.; Maja, V.; Sarkela, M.; Talja, P.; Tenkanen, N.; Tolvanen-Laakso, H.; Paloheimo, M.; Vakkuri, A.; Yli-Hankala, A. Description of the Entropy (TM) algorithm as applied in the Datex-Ohmeda S/5 (TM) Entropy Module. Acta Anaesthesiol. Scand. 2004, 48, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Won, Y.J.; Lim, B.G.; Kim, Y.S.; Lee, M.; Kim, H. Usefulness of surgical pleth index-guided analgesia during general anesthesia: A systematic review and meta-analysis of randomized controlled trials. J. Int. Med. Res. 2018, 46, 4386–4398. [Google Scholar] [CrossRef] [Green Version]
- Bonhomme, V.; Uutela, K.; Hans, G.; Maquoi, I.; Born, J.D.; Brichant, J.F.; Lamy, M.; Hans, P. Comparison of the surgical Pleth Index™ with haemodynamic variables to assess nociception-anti-nociception balance during general anaesthesia. Br. J. Anaesth. 2011, 106, 101–111. [Google Scholar] [CrossRef] [Green Version]
- Ancelin, M.L.; de Roquefeuil, G.; Ledésert, B.; Bonnel, F.; Cheminal, J.C.; Ritchie, K. Exposure to anaesthetic agents, cognitive functioning and depressive symptomatology in the elderly. Br. J. Psychiatry 2001, 178, 360–366. [Google Scholar] [CrossRef]
- Chan, M.T.V.; Cheng, B.C.P.; Lee, T.M.C.; Gin, T.; Coda Trial Group. BIS-guided anesthesia decreases postoperative delirium and cognitive decline. J. Neurosurg. Anesthesiol. 2013, 25, 33–42. [Google Scholar] [CrossRef]
- Chen, X.; Thee, C.; Gruenewald, M.; Wnent, J.; Illies, C.; Hoecker, J.; Hanss, R.; Steinfath, M.; Bein, B. Comparison of surgical stress index-guided analgesia with standard clinical practice during routine general anesthesia: A pilot study. Anesthesiology 2010, 112, 1175–1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rundshagen, I.; Hardt, T.; Cortina, K.; Pragst, F.; Fritzsche, T.; Spies, C. Narcotrend-assisted propofol/remifentanil anaesthesia vs clinical practice: Does it make a difference? Br. J. Anaesth. 2007, 99, 686–693. [Google Scholar] [CrossRef] [Green Version]
- Hor, T.; Linden, P.; Hert, S.; Mélot, C.; Bidgoli, J. Impact of entropy monitoring on volatile anesthetic uptake. Anesthesiology 2013, 118, 868–873. [Google Scholar] [CrossRef] [Green Version]
- Fedorow, C.; Grocott, H.P. Cerebral monitoring to optimize outcomes after cardiac surgery. Curr. Opin. Anaesthesiol. 2010, 23, 89–94. [Google Scholar] [CrossRef]
- Micha, G.; Tzimas, P.; Zalonis, I.; Kotsis, K.; Papdopoulos, G.; Arnaoutoglou, E. Propofol vs Sevoflurane anaesthesia on postoperative cognitive dysfunction in the elderly. A randomized controlled trial. Acta Anaesthesiol. Belg. 2016, 67, 129–137. [Google Scholar]
- Jiahai, M.; Xueyan, W.; Yonggang, X.; Jianhong, Y.; Qunhui, H.; Zhi, L.; Juan, D.; Xiuliang, J. Spectral entropy monitoring reduces anesthetic dosage for patients undergoing off-pump coronary artery bypass graft surgery. J. Cardiothorac. Vasc. Anesth. 2012, 26, 818–821. [Google Scholar] [CrossRef] [PubMed]
- Gruenewald, M.; Zhou, J.; Schloemerkemper, N.; Meybohm, P.; Weiler, N.; Tonner, P.H.; Scholz, J.; Bein, B. M-Entropy guidance vs standard practice during propofol-remifentanil anaesthesia: A randomised controlled trial. Anaesthesia 2007, 62, 1224–1229. [Google Scholar] [CrossRef]
- MacKenzie, K.K.; Britt-Spells, A.M.; Sands, L.P.; Leung, J.M. Processed Electroencephalogram Monitoring and Postoperative Delirium: A Systematic Review and Meta-analysis. Anesthesiology 2018, 129, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, J.; DePalma, G.; Tsai, T.T.; Sands, L.P.; Leung, J.M. Impact of intraoperative hypotension and blood pressure fluctuations on early postoperative delirium after non-cardiac surgery. Br. J. Anaesth. 2015, 115, 418–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selnes, O.A.; McKhann, G.M. Neurocognitive complications after coronary artery bypass surgery. Ann. Neurol. 2005, 57, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.C.; Wang, P.C.; Liao, W.T.; Shih, T.H.; Chang, K.A.; Lin, K.C.; Chou, A.K. Use of spectral entropy monitoring in reducing the quantity of sevoflurane as sole inhalational anesthetic and in decreasing the need for antihypertensive drugs in total knee replacement surgery. Acta Anaesthesiol. Taiwanica. 2008, 46, 106–111. [Google Scholar] [CrossRef]
- Ansaloni, L.; Catena, F.; Chattat, R.; Fortuna, D.; Franceschi, C.; Mascitti, P.; Melotti, R.M. Risk factors and incidence of postoperative delirium in elderly patients after elective and emergency surgery. Br. J. Surg. 2010, 97, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Brassard, P.; Seifert, T.; Secher, N.H. Is cerebral oxygenation negatively affected by infusion of norepinephrine in healthy subjects? Br. J. Anaesth. 2009, 102, 800–805. [Google Scholar] [CrossRef] [Green Version]
- Müller, S.; How, O.-J.; Hermansen, S.E.; Stenberg, T.A.; Sager, G.; Myrmel, T. Vasopressin impairs brain, heart and kidney perfusion: An experimental study in pigs after transient myocardial ischemia. Crit Care 2008, 12, R20. [Google Scholar] [CrossRef] [Green Version]
- Feinkohl, I.; Winterer, G.; Pischon, T. Hypertension and Risk of Post-Operative Cognitive Dysfunction (POCD): A Systematic Review and Meta-Analysis. Clin. Pract. Epidemiol. Ment. Health 2017, 13, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Feinkohl, I.; Winterer, G.; Pischon, T. Obesity and post-operative cognitive dysfunction: A systematic review and meta-analysis. Diabetes Metab. Res. Rev. 2016, 32, 643–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| SMG (n = 36) | ESMG (n = 38) | p-Value | ||
|---|---|---|---|---|
| Gender—Female/male ** | 15/21 | 17/21 | ||
| ASA Score *, n (%) ** | II | 12(33.3) | 9(23.6) | p = 0.582 |
| III | 17(47.2) | 18(47.3) | ||
| IV | 7(19.4) | 11(28.9) | ||
| Patient Characteristics | Median Group ESMG | Median Group SMG | 95%CI for the Median ESMG | 95%CI for the Median SMG | Interquartile Range ESMG | Interquartile Range SMG | p-Value |
|---|---|---|---|---|---|---|---|
| Age | 45 | 44 | 35.6 to 54.00 | 36.00 to 57.00 | 27.5 to 59.5 | 32.00 to 64.00 | 0.681 |
| Temperature | 36.7 | 37 | 36.5 to 36.9 | 36.7 to 37.1 | 36.4 to 37.00 | 36.5 to 37.2 | 0.024 |
| Fentanyl (µg) | 350 | 500 | 332.9 to 350.00 | 450.00 to 500.00 | 300.00 to 400.00 | 450.00 to 550.00 | <0.001 |
| Sevoflurane(mL/h) | 3.2 | 5.15 | 3.00 to 3.40 | 5.00to 5.3 | 2.9 to 3.6 | 4.9 to 5.6 | <0.001 |
| Crystalloid (mL) | 2500 | 3250 | 2500.00 to 3170.52 | 3000.00 to 4000.00 | 2500.00 to 3500.00 | 3000.00 to 4000.00 | 0.010 |
| Colloid (mL) | 1000 | 1000 | 500.00 to 1000.00 | 500.00 to 1000.00 | 500.00 to 1000.00 | 500.00 to 1000.00 | 0.324 |
| Noradrenaline (µg/kg/min) | 0.08 | 1 | 0.05 to 0.50 | 0.9 to 1.2 | 0.05 to 0.5 | 0.8 to 1.3 | <0.001 |
| SMG | ESMG | p-Value | |
|---|---|---|---|
| At least one intraoperatory episode of | |||
| Tachycardia | 10 | 12 | 0.61 |
| Bradycardia | 10 | 4 | 0.13 |
| Hypotension | 36 | 18 | 0.0001 |
| Coefficient and Standard Errors | ||||
|---|---|---|---|---|
| Variable | Coefficient | Std.Error | Wald | P |
| ESMG = 1 | 4.1 | 1.8 | 5.2 | 0.022 |
| Fentanyl µg | 0.006 | 0.004 | 1.7 | 0.182 |
| Noradrenaline µg/kg/min | 0.4 | 0.7 | 0.3 | 0.541 |
| Sevoflurane mL/h | 0.7 | 0.7 | 1.08 | 0.296 |
| Constant | −7.4 | 4.3 | 2.8 | 0.090 |
| Odds Ratios and 95% Confidence Intervals | ||||
| Variable | Odds Ratio | 95%CI | ||
| ESMG = 1 | 66.1 | 1.8 to 2423.3 | ||
| Fentanyl µg | 1.006 | 0.9 to 1.01 | ||
| Noradrenaline µg/kg/min | 1.5 | 0.3 to 7.03 | ||
| Sevoflurane mL/h | 2.1 | 0.5 to 9.3 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cotae, A.-M.; Ţigliş, M.; Cobilinschi, C.; Băetu, A.E.; Iacob, D.M.; Grinţescu, I.M. The Impact of Monitoring Depth of Anesthesia and Nociception on Postoperative Cognitive Function in Adult Multiple Trauma Patients. Medicina 2021, 57, 408. https://doi.org/10.3390/medicina57050408
Cotae A-M, Ţigliş M, Cobilinschi C, Băetu AE, Iacob DM, Grinţescu IM. The Impact of Monitoring Depth of Anesthesia and Nociception on Postoperative Cognitive Function in Adult Multiple Trauma Patients. Medicina. 2021; 57(5):408. https://doi.org/10.3390/medicina57050408
Chicago/Turabian StyleCotae, Ana-Maria, Mirela Ţigliş, Cristian Cobilinschi, Alexandru Emil Băetu, Diana Maria Iacob, and Ioana Marina Grinţescu. 2021. "The Impact of Monitoring Depth of Anesthesia and Nociception on Postoperative Cognitive Function in Adult Multiple Trauma Patients" Medicina 57, no. 5: 408. https://doi.org/10.3390/medicina57050408
APA StyleCotae, A. -M., Ţigliş, M., Cobilinschi, C., Băetu, A. E., Iacob, D. M., & Grinţescu, I. M. (2021). The Impact of Monitoring Depth of Anesthesia and Nociception on Postoperative Cognitive Function in Adult Multiple Trauma Patients. Medicina, 57(5), 408. https://doi.org/10.3390/medicina57050408